
Abstract
Background:
Continuous glucose monitors (CGMs) help people with type 1 diabetes (T1D) improve their glycemic profiles but are underutilized. To better understand why, perceived CGM burdens and benefits in nonusers versus users with type 1 diabetes across the lifespan were assessed.
Methods:
Burdens (BurCGM) and benefits of CGM (BenCGM) questionnaires were completed during T1D outpatient visits (n = 1334) from February 2019 to February 2020. Mean scores were calculated (scale one to five; higher scores reflect greater perceived burdens/benefits). Data were collected from medical records including glycated hemoglobin (HbA1c) within 3 months of the visit.
Results:
Individuals of all ages using CGM described more benefits and less burdens (mean scores 4.48 and 1.69, respectively) when compared with those who were not using CGM (mean score 4.19 and 2.35, respectively) (P < .001). There were no differences in burdens or benefits by sex. Non-CGM users aged ≥50 years had higher mean BurCGM scores than those aged <50 years (P = .004); the cost was the greatest barrier in those aged 27+ years. Other burdens were readings not trusted, painful to wear, and takes too much time to use. For those aged 65+, nonusers versus users, 18.5% versus 3.1% agreed with “it was too hard to understand CGM information,” and 21.4% versus 7.7% agreed that CGM causes too much worry. Mean HbA1C was lower in CGM users (8.1%) versus non-CGM users (mean A1c 9.1%; P < .001).
Conclusions:
CGM was perceived as having more burdens and less benefits in nonusers, with differences in concerns varying across the lifespan. Lower costs and age-appropriate education are needed to address these barriers.
Introduction
Continuous glucose monitors (CGMs) have revolutionized diabetes management, especially for people with type 1 diabetes. There is ample evidence that consistent use of CGM reduces glycemic variability, hypoglycemia, and glycated hemoglobin (HbA1c) levels1-6 and improves the quality of life.7,8 Early initiation of CGM in youth with new-onset type 1 diabetes is being employed to improve clinical outcomes. 9 In the COMISAIR study, CGM use in adults was more important than the insulin delivery method in improving glycemic outcomes. 10 In addition, a recent systematic review reports the cost-effectiveness of CGM use. 11
Despite these benefits of CGM use in people with type 1 diabetes in all age groups and endorsement of its use by the American Diabetes Association, 12 the American Association of Clinical Endocrinologists, 13 the International Society for Pediatric and Adolescent Diabetes, 14 and others, its uptake is relatively low, especially in those who use insulin injection therapy. The type 1 diabetes exchange clinic registry (n = 22,697) reported an increase in CGM use from 7% in 2012 to 38% in 2018, with the highest use in 2018 in those aged <6 years and the lowest use in those aged 18-22 years (22%). 15 Only one-third of adults aged ≥50 years in this registry were using CGM in 2018. 15
It is important to understand the reasons why people with type 1 diabetes are not using CGM in order to develop strategies to increase utilization. For young children aged <8 years with type 1 diabetes, parents describe painful insertions and challenges related to wearing multiple devices. 16 In adolescents, Messer et al 17 report barriers related to cost and the hassle and dislike of wearing the device. In adults (mean age 35 years), common barriers to CGM use were the hassle of wearing the device (47%) and dislike of wearing the device (35%).18,19 Alarm fatigue, concern about the inaccuracy, and the need for frequent calibrations have also been reported as barriers.18-21 The newest CGMs address some of these barriers since they are smaller, easier to apply, more accurate, and do not require calibration (less hassle) or confirmatory fingerstick blood glucose checks for insulin dosing, yet uptake is still relatively low. Barriers to CGM use in older adults have not been as well studied.
To better understand current barriers and perceived benefits of CGM use in our pediatric and adult patients with type 1 diabetes, we administered a brief validated survey. 22 Responses from people with type 1 diabetes currently using CGM were compared with those not using CGM across the lifespan. With a better understanding of perceived burdens in people with type 1 diabetes in different age groups who are not using CGM, targeted interventions to overcome these burdens and improve CGM uptake can be initiated. Our hypothesis was that barriers to CGM use would vary by age, with older adults having the greatest difficulty in understanding information related to CGM.
Methods
Design
This is a cross-sectional study in which surveys were distributed and collected during routine type 1 diabetes pediatric and adult visits to our diabetes center in Syracuse, NY, USA. Surveys were administered from February 2019 to February 2020 to patients with type 1 diabetes or their parent(s) if the patient was aged less than 12 years. The Burdens of CGM (BurCGM) and Benefits of CGM (BenCGM) questionnaires were used, which have been validated in adolescents. 22 Each questionnaire contained eight items which were rated on a Likert scale, one to five; a higher score indicates greater perceived burdens and benefits.
The survey responses were entered into REDCap, a HIPAA compliant web-based application developed by Vanderbilt University. Chart review was performed to collect the following data: gender, race/ethnicity, insurance, CGM and insulin pump use, CGM and insulin pump device types, and HbA1c result within three months of the visit at which the survey was completed.
Participants
Participants were any person with type 1 diabetes (or parents of children less than 12 years of age) with type 1 diabetes having a follow-up visit at our diabetes center. In total, 1757 surveys were collected, and 1334 were included for data analysis. Reasons for exclusion were: duplicate surveys (the patient had completed a survey during a previous visit) and a diagnosis of type 2 diabetes upon chart review. Informed consent was not required per the Institution for the Protection of Human Subjects at SUNY Upstate Medical University.
Analysis
Mean total scores as well as mean scores for each item were calculated separately for the BurCGM and BenCGM instruments. The t-tests were used to compare total mean scores and HbA1c by gender, CGM users versus non-CGM users, and insulin pump users versus those using multiple daily insulin injections (MDI). One-way analysis of variance followed by Tukey’s Honest Significant Difference test was used to determine differences in responses between age groups. Statistical analyses were performed using SPSS v26.
Results
Participants
Participant’s characteristics overall and by age group are shown in Table 1. The mean age was 30.0 years (SD 20.1) with a minimum age of two years and maximum age of 95 years. Approximately half of the participants were female and most were non-Hispanic white. Insurance, as expected, varied by age, with the highest percent of Medicaid in the pediatric population, and 90.2% of adults aged ≥65 years were covered by Medicare.
Participant’s Characteristics.
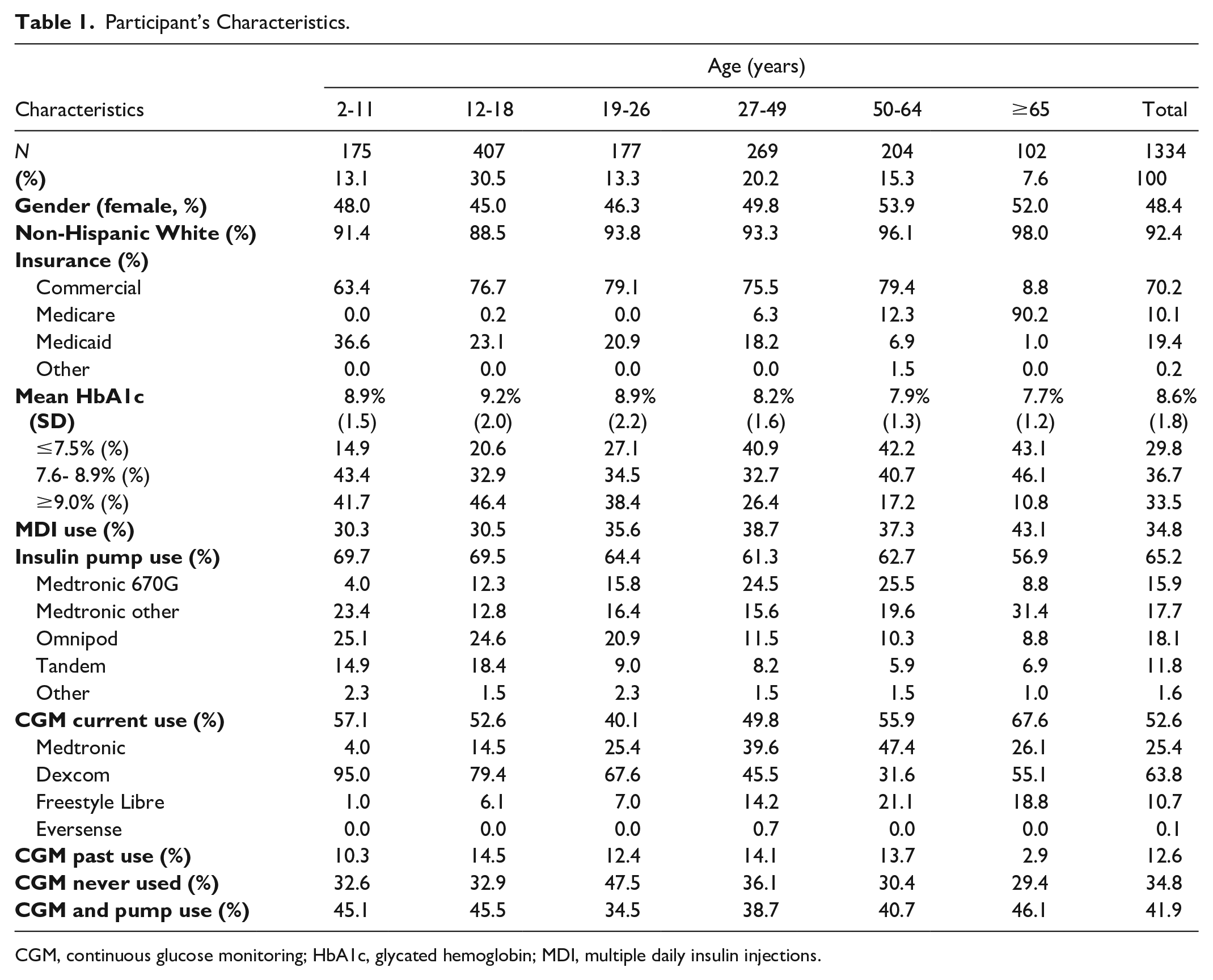
CGM, continuous glucose monitoring; HbA1c, glycated hemoglobin; MDI, multiple daily insulin injections.
The highest mean HbA1c was in the age group 12-18 years (mean HbA1c 9.2%); 44% of participants aged 12-26 years had HbA1c ≥ 9.0%. The lowest mean HbA1c was observed in the older adults (age ≥65 years, mean HbA1c 7.7%). This pattern is consistent with previous reports showing that HbA1c levels are highest in adolescents and emerging adults.15,23 Consistent with previous reports, the mean HbA1c among current CGM users was lower than the mean HbA1c in CGM nonusers, 8.1% and 9.1%, respectively (P < .001); 44.6% of non-CGM users versus 27.2% of real-time (RT)-CGM users and 29.7% of non-RT-CGM users had HbA1c > 9.0%. The mean A1c in those treated with insulin pump therapy was 8.5%, MDI 8.8%, CGM + pump use 8.2%, and in those not using a pump or CGM 9.2% (CGM and pump use vs not using pump or CGM, P < .001).
CGM use was 52.6% among participants overall (DexCom 63.8%, Medtronic 25.4%, Freestyle Libre 10.7%, and Eversense 0.1%). Insulin pump use was 65.2% overall, with 41.9% using both CGM and insulin pump therapy (9.4% of total participants were using the Medtronic 670G pump with Guardian sensor in Automode and 4.6% were using the Tandem T:slim X2 pump/DexCom G6 with Basal IQ).
Perceived Benefits and Burdens of CGM Use in Total Cohort
Perceived benefits and barriers (total mean scores) by age, gender, CGM use, and insulin pump use are shown in Table 2. The response rates for each item in the BurCGM and BenCGM questionnaires were >91%. Non-CGM users as well as individuals using MDI therapy perceive more burdens and less benefits from CGM use compared with participants who were using CGM or insulin pump therapy (P < .001). Among all participants, the most common agreed-upon burdens for non-CGM users (from items in the BurCGM questionnaire) were “CGM is too expensive to wear regularly” (cost), “CGM is painful to wear” (painful), “CGM sensor readings cannot be trusted” (readings not trusted), and “takes too much time to use.”
Perceived Benefits and Perceived Burdens of Using CGM.
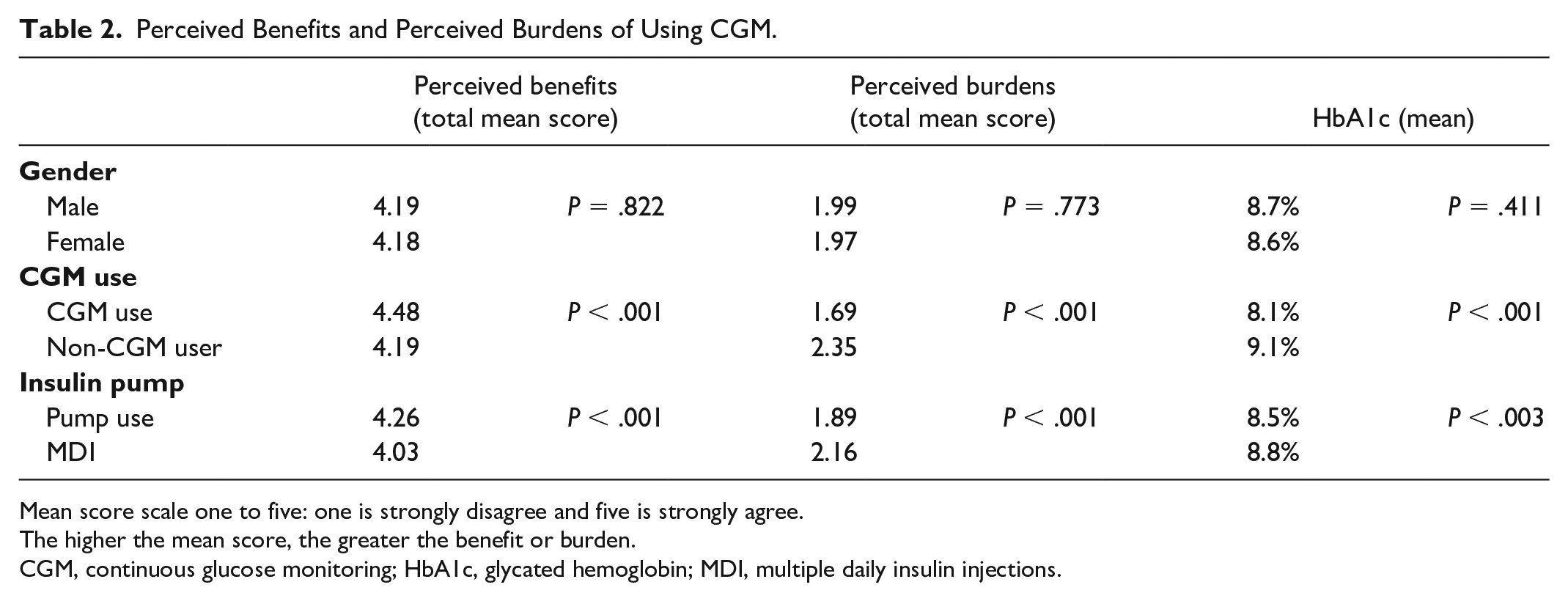
Mean score scale one to five: one is strongly disagree and five is strongly agree.
The higher the mean score, the greater the benefit or burden.
CGM, continuous glucose monitoring; HbA1c, glycated hemoglobin; MDI, multiple daily insulin injections.
Perceived Burdens of CGM in Nonusers
The perceived burdens to CGM use among CGM nonusers across different age groups are shown in Table 3. For individuals not using CGM, the mean BurCGM scores (reflecting higher perceived burden) were higher in older participants (≥50 years of age) compared with those less than 50 years (P = .004). In adults (aged 27+ years), cost was the greatest burden. When asked if CGM is too expensive to wear regularly, only 11.1%, 6.0%, and 11.5% of patients aged 2-11, 12-18, and 19-26, respectively, agreed, whereas 25.2%, 30.3%, and 24.0% of adults aged 27-49, 50-64, and 65+ years, respectively, agreed. In response to the statement, CGM sensor readings cannot be trusted; 19.2 % of those aged 65+ years, 15.4% of those aged 50-64 years, 12.3% of those aged 2-11 and 27-49 years, and 8.4% of those aged 12-26 years agreed. Other concerns included CGM is painful to wear and takes too much time to use (Table 3). Among non-CGM users, 21.4% of participants aged 65+, 11.7% of those aged 50-64 years, and 11.0% of those aged 12-18 years agreed with the statement that “CGM causes too much worry about blood sugars”; less than 10% of those in other age groups agreed with this statement. In those aged 65+, 18.5% agreed with the statement “it is too hard to understand CGM information,” compared with 6.5% in those aged 50-64 and <5% in other age groups.
Burdens of CGM Use by Age in Individuals Not Using CGM: Mean BurCGM Scores.
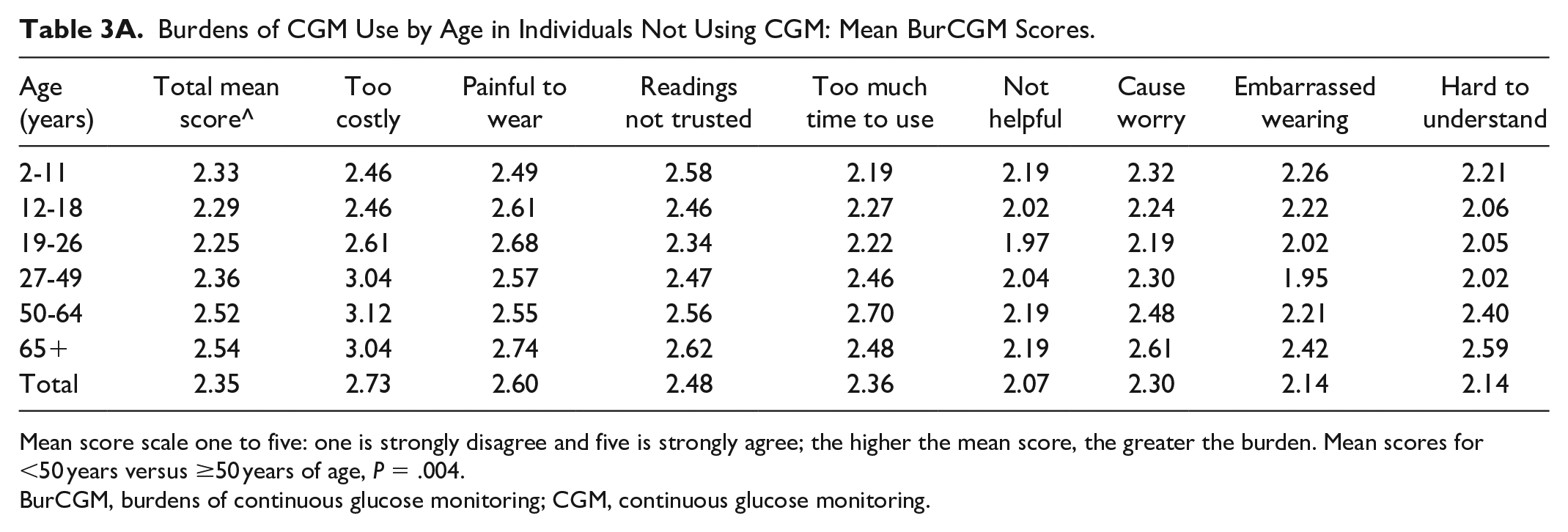
Mean score scale one to five: one is strongly disagree and five is strongly agree; the higher the mean score, the greater the burden. Mean scores for <50 years versus ≥50 years of age, P = .004.
BurCGM, burdens of continuous glucose monitoring; CGM, continuous glucose monitoring.
Burdens of CGM Use by Age in Individuals Not Using CGM: Item Agreement.
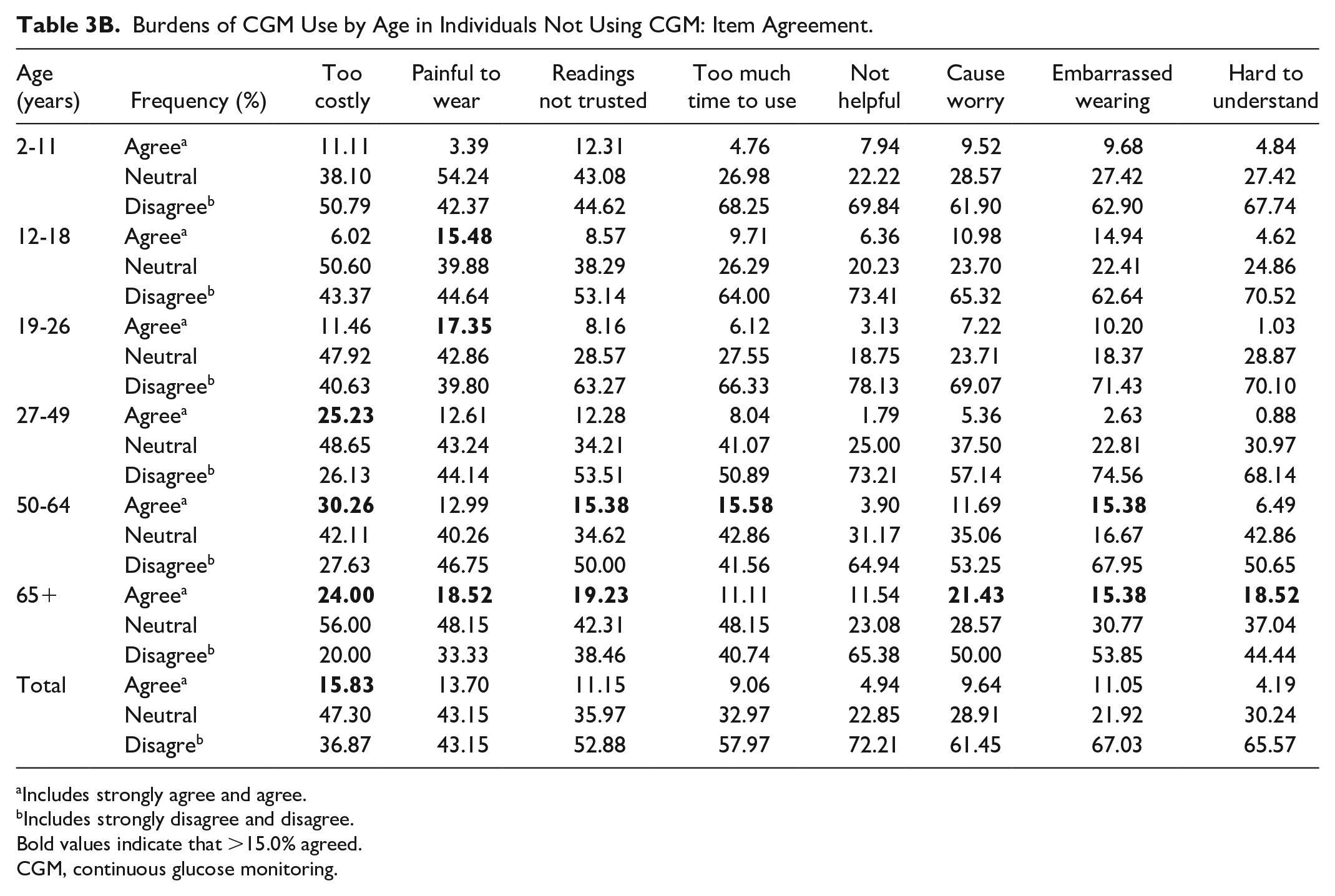
Includes strongly agree and agree.
Includes strongly disagree and disagree.
Bold values indicate that >15.0% agreed.
CGM, continuous glucose monitoring.
Perceived Burdens of CGM in Users
Perceived burdens of CGM use (mean BurCGM scores) among CGM users (Table 4) were lower (less perceived burden) in all age groups (Table 4). Older adults (ages 65+) using CGM had lower mean scores than nonusers, and mean BurCGM scores were higher in those aged 65+ compared with those aged 50-64 years (P = .041). Agreement with the statement “CGM is too expensive to wear regularly” was lower in all age groups except for those aged 2-11 years.
Burdens of CGM Use by Age in Individuals Using CGM: Mean BurCGM Scores.
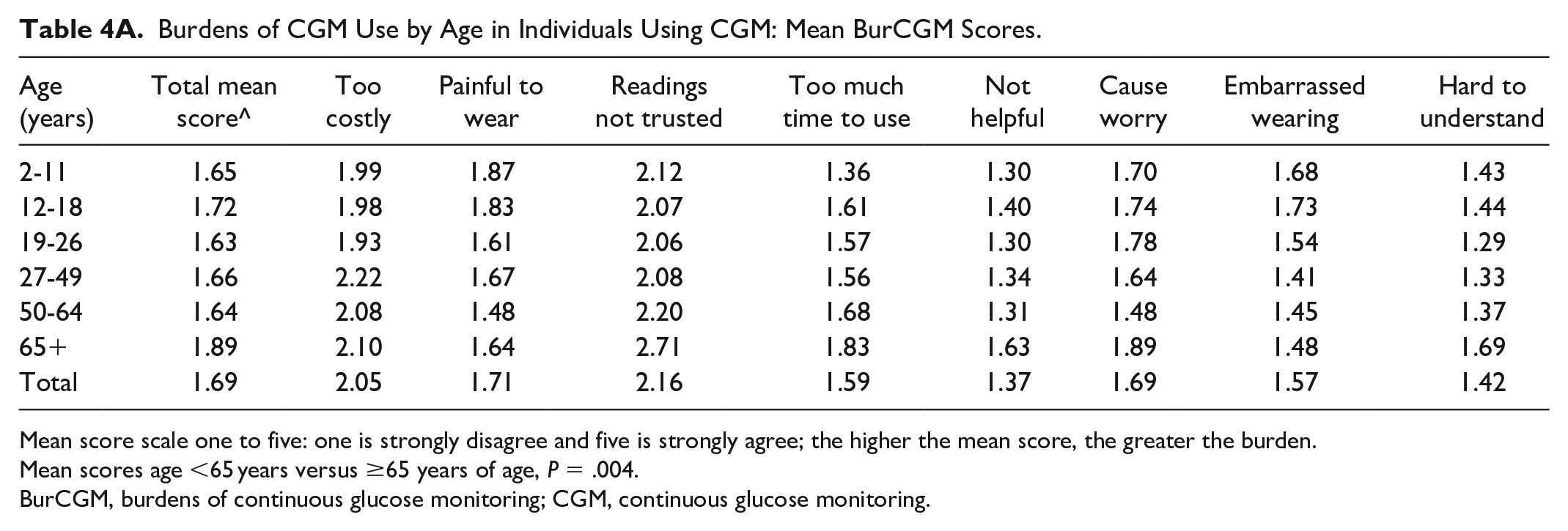
Mean score scale one to five: one is strongly disagree and five is strongly agree; the higher the mean score, the greater the burden.
Mean scores age <65 years versus ≥65 years of age, P = .004.
BurCGM, burdens of continuous glucose monitoring; CGM, continuous glucose monitoring.
Burdens of CGM Use by Age in Individuals Using CGM: Item Agreement.
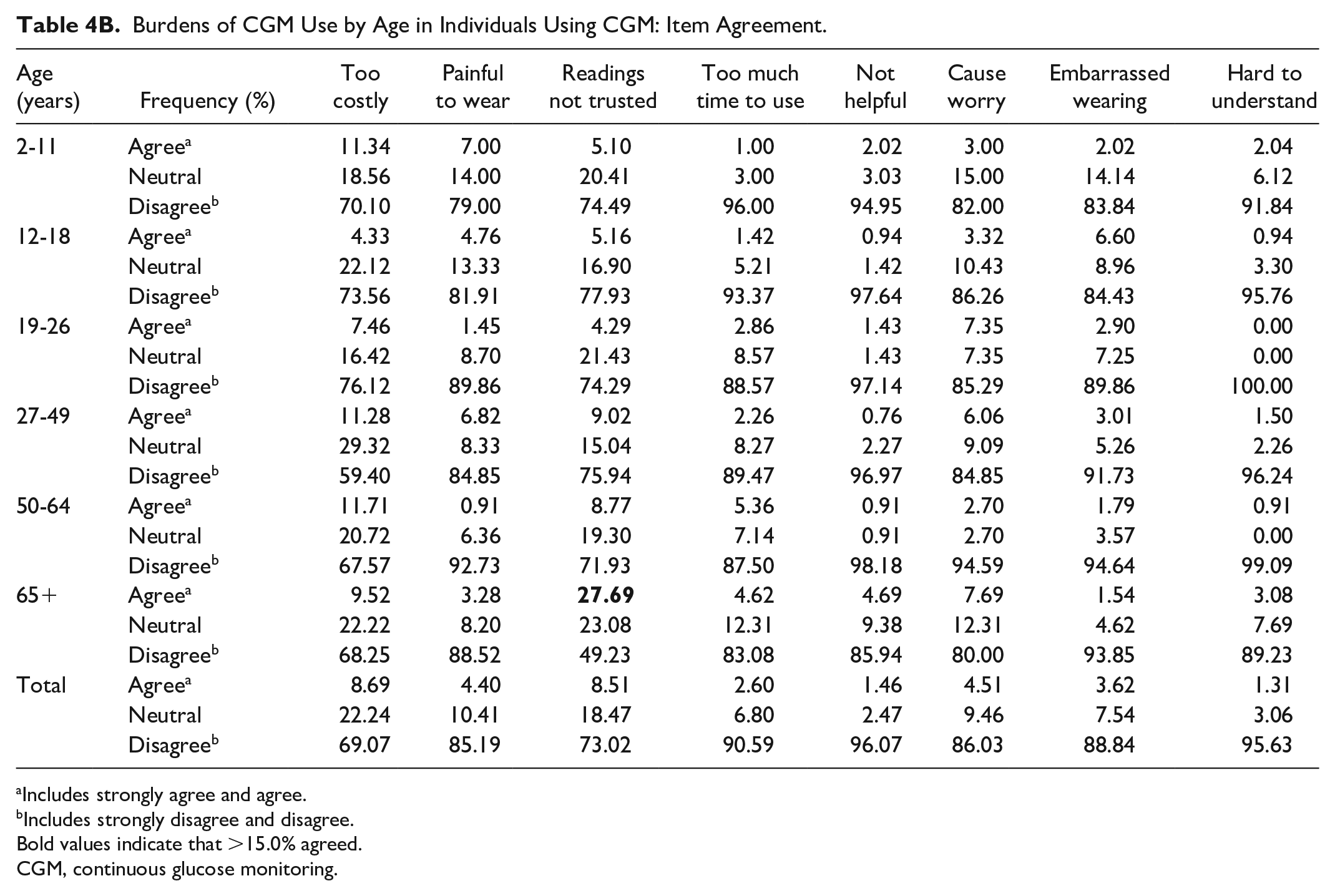
Includes strongly agree and agree.
Includes strongly disagree and disagree.
Bold values indicate that >15.0% agreed.
CGM, continuous glucose monitoring.
Perceived Burdens of CGM in Users Versus Nonusers
There are different (and greater) concerns about costs between CGM users and nonusers ages 27-49, 50-64, and 65+ years. Agreement with the statement “CGM sensor readings cannot be trusted” was less in CGM users versus nonusers except in those aged 65+ where 27.7% of users versus 19.2% of nonusers agreed with this statement. Compared with the 18.5% of non-CGM using adults ages 65+ who agreed with the statement “I think it is too hard to understand CGM information,” only 3.1% of CGM users in this age group agreed with this statement.
Perceived Benefits of CGM in Nonusers and Users
Tables 5 and 6 show the perceived benefits (BenCGM survey results) for individuals not using versus using CGM, respectively, across different age groups. The mean BenCGM scores are higher in CGM users in every age group (reflecting higher perceived benefit). Non-CGM users aged <50 years rated CGM benefits higher than those ≥50 years (P = .033); users aged <50 years also rated benefits higher than those who were older (P < .001). For users aged 2-11, the mean score is the highest and significantly different from those aged 27-49 years (P = .007), 50-64 years (P < .001), and 65+ (P = .002).
Benefits of CG Use by Age in Individuals Not Using CGM: Mean BenCGM Scores.
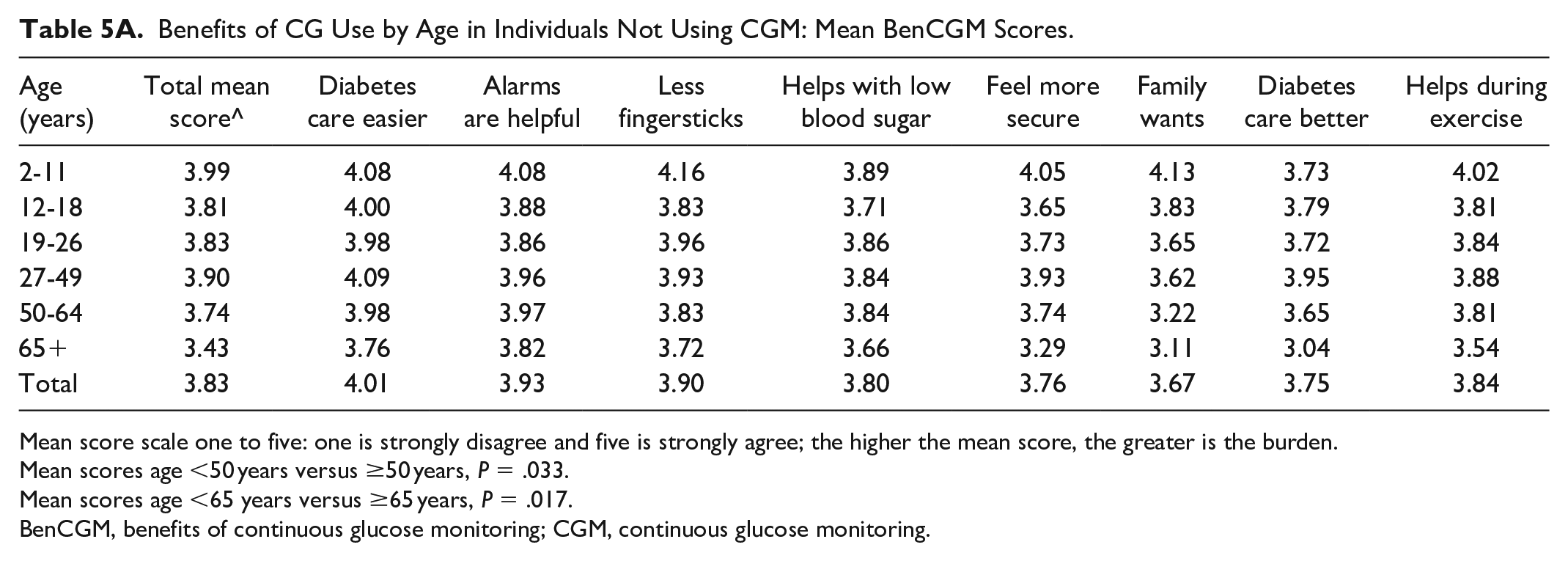
Mean score scale one to five: one is strongly disagree and five is strongly agree; the higher the mean score, the greater is the burden.
Mean scores age <50 years versus ≥50 years, P = .033.
Mean scores age <65 years versus ≥65 years, P = .017.
BenCGM, benefits of continuous glucose monitoring; CGM, continuous glucose monitoring.
Benefits of CGM Use by Age in Individuals Not Using CGM: Item Agreement.
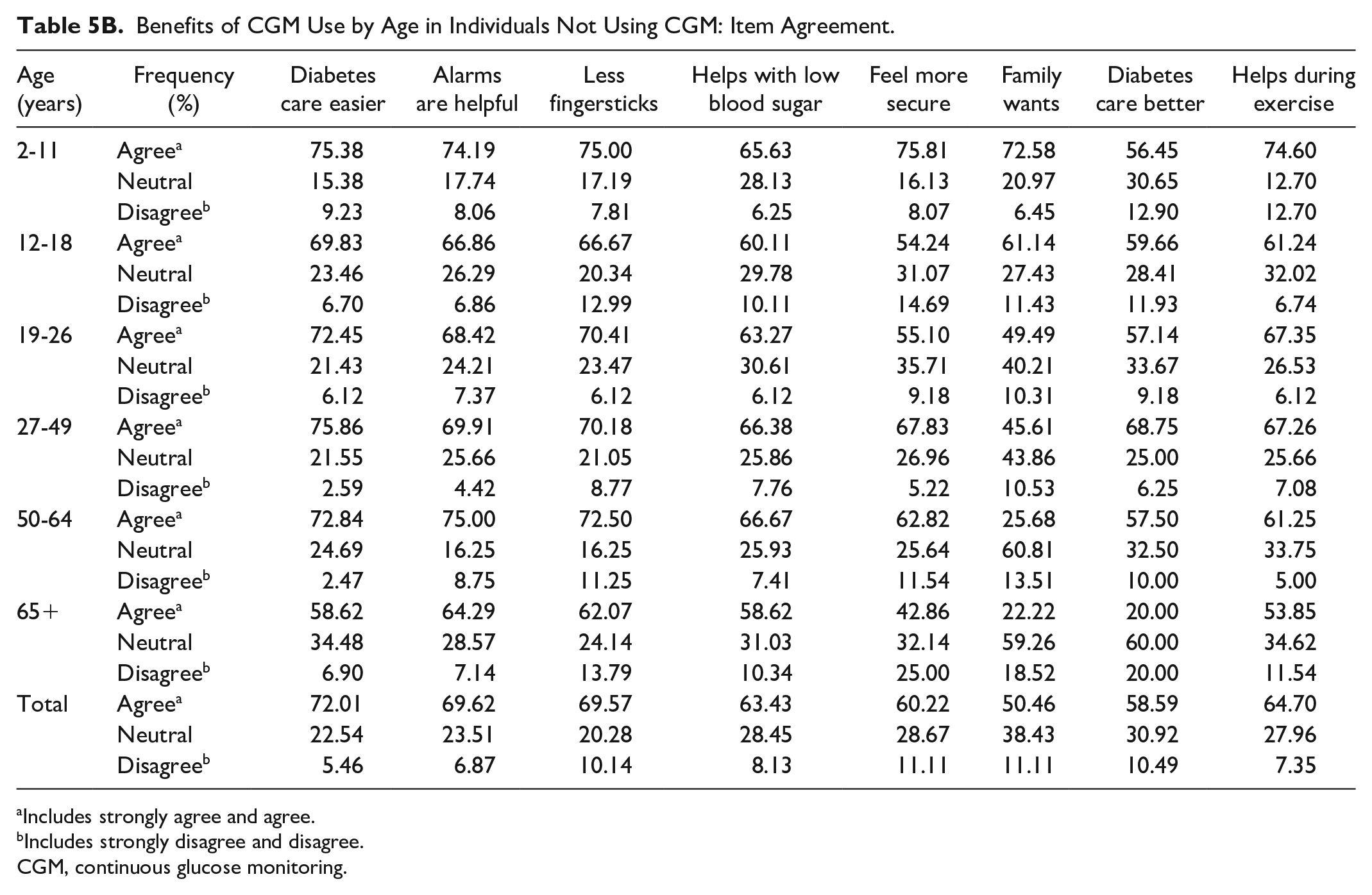
Includes strongly agree and agree.
Includes strongly disagree and disagree.
CGM, continuous glucose monitoring.
Specific CGM nonuser and CGM user perceived benefits across different age groups are shown in Tables 5 and 6. Over 80% of users in all age groups agree with the statements “CGM makes taking care of diabetes easier,” “CGM makes me feel more secure,” “I take better care of my diabetes with a CGM,” and “CGM helps take care of low blood sugars.” In those aged 65+ years, nonusers versus users, respectively, 58.6% versus 92.7% agree that “CGM makes taking care of diabetes easier,” 42.9% versus 94.1% agree that “CGM makes me feel more secure,” 20% versus 89.2% agree that “I take better care of my diabetes with a CGM,” and 58.6% versus 86.8% agree that “CGM helps take care of low blood sugars.”
Benefits of CGM Use by Age in Individuals Using CGM: Mean BenCGM Scores.
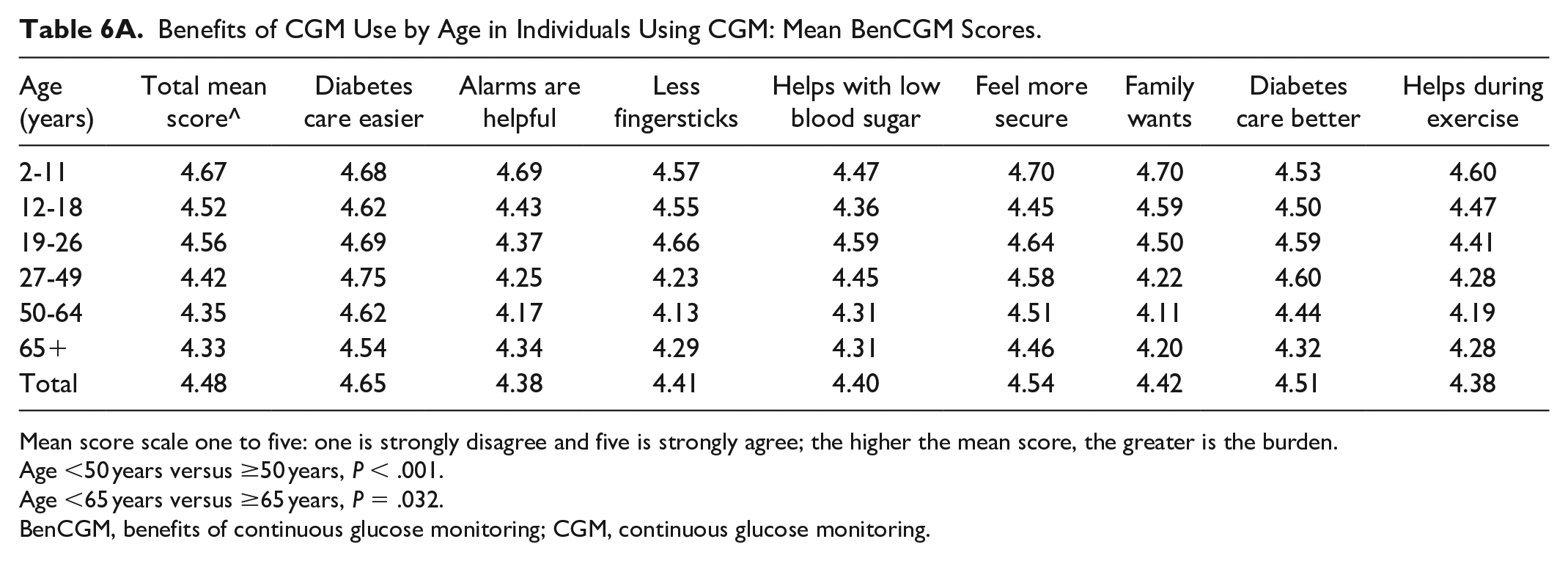
Mean score scale one to five: one is strongly disagree and five is strongly agree; the higher the mean score, the greater is the burden.
Age <50 years versus ≥50 years, P < .001.
Age <65 years versus ≥65 years, P = .032.
BenCGM, benefits of continuous glucose monitoring; CGM, continuous glucose monitoring.
Benefits of CGM Use by Age in Individuals Using CGM: Item Agreement.
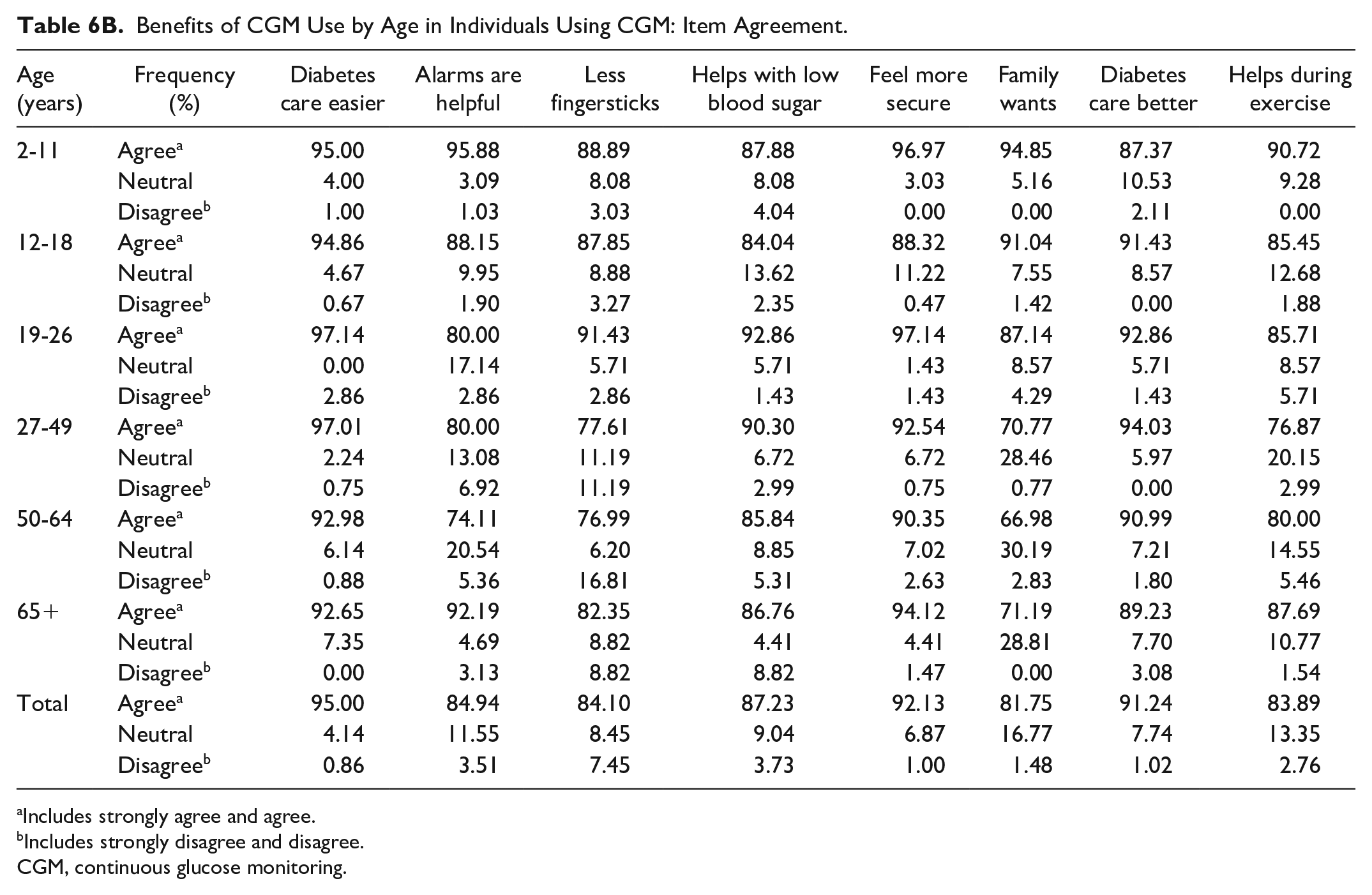
Includes strongly agree and agree.
Includes strongly disagree and disagree.
CGM, continuous glucose monitoring.
Discussion
Understanding barriers for CGM use in people with type 1 diabetes at different stages of life is crucial so that appropriate interventions can be developed. We report important differences across the lifespan as well as common concerns. Addressing these concerns should increase CGM utilization, thereby improving glycemic profiles and quality of life.
Cost was perceived as one of the top burdens among all age groups not using CGM, especially in adults aged 27 and older, where 24.0%-30.3% of nonusers agreed with the statement that “CGM is too expensive to wear regularly.” The policies of Medicare and other insurers have been changing, but continued advocacy is needed to further lower the cost and improve insurance coverage of CGM to increase regular access to CGM.
CGM use has been reported to be low amongst adolescents, despite the fact that use of CGM alone or in combination with the use of an insulin pump has been associated with less adolescent perceived diabetes distress and lower HbA1c.2,24,25 We found that “CGM is painful to wear” was perceived as the greatest burden in CGM nonusers ages 12-26 years. This can be addressed with education.
Our study provides data on adults aged 65+ years with type 1 diabetes, a group that is less studied than other age groups. In this age group, cost was the greatest burden for both CGM users and nonusers. An important finding was the large differences in CGM users versus nonuser responses concerning “worry about blood sugars” and “it is too hard to understand CGM information.” The relatively small number of participants in this age group precluded further subgroup analyses (eg, by education and socioeconomic status). Nevertheless, anecdotally, older adults require more time to train to use CGM and to learn to interpret CGM data, compared with younger people with type 1 diabetes. However, given sufficient time, attention, and education, most older adults can use CGM, and CGM use in this age group is associated with a reduction in hypoglycemia, a major concern in older adults. 5 Our results suggest that older adults, compared with younger people with diabetes, will need more education and support to help them understand CGM information and reduce their worry.
In our study, insulin pump users (vs injection users) had higher BenCGM scores and lower BurCGM scores, perhaps reflecting their relative comfort with or attitude toward the use of technology for diabetes self-management. As more individuals use hybrid closed-loop systems, it is anticipated that greater benefits will be perceived, and more use of CGM will ensue.
The inclusion of 1334 individuals aged two years to 95 years in a real-world setting is the strength of this study. The questionnaires used to assess the benefits and burdens of CGM use were validated in adolescents. 22 Since we use these measures in other age groups as well, we felt it is important to report not only the means scores but also the responses to the individual questions.
Limitations of this report include the following: this study was performed in a single center; most participants were non-Hispanic white, and there were a limited number of adult participants in each age group, with only 102 participants in the 65+ year age group. We were unable to compare the difference between BenCGM and BurCGM scores within age groups by race/ethnicity, insurance types, and CGM type, given the “n” and the unequal distribution of participants among subgroups. We were also unable to track the number of individuals who refused to complete the questionnaires. Lastly, surveys were completed from February 2019 to February 2020 (pre-COVID); results may be different now.
Conclusion
Perceived burdens and benefits of CGM use can vary in individuals with type 1 diabetes across the lifespan. Advocacy for making CGM more affordable, as well as interventions targeted to address specific barriers or burdens are needed to increase CGM use, with the goal of improving glycemic profiles as well as the quality of life.
Footnotes
Abbreviations
BenCGM, Benefits of continuous glucose monitoring; BurCGM, Burdens of continuous glucose monitoring; CGM, continuous glucose monitor; HbA1c, hemoglobin A1c; MDI, multiple daily insulin injections; RT-CGM, real-time continuous glucose monitor; T1D, type 1 diabetes.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: RSW participates in diabetes multicenter clinical trials, through her institution, sponsored by Medtronic, Eli Lilly, Kowa, Tolerion, Insulet, and Boehringer Mannheim. All other authors have no disclosures.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was funded in part by the Leona M and Harry B Helmsley Charitable Trust with support from the T1D Exchange Quality Improvement Collaborative and SUNY Upstate Medical University.