
Abstract

Dear Editor,
Poor adherence in adolescents with type 1 diabetes mellitus (T1DM) is a well-known phenomenon, occurring in a significant percentage of patients. While adherence promotion interventions in these patients showed substantially small or no improvement in the intervention groups, innovative approaches based on the use of technology have been proposed. However, a “challenging paradox” has been reported for hybrid closed loop (HCL) systems: 1 while young patients with higher A1C would benefit the most from this system, 2 they are precisely those with the highest probabilities of discontinuation (30% of youth interrupted HCL in the first six months of use); 3 therefore, HCL is not recommended in these cases. 1
In our current practice, we have 13 adolescents using the HCL system so far: the HCL system is proposed not only to individuals already on insulin pumps who want to improve their glycemic control but also to adolescent on basal bolus who struggle to have reasonable control. They all show a good metabolic control (glucose management indicator [GMI] 7%, time in range [TIR] around 70%), with the most extended follow-up of 20 months and no drop-out so far. 4
In particular, we had two adolescent girls (16 and 13.5 years), naïve to insulin pumps, with poorly controlled T1DM (A1c 10.8% and 10.3%, respectively) due to non-adherence to treatment which impressively, promptly, and durably benefited from the use of the HCL system together with personalized coaching, which included a therapeutic contract (Figure 1).
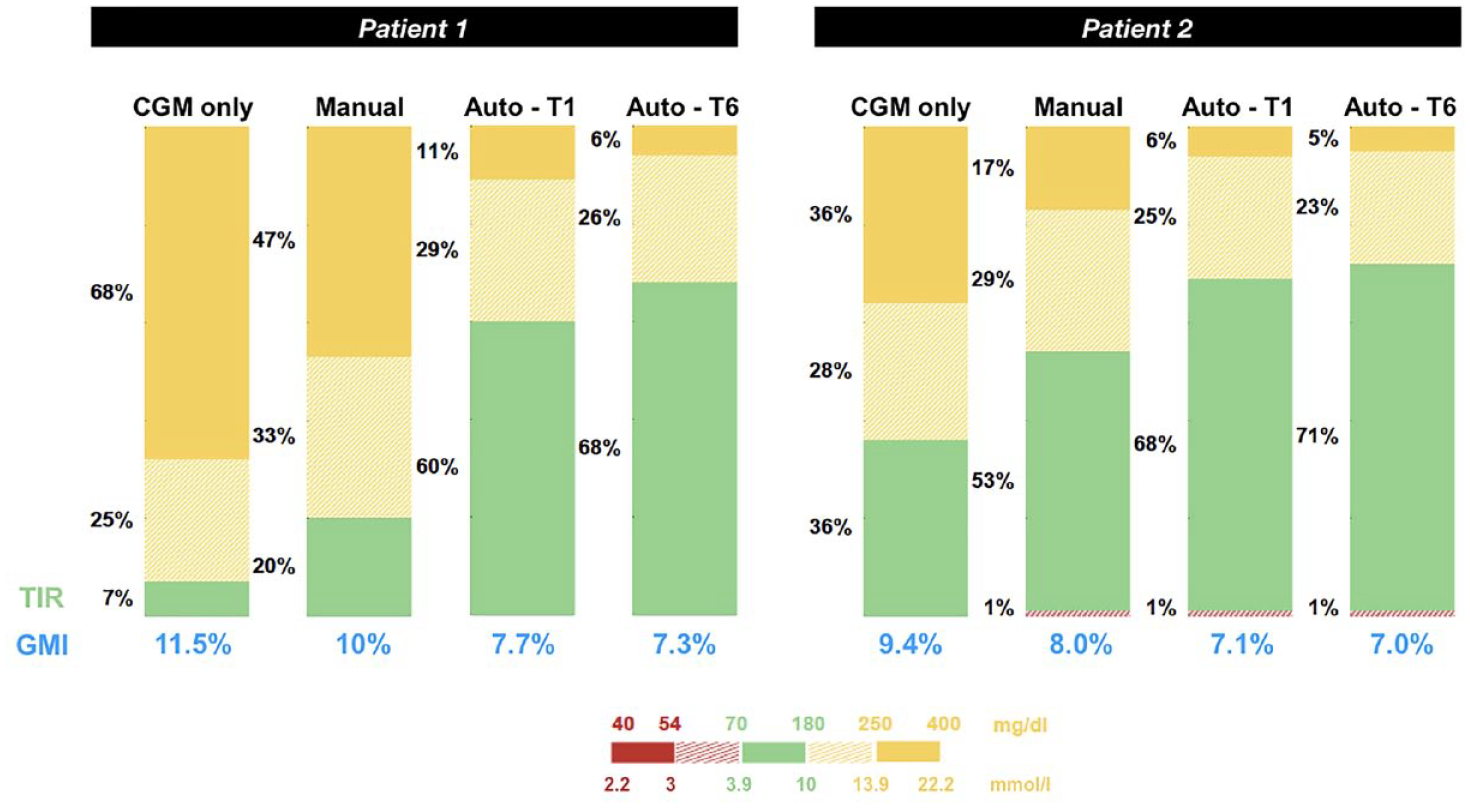
Progression of time in range (TIR) and glucose management indicator (GMI) in two adolescents from CareLink™ reports during continuous glucose monitoring (CGM) only, HCL in manual mode, after one month of HCL in auto mode (Auto-T1), after six months of HCL in auto mode (Auto-T6).
The therapeutic contract is a typical approach in our practice: it is usually signed—at the end of the individual, step-by-step personalized training—by every adolescent who decides to use an HCL system, and it has three mandatory commitments:
(1) to wear the sensor for at least 90% of the time and avoid prolonged periods without CGM and Auto Mode;
(2) to bolus for every meal (snacks included) 10-15 minutes before eating, carefully calculating carbohydrates (CHO);
(3) to download data every two weeks and share results with health care professionals and a brief report of positive and negative results.
Other targets and commitments are negotiated case by case, based on each individual’s weakness detected during the training.
According to our experience, these main tasks lead to the proper use of the system and its beneficial effect. When HCL is used correctly, adolescents perceive a prompt return to their efforts with a better quality of life and a reduction in the mental burden of diabetes that responded to the “concrete thinking” they still have while moving into the adult cognitive capacity, hence creating a virtuous circle.5,6
We therefore suggest that a starting point of poor glycemic control and adherence should not necessarily contraindicate HCL and that HCL systems should not only be reserved for better-controlled patients who wish to improve their glycemic control, but can also be very useful in adolescents with feeble adherence and very poor glycemic control, naïve to insulin pumps, in the context of a personalized coaching and a clear therapeutic contract.
Footnotes
Acknowledgements
The authors thank Martina Bradaschia for the English revision of the manuscript.
Declaration of Conflicting Interests
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.