
Abstract
Insulin bolus calculators have proven effective in improving glycemia and patient safety. Insulin calculators are increasingly being implemented for inpatient hospital care. Multidisciplinary teams are often involved in the design and review of the efficacy and utilization for these calculators. At times, unintended consequences and benefits of utilization are found on review. Integration of our insulin calculator into our electronic health record system was a multidisciplinary effort. During implementation, several obstacles to effective care were identified and are discussed in the following manuscript. We describe the barriers to utilization and potential pitfalls in clinical integration. We further describe benefits in patient education, time of insulin administration versus meal delivery, variations in insulin bolus for ketone correction, variation in care, and maximum bolus administration. Sharing lessons learned from experiences using electronic insulin calculator order sets will further our goals of improved patient care in the hospital setting.
Introduction
The Health Information Technology for Economic and Clinical Health Act was enacted in 2009 paving the way for electronic health records (EHR) and computer provider order entries for medication orders. 1 The development of digital glycemic management protocols has potential to bypass the tedious and inefficient method of hierarchical notification through patient, nurse, resident, fellow, and attending, and can bypass individual human calculation errors. We have previously described the build, satisfaction measures, and evolution of our insulin order set housed within our EPIC EHR. 2 Utilization and satisfaction of computer provider order entry of an insulin bolus calculator was assessed in our home institution with general positive regard. 2 However, the development of the calculator requires time and coordination between physicians, nursing, dietary professionals, pharmacy, and EHR staff. 3 The investment of EHR-based insulin order entries has demonstrated positive outcomes for the admitted patient with hyperglycemia, including a decrease in mean glucose concentration, improved time until dose administration, and provider and patient satisfaction.2,4
Our multidisciplinary team worked closely together as our insulin order set developed. 2 With any novel implementation there have been unforeseen consequences that can lead to different strategies of care, near misses, and medication errors that have been opportunities to refine our process. We aim to describe these opportunities for improvement and reflect on strategies for refinement.
Results
Time vs Mealtime Programming
The original insulin dose calculator was built with the carbohydrate coverage factor dependent on the “Meal/Time” selected while the correction factor was dependent upon the actual time of day. Daytime hours were defined as 6
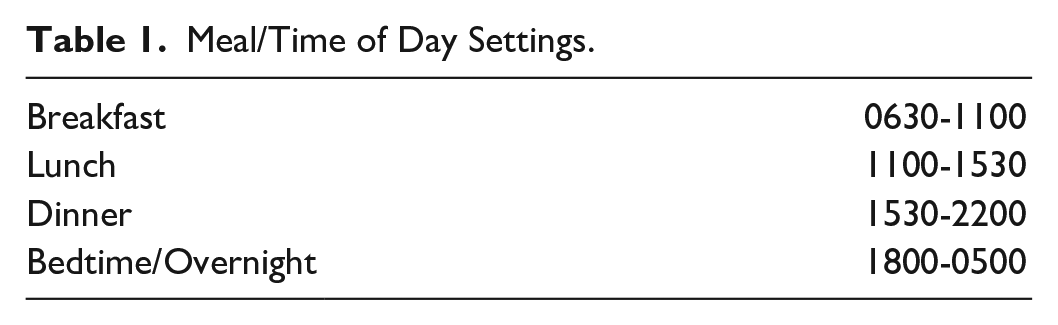
Therefore, a change was implemented in the insulin dose calculator to base the correction factor on “Meal/Time of Day” selected. The AM correction factor was linked to breakfast, lunch, and dinner; the PM correction factor was linked to bedtime/overnight. Due to the dosing of the insulin now completely dependent upon the nurse’s appropriate selection of the “Meal/Time of Day,” a safety check alert was put into place within the calculator. The line under the “Meal/Time of Day” was edited to include “Meal/Time of Day selected match actual time?” (Figures 1 and 2). Background parameters were put into place for the times associated with each dosing button (Table 1: Meal/Time of Day). If the nurse selects the “Meal/Time of Day” within the safety parameter timing, this line displays “Yes” (Figure 1). If the nurse selects the “Meal/Time of Day” outside of the specified safety parameter, this line would display “**WARNING** Check timing” (Figure 2).
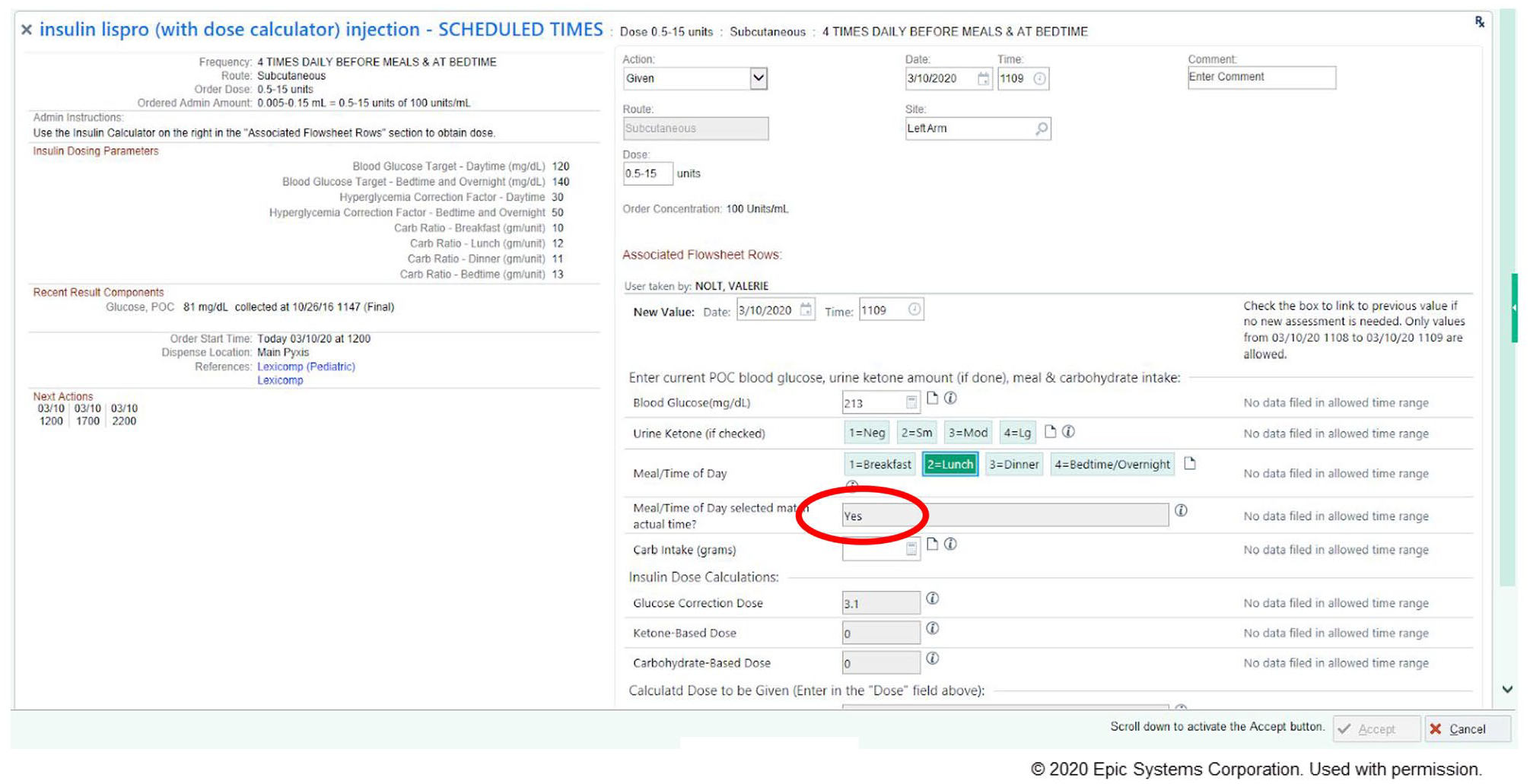
Mealtime insulin calculator screenshot.
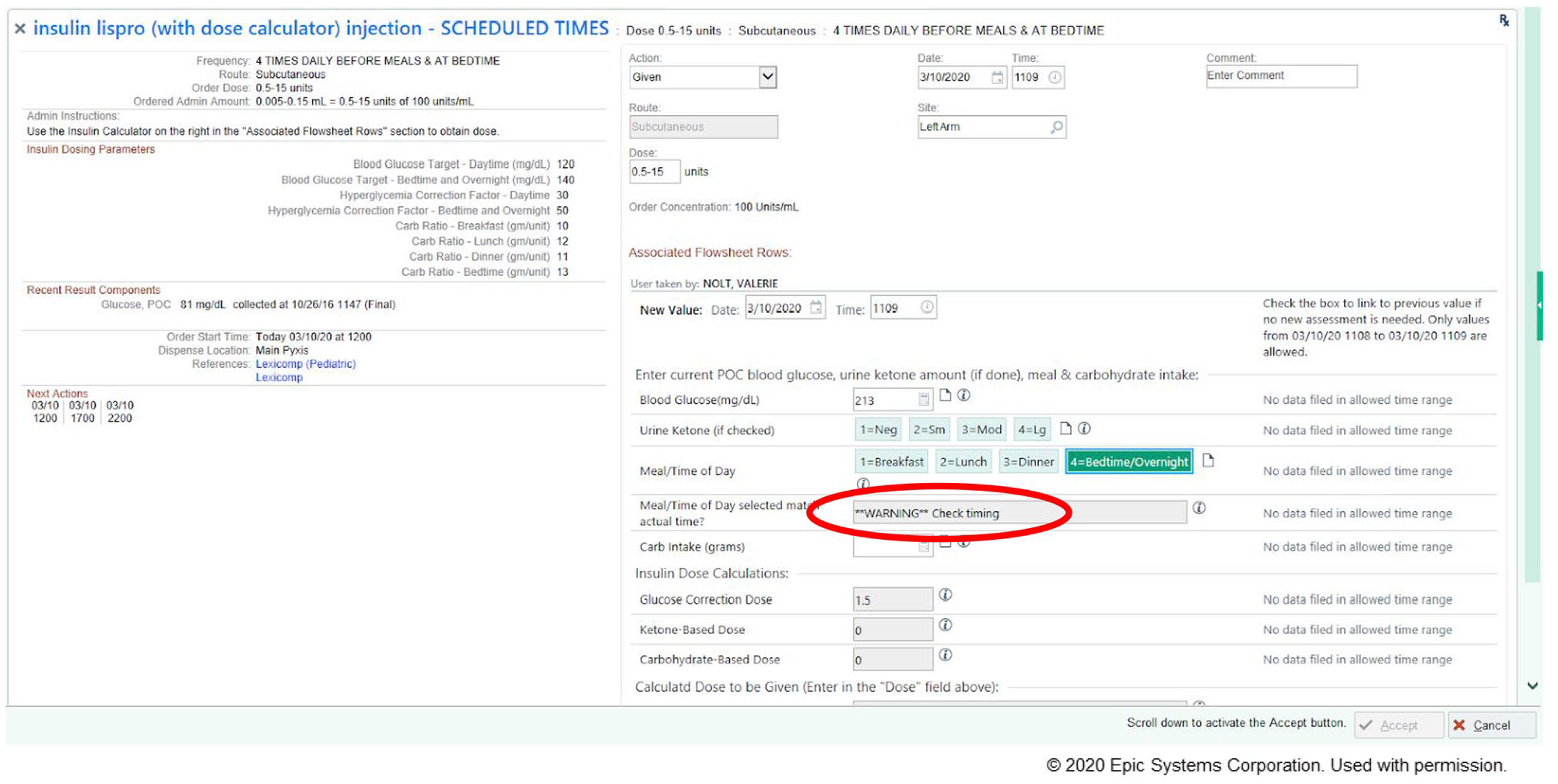
Mealtime warning insulin calculator screenshot.
Meal/Time of Day Settings.
For example, if a nurse was charting a dose of insulin at 7
Safety: Maximum Dosing Issues
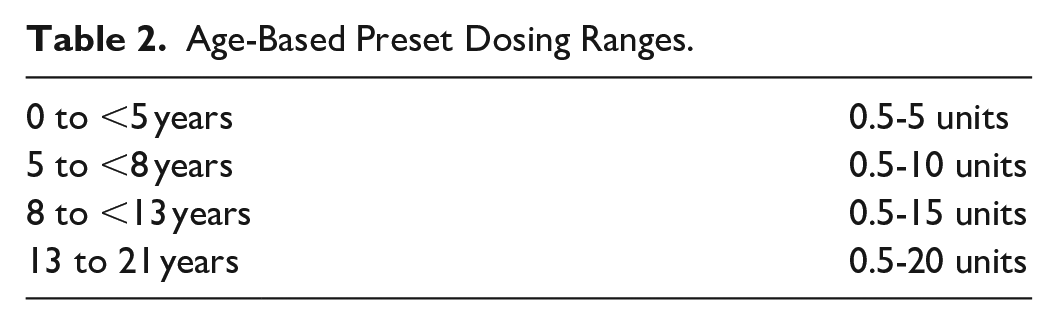
Along with timing, dosing of insulin is a major safety concern, and frequent review of events has allowed us to revise the order set based on safety reports submitted by hospital staff members. Our institution experienced a near-miss safety event regarding a one-time order of insulin lispro for a pediatric patient in our children’s emergency department with an inadvertently high dose. In response to this event, we edited our insulin lispro dose alert thresholds to be more stringent to prevent a similar error from occurring in the future. When implementing this change, it required disabling the dose alert thresholds used for standard insulin lispro orders from applying to the insulin dose calculator due to the range of 0-20 units flagging an alert on every insulin dose calculator order entered. Preset dosing ranges were created based on age to prepopulate on order entry (Table 2, Figure 3). Modification of the preset dosing range can be done on order entry by the ordering provider. If the calculated dose result during administration is greater than the maximum default dose or customized dose entered by the provider, a warning message displays (Figure 4) requiring the nurse to contact the provider or provide override rationale (Figure 5).
Age-Based Preset Dosing Ranges.
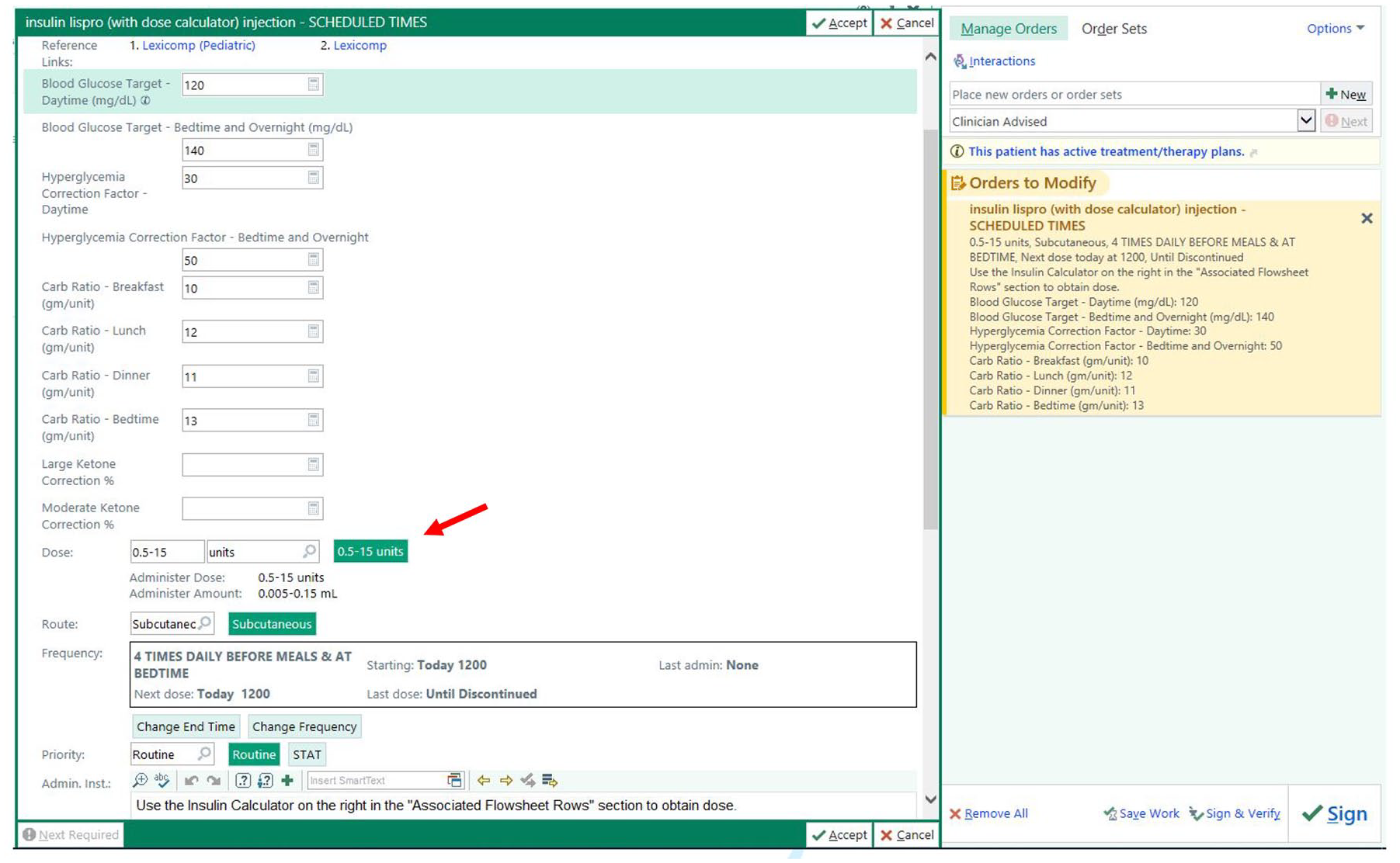
Dosing ranges for insulin calculator.
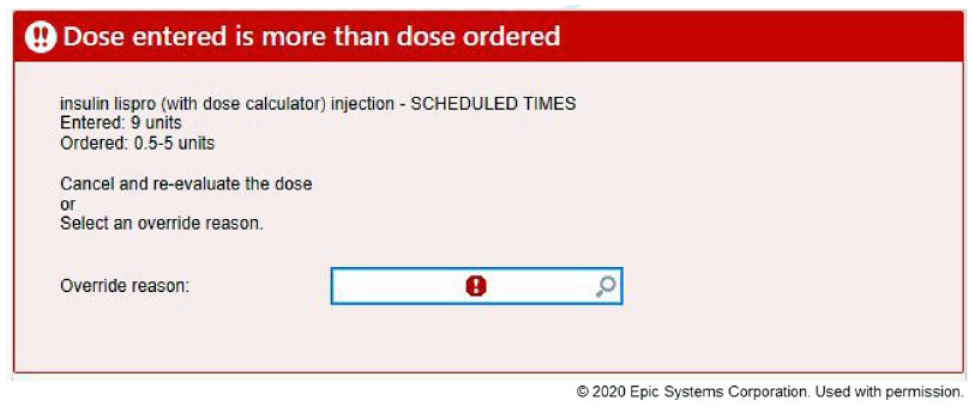
Dosing outside of range warning.
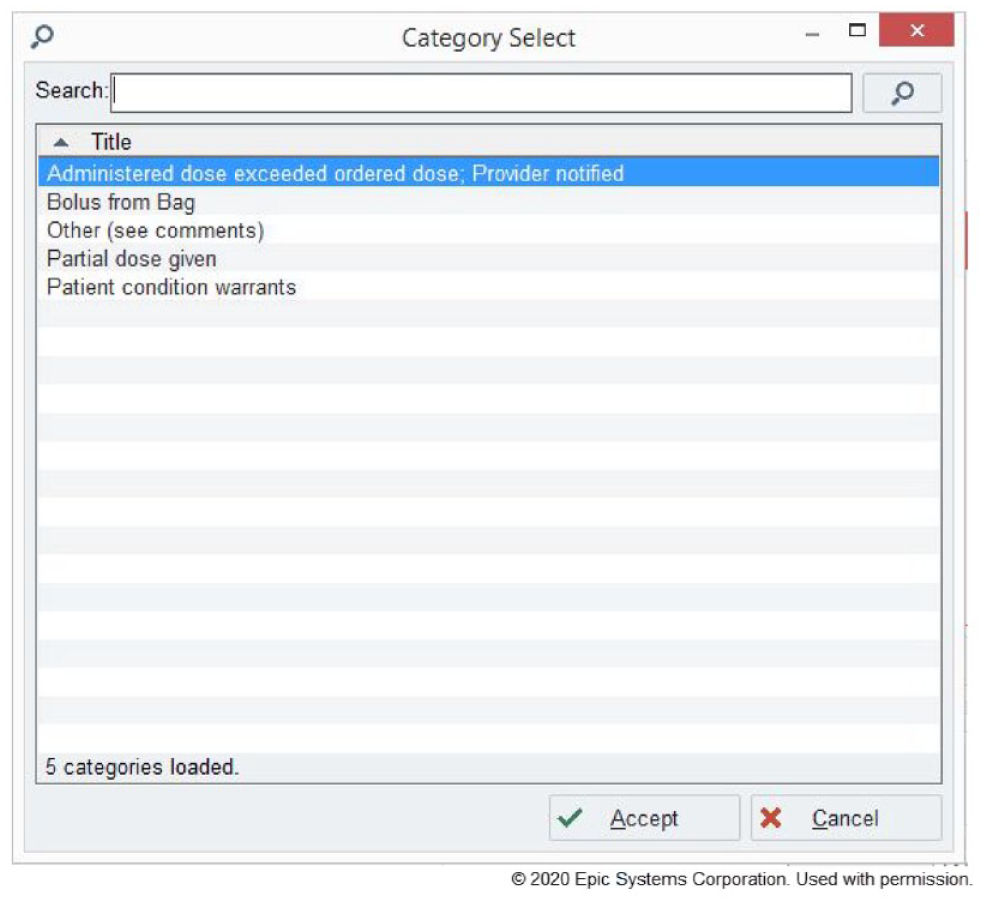
Insulin warning override.
The lower dosing limit of 0.5 units was selected for all age ranges for two reasons. First, 0.5 units is the lowest measurable dose using the institution’s half-unit insulin syringes. 5 Second, our institution recently implemented a new automated dispensing cabinet. 6 The automated dispensing cabinet does not recognize a dose of “0” for any product. Therefore, for the order to cross over from our EHR (EPIC) to the automated dispensing cabinet we had to create a dosing range that did not include “0” as a possible dose.
Dose Calculation: Glucose Value Double-Check by EHR
Some of the findings from our shared discussions are areas we are currently working on for future modifications to the workflow. For example, another complexity of the dose calculator is the reliance on accurate data entry. The patient’s insulin dose is calculated based on information that is entered by nursing staff. An error was reported in which a nurse entered into the calculator the glucose value from the morning comprehensive metabolic panel in lieu of the intended glucose value from the point-of-care glucose test performed prior to the afternoon meal. The difference in glucose values resulted in the patient receiving an additional 1.5 units of insulin lispro and the patient subsequently experienced a hypoglycemic episode that was managed with oral glucose intake. Although a minor incident, in response to this medication error, a safety double-check is being explored where the EHR would compare the most recent point-of-care glucose value with the glucose value entered into the calculator by the nurse to ensure there is no discrepancy. If these values do not match, the nurse would be alerted of the difference and would be able to rectify the problem. We are hoping to implement this double-check system rather than have the EHR pull in the value automatically as there is no precedence whereby the EHR would autonomously calculate a dose. Additionally, this emphasizes that the nurse should still be actively engaged in determining the dose of insulin to be administered. While serum glucose values are more accurate than point-of-care glucoses, our institution is not capable of rapid resolution of glucose in metabolic panels to effectively dose insulin without having significant time elapsed. It was essential to determine that the point-of-care glucose value is rapidly transmitted from the testing device to the EHR system in order to prevent delay of care. We look forward to being able to make such a process in the near future.
Pyxis Issues: One Vial for One Patient
An issue that may impact any hospital system is the specific guidance from the Centers for Disease Control and Prevention regarding multidose vials, defined as a vial of liquid medication intended for parenteral administration (injection or infusion) that contains more than one dose of medication. 7 Recommendations state that a multidose vial should be assigned to a single patient whenever possible, especially when used within immediate patient treatment areas such as a patient room. Nursing staff teaches the patients and families in the room and tries to provide as much real-time interactive education as possible from admission to discharge. Nurses need access to be able to calculate, draw up the insulin, and administer at bedside with caregivers and the patient to ensure hands-on demonstration and comprehension. The workflow necessitated by the insulin dose calculator requires the nurse to scan the insulin lispro vial, enter the dosing information (point-of-care glucose result, most recent urine ketone result [if applicable], amount of carbohydrate to be consumed, and the meal/time of day), and prepare the insulin dose at bedside. This is followed by a visual double-check from a secondary nurse on the dose drawn up prior to dose administration. As this process is completed at the patient’s bedside, in an immediate patient treatment area, it required an institutional shift to assign patient-specific insulin lispro vials and the creation of a specific workflow visual plan (Supplemental material).
Ketone Correction Issues
One question that often comes up in the clinical setting is that of insulin management during illness. Illness can be complicated by counter-regulatory hormones released in response to stress leading to insulin resistance. Hyperglycemia can develop and is typically less responsive to the corrective bolus insulin doses. Higher doses of corrective bolus insulin are commonly recommended in the presence of ketones. 8 Due to individual physicians’ experiences and the variation in the severity of the child’s sickness, there is a wide range of opinions on the additional correction doses for the different levels of ketosis. For example, the recommended additional correction doses for the presence of large ketones among the North American medical centers range from as low as 0%-20% to as high as 100% on top of the calculated routine corrective bolus insulin doses. 9 Some organizations advise patients to give 10%-20% of the total daily dose of insulin (or 0.1 unit/kg) as rapid-acting insulin in the presence of moderate or large ketones. 9 This variation in protocols exists even among the physicians/nurses in the same hospital/group.
While this order set is not intended for patients in diabetic ketoacidosis, it can be used for those patients still resolving their ketones and closed anion gap. We believe that the addition of a ketone correction factor in the algorithm of the insulin calculator is necessary and provides better and safer management of sick patients with diabetes and ketones. The managing team can easily choose the additional correction doses from 0% to 100% as a percentage of calculated correction depending on how sick the patient is. Overall, we found in reviewing data for the last year that this option was used about 15% of the time in encounters where the diabetes calculator was ordered, and doses typically ranged from 10% to 50% based on moderate or large ketones. Unfortunately, we are unable to easily identify how many patients using the order set had ketones, which would be a better way to evaluate the frequency of use of the ketone correction order option.
Unintended Benefits of Calculator Screens in Education
A continued problem encountered with the insulin dose calculator is only having the ability to round doses to either the nearest half unit or the nearest whole unit. In order to have the most accurate dosing during inpatient admissions and critical illness, our institution’s insulin dose calculator is currently set to round to the nearest half unit for all patients. This does sometimes cause difficulty when utilizing the insulin dose calculator for patient and family education as patients may use half units during admission but may be sent home on whole unit dosing due to insurance coverage of only whole unit insulin needles or whole unit insulin pen products. This also causes confusion regarding how to account for this discrepancy while teaching the patient and caregivers at the bedside. For instance, if the patient has a half dose for Lantus in the evening and is prescribed a whole unit dose pen for home, this significantly affects teaching and identifies a potential for error. In an ideal state, the insulin dose calculator would be able to round to the half unit for patients less than 10 years and to the whole unit for patients greater than or equal to 10 years, based on the typical age in which patients are switched from half unit to whole unit dosing at our institution or have flexibility to choose the rounding based on discharge medication plan.
Discussion/Future Directions
The creation of the insulin dose calculator order set has facilitated ordering insulin within the hospital setting with an increase in provider and patient satisfaction but with unintended aforementioned consequences as we have described. Our patients’ lives and behaviors vary from their home environment when they are admitted to the hospital and the schedule of activities that occur in the hospital setting. Whether they are an adolescent who prefers to stay up late and snack during the night, inversion of sleep–wake cycle in prolonged hospitalization, underlying pathology influencing mealtime patterns, or observance of sociocultural influences, no two patients are alike. When utilizing this inpatient regimen and continuing this as an outpatient, our artificial timing of meals and day versus night is adjusted based on individual patient interpretation. While admitted, however, it is safest to have standardized definition of day and night, with associated double-check of insulin correction and carbohydrate ratios, to prevent iatrogenic hypoglycemia or hyperglycemia by overdosing or underdosing insulin.
To further add to variable patient experience is the utilization of ketone correction. Currently, at our institution, we are not utilizing beta hydroxybutyrate as a means of assessing resolving ketonemia and are relying solely on urine ketones. This test requires conversion of beta hydroxybutyrate to acetoacetate and can thus shift during the course of treatment as more beta hydroxybutyrate is converted to acetoacetate. 10 The definitive treatment for ketone suppression is insulin administration, and with variable ketone correction utilization among providers, this can impact patient stay. Variable utilization of ketone correction is likely due to patient insulin sensitivity based on age and presenting symptoms as well as hospital course.
Major limitations to our current efforts has been the lack of data collection on when we have reached max bolus, when ketone correction is used, and how this improved glucose control and outcomes. These gaps provide areas for future investigation. Future modifications of an EHR order set may also seek to utilize serum ketone evaluations and adjust correction doses based on response to previous doses. In addition, there is an opportunity in general to use EHR data about responsiveness to insulin doses to further help refine carbohydrate coverage and correction factors through EHR trend analysis.
Recently, there has been an increase in younger patients who require special dilution insulin while inpatient to provide better glycemic control and safe dosing of insulin. The calculator is not currently able to calculate special dilution doses. This presents an opportunity as a calculator would improve the time to obtain a dose and, subsequently, blood glucose regulation. The workflow without the dosing calculator is complicated and takes time, and similar to our pre-calculator workflow it requires the nurse to notify the medical team of the blood glucose prior to feeds or breakfast, lunch, and dinner via paging and then the physician notifies pharmacy of the correction dose. Currently, the special dilution order is seen by the pharmacy team, prepared in the pharmacy and dispensed in a syringe, and delivered as a one-time order. One-time orders are more difficult for nurses to be able to see, because once completed, the order is moved on the medication administration record to discontinued medications. This requires scrolling and creates opportunity for the patient to receive correction doses too close together. In the future, it would be optimal if the nurse would be able to utilize a version of the insulin dosing calculator to calculate doses in real time with pharmacy notification, so the doses can be made quickly, the patient can receive it more efficiently, and can receive the same teaching of insulin calculation with the calculator as a tool even while using diluted insulin.
The exploration and further refinement of the aforementioned issues is helmed by a multidisciplinary team including nurses, pharmacists, endocrinologists, diabetes team members, and EHR specialists in our institution as is seen in other institutions that have implemented computer provider order entries. 3 This approach is critical, and we have found from our experience that having a distinct team and committees focused on responding to issues that arise is beneficial for safety and for quality improvement. It is unlikely at any point in the future that all issues will be resolved, and having a team in place with representative members that have a stake in utilization is essential, not only to further refine the process through iterative quality improvement cycles, but to further ensure that clinical practice guidelines are upheld as medicine further advances.
Supplemental Material
Supplement – Supplemental material for Insulin Bolus Calculator: Lessons Learned from Institutional Experience
Supplemental material, Supplement for Insulin Bolus Calculator: Lessons Learned from Institutional Experience by Valerie D. Nolt, Adrian Araya, Mohammed B. Ateya, Ming Chen, Jennifer Kelley, Patrick Arnold and Kanakadurga Singer in Journal of Diabetes Science and Technology
Footnotes
Acknowledgements
We would like to thank our Pediatric Diabetes Team, pharmacists, nurses, trainees, and the committees that have helped design, implement, test, and improve this calculator.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.