
Abstract
Several studies have shown the usefulness of an automated insulin dose bolus advisor (BA) in achieving improved glycemic control for insulin-using diabetes patients. Although regulatory agencies have approved several BAs over the past decades, these devices are not standardized in their approach to dosage calculation and include many features that may introduce risk to patients. Moreover, there is no single standard of care for diabetes worldwide and no guidance documents for BAs, specifically. Given the emerging and more stringent regulations on software used in medical devices, the approval process is becoming more difficult for manufacturers to navigate, with some manufacturers opting to remove BAs from their products altogether. A comprehensive literature search was performed, including publications discussing: diabetes BA use and benefit, infusion pump safety and regulation, regulatory submissions, novel BAs, and recommendations for regulation and risk management of BAs. Also included were country-specific and international guidance documents for medical device, infusion pump, medical software, and mobile medical application risk management and regulation. No definitive worldwide guidance exists regarding risk management requirements for BAs, specifically. However, local and international guidance documents for medical devices, infusion pumps, and medical device software offer guidance that can be applied to this technology. In addition, risk management exercises that are algorithm-specific can help prepare manufacturers for regulatory submissions. This article discusses key issues relevant to BA use and safety, and recommends risk management activities incorporating current research and guidance.
Keywords
Automated insulin dose bolus advisors (BAs) are used by insulin-treated diabetic patients to calculate insulin dosages for correction of out-of-target blood glucose and/or intake of carbohydrates. BAs provide a useful and simplified alternative to manual calculations of insulin dosing. To calculate appropriate bolus doses, a BA requires accurate settings for the insulin-to-carbohydrate ratio, glucose-correction factor, duration-of-insulin action, and correction target. 1 The BA then utilizes a proprietary algorithm to calculate the dose of insulin recommended for the user based on their inputs, and in some insulin dose advisors, historical data input by the user. Current literature has shown that integration of BAs into insulin pump software may help individuals more accurately meet prandial insulin dosage requirements, improve postprandial glycemic excursions, and achieve optimal glycemic control.2-5 However, evidence is sparse regarding the specifics of risk management for algorithms such as those used in BAs. In addition, there is no worldwide standard of care for diabetes, which complicates the development of software and/or devices intended to optimize glycemic control. Not surprisingly, BAs currently on the market around the world differ widely in their approaches to dosage calculation. More specifically, inputs required for calculation, handling of insulin-on-board calculations, and outputs shown to the user all vary widely from manufacturer to manufacturer.
Medical device safety is a risk management process that must encompass the life span of medical devices from inception to disposal. 6 These activities should be conducted in a consistent fashion, globally, to ensure the health and safety of diabetic patients in all countries. There are many local and global organizations with the charter of ensuring adequate regulation of medical devices and publishing and communicating regulations and standards to their audience. This article discusses key issues relevant to BA use and safety and provides recommendations for risk management activities incorporating current research and guidance. The purpose of this article is to present the current landscape and provide prompt further discussion on the topic of BA risk management.
Current Guidance for Development of BA Algorithms
Literature Review
Published articles, regulatory submissions, and books, primarily published within the past 10 years, with the majority being published within the last 3 years, were reviewed. International and local guidance documents were reviewed irrespective of year published, only with regard to topic and latest revision. A total of 142 sources were reviewed (see the appendix), with the following breakdown: insulin BA use/benefit (28%), standards of care/guidance documents (18%), insulin BA regulation/safety (25%), novel insulin dose algorithm (25%), and other (2%). Sources were included if they contained relevant information on drug BAs or insulin BAs, medical device regulation, and medical product risk management. Literature was excluded from the review if it did not include discussion regarding risks of drug BA use, regulation of medical devices or software, BA standards of care, development of insulin dose algorithms, or insulin BA use.
Current Guidance Documents
While numerous studies have shown that use an insulin BA is beneficial to most diabetic patients on continuous subcutaneous insulin infusion (CSII) therapy,2-5 the standards of care published by medical organizations vary in their recommendations for therapy goals, glycemic targets, and starting parameters for insulin BAs and CSII.7,8 For example, the 2011 American Association of Clinical Endocrinologists (AACE) Diabetes Care Plan Guidelines recommend fasting plasma glucose levels of less than 110 mg/dL and 2-hour postprandial glucose concentrations of less than 140 mg/dL. However, the 2012 American Diabetes Association (ADA) Standards of Diabetes Care recommends preprandial capillary plasma glucose of 70-130 mg/dL and peak postprandial capillary plasma glucose of less than 180 mg/dL. Neither guideline describes use or setting up of BAs for diabetes care.7,8 Moreover, many of the publications regarding medical device risk management are case studies and implementation guides, which can make interpretation and utilization of this information difficult for manufacturers.
Local and international regulatory bodies currently provide no guidance documents published specifically pertaining to insulin BAs. However, representatives from the regulatory agencies have shared expectations regarding BA functionality and safety at various meetings and conferences in recent years. As well, both the UK Medicines and Healthcare Products Regulatory Agency (MHRA) in the United Kingdom and the US Food and Drug Administration (FDA) have recently released documents pertaining to infusion pumps specifically, which often incorporate BA technology. Both of these documents describe basic infusion pump safety considerations for their respective countries.
The MHRA document (Device Bulletin, Infusion Systems) was a device bulletin released in 2010 and is intended for use by physicians and medical staff using infusion pumps. 9 It provides general infusion pump safety considerations for use and training of the devices.
The FDA document (Guidance for Industry and FDA Staff—Total Product Life Cycle: Infusion Pump—Premarket Notification) was released in 2010 as draft guidance and has not been finalized as of the date of this research. 10 This document provides recommendations for infusion pump regulatory submission as well as specific information on insulin dosing algorithms; the MHRA document does not provide these recommendations. The document also states that for infusion pumps that contain algorithms intended to provide dosing recommendations, it is recommended that manufacturers include the following information in their premarket notification: each dosing algorithm used, each algorithm in symbolic form, all parameters in each algorithm with identification of which parameters can be modified by the user, clinical data or other justification for why it is believed that the algorithm is appropriate for the target population, proof of verification and validation activities showing that calculations made by the BA are correct, and data demonstrating that the algorithm calculates insulin doses correctly. 10
In presentations at various meetings and conferences, the FDA has identified decision-making software such as insulin BAs as medical devices and actively regulates these devices. 11 Additional guidance released by the FDA’s Center for Devices and Radiological Health (CDRH) in 2005 (Guidance for Industry and FDA Staff: Guidance for the Content of Premarket Submissions for Software Contained in Medical Devices) describes the expectations regarding software development, level of concern, and scope of the guidance. 12 The FDA considers insulin BAs to fall under this guidance 11 and recognizes 4 primary review areas for insulin BAs: (1) intended use, (2) algorithm, (3) clinical evidence, and (4) documentation.
Risk management activities are also described in documents from the American National Standards Institute (ANSI), Association for the Advancement of Medical Instrumentation (AAMI), and the International Organization for Standardization (ISO). Medical Devices—Application of Risk Management to Medical Devices 13 and Medical Device Software Risk Management 14 recommend the following software-specific risk management activities: (1) analysis of the clinical or other intended use(s) of the device to identify clinical hazards and related software functionality providing clinical information or control commands related to safety and effectiveness; (2) identification of potential software causes that could contribute to a hazardous situation; (3) identification of software components that implement or could affect functionality related to safety or the implementation of risk control measures and identification of hardware, software, and/or labeling risk control measures to prevent software errors from resulting in a hazardous situation or to reduce the probability of such errors; (4) evaluation of residual risk after risk control measures are identified and determination of whether the risk is acceptable given the intended use and target population of the device; and (5) verification of risk control measures and software-related software components. 14
Use of an In Vitro Simulator
While some rules regarding BA algorithm assessment are supported by current literature and standards of care, other rules require additional support to demonstrate safety. Exercising the algorithm with an in vitro simulator can provide medical evidence of safety.
In vitro simulation allows the full functionality of the algorithm to be tested, especially the least likely scenarios that may not occur in a clinical trial. However, for product risk management activities, it is important that the simulator used be standardized and approved by regulatory agencies.
In 2011, the FDA approved the University of Virginia (UV) simulator for in silico testing of artificial pancreas control systems in the United States. This simulator is a computer-based diabetes simulation tool developed by UV and has been accepted by the FDA as an alternative to animal testing of type 1 diabetes control strategies. 15 The simulator uses a software algorithm to model the human metabolic system. There are now hundreds of theoretical, FDA-accepted patient models that researchers can use to test control algorithms. 16
Based on patient data from 300 children, adolescents, and adults with type 1 diabetes, the UV algorithm uses 26 different parameters to mimic human metabolism at the individual level, through several distinct patient profiles. Within these individual profiles, variables such as diet, exercise behavior, and insulin intake can be manipulated to test the accuracy or effectiveness of a new product under varying conditions—or to compare it to existing products. 15 This simulator, or a similar approach, would be ideal for exercising the capabilities of insulin dose algorithms to demonstrate safety.
Recommendations
The availability of published guidance documents can help alleviate some of the challenges that manufacturers face and can help ensure that products brought to market are safe and effective around the world. This is especially important when considering the safety concerns of algorithms, which do not specifically fall under the guidance of medical devices or medical software. However, if the guidance is not harmonized internationally, risk management activities and, ultimately, product safety may be critically inconsistent. My opinion, after performing the extensive research (appendix) and case study activities described in this report, is as follows: because of their unique functionality and risks posed to users, insulin dose calculating algorithms should have specifically dedicated risk management activities assigned. The following recommendations may be helpful in developing standardized, international guidance for software designers, manufacturers, and regulatory agencies (Table 1).
Recommendations for Insulin Dose Calculator Risk Management.
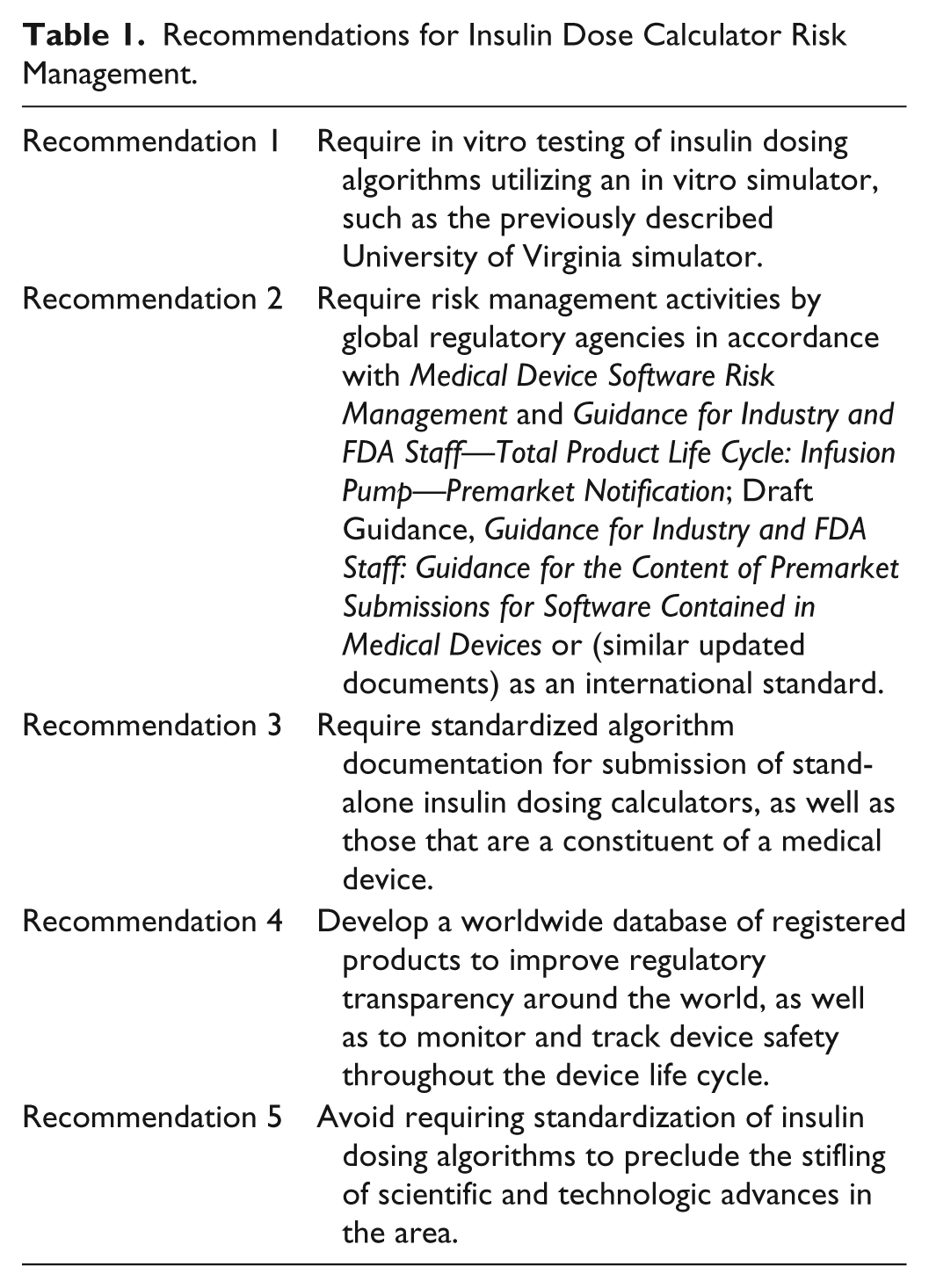
In vitro testing of insulin dosing algorithms with the educational version of the simulator would provide a standard platform for algorithm testing. If accepted as an international standard, all algorithms developed in other countries would be held to the same standard of proof. This would promote consistency and safety of insulin dosing algorithms, and would assist regulatory agencies in reviewing in vitro testing results.
Risk management activities in accordance with these recommendations would ensure the consistency of risk management activities for all insulin dosing algorithms. Once provided as an international standard, this document would provide the much-needed guidance for manufacturers to follow and ensure the safety of their algorithms, as well as for submission of their algorithm-containing software or device to regulatory agencies. For the regulatory bodies, having an approved guidance would ensure clear directives for submissions to follow, thus making the approval process more straightforward with clear expectations.
This type of exploration and documentation would be extremely helpful for manufacturers and regulatory agencies as it clearly demonstrates the medical evidence associated with each component of the insulin BA algorithm. In addition, appropriately modified information of this type may even be beneficial to consumers. The exploration of literature and justification of algorithm rules would identify gaps in the literature support of the algorithm. The areas of the algorithm not supported by current literature or standards of care could then be justified in another manner, such as in vitro simulation or clinical studies, to meet regulatory standards for safety. This would ensure that all aspects of the algorithm are thoroughly explored and supported to ensure safety.
The benefit of these databases is well known; however, their benefit is limited to the geographic area(s) which they support. If a product is sold in an area of the world where it is not registered, then that country will have no record of the product or any postmarket reporting on that product. This is especially problematic in the EU, where registers are maintained by competent authorities and a manufacturer needs register with only one to market its product throughout the EU.
There are many different insulin dosing algorithms currently available globally, and novel algorithms continue to be researched and developed. Many of these algorithms behave differently from one another in their calculation method and logic, but generate similar recommendations. Fine-tuning the algorithm, allowing varying inputs, creating “smart” algorithms, and integrating blood glucose (BG) and continuous glucose monitoring (CGM) data all enhance the functioning of insulin BAs over time. To avoid hindering innovation, it is essential that a standardized algorithm not be mandated by regulatory agencies. Acceptance of a policy such as this would stifle the evolution of these algorithms and prevent potential breakthroughs in diabetes care.
Conclusions
There is a general consensus that insulin BAs are useful and beneficial.2-5 Current literature also shows that additional novel insulin dosing algorithms are being researched and developed.17-20 After an extensive literature research (see the appendix) and case study exploration, my opinion on this topic is as follows: clearer guidance is needed to assist both the manufacturers creating these algorithms and the regulatory agencies that will ultimately review them.
Specific risk management activities for BA algorithms, including simulator testing, flowchart diagramming, and literature support search, have been recommended in this article. Risk management activities, as described in a few key guidance documents related to medical device software and infusion pumps, have also been identified.
Manufacturers and developers of insulin BAs would benefit from standardized guidance because risk management expectations would be clearly defined and well organized, thus facilitating greater adherence. It would also provide consistency for regulatory agencies reviewing submissions, to ensure the testing and results were consistent and more easily reviewed.
However, while required standardization of algorithm may ease regulatory burden regarding insulin BAs, this would likely stifle innovation in the field of diabetes. Mandating a standard method for calculating insulin dosage may hinder the development of algorithmic advances that could potentially provide breakthroughs in the field of diabetes care around the world.
In summary, international acceptance and adoption of the recommendations put forth in this article for insulin BA risk management and guidance may greatly benefit manufacturers, regulatory agencies, and, most important, people with diabetes worldwide. This article provides a short but solid survey of the problem and will hopefully prompt further attention and publication regarding this topic.
Footnotes
Appendix
Comprehensive Literature Review List

| Group | First author | Subject | Year |
|---|---|---|---|
| Insulin dose algorithm/use | |||
| Barnard | Use of an automated bolus calculator in MDI patients | 2012 | |
| Bernasko | Intensive insulin therapy | 2007 | |
| Blazik | The education of patients | 2010 | |
| Bode | Diabetes management in the new millennium | 2002 | |
| Cavan | Automated bolus advisor control and usability study (ABACUS): protocol | 2012 | |
| Clavel | Treatment by external insulin pump | 2010 | |
| Colin | Glucose meters with built-in automated bolus calculator | 2013 | |
| Colquitt | Clinical and cost-effectiveness | 2004 | |
| Cukiermann-Yaffe | Key elements for successful | 2011 | |
| Gross | A bolus calculator | 2003 | |
| Hirsch | Practical pearls | 2010 | |
| King | Basal bolus dosing | 2005 | |
| King | A prospective evaluation | 2007 | |
| Klupa | Clinical usefulness of a bolus calculator | 2008 | |
| Mastrototaro | The integrated minimed | 2009 | |
| Michon | Insulin pump and intensive | 2002 | |
| Murphy | Reducing hyperglycemia | 2009 | |
| Pollom | Optimizing inpatient glycemic control | 2010 | |
| Renard | Insulin pump use in Europe | 2010 | |
| Roemer | Tips and tools for insulin pump | 2009 | |
| Romatowska | The effect of using the insulin pump bolus calculator compared to standard insulin dosage calculations in patients with type 1 diabetes mellitus—systematic review | 2013 | |
| Scheiner | Insulin pump therapy | 2009 | |
| Schmidt | Use of an automated bolus calculator in MDI-treated type 1 diabetes: the BolusCal Study | 2012 | |
| Shalitin | Benefits of a bolus calculator | 2010 | |
| Shashaj | Benefits of a bolus calculator | 2008 | |
| Spellman | Management of diabetes | 2003 | |
| Tamborlane | Insulin pump therapy in childhood | 2003 | |
| Unger | Optimizing insulin therapy | 2008 | |
| Walsh | Guidelines for insulin dosing | 2010 | |
| Walsh | Guidelines for optimal bolus | 2011 | |
| Walsh | Pumping insulin | 2003 | |
| Walsh | Pumping insulin | 2006 | |
| Wei | Basal-bolus insulin protocols | 2011 | |
| Weissberg | Insulin pump therapy | 2003 | |
| White | Insulin pump therapy | 2007 | |
| White | When and how to implement | 2009 | |
| Wilson | Intensive insulin therapy | 2007 | |
| Wolpert | Hands-on demonstration | 2005 | |
| Zhang | The current situation review | 2010 | |
| Zhang | Second insulin pump safety | 2010 | |
| Zisser | Bolus calculator: a review | 2008 | |
| Zisser | Clinical performance of 3 bolus | 2010 | |
| Zisser | Clinical update on optimal prandial insulin | 2009 | |
| Standards of care/guidance documents | |||
| AACE | Diabetes care plan guidelines | 2011 | |
| AADE | Consensus insulin pump therapy | 2008 | |
| AAMI | Medical device software risk management | 2005 | |
| ADA | Practical insulin | 2011 | |
| ADA | Standards of medical care | 2011 | |
| EC | Directive 98/79/EC | 1998 | |
| EN | Biological evaluation | 2009 | |
| EN | Clinical investigation of medical devices | 2009 | |
| EN | Medical device software | 2006 | |
| EN | Medical devices—application of risk management | 2009 | |
| EN | Medical devices—application of usability | 2008 | |
| EN | Medical devices—quality management | 2009 | |
| EN | Medical electrical equipment part 1-10 | 2008 | |
| EN | Medical electrical equipment part 2-24 | 1998 | |
| FDA | Draft guidance | 2011 | |
| FDA | Guidance for industry | 2010 | |
| ISO | Guide to the development | 2012 | |
| ISO | Risk management | 2009 | |
| ISO | Safety aspects | 1999 | |
| Malerbi | Brazilian diabetes society | 2006 | |
| TIR | Technical information report | 2009 | |
| WHO | Medical device regulations | 2003 | |
| aami.org | |||
| fda.gov | |||
| iso.org | |||
| Medical device regulation/safety | |||
| Babamir | Constructing a model-based | 2010 | |
| Bartoo | Risk management | 2003 | |
| Benet | A risk driven approach | 2011 | |
| Burton | Improving software risk management | 2008 | |
| Burton | A risk management capability model | 2008 | |
| Burton | A software risk management capability model | 2008 | |
| Coverity | Governance, risk, and compliance | 2011 | |
| Devices4Limited | Regulation of health apps | 2012 | |
| Donawa | Effective risk management | 2004 | |
| Goodman | Medical device error | 2002 | |
| Grimes | Medical device security | 2004 | |
| Hedge | Case study—risk management | 2011 | |
| Israelski | Human factors risk management | 2004 | |
| Jardine | Risk management frameworks | 2003 | |
| Jones | Risk management in the design | 2002 | |
| Klonoff | Insulin pump safety meeting | 2009 | |
| McCaffery | Improving software risk | 2009 | |
| McCaffery | Risk management capability model | 2009 | |
| Mingziao | A quantitative approach | 2011 | |
| Narvaez | Prospective risk management | 2010 | |
| Paul | A review of the security | 2011 | |
| Pietzsch | Review of US medical device | 2007 | |
| Rakitin | Coping with defective software | 2006 | |
| Reviewers | Guidance for industry and FDA | 2000 | |
| Robson | Risk management and biomedical | 2005 | |
| Schultz | Medical device safety | 2007 | |
| Shah | Current status of the regulation | 2008 | |
| Sherwin-Smith | Medical applications—the future of regulation | 2012 | |
| Small | Medical device-associated safety | 2004 | |
| Wang | Discussions on the regulatory | 2009 | |
| Wood | Software risk management | 2008 | |
| Xie | Risk management for medical devices | 2007 | |
| Xu | Discussion about the application | 2006 | |
| Zimlicki | Bolus calculator regulation | 2011 | |
| Zuckerman | Medical device recalls | 2011 | |
| Novel algorithm | |||
| Anderson | Multiple daily injections | 2009 | |
| Boiroux | Optimal insulin administration | 2009 | |
| Boiroux | Strategies for glucose control | 2010 | |
| Bondia | Coordinated basal-bolus | 2009 | |
| Campbell | Calculating insulin on board for extended bolus | ||
| Charpentier | The Diabeo software | 2011 | |
| Cook | The intelligent dosing system | 2005 | |
| Davidson | Analysis of guidelines | 2008 | |
| Edelman | Insulin pump therapy | 2010 | |
| FDA | Endotool drug dose calculator | 2006 | |
| FDA | Glucommander plus | 2006 | |
| FDA | Glytec, LLC | 2010 | |
| FDA | Intelligent dosing system | 2008 | |
| Gonzalez-Rodriguez | Should the amount of fat and protein | 2010 | |
| Grandinetti | Web-based prediction | 2011 | |
| Hedbrandt | The Sarimner diabetes simulator | 2007 | |
| Juneja | Safety and effectiveness | 2008 | |
| King | How much do I give? | 2010 | |
| Kordonouri | Supplementary fat plus protein | 2010 | |
| Laha | Glucose control in critical illness | 2008 | |
| Lippaiova | Safety of new algorithms | 2008 | |
| Marling | Case-based decision support | 2008 | |
| Mathews | A new model to estimate bolus | 2009 | |
| Olinder | Postprandial glucose levels | 2009 | |
| Palerm | Prandial insulin dosing using | 2007 | |
| Pankowska | Bolus calculator with nutritional | 2010 | |
| Pankowska | A review of the “bolus guide” | 2010 | |
| Pelzer | Preliminary application of a new bolus | 2011 | |
| Revert | Calculation of the best basal-bolus therapy | 2011 | |
| Revert | Combining basal-bolus | 2010 | |
| Rossi | Diabetes interactive diary | 2010 | |
| Rossi | Interactive diary for diabetes | 2009 | |
| Sahota | Computerized clinical decision | 2011 | |
| Schwartz | Use of case-based reasoning | 2008 | |
| Shapira | Bolus guide: a novel insulin | 2010 | |
| Other | |||
| ADA | Workgroup on Hypoglycemia | 2005 | |
| Estabrook | Commercially available UV simulator | 2011 | |
| Kravitz | From insight to implementation | 2005 |
Acknowledgements
Christen Rees penned this article while a student in the Health Product Risk Management program at Virginia Polytechnic Institute and State College. This article is a modification of the final project and report for her master’s degree. The author would like to acknowledge Robin Wagner, Patsy Allen, Ann Buskirk, George Flick, Stan Mastrangelo, Al Dolan, and Lori Marsh for their inspiration and guidance during her work.
Abbreviations
AACE, American Association of Clinical Endocrinologists; AAMI, Association for the Advancement of Medical Instrumentation; ADA, American Diabetes Association; BA, bolus advisor; BG, blood glucose; CDRH, Center for Devices and Radiological Health; CE, Conformité Européenne; CGM, continuous glucose monitoring; CSII, continuous subcutaneous insulin infusion; FDA, Food and Drug Administration; GHTF, Global Harmonization Task Force; HbA1c, glycosylated hemoglobin; IDDM, insulin-dependent diabetes mellitus; ISO, International Organization for Standardization; MDD, Medical Devices Directive; MDI, multiple daily injections; MHRA, Medicines and Healthcare Products Regulatory Agency; TIR, Technical Information Report; UN, United Nations; WHO, World Health Organization.
Declaration of Conflicting Interests
The author(s) declared the following potential conflict of interest with respect to the research, authorship, and/or publication of this article: Christen Rees is employed at Roche Diagnostics Operations, Indianapolis, IN, USA.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.