
Abstract
Background:
Blood glucose meters remain an effective tool for blood glucose monitoring (BGM) but not all meters provide the same level of insight beyond the numerical glucose result.
Objective:
To investigate healthcare professional (HCP) perceptions of four meters and how these meters support the achievement of self-management goals recommended by diabetes clinical practice guidelines.
Methods:
Three hundred and fifty-three HCPs from five countries reviewed the features and benefits of four meters using interactive webpages and then responded to statements about the utility of each meter and ranked each meter in terms of clinical value.
Results:
Meter D ranked significantly higher in terms of clinical utility for all 13 guideline questions (70%-84%, P < .05) compared to other meters. Endocrinologists (69%-85%), primary care physicians (PCP; 63%-80%), and diabetes nurses (DN; 80%-89%) consistently ranked meter D highest for all guideline questions. DNs ranked selected questions significantly higher compared to PCPs (8 of 13) or endocrinologists (3 of 13; P < .05). Meter D achieved strong endorsement from HCPs in France and Germany, followed by the United States and Canada, with comparatively lower responses from Italian HCPs (P < 0.05). With respect to self-management, 80% of HCPs selected meter D as their first choice for patients with type 1 diabetes to help patients improve diabetes management or understand their numbers to help them stay in range.
Conclusions:
HCPs had strong preference for a meter providing additional insights, messages, and guidance direct to the patient to support achievement of self-management goals recommended by diabetes clinical practice guidelines.
Keywords
Introduction
Monitoring is one of the Association of Diabetes Care and Education Specialists AADE7 self-care behaviors required to achieve diabetes outcomes. 1 Blood glucose monitoring (BGM) generates information that can be shared with the healthcare team to facilitate problem-solving discussions to modify multiple self-care behaviors including healthy eating, being active, and taking medications while supporting risk reduction (eg, hypoglycemia prevention) and healthy coping. 1 Diabetes clinical and educational guidelines support the use of BGM to manage diabetes.2-6 The incorporation of monitoring data into the care plan is required to individualize treatment and to effectively evaluate the impact of changes in medications or health behaviors on diabetes outcomes.4-6 Structured monitoring (eg, a seven-point profile of blood glucose (BG) values before meals, two hours after meals, and at bed time) over several days provides multiple data points to identify trends and patterns and is recommended over single-point random glucose checks.1,7-9 Structured checking supports the use of BGM data to make appropriate therapy adjustments 10 and can reduce therapeutic inertia.11,12 A systematic review identified that telehealth interventions that incorporated structured BGM into these intervention were associated with lower hemoglobin A1C (A1C) and studies with more BGM elements showed larger A1C improvement. 7
Selecting a meter that best matches the needs of the individual ensures that sufficient data are available for review and interpretation. 5 However, many people living with diabetes report that their HCPs do not routinely review their monitoring data and that they personally take no action on their results.5,13 A study focusing on patient perceptions of monitoring found that only 28% considered values higher than 235 mg/dL as above range. 13
While continuous glucose monitors (CGMs) are becoming more common, the majority of people living with diabetes still use glucose meters. However, not all meters are equal in terms of the features or functionality they provide; therefore, understanding how various meters meet the needs of individual patients and their HCPs is timely. The current study sought to evaluate HCP perceptions regarding the clinical utility of meters from four leading manufacturers to understand how each meter could support the achievement of self-management goals recommended by diabetes guidelines.
Methods
Materials
Four meters were evaluated in this study, which included Meter A (Accu-Check Guide, Roche Diabetes Care, Indianapolis, IN, USA), Meter B (Contour Next ONE, Ascensia Diabetes Care, Parsippany, NJ, USA), Meter C (FreeStyle Lite, Abbott Diabetes Care, Inc, Alameda, CA, USA), and Meter D (OneTouch Verio Reflect, Lifescan, Wayne, PA, USA; Figure 1). Meter screen images used in online exercises were taken from current owners’ booklets (OBs) and/or quick start guides (QSGs) for each meter.

Example webpages for clinical guidance statements 1 and 2.
Procedure
This online evaluation was conducted in five countries (Canada, France, Germany, Italy, and the United States). Meter screen images were shown in the appropriate languages and with representative glucose values in mg/dL or mmol/L. Numerical values shown with the four meters (Figure 1) were kept consistent to ensure HCP feedback was focused on how information was visually presented and not influenced by the glucose values. HCPs from individual practices and institutions, including endocrinologists, PCPs, and DNs, were screened and recruited by an external vendor (IPSOS, Parsippany, USA) who also conducted the online study. A steering group of HCPs reviewed current clinical guidelines (eg, American Diabetes Association [ADA] Standards of Medical Care in Diabetes, 201914,15; Management of Hyperglycemia in Type 2 Diabetes: European Association for the Study of Diabetes (EASD) & ADA, 2018 6 ) and identified and agreed on eight key clinical guidance statements from these guidelines (Table 1) that best described needs that could be met by glucose monitoring. The steering group of HCPs also reviewed webpage content representing each meter (per guideline statement) as the basis for the online feedback from the recruited HCPs.
Clinical Guidance and Related Survey Questions.
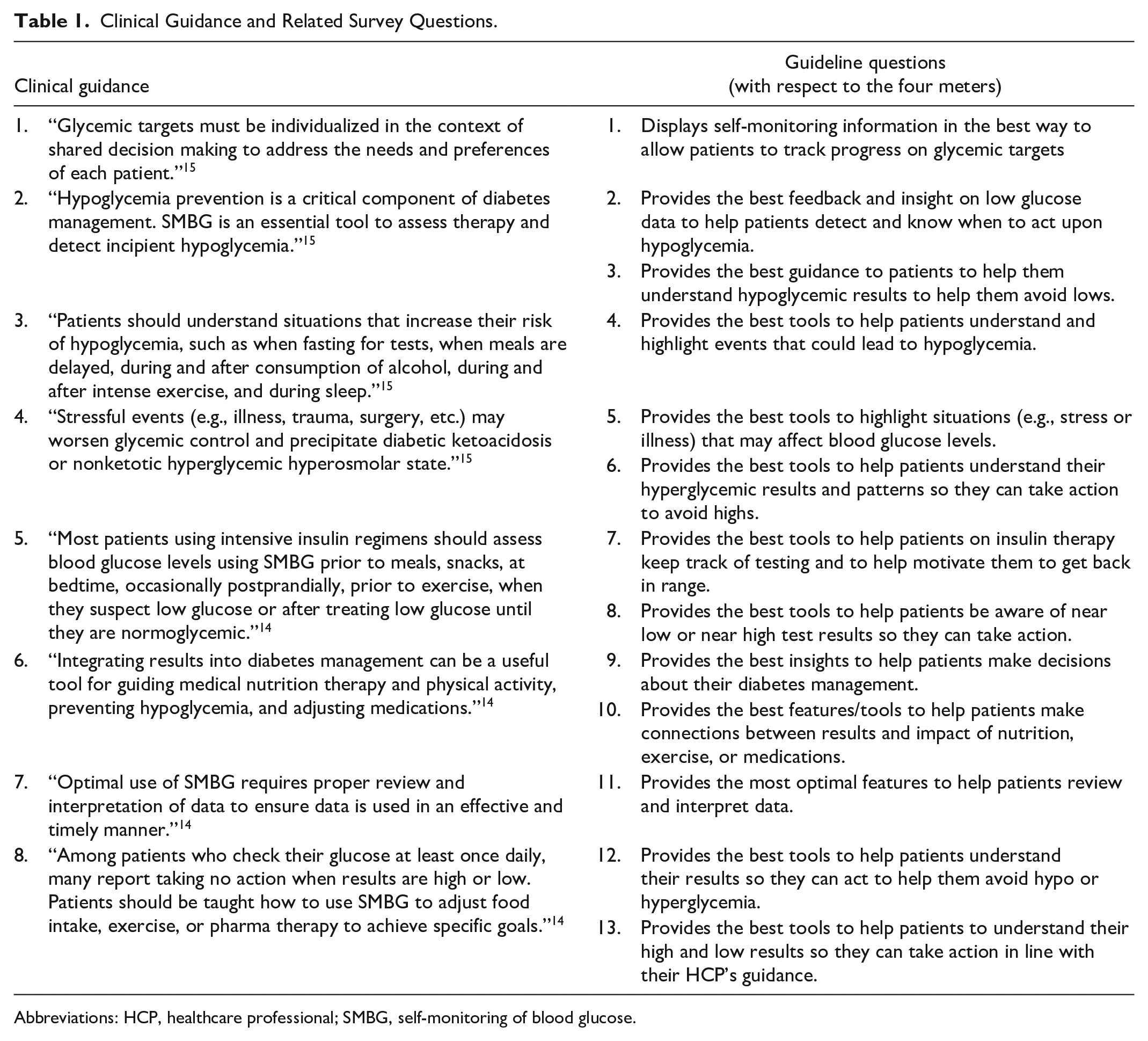
Abbreviations: HCP, healthcare professional; SMBG, self-monitoring of blood glucose.
To ensure adequate representation, a sampling target of 30 endocrinologists, 20 PCPs, and 20 DNs for a total of 70 HCPs per country were indicated. HCPs were initially identified from existing IPSOS databases and then sent an email inviting them to consider participation by connecting to the online study webpage to read further information. HCPs completed online pre-study screening questions to determine eligibility. Inclusion criteria required HCPs to treat 10 or more people with type 1 diabetes or type 2 diabetes per week with at least 15% using insulin therapy. Additionally, the HCPs must use meter data to facilitate treatment decisions and behavior changes. HCPs not meeting all inclusion criteria or with a conflict of interest were excluded. Eligible HCPs completed pre-study demographic and clinical practice questions. During the online study, the HCPs were shown each clinical guidance statement one at a time in association with meter screens (from meters A, B, C, and D) relevant to addressing that specific statement (see examples in Figure 1). This allowed HCPs to respond to one or more questions pertaining to each statement and to rank each meter (from one to four, with one being the highest score) based on how well each meter supports the clinical guidance (for example, “Provides the best features/tools to help patients make connections between results and impact of nutrition, exercise, or medications”). This same review and ranking process continued for all 8 clinical guidance statements and 13 guideline questions.
Finally, HCPs read 13 additional questions to evaluate the potential clinical benefit of each meter to support self-management and selected their first choice of the 4 unbranded meters for each statement. For example, “[A, B, C or D meter] is the best meter to help patients understand their results to help them stay within the glycemic range set with their HCP.” The study was conducted from November 11 to 29, 2019.
Statistical Analyses
Analysis of variance was used to determine statistically significant differences between the mean scores across the four meter types. If a statistical difference was found at the 5% significance level, pairwise multiple comparisons were conducted to identify which pairs of meter models were statistically different. If the data were found to be non-normally distributed, an equivalent nonparametric test was used (eg, Kruskal Wallis). For secondary end points (eg, HCP demographics) continuous demographic variables were presented as mean and standard deviation (SD) and median and range. Minitab 18.0 and IBM SPSS V21.0 were used for all analyses.
Results
Healthcare Professionals’ Demographic and Clinical Practice Information
The study population included 353 HCPs from Canada (n = 71), France (n = 70), Germany (n = 70), Italy (n = 72), and the United States (n = 70), and 55% (n = 193) were male. The HCP groups included 43% endocrinologists (n = 151), 29% PCPs (n = 102), and 28% DNs (n = 100). Age ranged from 25 to 65+ years with the 50 to 65+ age group accounting for 50% of all HCPs (n = 177). Mean time in clinical practice treating people with diabetes was 16.9 years for endocrinologists, 19.2 for PCPs, and 15.0 for DNs. The average number of patients seen per week was 96.0 for endocrinologists, 45.7 for PCPs, and 49.0 for DNs. People with type 1 diabetes accounted for 21.9% of all patients seen by HCPs, and 55.4% patients were on some form of insulin therapy. Use of new continuous glucose monitoring (CGM) technology was evident, with 29.3% and 18.2% of HCPs reporting that their patients were using a sensor in conjunction with insulin injections or pumps, respectively (Table 2).
Summary of Demographics Data for All Healthcare Professionals (n = 353).
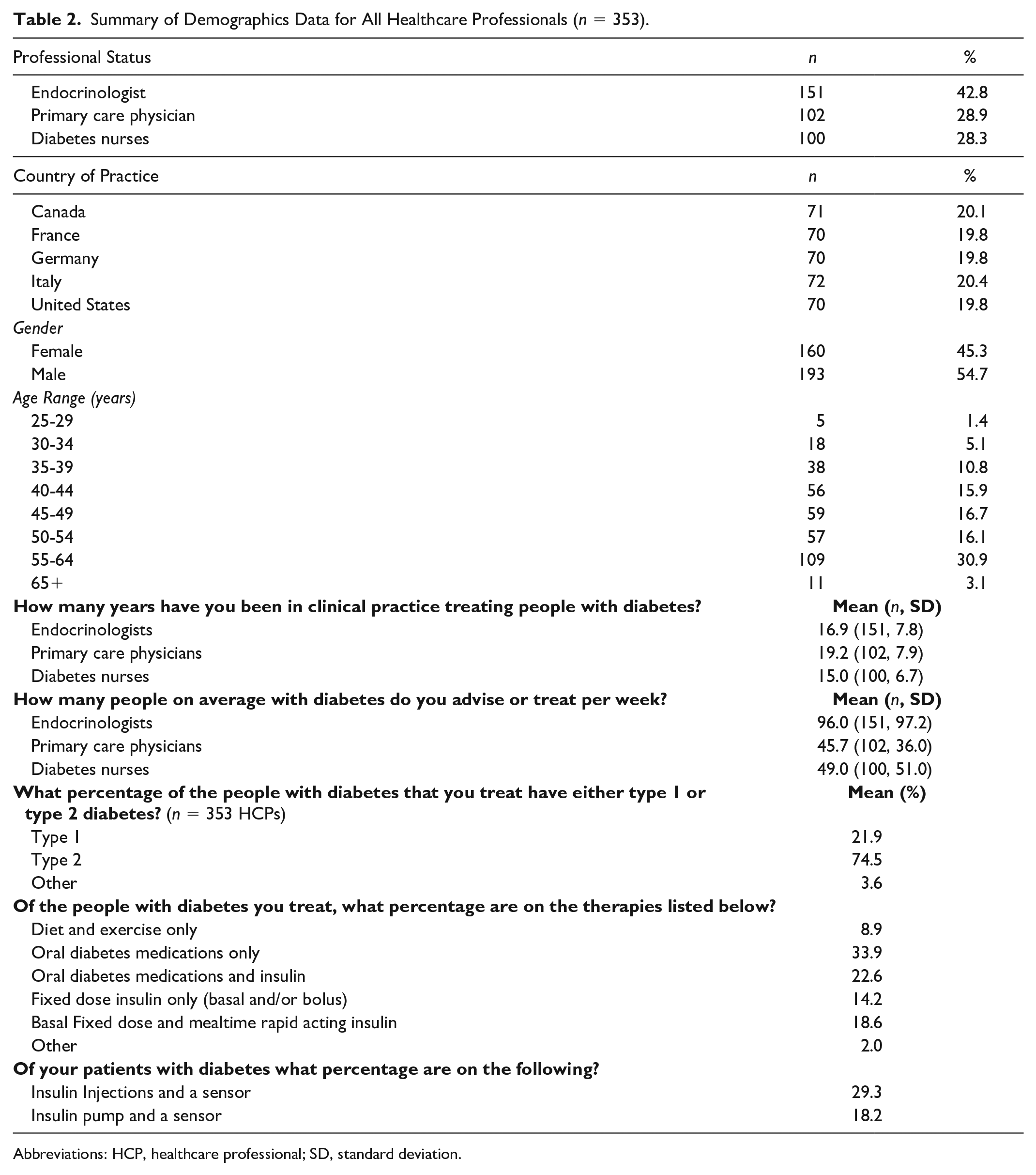
Abbreviations: HCP, healthcare professional; SD, standard deviation.
Healthcare Professionals’ Satisfaction With the Four Meters Based on Clinical Guidelines
The percentage of first choice rankings from HCPs for the 13 guideline questions are shown in Figure 2. Meter D received the highest ranking for all 13 guideline questions relating to the 8 clinical guidance statements, garnering between 70% and 84% of first choice rankings across all questions. Post hoc pair-wise comparisons confirmed meter D scored statistically higher than all other meters for all questions (P < .05). Meter A received the highest rank from HCPs but only 8% to 19% of the time across the 13 guideline questions, followed by meter B (2%-9%) and meter C (3%-7%). Guideline question 6 (“Provides the best tools to help patients understand their hyperglycemic results and patterns so they can take action to avoid highs”), relating to clinical guidance statement 4, scored the highest for meter D at 84%. Meter D scored its lowest top rank of 70% for guideline question 12 (“Provides the best tools to help patients understand their results so they can act to help them avoid hypo or hyperglycemic”) relating to clinical guidance statement 8.
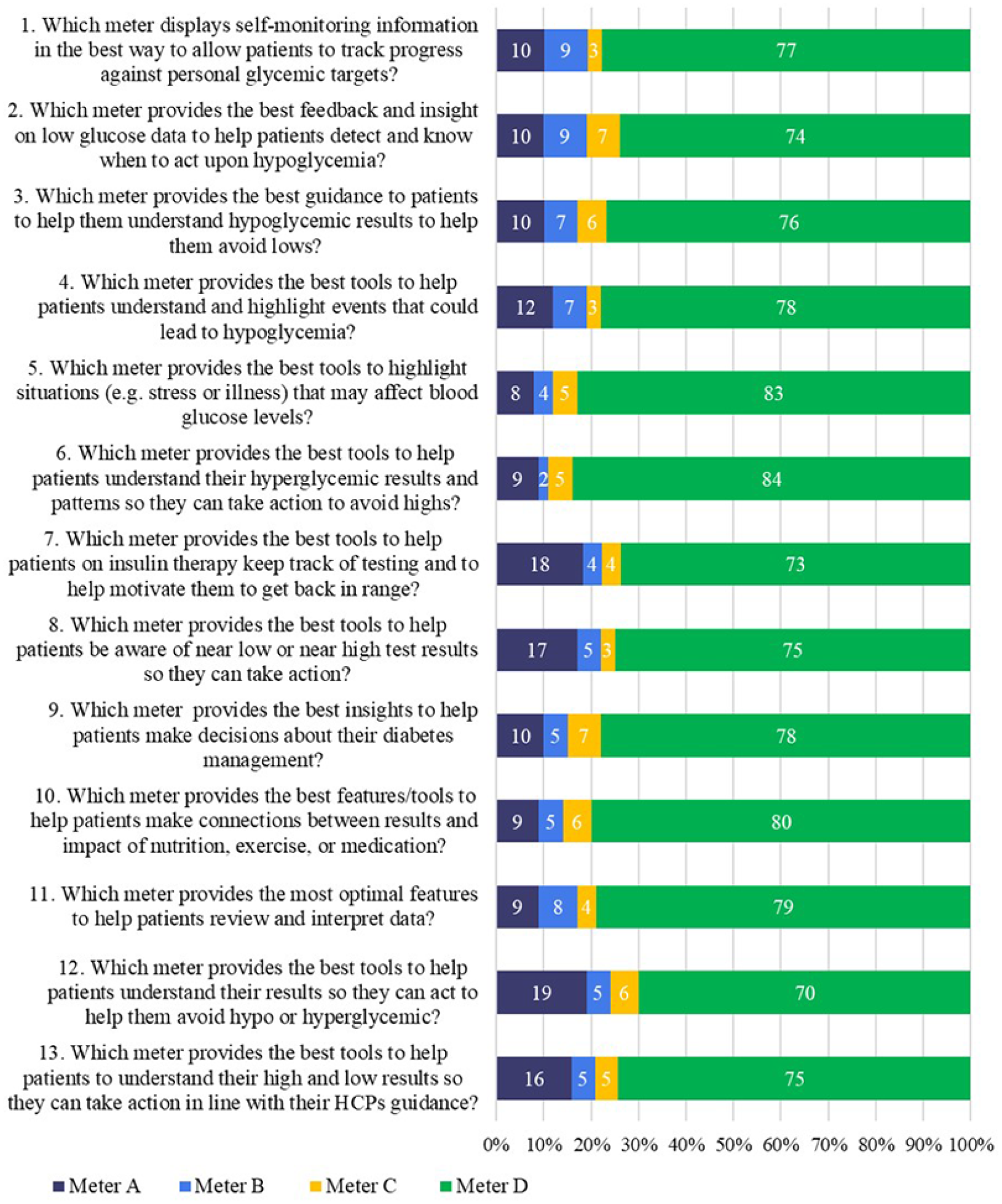
First-place rankings (%) received from healthcare professionals for meter A, B, C, or D in response to how well each meter satisfied the 13 guideline questions.
Individual Responses From Endocrinologists, PCPs, and DNs for Meter D
Across all 13 guideline questions, meter D scored the highest from endocrinologists (69%-85%), PCPs (63%-80%), and DNs (80%-89%) for each question, compared to meter A, B, or C. The mean (SD) for meter D after combining responses to all 13 guideline questions was 76.1 (4.96) for endocrinologists, 71.5 (4.55) for PCPs, and 84.7 (2.93) for DNs. DNs ranked meter D higher than endocrinologists or PCPs did for all 13 guideline questions and significantly higher for 8 of 13 guideline questions (P < .05) compared to PCPs and for 3 of 13 guideline questions compared to endocrinologists (P < .05; Figure 3). PCPs gave their highest response for meter D in response to guideline question 5 (“Provides the best tools to highlight situations (eg, stress or illness) that may affect blood glucose levels”), whereas endocrinologists and DNs both gave highest responses of 85% and 89%, respectively, for guideline question 6 (“Provides the best tools to help patients understand their hyperglycemic results and patterns so they can take action to avoid highs”). DNs rated guideline question 10 equally high at 89% (“Provides the best features/tools to help patients make connections between results and impact of nutrition, exercise, or medications”).
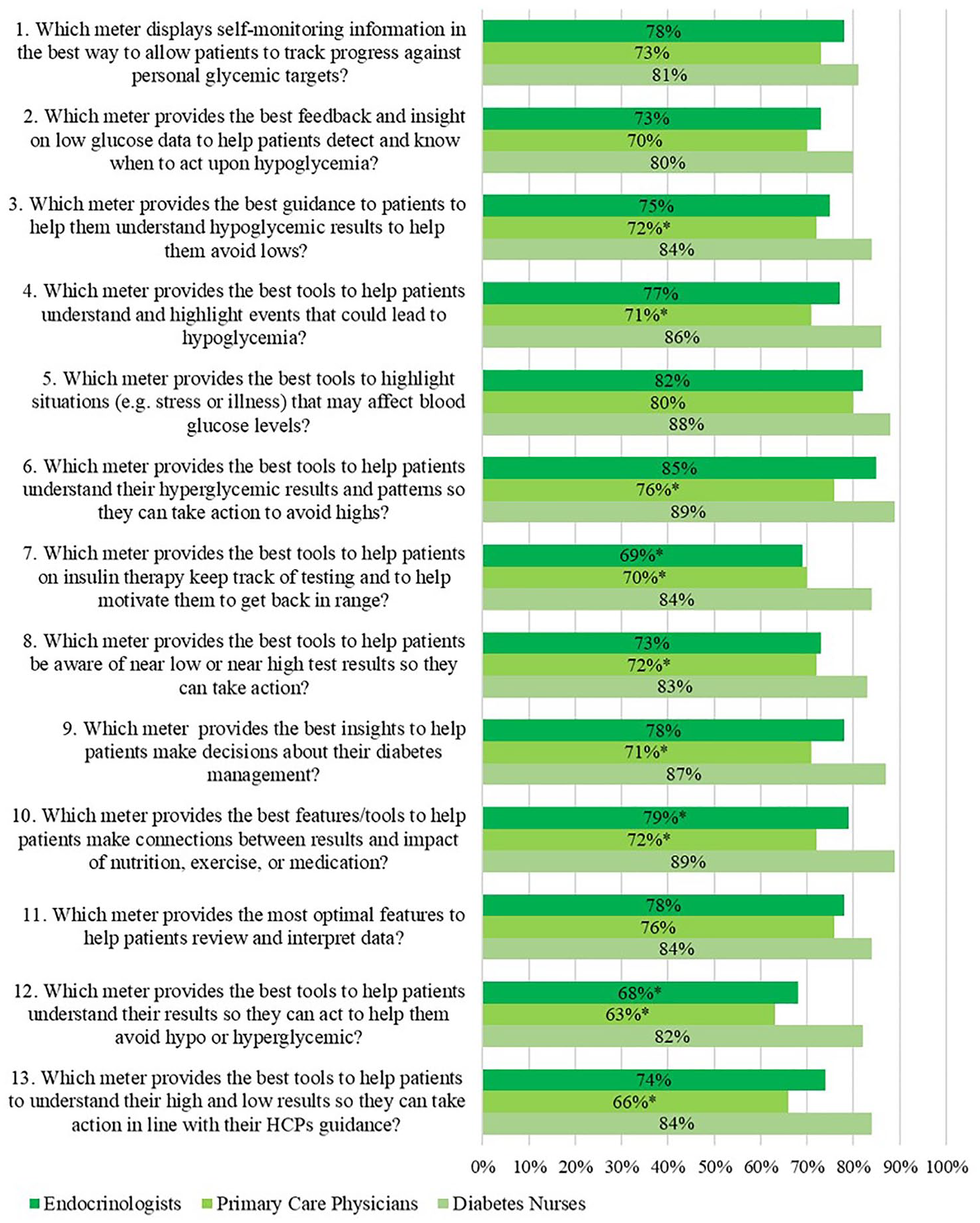
First choice rankings (%) for meter D received from endocrinologists, primary care physicians (PCPs), and diabetes nurses (DNs) in response to how well meter D satisfied 13 guideline questions.
Individual Responses From Endocrinologists, PCPs, and DNs by Country for Meter D
Across all 13 guideline questions, meter D scored the highest by HCPs in Canada (65%-89%), France (79%-89%), Germany (74%-87%), Italy (61%-76%), and the United States (73%-81%) compared to meter A, B, or C (Figure 4). The mean (SD) for meter D after combining responses to all 13 guideline questions per country was 79.0 (8.38) for Canada, 84.20 (2.94) for France, 81.5 (3.93) for Germany, 65.7 (5.90) for Italy, and 75.8 (3.52) for the United States. There were some variations among the countries. Italy scored significantly lower (P < .05) than all countries while the United States was significantly higher than Italy yet significantly lower (P < .05) than France and Germany and not different from Canada.
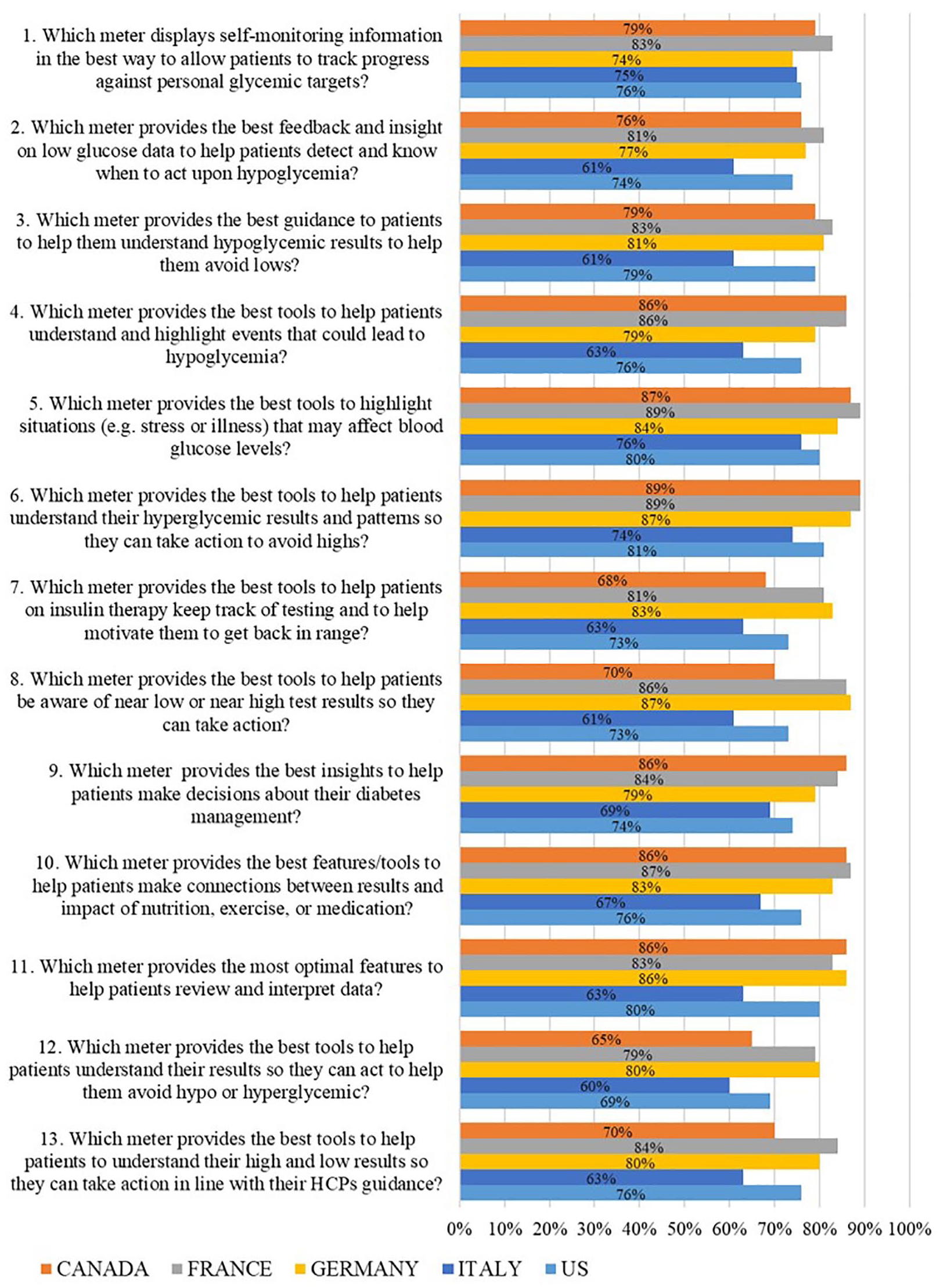
First choice rankings (%) for meter D received from healthcare professionals in 5 countries in response to how well meter D satisfied 13 guideline questions.
HCP Responses on the Clinical Benefit of Meter A, B, C, or D to Support Self-Management
Meter D received significantly higher responses than the other meters for all 13 clinical benefits for self-management support questions (P < .05) focused on the clinical benefits of the 4 meters (Table 3). The statement “Is the best meter in helping patients understand their results so they know if they need to make any behavior changes to manage blood glucose variability” received 82% of all HCP responses for meter D, compared to only 7%, 7%, and 5% for meters A, B, and C, respectively. Furthermore, 80% of all HCPs felt meter D was “the best meter to help patients improve their diabetes management,” “best meter for patients with Diabetes Type 1,” or “best meter to help patients understand their numbers to help them stay in range.” Meter D scored slightly lower on two questions “best meter for patients with Diabetes Type 2” and “best meter to provide guidance for patients that are newly diagnosed with diabetes.” Even so, meter D still scored considerably higher than meter A, B, or C for these two questions.
Healthcare Professionals’ Responses on the Clinical Benefit of Meter A, B, C, or D to Support Self-Management.
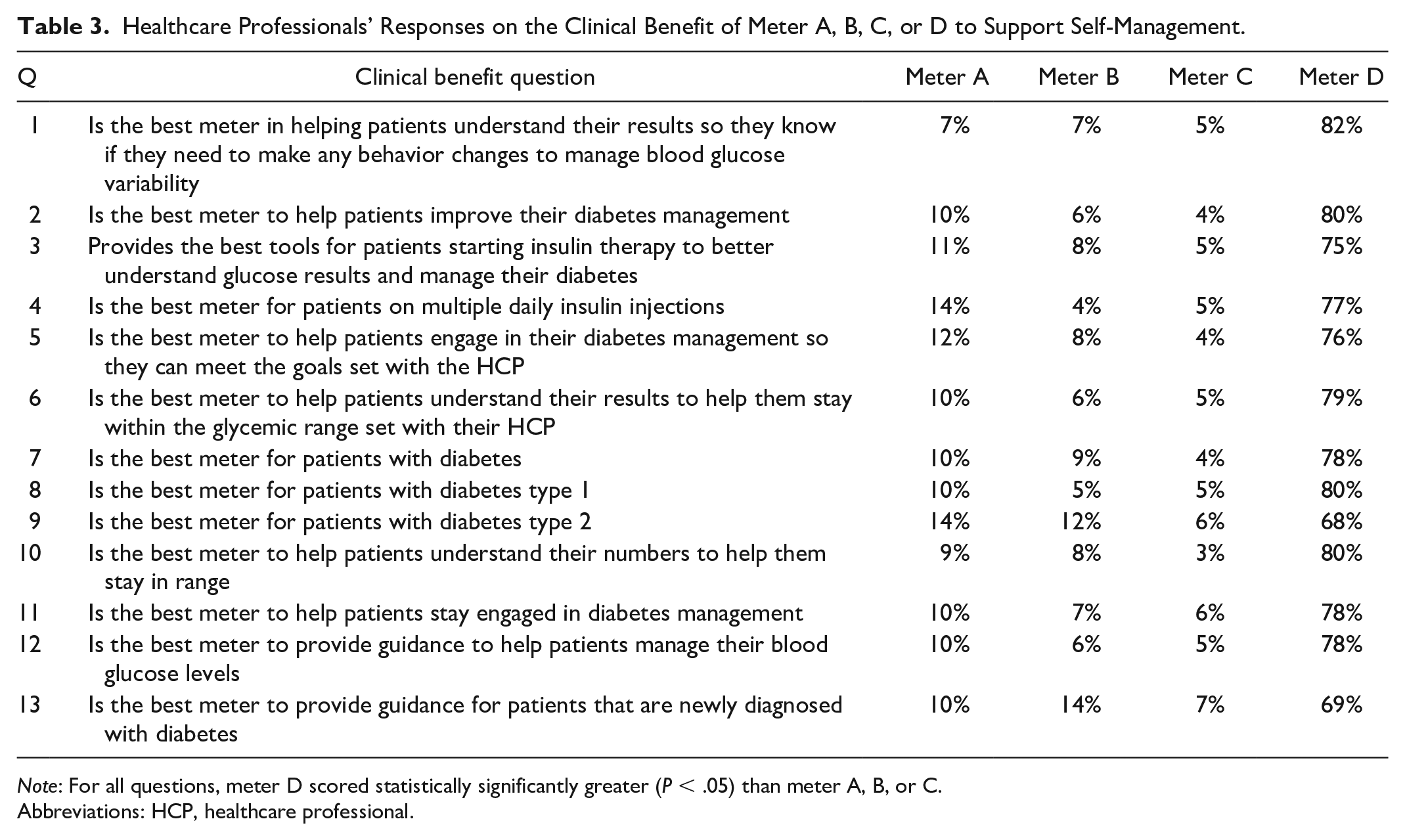
Note: For all questions, meter D scored statistically significantly greater (P < .05) than meter A, B, or C.
Abbreviations: HCP, healthcare professional.
Discussion
HCPs from five countries strongly identified one glucose meter in terms of assisting them to implement clinical guidance goals relating to patient self-management. Positive feedback for meter D was comparable across all five countries indicating that HCPs had similar views regarding the merits of this meter. Although all four meters were de-identified (in terms of branding), it is likely that many HCPs were familiar with meter screen images, especially for meters A, B, and C, given that these meters have been available for longer per country. By contrast, meter D had not yet been launched in the United States, was only recently launched in Canada, and had been available in France, Germany, and Italy only since 2019. However, despite arguably being the least familiar meter, it was interesting that the features and benefits of meter D resonated most strongly with HCPs.
Responses from DNs pertaining to how well meter D satisfied clinical guideline statements were significantly higher for eight statements compared to those of PCPs and significantly higher for three statements compared to those of endocrinologists. DNs, like endocrinologists, may be more familiar with diabetes guidelines since they engage in specialty diabetes services in comparison to PCPs who cater to a wider array of medical conditions including many patients without diabetes. DNs may also be more aware of the benefit of structured self-monitoring data, pattern analysis, and just-in-time insights and feedback to support self-management.2,16 For example, guideline question 10 (“Provides the best features/tools to help patients make connections between results and impact of nutrition, exercise, or medications”) tied for first place for DNs, which affirms their knowledge of the value of using structured data to make connections and learn from patterns of data to make modifications that can impact glycemic outcomes. Furthermore, DNs scored question 7 (“Provides the best tools to help patients on insulin therapy keep track of testing and to help motivate them to get back in range”) and 12 (“Provides the best tools to help patients understand their results so they can act to help them avoid hypo or hyperglycemic”) significantly higher than endocrinologists did. This may be due to the fact that DNs are the key team members to help patients identify and select an appropriate meter and are the primary HCPs to customize and configure meter features, train patients on meter usage, and collaborate on ongoing use of data to modify behavior and treatment. 17
With respect to clinical benefits that support actionable goals for self-management, meter D ranked higher than the other 3 meters, achieving 68% to 80% of first choice responses for all 13 clinical benefit questions including “best meter in helping patients understand their results,” “best meter to help patients improve diabetes management,” and “best meter to help patients understand their numbers to help them stay in range.” Despite meter D scoring significantly higher on every benefit question (the nearest meter scoring only 7%-14%), it scored slightly lower when applied to patients with type 2 diabetes (68%) or newly diagnosed patients (69%), potentially reflecting a stronger guideline focus on prevention of hypoglycemia and support for individuals on insulin therapy. We would argue that all individuals with diabetes, and especially those newly diagnosed, can benefit from advanced meter features while they are learning how to identify when glucose values are in range, above range, or below range. 18 Specifically for meter D, the dynamic color range indicator (DCRI) could help newly diagnosed patients associate results with information (eg, green meaning results are in range) and gain knowledge about how to use such insights to make health decisions. 19
Meters D and A provide more guidance, support, and real-time advice screens than the other two meters in the study. However, the usage of color screens, DCRI, and variety and clarity of the blood sugar mentor (BSM) messages seem to have resulted in far higher appeal for meter D. A prior home experience study with meter D in people with type 1 and type 2 diabetes found that 73% agreed the BSM provided deeper insights into their results and 71% agreed that the BSM advice and supportive tips would help them achieve more results in range. 20 Additional reports have shown that meters with a color range indicator similar to meter D improved patient decision-making 21 and glucose range interpretation.22,23 In terms of glycemic outcomes, there is also ample evidence that advanced meters with color range indication significantly improve A1C24,25 and additionally this A1c benefit was also observed when meters with color range indicators were directly compared to a variety of current meters (without color range indicators) in a randomized controlled trial. 26
Advanced meter features that analyze patient data to algorithmically tailor education and generate feedback for the patient and healthcare team can create a technology-enabled feedback loop to support individual care plans and improve diabetes outcomes. 27 Continued innovation in the area of glucose meters remains critical to provide HCPs with on-board meter features that can be customized and targeted to a broad range of patients. DNs are key team members to identify the appropriate meter for individual patients and configure meters to address individual patient goals. 17 When advanced meters are connected to medical software and apps, the opportunity for telemedicine and for remote monitoring between healthcare site visits exists.12,24,28 Widespread CGM access and adoption remains lower in the PCP environment than in specialty clinics 29 and therefore more advanced meters, like meter D, could be used as a stepping stone to future CGM, ensuring that patients first gain the essential skills and confidence before embarking on CGM.
Limitations
Although representative of North America and Europe, HCP perceptions may not be generalizable to countries beyond those studied. Participants were selected who routinely used glucose meter data for treatment decisions and therefore they may have been more receptive or familiar with the benefits of more advanced meters. The four meters selected, although representative and demonstrating a wide range of functionality, are not the only meters available.
Conclusion
After reviewing a selection of meters in terms of their ability to support HCPs to deliver upon selected self-management goals within clinical practice guidelines, HCPs strongly and routinely identified meter D (OneTouch Reflect) as their preferred meter to help them achieve the goals outlined within such guidelines.
Footnotes
Acknowledgements
The authors thank Ipsos, Parsippany, NJ, for the creation of webpages and HCP recruitment.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: DAG is a consultant for LifeScan Diabetes Institute and served as a clinical advisor for the study; MG is an employee of LifeScan Scotland, Ltd.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by LifeScan, Inc.