
Abstract
Excessive stress on plantar tissue over time is one of the leading causes of diabetic foot ulcers among people with diabetic peripheral neuropathy. Plantar tissue stress (PTS) is a concept that attempts to integrate several well-known mechanical factors into one measure, including plantar pressure, shear stress, daily weight-bearing activity, and time spent in prescribed offloading interventions (adherence). Despite international diabetic foot guidelines recommending the measure of each of these individual mechanical factors in people with neuropathy, only recently has technology enabled their combined measurement to determine PTS. In this article we review the concept of PTS, the mechanical factors involved, and the findings of pivotal articles reporting measures of PTS in people with neuropathy. We also discuss key existing gaps in this field, including the lack of standards to measure and report PTS, a lack of practical solutions to measure shear stress, and the lack of PTS thresholds that may indicate benefit or detriment to people with neuropathy. To address some of these gaps, we propose recommended clinical and research standards for measuring and reporting PTS in people with neuropathy. Last, we forecast future clinical, research, and technological advancements that may use PTS to highlight the importance of this critical concept in the prevention and management of diabetic foot ulcers.
Diabetic foot ulcers (DFUs) are a leading cause of global hospitalization, amputation, disability, and death.1-3 It is estimated that 20 million people worldwide currently have a DFU, with a further 130 million at risk of developing a DFU due to having diabetic peripheral neuropathy.1,2 The most common pathway to developing a DFU is via excessive mechanical stress on insensate neuropathic plantar tissue.1,4,5 If mechanical stress remains excessive, it results in subdermal trauma, inflammation and eventually a DFU will develop.1,4,5 Unfortunately, neuropathy not only results in the inability of the individual to detect excessive levels of mechanical stress, but can also cause gait abnormalities and foot deformities that further elevate mechanical stress levels.1,4-6
A better understanding of mechanical stress in DFU is therefore considered critical to improving the prevention and management of DFU. Until recently, few studies had attempted to comprehensively investigate mechanical stress in people with neuropathy.7-9 In this article we review and discuss the critical mechanical stress concept of plantar tissue stress (PTS), the individual mechanical factors that contribute to PTS, pivotal studies investigating PTS in people with neuropathy and key existing gaps in this field. We then propose recommended clinical and research standards for measuring and reporting PTS in people with neuropathy, along with forecasting future clinical applications, research and technological advancements that may be possible using PTS to highlight what is a critical global concept in the prevention and management of DFUs.
The Concept of Plantar Tissue Stress
We generally define PTS as “the accumulation of all mechanical stresses on an area of plantar foot tissue from all weight-bearing activity over time.” PTS is typically accumulated over days, highly influenced by footwear conditions and predominantly made up of the interplay of the following individual mechanical factors: vertical (normal) pressure (“plantar pressure”), horizontal pressure (“shear stress”), and the frequency of application of these pressures (“weight-bearing activity”)7-9 (Figure 1).
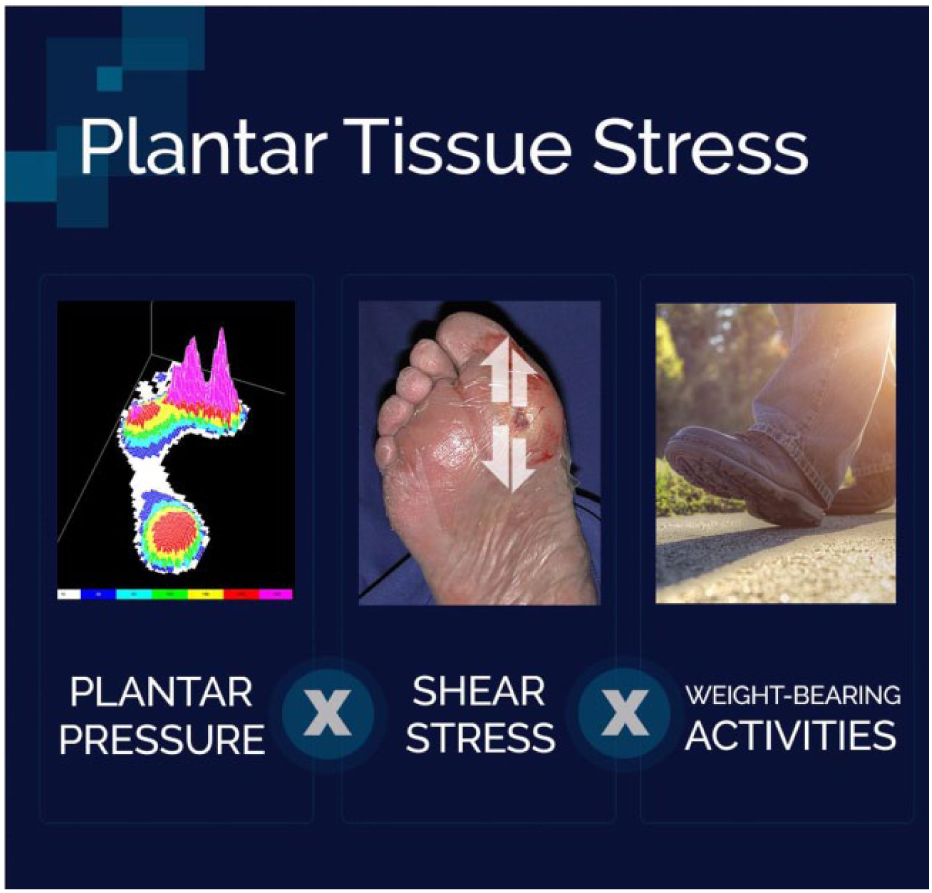
The concept of plantar tissue stress.
For well over 50 years clinicians and researchers have been attempting to measure and modify the individual mechanical factors that make up PTS in people with neuropathy.10,11 Historically, these attempts were based on subjective clinical judgements to guide pressure reduction or “offloading” treatments to try and reduce PTS and in turn prevent or heal DFUs.10,11 Over the last 20 years, these clinical judgements have been augmented by knowledge from objective measurements demonstrating the capacity of various footwear and offloading devices to reduce plantar pressure in controlled research settings.12-16 More recently, high-quality studies have gone further and demonstrated that objective clinical measurements of plantar pressure can be used to successfully guide clinical treatment decisions for prevention.17,18 This has led to international guidelines recommending that clinicians should objectively measure plantar pressure to guide the prescription of their footwear-related offloading treatments to prevent DFUs.5,19,20 Although measuring and modifying one individual mechanical factor at one moment in time has proven clinically beneficial, it is still far from a complete representation of a person’s entire PTS profile.
As technology has become more user-friendly, less expensive and more accurate, the ability to simultaneously measure the individual mechanical factors comprising PTS has become more achievable.8,9 Some studies have attempted to combine multiple individual mechanical factors to estimate PTS levels and report some interesting differences in PTS levels between subgroups with neuropathy.7-9 Although promising, these results were performed using different definitions and methodologies for estimating PTS.7-9 As no standards for measuring and reporting have been defined to date, there is an urgent need for standardization in measuring and reporting PTS if we are to progress this critical concept of diabetic foot management. Before attempting to address this gap and recommend standards for PTS, a base level of understanding of each of the individual mechanical factors involved in PTS is required. Thus, we will first discuss the factors of plantar pressure, shear stress, weight-bearing activity and adherence to offloading interventions designed to modify these factors.
Individual Mechanical Factors That Make Up Plantar Tissue Stress
Plantar Pressure
Forces that act on the foot when a person is weight-bearing are largely defined by body-mass, walking speed and footwear conditions. Ground reaction forces are measured as resultant forces of foot progression during gait. The distribution of these forces over the plantar foot surface is measured as pressure, defined as the force divided by the contact area of the foot. Plantar pressure (also called “normal pressure”) is the pressure applied perpendicular to the plantar surface.
The clinical importance of plantar pressure measurement was first shown by Dr Paul Brand during the 1960s, in people with leprosy and later in people with diabetes.10,11 Dr Brand did this using individual pressure sensors applied to different regions of the foot.10,11 This created the concept that “pressure is the harm done by the forces acting on the foot”, because these neuropathic patients showed skin lesions at locations of high pressure.10,11 This “high plantar pressure” concept has since been supported by many risk factor studies on DFU and its recurrence.8,21
Plantar pressure is typically measured with either a pressure platform, an insole system or with individual pressure sensors. Both the platform and insole systems contain a matrix of sensors providing a measurement of the pressure distribution across the area of contact. Many different systems are available to measure plantar pressure distribution and they vary greatly in terms of sensor technology (eg, capacitive, force resistive), single sensor or sensor matrix, spatial resolution of the sensors, sensor thickness, sample frequency, and other technical properties. The peak plantar pressure at a given location over the duration of stance during gait is the most reported pressure outcome, as it has been shown to be best associated with clinical outcome.15,22,23 Alternative plantar pressure parameters used are peak pressure-time integral (area under a pressure vs time plot) and the average plantar pressure.
In people with neuropathy, peak plantar pressures can be high because of foot deformity, gait changes or changes in plantar soft tissues that increase pressure and decrease shock absorption.1,6 Peak plantar pressures are typically highest in the metatarsal regions and the hallux. 6 Plantar pressures during barefoot walking on a pressure platform are mostly used to define the risk of DFU, whereas in-shoe insole systems are used to evaluate the pressure-relieving properties of footwear and other pressure-reducing offloading interventions.15,24 Recently, both barefoot and in-shoe plantar pressure measurements have been applied successfully in the design and optimization of therapeutic footwear to prevent DFU in patients with DFU history.17,18,25-28 These measurements are now recommended in international guidelines.5,19,20 Through these mechanisms, plantar pressure measurement is becoming more integrated in clinical practice to prevent DFU recurrence.
The strengths of plantar pressure assessment are its ability to quantify a modifiable risk factor for DFU in people with neuropathy, and to quantitatively evaluate the impact of pressure-relieving interventions. This has similar fundamental clinical importance in patients with neuropathy as does the monitoring of blood pressure in patients receiving treatment for hypertension. A limitation is the large variation in measurements both within and between available plantar pressure measurement systems, and differences in the quality and technical specifications of these systems, which limits the comparison of measurements using different systems. 29 Thus, it is recommended to use a valid system that can be calibrated with known accuracy. Another limitation is that plantar pressure is only one of the mechanical factors contributing to PTS.
Shear Stress
Pressure has multiple directions and magnitudes. Shear stress acts horizontally to the contact surface, is typically due to friction, and consists of medial-lateral and anterior-posterior forces. For several decades shear stresses has also been implicated in DFU development.25,30-35 However, it has remained an obscure and often misconstrued subject in the field.
Peak shear stress and peak plantar pressure often do not occur at the same location or time.36-38 For example, medial-lateral shear tends to straddle the peak plantar pressure location and time, 36 whereas anterior-posterior shear occurs in opposite directions and at different locations depending on the phase of gait. 36 These differences between locations and times of peak plantar pressure and peak shear stress may partly explain why only a proportion of DFUs occur at sites of peak plantar pressure 39 and how shear stress may account for DFUs at “unexpected” sites. 40
Shear stress also affects both the deep and superficial soft tissues in people with neuropathy, where elastic and viscoelastic properties yield tissues that are stiffer yet also quicker to relax compared to non-neuropathy counterparts. 41 Although theoretically materials designed to reduce friction between the plantar skin and the footwear surface should reduce the impact of shear, as demonstrated by reductions in skin temperature 42 or reduced shear-forces, 43 this has yet to be demonstrated in prospective studies measuring shear stress.
The main difficulty with shear stress though is the significant technical challenge required to properly validate and calibrate measuring systems that can accurately quantify shear. Such systems are inherently predisposed to cross-talk as they typically require an array of flexible sensors and from a practical point of view are very difficult to calibrate due to the different directions in which shear force acts. However, considerable efforts have been invested in trying to develop systems and sensors capable of measuring shear stress, with limited and varying results. 44 The types of sensors developed have included magnetic-resistive based transducers,35,45 strain gauge systems,46,47 optical methods,48,49 tri-axial piezoelectric transducers, 50 capacitive microsensors, 51 microstrip antennas, 52 and surface stress sensitive film-based devices. 36 Like plantar pressure measurement, there are also many differences between the various types of shear stress measurement modalities developed which result in further significant challenges when interpreting results across different studies, as magnitudes as well as locations can vary greatly. 44 Thus, currently there is no valid commercially available in-shoe shear stress measurement device and no gold standard method of measurement that has overcome the significant technical challenges of measuring shear. 25
Given the paucity of commercially available devices, several researchers have focused on developing surrogate markers for measuring shear stress, such as using horizontal and anterior-posterior components of ground reaction force,43,53 algorithms to convert conventional plantar pressure data into surrogate shear outcomes (such as peak pressure gradients),54-56 and thermometry.57,58 Perhaps the most clinically promising of these surrogate markers is the thermal stress response. Temperature changes in response to walking may be monitored using either thermography, insoles, or flexible sensors (eg, smart socks).57-61 These methods assume that increases in shear stress will increase thermal stress responses.60,61 Such approaches can measure short-term acute increases in regional skin temperature of the foot in response to number of steps taken or in comparison to the same regions on the contralateral foot.42,58,59,62 These short-term acute temperature increases have been found to be correlated with the magnitude and locations of shear stress measured by research modalities (Figure 2).58,60
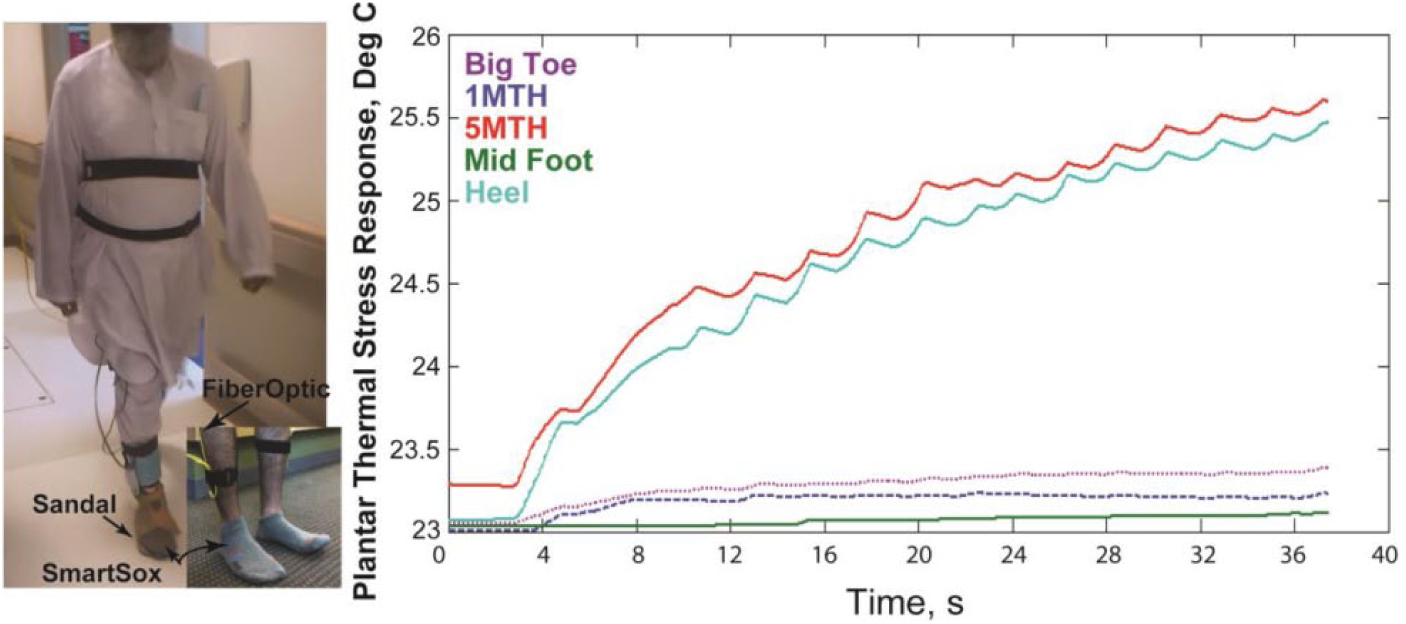
Example of plantar thermal stress response measurement showing short-term acute increases in regional skin temperature in response to shear when walking for 40 seconds.
Although some methods of measuring shear stress are promising, as discussed all methods should be considered within the context of their limitations. Many of the developed sensors lack adequate spatial resolution, are prone to structural, mechanical and thermal damage, and are sensitive to ambient temperature-related errors. 44 Furthermore, not all methods can be safely used inside footwear conditions and there is no consensus on what constitutes a high shear stress threshold. A limitation of using surrogate shear markers, such as ground reaction force data, are that they are incapable of being completely representative of localized mechanical stress as the pressure effect is dependent on the area over which the force acts. 53 Other algorithm-based markers are reliant on the assumption that peak shear stress is focused around the site of peak vertical pressure. Although some level of plantar pressure is fundamental to generating some level of shear, as discussed earlier, this does not automatically translate to the locations of the peak plantar pressure and the peak shear stress being at the same location. 34 Thermometry, whilst arguably the most promising surrogate marker, is still limited by the fact that there are also multiple factors that may increase skin-temperature besides shear stress.25,58
Weight-Bearing Activity
Unless a person steps on a foreign body such as a sharp stone, the plantar pressure and shear stress encountered in a single step are generally not of great enough magnitude to develop a DFU. Thus, PTS is further made up of the frequency with which plantar pressure and shear stress are applied. As such, a person’s weight-bearing activity should be considered when measuring PTS.
Early studies investigating weight-bearing activity in patients with neuropathy were dependent on participants self-reporting this outcome. 63 Such self-reporting suffers from both intentional and unintentional errors in reporting. 63 Subsequent studies have overcome this limitation by using computerized pedometers or accelerometers that objectively monitor patients’ daily step or stride counts.8,64-66 With advances in signal processing and multisensor devices, it is now possible to more comprehensively monitor activity, beyond simply counting steps. This includes total weight-bearing activity, bouts of weight-bearing activity and intensity of such activity.63,67,68 One such study found that people with neuropathy spent approximately twice as much weight-bearing time per day standing as they did walking, whereas another found daily standing time may be predictive of healing DFU.69,70 An additional recent advancement in objective activity monitoring has been the synchronous collection of location and activity data using global positioning system monitors. 67 This type of activity monitoring shows promise in providing a richer insight into not only daily activity, but also how one’s environment influences their weight-bearing activity behaviors. 67
Remaining challenges for activity monitoring include the collection of accurate data of specific weight-bearing activities. This is because each weight-bearing activity (eg, standing, walking at different speeds, turning, standing up from a chair) may have different plantar pressure patterns, and as such varying PTS values. Another challenge is the collection of data on gait variability, consistency or shuffling gait, and investigations in their relations with DFUs. A crucial and even more difficult challenge lies in the potentially complex relationship between daily weight-bearing activity and DFU. Where some studies have reported a higher level or variability in weight-bearing activity over time in people who develop DFUs, 64 others have opposing findings,8,68 but both may be true. It is likely that the risk of DFU in such studies was dependent on the overall PTS rather than daily activity alone. Regular engagement in weight-bearing activity may also lead to greater stress tolerance in the plantar skin. This is described as the “physical stress theory.” 71 Historically, exercise guidelines for persons with neuropathy recommended avoiding weight-bearing activities to prevent DFU. However, more recent guidelines suggest such individuals may participate in “moderate” weight-bearing activity without increasing their DFU risk. 72 Like concepts in the training of athletes to reduce their risk of injury, the “physical stress theory” suggests regular, stable and gradually dosed weight-bearing exercise could also reduce the risk of DFU. This is an important area for future research.
Finally, all activity monitoring research is dependent upon individuals wearing activity monitors. Although researchers and clinicians have sought to force adherence through limiting patients’ ability to remove such monitors with some success, means for monitoring patient adherence with monitors are being developed to identify periods when activity monitors were not worn, such as data processing rules and integrating thermal sensors with activity monitors. 68 The next section will further discuss the important implications of measuring adherence, but this time with therapeutic footwear and other offloading interventions.
Adherence to Offloading Interventions
Adherence to wearing offloading interventions (eg, footwear, walkers, casts, etc) to reduce mechanical stress has been found to improve outcomes, since such offloading devices can only be effective when they are worn.73,74 Based on definitions by the World Health Organisation, 75 we suggest the following definition for adherence to wearing such offloading interventions be used, “the extent to which a person is adhering to wearing a prescribed offloading intervention while weight-bearing.” Measuring wearing time alone is not a sufficient metric for adherence, as some patients may be very active when they do not wear their device (and experience very high PTS) while others may be mostly sedentary when they do wear their device (and experience very low PTS). Thus, adherence should be measured with a sensor in the offloading device that registers wear time and synchronized with a sensor on the person that registers weight-bearing activity.
Adherence should also be measured quantitatively. 66 This has already been performed successfully for custom-made orthopedic footwear17,65 and removable cast walkers, 76 and thus such measurements should be feasible in any footwear and offloading device condition. When both wear-time and weight-bearing activity are captured, adherence can be expressed as the percentage of total weight-bearing activity (eg, number of steps, number of bouts, etc) while wearing the device. When PTS measurements are available both in and outside an offloading device (as described in the next sections), adherence may also be expressed as the percentage PTS while wearing the device of the total PTS experienced. In line with research on valid periods for weight-bearing activity monitoring, it is recommended to also measure adherence over a one-week period, 77 with four days (including one weekend day) being adequate to obtain reliable information on a person’s total activity. 77
Strengths of such a method of measuring offloading treatment adherence in this context are that such objective adherence measures are already available, and have potential to visualize results for patients. A limitation is the need to use a minimum of two sensors of which the outcomes need to be synchronized, thereby requiring extra computational power and time (if the synchronization of data occurs post data collection). The need to use an activity sensor on the patient is also a limitation, as these sensors generally only have the battery power to store up to two weeks of activity data. Further, people can choose not to “adhere” to measuring weight-bearing activity by removing these sensors. Clinically, objective measurement of adherence is already a promising tool to evaluate clinical care in offloading and to inform patients to the benefits of being adherent. With the large effects of adherence demonstrated on DFU outcomes,1,73,74 quantitative adherence measurements are recommended to be included in every trial and daily clinical practice and incorporated into any overall measure of PTS.
A significant gap in the field is the lack of practical and effective solutions to improve adherence to prescribed footwear and offloading devices in neuropathic patients.76,78,79 Few studies have explored the benefits of technologies for improving adherence to these treatment devices in people with diabetes. 80 Najafi et al 81 suggested that using a gamification approach for monitoring and real-time notification of prolonged foot loading condition, via a combination of smart watch and smart insoles, is effective for improving footwear adherence over time, while Keukenkamp et al found some potential for motivational interviewing based on objective adherence measurements. 79 Further studies are still required to determine effective and practical technical solutions to improve adherence to prescribed offloading devices.
Combined Measurements of Plantar Tissue Stress
As each of the above individual mechanical factors have been demonstrated to individually affect DFU development and healing, there is strong rationale for the need to investigate them in combination to see if an overarching PTS measure has an accumulative effect on DFU development and healing.7-9 For a variety of (mostly technological) reasons, very few studies have attempted to estimate PTS in people with neuropathy. These few studies have typically been limited to pairing a measure of plantar pressure with a measure of weight-bearing activity.7-9
The first such study in people with neuropathy was performed by Maluf and Mueller, who combined plantar pressure magnitudes with daily weight-bearing activity volume in their participants. 7 They calculated PTS as the product of the mean in-shoe pressure-time integral measured in a research laboratory setting by the mean daily step count over seven consecutive days in the patient’s everyday environment. Interestingly, they found participants with a DFU history had significantly less forefoot PTS than controls. The authors hypothesized that people with a history of DFUs may have deconditioned their PTS tolerance through limited engagement in weight-bearing activity, thus aligning their findings with their earlier described “physical stress theory” hypothesis. 71
Maluf and Mueller’s methodology was subsequently adopted in a study investigating PTS in populations with active DFU. 9 This study by van Netten and colleagues was an exploratory study of 31 participants with active DFU from a larger randomized controlled trial assessing healing efficacy of removable offloading devices. 9 Although this study’s results failed to yield statistically significant differences, it did find moderate to large effect sizes regarding higher PTS in those with poor healing outcomes. They hypothesized that prolonged elevated PTS results in prolonged healing times, and thus, PTS needs to be reduced as much as possible.
A refined methodology for calculating PTS was used by Waaijman and colleagues in their investigation of risk factors for DFU recurrence. 8 They investigated plantar pressure in both prescribed therapeutic footwear and barefoot conditions in people with a DFU history. During the one-week activity monitoring period, adherence to the prescribed therapeutic footwear was also quantitatively assessed. They calculated PTS as the product of the mean in-shoe pressure-time integral by the mean daily strides when adherent to the therapeutic footwear, summed with the barefoot pressure-time integral by mean daily strides when not adherent to the therapeutic footwear. Based on this method, they did not find PTS predictive of DFU recurrence; however, the authors noted that further refinement of these methods was needed in these populations. 8
Although these studies build nicely on the combined measurement of individual mechanical factors and have reported promising findings using estimated PTS, limitations remain. The overarching limitation is the inability to continuously measure PTS in free-living conditions. Current measures rely on assumptions to be factored into calculations of PTS. These assumptions include a single mean plantar pressure measurement in one footwear condition being representative of plantar pressure for all steps in free-living environments, mean daily steps being representative of all weight bearing activity in free-living environments, a one-week period of daily activity measurement being representative of all daily activity over time, and a limited influence of shear stress on PTS.7-9 These assumptions, along with different methodologies used by all authors to measure these individual factors and calculate PTS are likely to be a source of unaccounted confounding in studies to date.
Although there have been limitations identified, there are also many strengths. These include using the individual mechanical factor measures that have been identified to be associated with DFU outcomes in people with neuropathy, early findings of estimated PTS differences in important neuropathic populations in most studies, ability to measure PTS in different footwear conditions (by using adherence measures), improvements in technology that allow synchronization of measures for longer durations, and the potential to add in surrogate measures for shear stress that haven’t been included in PTS measures to date.7-9
Therefore, along with authors that have used PTS, we believe there is significant merit in pursuing a measure of PTS that is representative of free-living PTS in populations with neuropathy. However, consensus on the standards required to appropriately measure and report PTS is lacking and urgently required. We introduce recommendations for such potential standards in the following section.
Recommended Standards for Measuring Plantar Tissue Stress
When attempting to measure PTS, it is important that valid and repeatable means of measurement are used. Strengths and limitations in this regard for the measures of plantar pressure, shear stress, weight-bearing activity, and offloading treatment adherence have been discussed in sections above. In this section, we propose recommended standards as agreed by all authors that in our opinion should be appropriate, reliable and feasible for the effective measurement and reporting of estimated PTS in people with neuropathy. Table 1 outlines specific sets of clinical and research standards that include the equipment, measurements and variables considered necessary to measure PTS. It should be noted with no available valid and reliable instrument to directly measure shear, we have omitted shear stress from our recommended standards. However, we do suggest that when shear measuring systems or surrogate shear markers are validated and commercially available then shear stress recommendations should be added to these standards in the future.
Recommended Standards for Measuring and Reporting Plantar Tissue Stress.
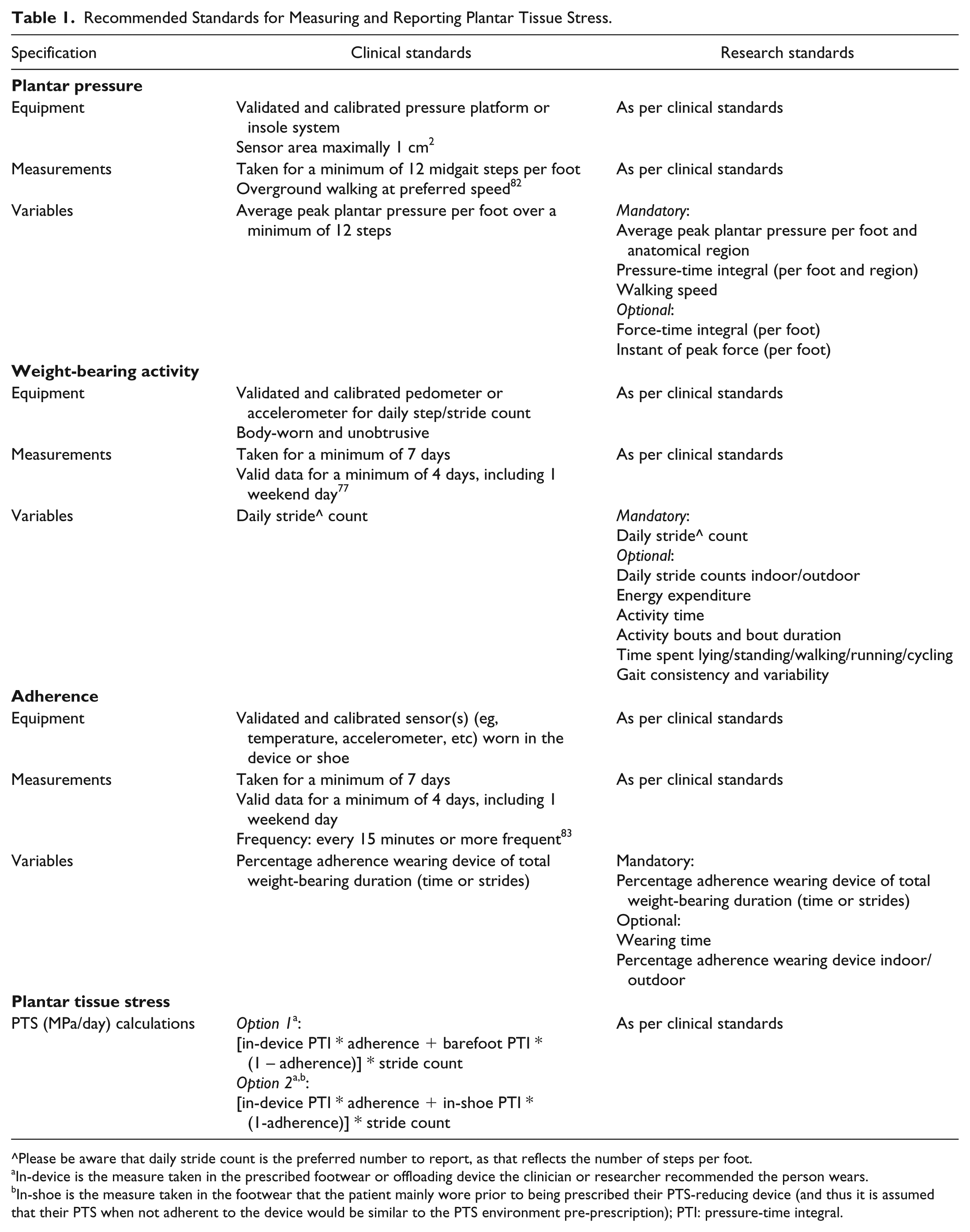
^Please be aware that daily stride count is the preferred number to report, as that reflects the number of steps per foot.
In-device is the measure taken in the prescribed footwear or offloading device the clinician or researcher recommended the person wears.
In-shoe is the measure taken in the footwear that the patient mainly wore prior to being prescribed their PTS-reducing device (and thus it is assumed that their PTS when not adherent to the device would be similar to the PTS environment pre-prescription); PTI: pressure-time integral.
The
The
We acknowledge that these clinical or research standards may not be feasible for all clinicians or researchers in the field. However, offering deviations from these standards, without supporting evidence, does not align with offering best clinical or research practice. We propose these standards as the basis for global discussion, debate, modification and eventual adoption by international groups in an attempt to accelerate our understanding of what is a critical measure in the prevention and management of people with DFU.
Future Directions
Clinical
As we identify above, our proposed recommended clinical standards are in large part already internationally recommended in guidelines,5,19,20 and we have simply extended these recommendations by adding our primary recommendation of calculating the combined PTS. Furthermore, these guidelines also recommend that adherence and activity should be measured and considered when prescribing footwear and other offloading devices.5,19,20 Thus, determining PTS should not only be already feasible, but will provide additional clinical value beyond that already obtained from determining those individual mechanical factors alone.
A calculation of PTS should enable clinicians to more comprehensively tailor personalized offloading treatment that inherently takes into consideration all individual mechanical factors known to cause or delay DFU healing. This extends current clinical practice that tailors offloading treatment for patients based on considering individual mechanical factors in isolation, such as plantar pressure at one snapshot in time. For example, a clinician with access to PTS measurements would be able to design innovative offloading strategies based on the reduction of PTS, and should more comprehensively understand their patient’s situation regarding their likely plantar pressures, shear stresses, activities and adherence over time. In future, instead of prescribing a “one-size-fits-all” approach of a knee-high offloading device for a patient with DFU, as currently recommended, such new personal PTS information could guide the patient to choose offloading interventions that best manage their day-to-day PTS and not just their plantar pressure at one point in time. Furthermore, the measurement of PTS may also provide useful future clinical benefits in the management of other conditions such as reducing deformity-causing high PTS levels in acute Charcot feet, planning surgical offloading or even amputation procedures to target the permanent reduction of PTS levels, and delivering more functional feet and other bodily parameters after orthopedic or bariatric surgery for example.
Research
Future research directions include validating and refining the assumptions underlying the PTS measurements, development of systems or modalities to better quantify shear stress, investigating the relation between PTS and ulcer development and healing, and studying the educational aspects of communicating PTS outcomes with patients.
Validating the assumptions as described in the section on the combined PTS measurement is vital, as that will provide the key to translate laboratory findings to real-world findings, without the need for patients to wear continuous monitoring devices. Or alternatively it will show that it is essential to combine lab-based and real-world measurements to accurately estimate PTS. The development of shear stress instrumentation is also important in this regard, as it will allow for the missing link to be added to our current PTS measurement recommendations.
Once validated, the association between PTS and ulcer development and healing needs to be further investigated in different clinical environments around the world. The natural extension to this is the determination of PTS thresholds that may predict DFU prevention or healing in longitudinal studies. Such thresholds would further enable clinicians and patients to objectively tailor their personalized offloading interventions at the initiation of treatment to fit within such thresholds, and researchers to design new innovative patient-centered offloading strategies based on addressing these thresholds. Only when joint research efforts in this topic are undertaken can we expect to obtain adequate power to understand PTS and its relationship with DFUs and inturn personalize clinical treatment advices based on these measurements.
Simultaneously, the educational aspects of PTS outcomes and their communication with patients should be investigated. Patients’ understanding of the concept of PTS needs to be examined before potentially successful educational interventions may be developed. Personalized treatment and feedback systems will need to align with patients’ understanding of the concept and need to be tailored to their health literacy levels. This is an important consideration as technological development always needs to consider the end user. Finally, additional instrumentation development priorities include the creation of sensors or sensor-systems capable of longer-term monitoring, with batteries that can be easily charged, limited need for calibration and systems that are small, easy to use, and with capacity to integrate with smart device applications.
Technological Advances
In light of the impending diabetes epidemic and the already high prevalence of neuropathy, the need for enhancing the prevention and management of DFU is clear. Fortunately, we live in a world where technology is increasingly being integrated into every aspect of our lives, representing an opportunity for creative solutions to prevent this devastating condition. However, the translation of these technologies toward the clinic is still in its infancy. PTS is a concept that lends itself to these technological advancements, and perhaps PTS could be used as the basis to initially integrate these technologies into the care of people with neuropathy.
Thanks to new “smart” sensors and communications technology, new opportunities have opened to measure and modify dosages of PTS with personalized screening and timely intervention. With the help of potential automated measurement of PTS, such as those in smart insoles, patients could have their PTS constantly monitored via machine algorithms and even be prompted to change their PTS level if it becomes too high or too low (eg, change offloading device, increase offloading wear, decrease (or even increase) steps per day, avoid prolonged standing, reduce day-to-day physical activity variation, etc), or alert them to dangerous levels of PTS via the use of smart phones and smartwatches (Figure 3).57,81,85-87 Furthermore, patients could transmit their PTS results to their health care professionals or their caregivers in real time to reinforce adherence and facilitate timely advice and interventions.85,87

Example of smart insoles used in Najafi et al study 81 that may in the future continuously monitor plantar tissue stress during everyday activities and provide real-time alerts to patients via smartwatches to reduce their plantar tissue stress to safe levels. Frequency of similar real-time alerts has already been shown to be beneficial to improve footwear adherence. 81
Efforts are required to empower patients and their caregivers via the provision of comprehensive and easy to execute feedback that can reduce negative impacts from PTS (eg, feedback about shoelace closure to minimize shear force, limit prolonged unbroken walking and standing, etc). A key challenge that needs to be addressed by future technology is personalization of thresholds for harmful PTS. For instance, as discussed above, the difference between tolerable safe doses of weight-bearing activities that may help prevent DFU and doses that may increase the risk of DFU or delay DFU healing remains uncertain and may be different in different people due to other factors, such as their degree of frailty or quality of their plantar tissue. It is likely that many different factors may impact the risk of DFU in different patients and hence we will continually need to be cognizant of these factors, and perhaps integrate machine algorithms, so we can properly personalize offloading interventions in the future based on tolerable or harmful ranges of PTS experienced by the individual patient. 64
Conclusion
Plantar tissue stress is an increasingly recognized critical factor in DFU development and healing in people with neuropathy. We hope that the proposed standardized measurement, reporting and future directions described in this article will benefit clinicians today and serve as a starting point for more high-quality research into this critical concept that may just shape the global prevention and management of DFU into the future.
Footnotes
Acknowledgements
Abbreviations
DFU, diabetic foot ulcer; PTI, pressure-time integral; PTS, plantar tissue stress; 1MTH: first metatarsal head; 5MTH: fifth metatarsal head; s, seconds.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The contents of this article were developed in part with the support of an Innovation Grant from The Prince Charles Hospital Foundation, Australia (TPCHF Grant INN2018-41). The contents are solely the responsibility of the authors and do not necessarily represent the official views of the granting body.