
Abstract
Objective:
Areas of the foot with diabetic ulcers have been observed to have greater plantar pressures compared to non-ulcerated. Pressures play an essential role in the mechanism of lesion, and their reduction is effective in prevention. We conducted a systematic review to evaluate pedobarography as a predictive tool for ulcer development, since there is still no consensus on this aspect.
Methods:
We searched PUBMED (MedLine), EMBASE, Scopus, Web of Science, CINAHL and Scielo for cohort studies that measured plantar pressure at baseline and verified ulcer development on follow-up. Pooled effects of accuracy, sensitivity, specificity and relative risk were calculated using the inverse variance method. Risk of bias was assessed using the QUADAS-2 tool.
Results:
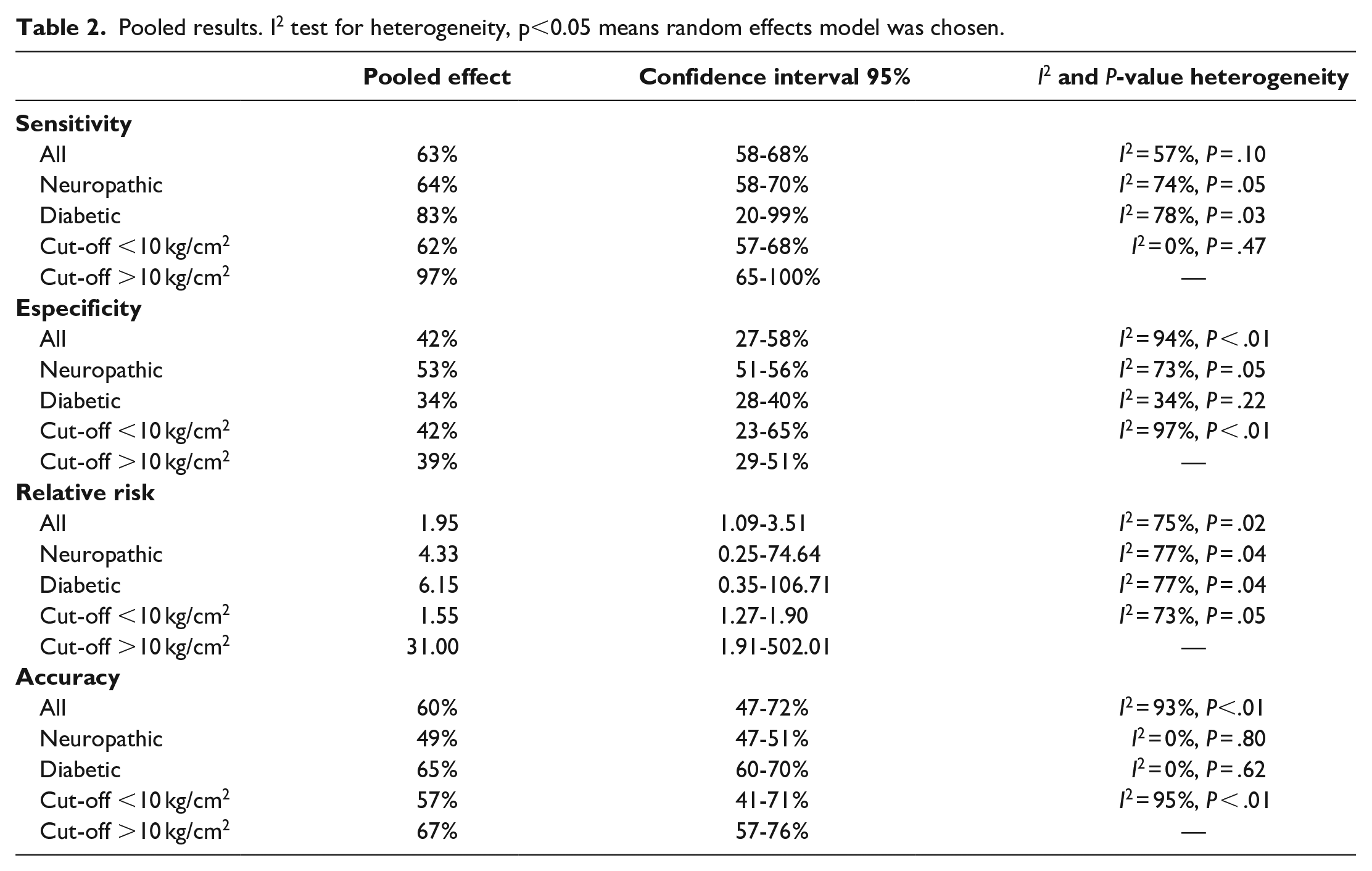
Three studies (n = 2000) had enough information on accuracy to be included into a meta-analysis, and 4 (n = 2651) were analyzed using qualitative methods. Pooled sensitivity and specificity were found to be 0.63 (Confidence Interval (CI) 0.58-0.68) and 0.42 (CI 0.27-0.58), respectively. Pooled relative risk was 1.95 (CI 1.09-3.51). Risk of bias was low to uncertain.
Conclusions:
Pedobarography in itself appears to have low accuracy in evaluating risk of ulceration. Several methodological heterogeneities were found, and the most optimal cut-off value is yet to be determined.
Introduction
Globally, there are around 463 million people diagnosed with Diabetes Mellitus (DM). 1 Among its well-established chronic complications, diabetic foot ulcers are an important factor to scan for. These are caused by a multifactorial process mainly associated with small repeated traumas, foot deformities and lower-extremity neuropathy, responsible for loss of protective sensations. 2 Neuropathy also may cause musculoskeletal dysfunction and affect skin integrity, increasing risk even further. 3 Transversally, the global prevalence of ulcers in the population with DM was reported as 6% in a recent study, 4 but other estimates indicate that, during their lifetime, 19% to 34% of these people may be affected by these lesions, to some degree. 5 Diabetic foot ulcers are the main cause of non-traumatic amputations. 6
Studies have proposed a myriad of tests to assess risk of ulceration. Quantifying and mitigating stress cycles and sites of pressure is important for risk management, before, during, and after ulceration. 7 Pedobarography has emerged as a promising method of finding areas subject to stronger forces during gait. In the last 20 years, evidences have associated neuropathy degree with higher peaks of plantar pressure, and consequently, higher risk of ulceration. 8
The kinematics of the diabetic foot have been thoroughly described, 9 and other systematic reviews have addressed the role of plantar pressure on the natural history of ulceration, 10 but none have so far compiled these data in a review with meta-analysis. There is still no consensus on both the accuracy of this test and the optimal cut-off value to categorize risk, associated or not with neuropathy. In that context, the present study aimed to fill those gaps, finding the predictive value of pedobarography in subsequent ulcer development in patients with DM and neuropathy, through a systematic review of cohort studies.
Methods
The pooled effects were estimated using the inverse variance method for proportions and binary outcomes. Heterogeneity between studies was verified with the I2 test, being considered significant when P < .05. Alternative hypothesis for the was whether this variability was significant, and so the models of fixed effect or random effect were chosen based on acceptance or denial of the null hypothesis. All analyses were done in the R environment 11 with the “meta” pack. 12
Results
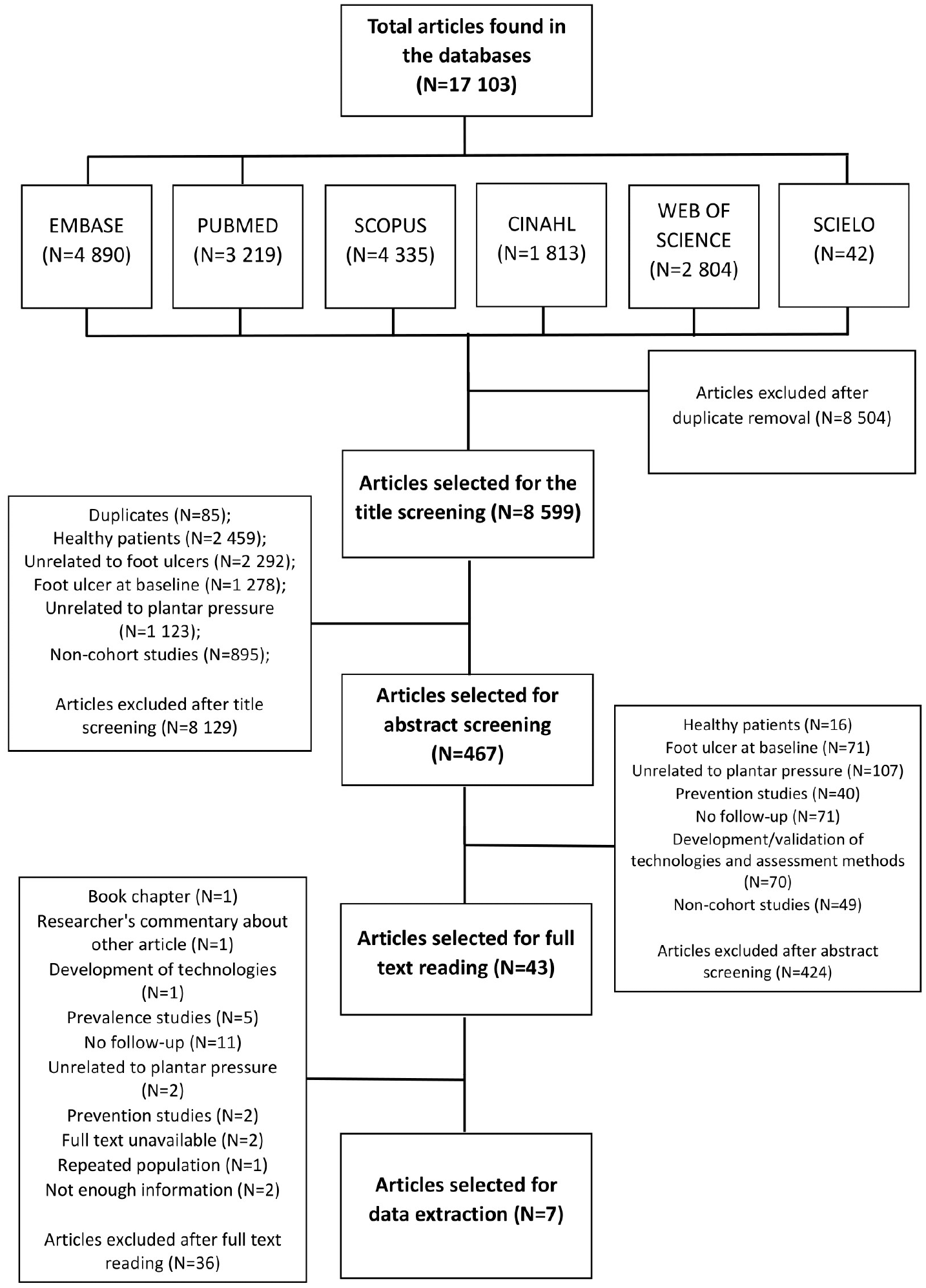
Flowchart of the study search.
Of the 36 remaining works, 1 was a book chapter; 1 was a researcher’s commentary about another pre-existing study; 9 described the development of technologies for assessment of plantar pressure; 5 were cross-sectional studies that verified the prevalence of foot ulcer; 11 were cross-sectional studies that associated plantar pressure to previously active or healed foot ulcers; 2 studies associated foot ulcer to other tests (1 to a Semmes-Weinstein monofilament and 1 to shear stress); 2 were experimental studies on ulcer prevention through reducing plantar pressure; 2 were congress abstracts or early reports, of which we couldn’t find any published article or complete results; 2 full texts could not be found; finally, one study 13 was excluded due to the use of the same patient sample in the same period as another 14 ; as the main goal of the former was to determine the accuracy of a new index (forefoot/rearfoot) and patient’s data were classified in subgroups, we considered the latter as more adequate to the context of our analysis.
Details from each selected study
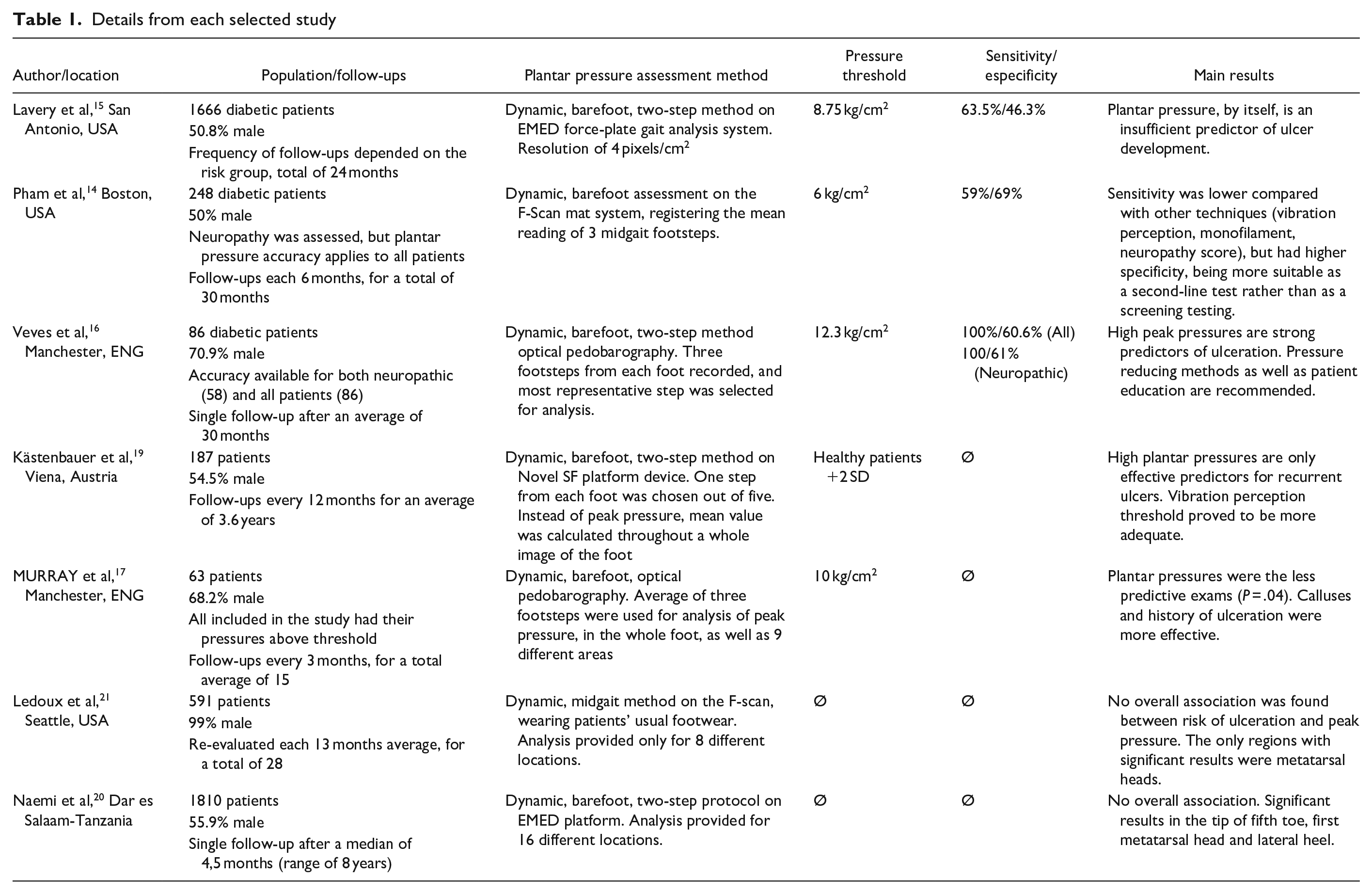
Lavery et al 15 monitored a total of 1666 patients and obtained the value of 8.75 kg/cm2 as their optimal cut point (63.5% sensitivity 46.3% specificity). That accuracy was obtained after removing patients with normal Semmes-Weinstein monofilament test. Hence, it is only related to neuropathic patients.
Pham et al 14 observed 248 patients for a variety of risk factors, and perceived plantar pressure as one of the least accurate tests to predict the development of foot ulcers. In this study, no subgroup analysis was made; therefore, its accuracy is applied to all the patients with DM, and not only to the neuropathic group.
Veves el al 16 observed 86 patients, which were classified according to a neuropathy score. Though values were not informed, enough data was described in the text so that we could calculate data for both diabetes and neuropathy meta-analysis. This study utilized a higher cut point of 12.3 kg/cm2, with 100% sensitivity for both groups, meaning all ulcerated patients were above the cut point at baseline.
Murray et al 17 conducted a study with the main objective of quantifying the influence of callus formation in ulceration, but also observed plantar pressure. One inclusion criteria was patients that had at least one region with the peak plantar pressure above 10 kg/cm2. Hence, patients with healthy plantar pressure were not available. As we couldn’t calculate the accuracy, this study was left out of our meta-analysis. It is important to highlight that the calluses were sanded before the assessment, which could have masked areas with high plantar pressure, as explained by Young et al. 18 Similar procedures were not described in other cohorts. Association between plantar pressure and foot ulcers was one of the lowest in the study (RR = 4.7), but if we take those calluses into consideration, that risk could be higher than reported. Of the 6 patients that ulcerated, 5 had a previous history of foot ulcer, which can also be an important confusion variable.
Kästenbauer et al 19 followed 187 patients for a mean period of 3.6 years and observed a variety of factors like vibration perception threshold, plantar pressure and daily ingestion of alcohol as important predictive factors for ulceration. Although the authors collected pressure data for 5 different steps for each participant, their analyses focused on a single step for each participant. On these single steps, authors calculated mean pressure of all points in 8 different areas of the foot. If mean pressure in at least one area was higher than a healthy control group, they were considered elevated. The heterogeneities in peak pressure measurement, lack of cut-off value and of information on TP, FP, TN, FN, lead us not to include the study in our meta-analysis.
Naemi et al 20 pointed to clinic, serological and psychosocial factors in the development of foot ulcers. The mean peak pressure, hazard ratio and odds ratio were given for 15 different regions of the plantar foot, with meaningful associations in the tip of fifth toe, first metatarsal head and lateral heel, concluding that it was not effective. Even the meaningful values became minimal compared to the risk of having previous foot ulcers, nail ingrowth, callus formation, smoking, dry skin, neuropathy, sensitivity loss, edema or limited joint movements. We couldn’t find values to include in the meta-analysis.
Ledoux et al 21 also did a prospective analysis of 8 different areas of the foot, in 591 patients. The metatarsal area was the only one with significant results, but after adjusting for each areas’ variation, this meaningfulness is lost. They also calculated the pressure-time integral, a promising tool that measures the pressure by time unit, which was also related with non-meaningful hazard ratios. There were no descriptions for cut-off values or healthy reference group. This study also differs from others as it did not have patients barefoot on evaluation; instead, they wore their usual footwear and a sensor insole was utilized.
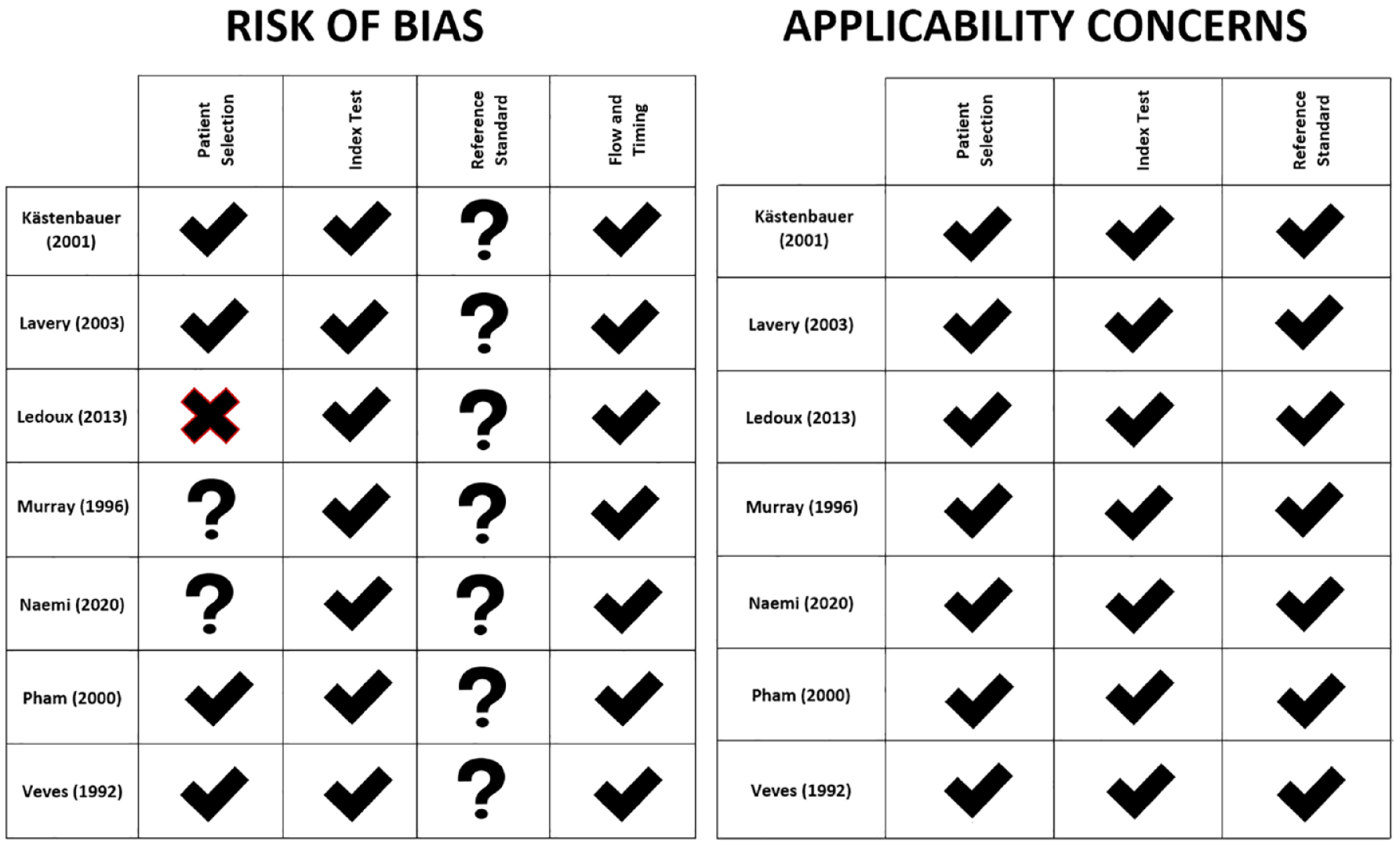
Risk of bias and applicability concerns for each study based on the QUADAS-2 protocol.
Pooled results. I2 test for heterogeneity, p<0.05 means random effects model was chosen.
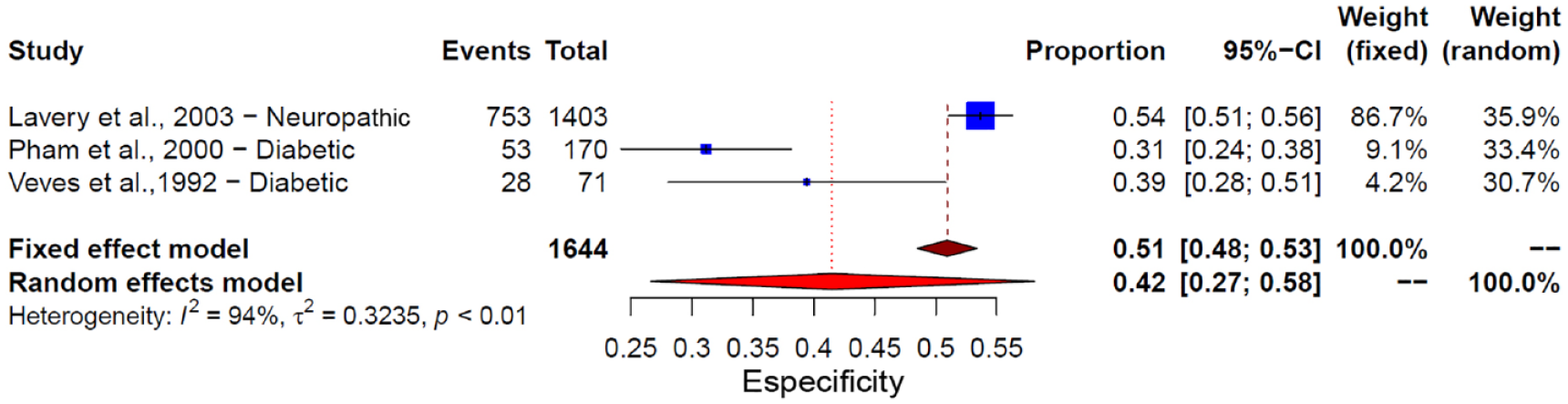
Forest plot detailing the combined effects for specificity.
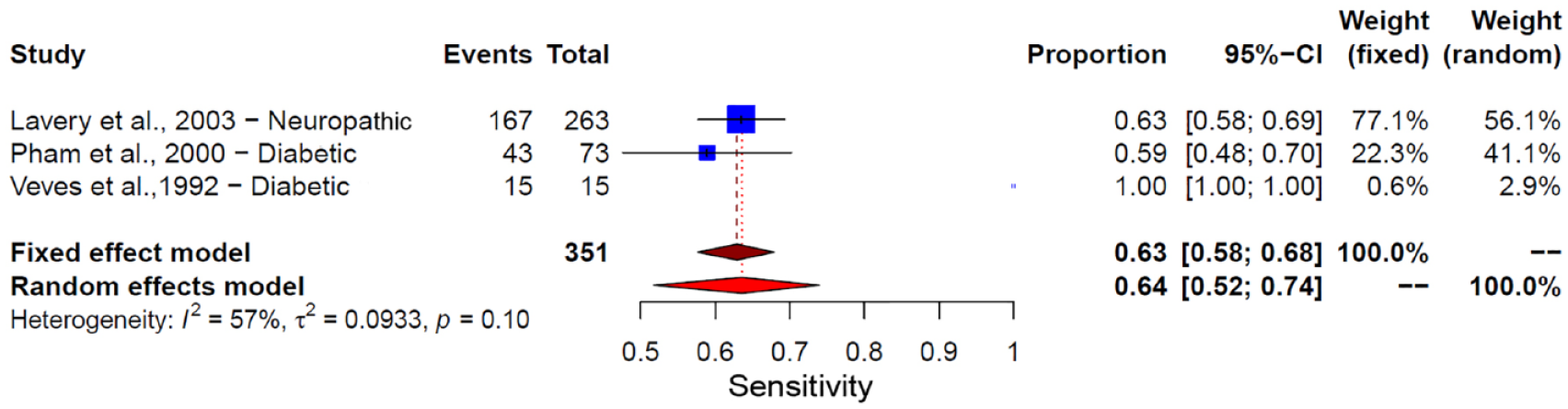
Forest plot detailing the combined effects for sensitivity.
Discussion
As an inexpensive, objectively quantifiable method of measuring forces acting on the foot, pedobarography has been widely used in clinical practice, and to some point is used by itself to quantify tissue damage. Our findings, in contrast, point to low diagnostic predictive capacity, especially in regards to specificity. That is explained by the multifactorial etiology of foot ulcers: patients may have varying degrees of loss of protective sensitivity or peripheral circulation, affecting rate of healing, as well as other factors that damage tissue overtime. Lazzarini et al 22 have conducted an extensive systematic review on plantar tissue stress, that is, an association between vertical stress (plantar pressure), horizontal stress (shear stress), and the frequency in which they occur (weight-bearing activity).
Our significant results on pooled relative risks indicate that, as expected, risk increases with different values of peak pressure, since they indicate higher levels of stress, but this contribution may be variable. In order to accurately predict ulcers, all factors that contribute to plantar tissue stress must be evaluated, not only considering lab exams, but the patients day-to-day life. Although this is not viable in most contexts, continuously measuring plantar tissue stress in a free-living environment would, as far as we know, be the ideal procedure, as it would not assume a single measurement to be representative of stress during the whole day.
There is great heterogeneity in regards to a cut-off value, ranging from 6 to 12.3 kg/cm2, and so far, it would be unwise trying to standardize this parameter. Wrobel and Najafi 23 have highlighted this fact before, and after literature update and meta-analysis, still no conclusion can be drawn about an adequate cut-off value. Data from one study 16 suggests a sensitivity of up to 97% when establishing a higher-pressure cut-off (>10 kg/cm2), with low reduction in specificity. We recommend its usage, in those circumstances, as an initial triage method, discriminating the positive sample immediately as high risk and evaluating remaining patients individually. Even though that is still the only study available with such a value, and more studies would contribute, it seems to be a promising method, since specificity was overall low in this meta-analysis.
Even though various studies described a great incidence of ulcers in the specific areas of higher peak pressure, 2 studies stratified the analysis in different regions, providing odds ratios that, in the great majority of regions, were non-significant. Even in regions that had significant results (metatarsals, tip of the fifth toe and lateral rearfoot) those risks have their values diminished when compared to our pooled effects, which only focused in defining whether or not an ulcer would be developed in the entire plantar area. The interpretation of the optical pedobarography should be done with extreme caution, since, by using it in a localized form, a great deal of information could possibly be lost with greater chance of error.
Reducing pressures through customized insoles is, nonetheless, great for ulcer treatment and prevention, and has been recommended as one of the guides for this holistic approach. Sessions could be conducted similar to the one described by Bus et al, 24 where pedobarography is applied with footwear modifications in order to quickly optimize plantar pressure and decrease risk. This is more strongly recommended in treating neuropathic foot ulcers and also preventing their recurrence. 25
From the 7 studies included in our analysis, 2 of them share the same primary attention clinic responsible for the recruitment,16,17 though they were made in different time periods and there is no evidence that the same individual could have been recruited in more than one study. Additionally, 3 were made in the USA.14,15,21 These studies had a great impact in the qualitative analysis, and some constitute the only studies included in the meta-analysis. More observational studies with robust cohorts in other regional, cultural and socioeconomic contexts would be necessary to ensure that the results of this review are projectable to the global reality.
This systematic review relied on data from prospective studies, in order to establish if pressure increase could precede and be a sign for ulcer formation, although high quality retrospective studies could be developed with the same design, contributing greatly. We also encourage researchers to attempt to clarify the exact contribution of plantar pressure to tissue stress and ulceration, and their applicability on clinical practice, so that our knowledge of foot mechanics and all its variables may fully increase quality of life for patients with diabetes.
Conclusion
In essence, our study concluded that pedobarography is an instrument with limited accuracy, as used to date, to predict the development of plantar ulcers, even though pressure relief is still one of the most important treatment and prevention methods. A large portion of the available studies are considered of high quality, but there is still large methodological heterogeneity and the evidence level is still low. More robust longitudinal studies that research plantar pressure are necessary.
Supplemental Material
sj-pdf-1-dst-10.1177_19322968211043550 – Supplemental material for Accuracy of Foot Pressure Measurement on Predicting the Development of Foot Ulcer in Patients with Diabetes: A Systematic Review and Meta-Analysis
Supplemental material, sj-pdf-1-dst-10.1177_19322968211043550 for Accuracy of Foot Pressure Measurement on Predicting the Development of Foot Ulcer in Patients with Diabetes: A Systematic Review and Meta-Analysis by João Pedro Wardani de Castro, Felipe Camargo Ferreira, João Gustavo Franco Vargas, Lucas Bressan Bosso, Nathan Nabozny, Camila Marinelli Martins, Gabriel Farhat and Ricardo Zanetti Gomes in Journal of Diabetes Science and Technology
Footnotes
Acknowledgements
None
Abbreviations
CI, confidence interval; DM, diabetes melitus; TP, True positive; FP, False Positive; TN, True negative; FN, False Negatives; RR, Relative Risk.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.