
Abstract
Background:
Individuals with diabetes are using online resources to engage in diabetes online communities to find diabetes-related support and information. The benefits and consequences of DOC (diabetes online community) use are unclear. This scoping review aims to map existing research focused on organic DOCs in which individuals affected by diabetes are interacting with peers.
Method:
A scoping review was conducted to comprehensively report and synthesize relevant literature published prior to 2018. Attention was paid to variations in study design, DOC user and platform characteristics, and potential or actual benefits and consequences.
Results:
Of the 14 486 titles identified, 47 articles met the inclusion criteria and were included in this scoping review. No overt definition of the DOC could be identified. Perceived or actual benefits associated with DOC use can be broadly categorized as clinical, behavioral, psychosocial and community outcomes. Perceived, potential, or actual consequences associated with DOC use were categorized as quality of information, risky behavior exploration, acute concerns, psychosocial, privacy, and inactivity.
Conclusions:
The results of this review strongly suggest DOC use is highly beneficial with relatively few negative consequences. DOC use is an emerging area of research and research gaps exist. Future research should seek to identify benefits and consequences to DOC use in experimental trials.
Diabetes is a complex chronic condition that requires ongoing self-management. People with diabetes (PWD) and their caregivers (ie, parent) spend less than 1% of their time in a year visiting with their diabetes health care provider (HCP).1,2 As a result, PWD and their caregivers troubleshoot day-to-day activities on their own. It is estimated PWD spend 8000 hours per year self-managing their diabetes outside of the medical setting. 1 The Diabetes, Attitudes, Wishes and Needs Second Study (DAWN2) suggests PWD feel that their HCPs aren’t always available to provide patient-centered care related to their diabetes. 3 This lack of support, intensity of diabetes management, and social stigma can be associated with burnout, diabetes distress, 4 higher hemoglobin A1C (A1C) and body mass index. 5 In order to fill these gaps, PWD are seeking peer support in online and in-person settings.
Individuals are turning to the Internet to find support and information about their diabetes. In the United States, 23-39% of emerging adults and adults with chronic conditions are seeking peers online.6,7 The American Diabetes Association and the American Association of Diabetes Educators have endorsed the importance of peer support,8-10 such as the Diabetes Online Community (DOC). Further, the American Association of Diabetes Educators has embarked on an initiative to work closely with DOC leadership. 11 Although no studies have been performed to date, the rise in social media use coupled with an increasing number of presentations and research reports focused on the DOC suggests its ongoing growth. Despite this likely increase, we do not fully understand the benefits and negative consequences associated with DOC use. Further, there are no guidelines to assist HCPs in making recommendations to their patients about DOC use.
Understanding that a wide range of methods and outcome variables have been used to explore the DOC, the purpose of this scoping review is to map the current research focused on organic DOCs to characterize the reported positive and negative aspects of DOC use. For the purposes of this study, an organic DOC is defined as a grassroots group of individuals living with or caring for someone with diabetes who gather in online spaces to interact with peers. Although the DOC includes HCPs and industry stakeholders, we only explored research focused on peer-to-peer engagement. Organic DOCs were selected given their relative accessibility and their emerging body of literature. In this paper we will draw conclusions from existing literature regarding the state of the science and identify gaps in the literature.12,13
Methods
We used a rigorous and transparent five step approach 13 to guide this scoping review. The steps included (1) identifying the research questions, (2) identifying relevant studies, (3) selecting studies, (4) charting the data, and (5) collating, summarizing, and reporting the data. Although not typically reported in scoping reviews, the research team assessed the quality of data in order to fully describe the included studies in this emerging field of research. Our approach, as detailed below, should allow for replication of the search strategy, increasing the reliability of our findings.
Research Questions
The focus of this scoping review was to characterize the DOC and the positive or negative aspects of organic DOC use. To ensure the appropriate literature was captured, we posed the following research questions.
How is the DOC defined?
How are the DOC platforms and its users characterized?
What actual or perceived benefits are associated with organic DOC use?
What actual or perceived negative consequences are associated with organic DOC use?
What gaps exist in the current DOC literature?
Identifying Relevant Studies
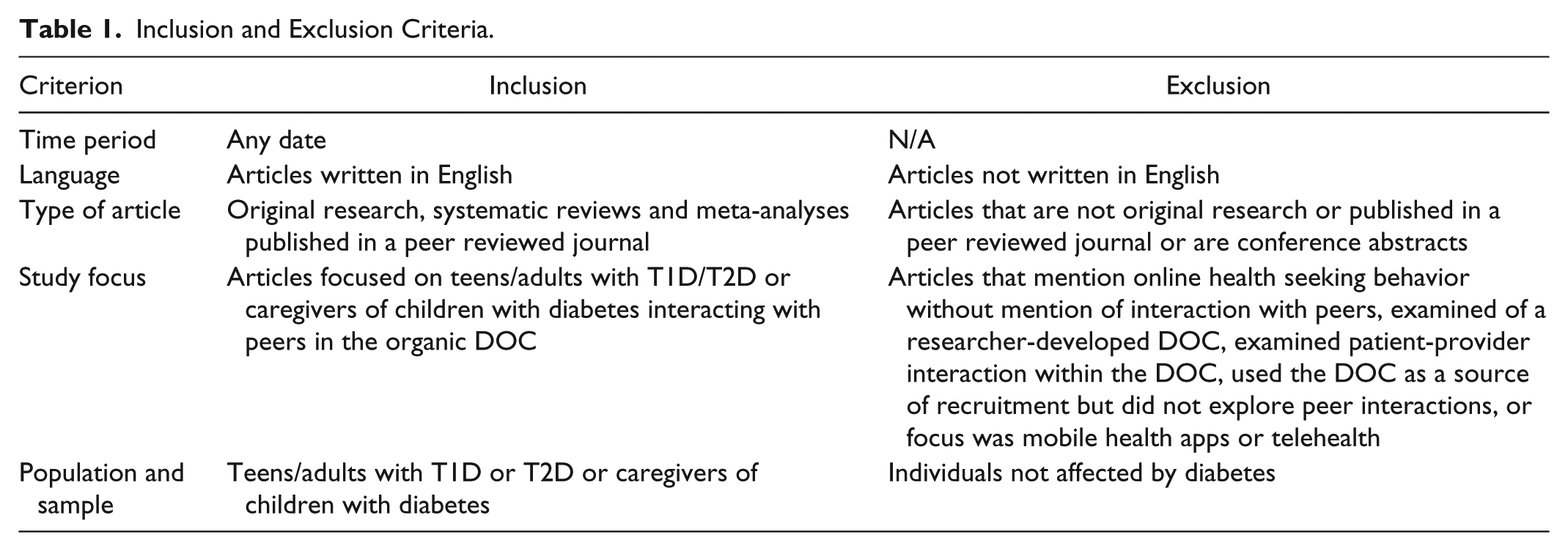
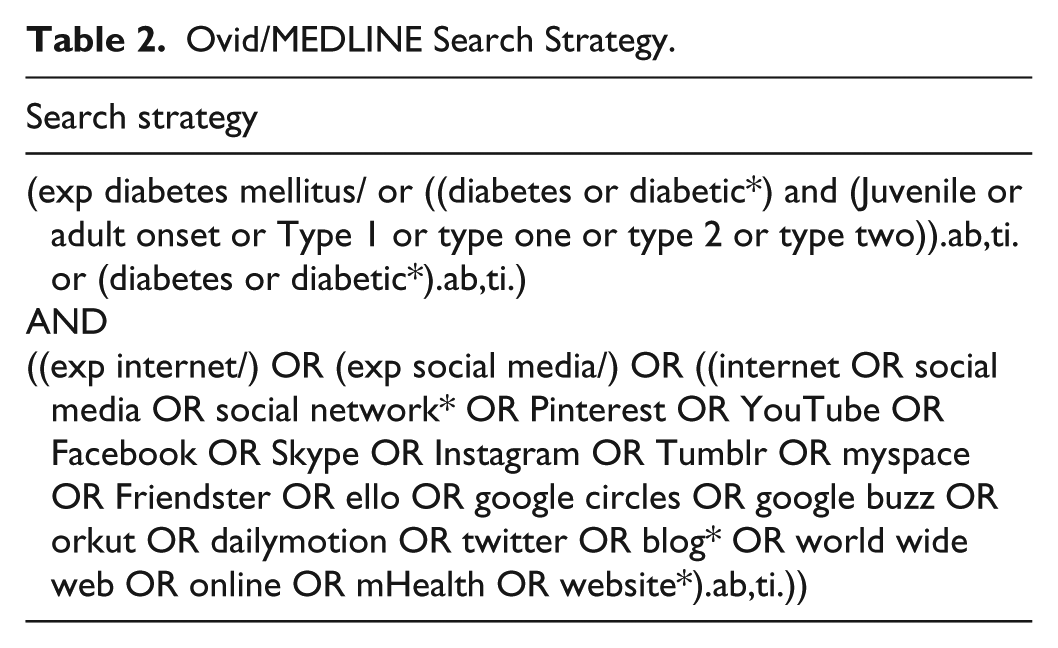
A combination of search terms about diabetes and social media were used and a sensitive search was performed to assure broad retrieval of relevant literature on 19 March 2018 and again on 25 October 2018. No date limitations were set in order to include all known literature in this review. Inclusion and exclusion criteria are listed in Table 1. Terms about communities were intentionally omitted as their use was not consistent among a sample set of desired citations. A medical librarian developed the search strategy using Ovid/MEDLINE (ovid.com) and then translated it for: EMBASE (embase.com), CINAHL (EBSCOhost), PsycINFO (EBSCOhost), Web of Science, and Communication and Mass Media (EBSCOhost). Key search terms and the complete search strategy developed for Ovid/MEDLINE is listed in Table 2.
Inclusion and Exclusion Criteria.
Ovid/MEDLINE Search Strategy.
Study Selection
The search strategy yielded 14 486 studies. Covidence systematic review software (http://www.covidence.org) was used following the removal of duplicate citations. 14 An additional 21 papers not retrieved in database searches were identified. The authors independently screened titles and abstracts for relevance. Full-text articles were double-blind reviewed by two authors for inclusion. Two additional authors resolved disagreements. Thus, 47 articles were included in this scoping review. Preferred Reporting of Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines 15 were used to describe the article selection process (Figure 1).
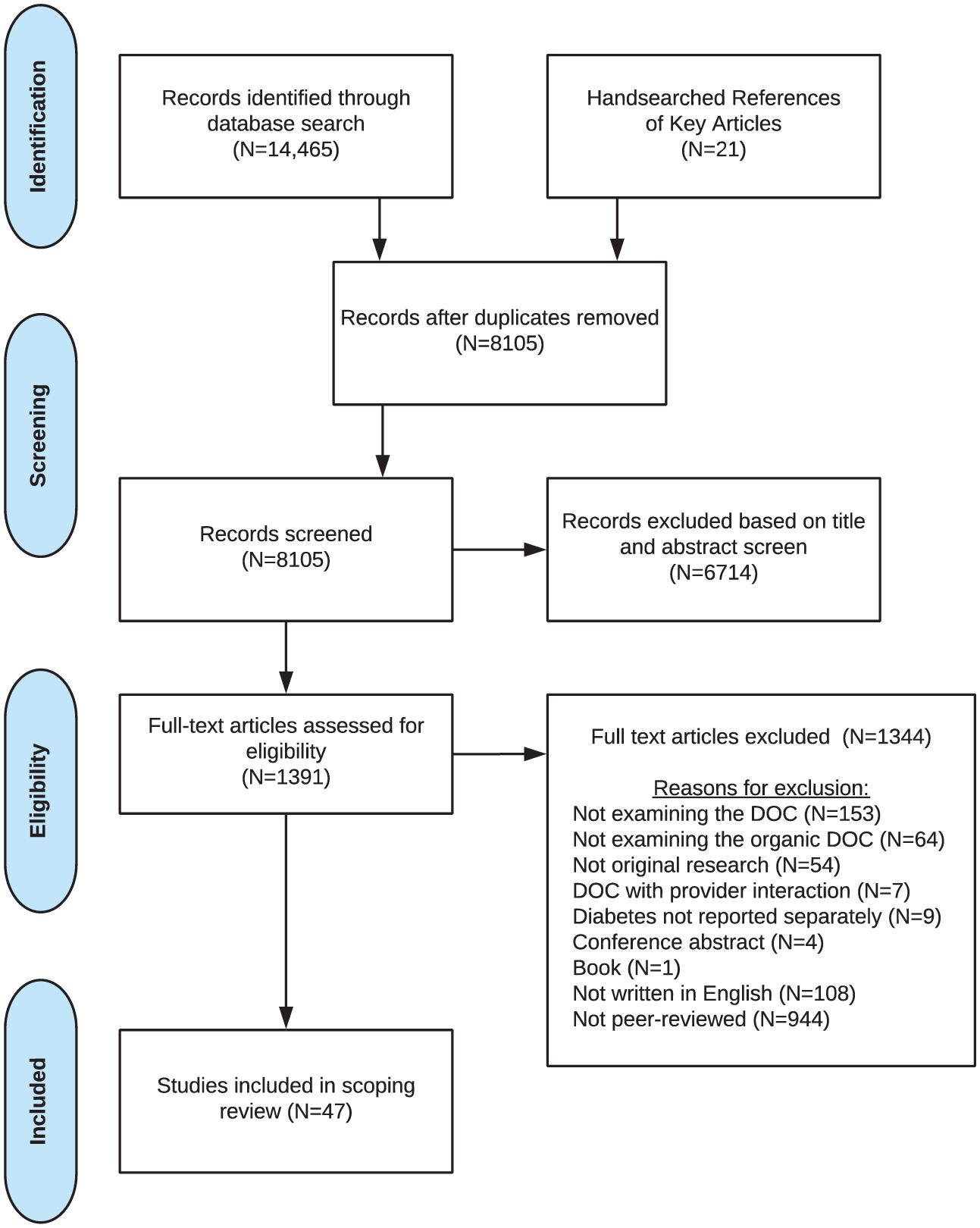
PRISMA diagram.
Data Charting
Summaries of each article were documented, noting the author, year, study aims, methods, sample, location, themes, outcome measures, results, ethics approval, funding source, and data quality. Covidence was used to tag studies. Tags included (1) sample (child with diabetes, <12 years; adolescent, 13-18 years; parent of child with diabetes; person with diabetes, T1D; person with diabetes, T2D); (2) setting (Facebook, Twitter, Instagram, online forum, other); (3) location (based in United States, not based in United States); (4) method (qualitative; quantitative; review); (5) outcome (psychosocial, clinical, behavioral).
Assessing Data Quality
Joanna Briggs Institute critical appraisal checklists 16 were selected to assess the methodological quality of the selected articles given the breadth of research designs included in this scoping review. Two authors assessed and reached consensus for all 47 selected studies. Checklists were unavailable for social network analysis and text mining studies. For these studies, authors reached consensus through discussion. No studies were omitted due to the quality of data being too poor. Quality assessment checklists are described in detail in Appendix A.
Results
Study Selection
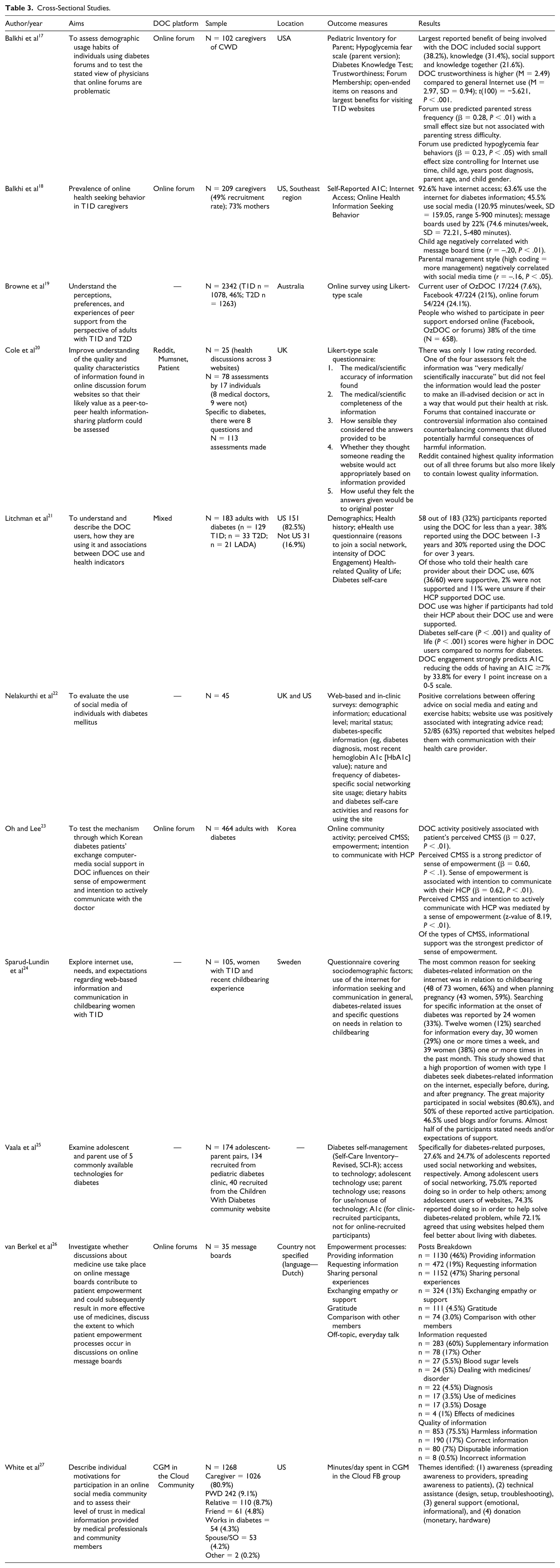
This scoping review initially identified 14 483 articles. After removing duplicates and ineligible reports, 47 articles representing 43 studies were examined. Study methodology varied and was categorized as cross-sectional, prospective qualitative, retrospective qualitative, social network analysis, and text mining (Tables 3-6).
Cross-Sectional Studies.
Prospective Qualitative Studies (Interviews/Focus Groups).
Social Network Analysis Studies.
Text Mining Studies.
1. Research Question 1: How is the DOC defined?
There were no overt definitions of the DOC. Litchman et al 34 described the DOC as having components of peer health, defined as “the interaction, education, and support offered by peers with the same condition to promote health-enhancing change.”
2. Research Question 2: How are the DOC platforms and its users characterized?
DOC Platforms, Users, and Measures
A variety of DOC platforms (Twitter, Facebook, Google+, YouTube, and blogs) were used to examine DOC users, with the most common being online forums. One study 35 explicitly looked at DOC users engaging in more than one platform and two studies recruited from multiple DOC platforms, but did not explicitly identify users who engaged with multiple platforms.21,34 Each platform investigated seem to have its own dedicated userbase with little overlap between DOC users. DOC users spanned at least 92 countries. Most studies focused on T1D.17,18,24,25,27,37,38,50,52,53,57,58 Twenty articles contained demographic information about DOC users.17-19,21,23-25,27-34,37-39,41,48,53 Age of DOC users range from 12-82 years.17,18,21,23,25,27-34,37 Overall, there were more female than male DOC users examined.17,21,23,24,27,30-32,34,35,38,39,48,53 The majority of DOC users were white17-19,21,25,27-29,34 college graduates17,21,23,25,27,34 with few healthcare provider users. Lurkers, individuals who read but do not generate posts were described.31,32 There were a variety of ways in with DOC use was measured, which included activity, intensity, engagement, time spent, and number of posts (Table 7).
3. Research Question 3: What actual or perceived benefits are associated with organic DOC use?
Measures of DOC Use.
Actual or perceived benefits associated with DOC use were categorized on the individual level, which focused on clinical, behavioral, and psychosocial outcomes; and on the collective level, which focused on community building (Table 8).
Benefits and Consequences Related to DOC Use and Diabetes Type.
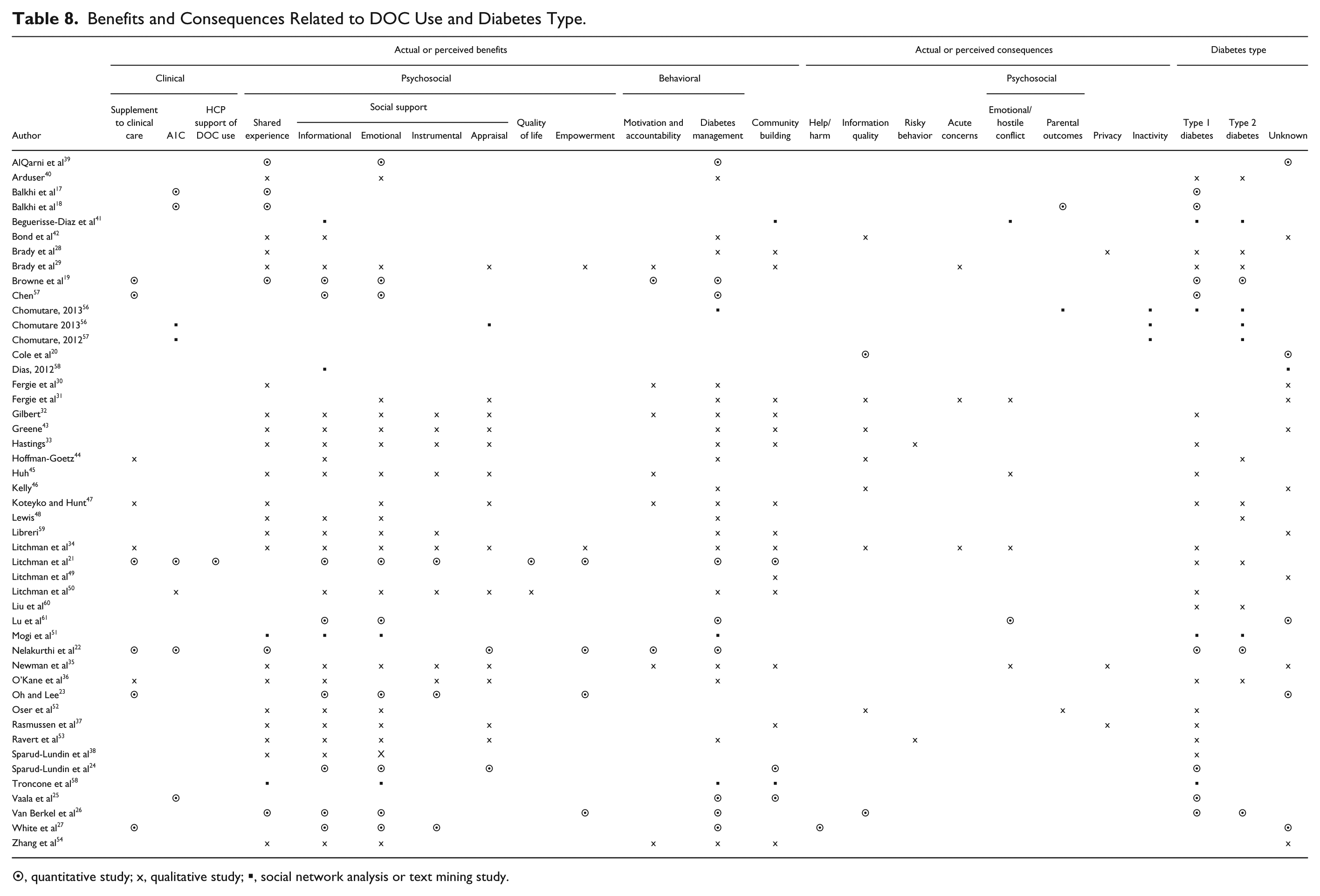
⊙, quantitative study; x, qualitative study; ▪, social network analysis or text mining study.
Clinical
In the studies reviewed, DOC use supplemented clinical care, but did not replace it.21,22,34,36 Of DOC users, 87% saw their HCP at least biannually. 21 Clinical measures were used to gauge outcomes associated with DOC use, including self-reported A1C and survey items exploring HCP support of DOC use.
A1C
Self-reported A1C had neutral or beneficial associations with DOC use.17,18,21,25,41,56 A1C was neutral among children whose parents used the DOC17,18 and adolescents. 25 Conversely, in adult DOC users with T1D and T2D, high levels of DOC engagement predicted A1C. For every point increase on a 5-point DOC engagement scale, there was a 33.8% reduced odds of having an A1C ≥ 7.0%, although causation could not be determined. 21 In one study, A1C was within target range for DOC users engaging in patient-driven innovation, such as the open-source artificial pancreas. 41 Although no analysis correlated A1C to frequency of posting, in a social network analysis of 107 927 posts, the “majority” (no sample size defined) disclosed an A1C ranging from 6-9%. 56 No studies examined biophysical measures of A1C.
HCP Support of DOC Use
Some (31-67%) DOC users had not discussed their DOC use with their HCP.19,21 Those with T1D were more likely to disclose; however, those with T2D felt more supported when they chose to disclose. 19 DOC use was higher among PWD who told their HCP of their DOC use and felt supported to continue. 21 DOC users wanted HCPs to read DOC postings to enhance their understanding of living with diabetes and the value the DOC has for its users, 28 but did not suggest that HCPs interact with DOC users online. Few (2%) DOC users were not supported by their HCP to use the DOC, 21 perhaps because the HCP didn’t understand the benefits. 29
Psychosocial
There were a myriad of psychosocial benefits noted. Health-related quality of life was higher in DOC users when compared to a general population of PWD. DOC users engaged in patient-driven innovation, experienced reduced diabetes burden and enhanced quality of life. While only two studies explicitly examined quality of life21,41, multiple studies implied that improving psychosocial outcomes would lead to the improvement of quality of life of PWD. Other variables examined focusing on the psychosocial aspect of living with diabetes as it relates to DOC use included shared experience, social support, and empowerment.
Shared Experience
Shared experience was commonly identified.17,19,21,26,28,29,31-40,42,43,45,47,48,51-54,57-59 Shared experience in the DOC was qualified as (1) a value and role marker for members (DOC users valued those with more diabetes experience 34 with some members taking on mentor-like roles);35,43,54 (2) a post category that occurred most frequently (27-35% of the time);39,51 (3) a method of normalization which validated the lived-experience of members 36 and provided comfort resulting in decreased feelings of isolation;19,21,29,30,36,37 (4) a learning opportunity21,26,28,29,33-35,54 sometimes gained through humor and venting;29,41,47 (5) a mode of story-telling;43,45,52 (6) a pathway toward empowerment;26,29,34 and (7) a relationship-building process between users35,53,57 and between users and the wider DOC network. 47 Shared experience appears to underpin activity toward other psychosocial benefits and negative consequences within the DOC.
Social Support
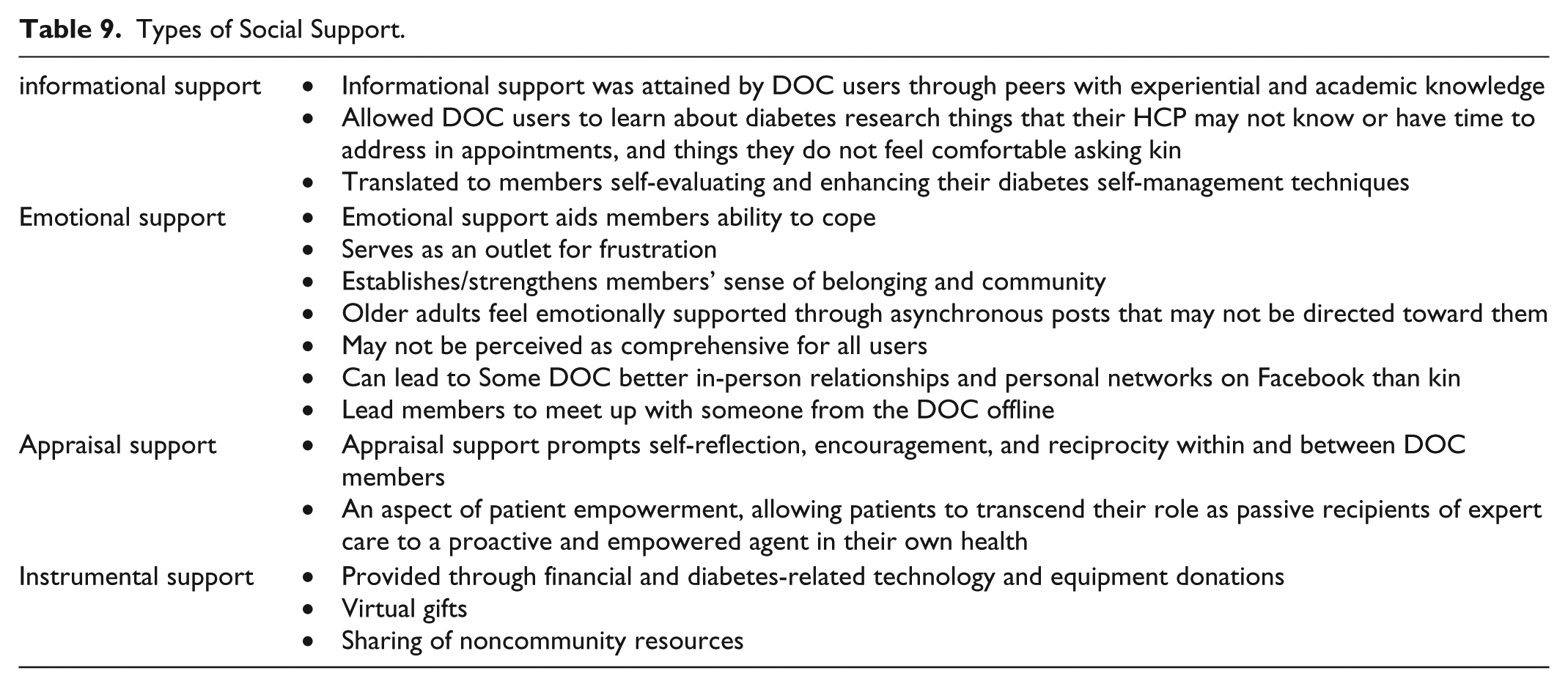
Social support was an overarching multimodal theme. Broadly, social support was identified as helpful during life transitions, such as a new diabetes diagnosis or pregnancy.30,31,35,37,57 DOC use is positively correlated with social support. 23 Half of posts from adolescent DOC users sought social support from peers. 53 Social support was most commonly subcategorized as informational, emotional, instrumental, or appraisal support (Table 9). While there was occasional overlap, these categories remained distinct across most studies.
Types of Social Support.
Empowerment
Empowerment was reciprocated through a learning and sharing process. High DOC use was associated with feelings of empowerment. 21 As a result, DOC users were more likely to communicate with their health care providers.22,23 DOC use helped individuals take ownership of their condition, resulting in more active engagement with HCPs. 29 Interaction with the DOC allowed some individuals to question their T2D diagnosis, leading to a subsequent correct T1D diagnosis and treatment regimen. 29 One pathway suggested increased DOC use predicted increased social support, which predicted sense of empowerment. 23
Behavioral
Behavioral outcomes were discussed across studies of varying methodologic approaches. Motivation and accountability emerged as a subcategory based on frequency of DOC use. The majority of benefits related to DOC use discussed concepts of diabetes self-management in some capacity. Enveloped within the larger category of self-management emerged the subcategory of diabetes self-care.
Motivation and Accountability
The DOC was used as a source for motivation and accountability.19,22,29,30,32,35,45,47,54 DOC users varied in how they were motivated, some of which included (1) healthy eating or exercise check-ins, (2) interaction with role models who had achieved their weight loss or diabetes management goals, (3) PWD with similar circumstances and goals, and (4) competition.
Diabetes Self-Care
Two studies21,25 examined the Diabetes Self-Care Inventory Revised tool, 60 while one study 22 used the Diabetes Self-Care Activities measure. 61 Diabetes self-care scores were higher (indicating more self-care) in adult 21 and adolescent 25 DOC users when compared to those not using the DOC. Diabetes self-care was also positively correlated with DOC use. 21 Specific self-care tasks, such as healthy eating, exercising, checking glucose levels and taking insulin were more frequently self-reported in DOC users compared to nonusers. 22 Qualitatively, the DOC was identified as an important factor in supporting diabetes self-care.34,40,47,57 DOC users used peers to problem-solve by crowdsourcing diabetes related issues and concerns.25,30,41
Community Building
Community building motivated DOC participation,33,43 as expressed through linguistic solidarity,47,58 and as facilitated by identity construction and validation.33,47,54 To keep some individuals more closely tied to their network, some DOC users engaged with more than one DOC platform, deepening relationships and access to support. 35 Engaging in a DOC required effort, such as identifying supportive contacts or nudging existing contacts to be healthier. 35 While financial compensation for product sponsorship was mentioned for some bloggers, 41 no studies commodified DOC participation in terms of work or labor, nor did they examine changing community dynamics if and when key DOC users choose to leave, decrease activity, or expire.
The curation of online diabetes-related content was identified as a beneficial aspect of DOC use.28,41,43,47,59 Several studies indicated that adult21,27,28,34,41 and adolescent25,53 DOC users participated to help others. This help occurred even when the DOC user didn’t need help in return, 34 suggesting altruism. Efforts to help others sometimes resulted in patient-driven innovation27,41 and in personal and public advocacy efforts.43,52 DOC users desired lifelong relationships with peers. 49
4. Research Question 4: What actual or perceived negative consequences are associated with organic DOC use?
Actual and perceived negative consequences were minimal and were categorized as help or harm, information quality, risky behavior, acute concerns, psychosocial, privacy and inactivity.
Help or Harm
Using similar questions to the Pew Research Center’s Internet and American Life Project, 63 two studies examined how helpful or harmful the DOC is.21,27 The DOC was reported as being helpful 38-70% of the time. Conversely, only 0.07-1.8% of DOC users reported the DOC causing minor harm.21,27 This harm was further characterized in one study 27 as glucose information overload which related to technology, and not community interactions. In one study, some DOC users weren’t sure if help (27.3%) or harm (45%) had taken place. 21
Information Quality
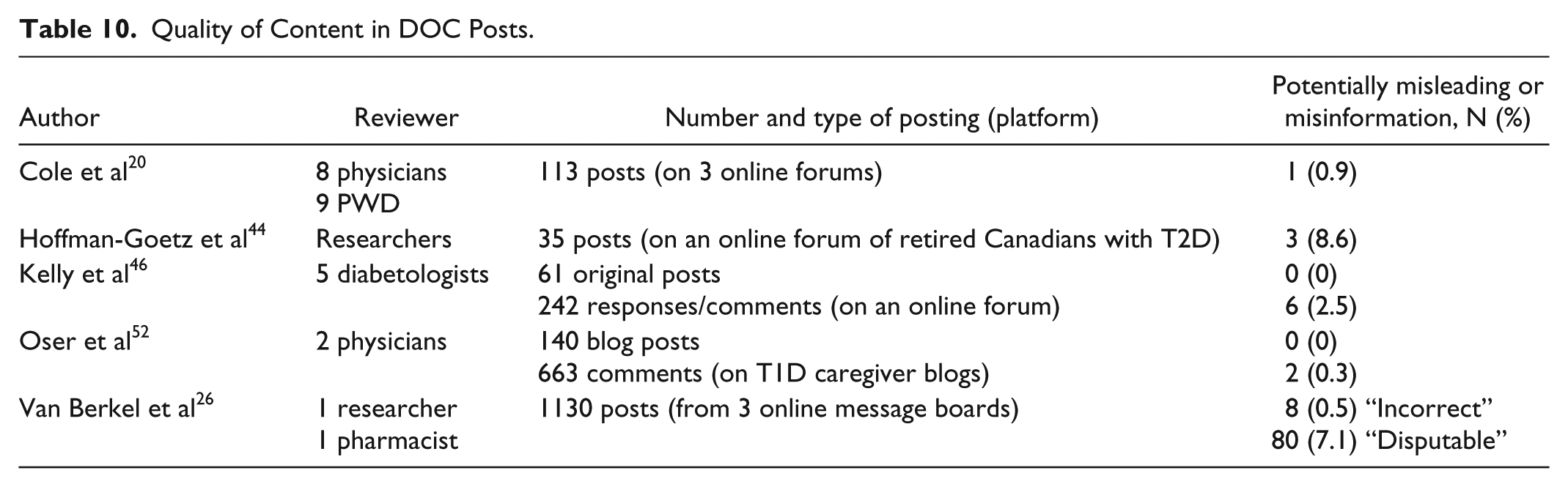
Misinformation was uncommon in online forums and blogs.20,26,44,46,52 Potentially misleading and misinformation in DOC posts ranged from 0-9% and were characterized as unlikely to lead to untoward effects (Table 10). A self-policing process among DOC users to dilute misinformation was described.20,34 Some DOC users were forthright in notifying others that their experience may differ from the experiences of others, making posts more trustworthy.34,42 Many DOC users underwent a vetting process to determine accuracy and quality of information found within the DOC,30,34,42 which sometimes included contacting HCPs. 34 Sharing and “like” features are used by some DOC users to highlight quality information. 47
Quality of Content in DOC Posts.
Risky Behavior and Acute Concerns
The DOC was sometimes used to explore risky behavior, such as alcohol or drug use and diabulimia. Adolescents 53 and Facebook DOC users 43 wanted to learn about how risky behaviors might affect their diabetes. While use of the DOC could be helpful to some with diabulimia, it could threaten recovery in others. 33 There were mixed reports of the DOC being used for acute concerns. While Brady 29 did not identify the DOC being used for acute concerns, others did.30,34 When offline support was unavailable or not helpful, some individuals would turn to the DOC to obtain timely assistance.30,34 Although, during acute situations, DOC users would refer individuals to a HCP. 34
Psychosocial
As described above, the DOC was used as a way to provide and receive psychosocial support. However, there were instances in which negative aspects were reported, though they were infrequent. Topical areas included emotional or hostile posts and parent outcomes.
Avoidance of Posts with Emotional or Hostile Conflict
Some DOC users reported purposefully avoiding posts that were excessively emotional.30,34,35 There were also instances of infighting among DOC users resulting in negative discussions about T1D and T2D that appeared to be rooted in misconceptions and possibly stigmatizing attitudes.34,41 This infighting sometimes drove individuals away from the DOC, at least temporarily. 34 One study identified Twitter DOC users wishing diabetes upon individuals who didn’t have diabetes in response to stigmatizing comments. 41 There are differences in how individuals present themselves based on platform. For example, hate comments were not identified in diabetes vlogs on YouTube. 45 In one study, DOC users presented themselves as more composed on Facebook compared to other DOC platforms. 35
Parental Outcomes
DOC use by parents has been associated with parental hypoglycemia fear and parental stress frequency, 17 however, causation could not be determined. It is unknown if parents with hypoglycemia fear or increased parental stress frequency are more likely to engage in the DOC for support or other factors, or if DOC use might increase hypoglycemia fear and parental stress frequency. Similarly, a social network analysis identified that parents of children with diabetes struggled the most among online forum users, although did not characterize this further. 55
Privacy
The DOC was often viewed as a public space and DOC users shared information in a variety of ways. Some DOC users were more willing to share personal health information in a live chat session where data wasn’t stored, in a private group, or filtered personal information in more public spaces.28,35 Some DOC users were intentionally selective about which DOC platforms they would share personal information with emotional content31,35,37 while others shared openly among “friends,” forgetting that strangers could also view the information 28 or that posts could automatically update on other social networking profiles. 35 Very few studies mentioned lurking,32,34,35,46 a concept used to describe DOC users who passively engage (ie, read content) in DOC activity generated by others, but do not actively participate (ie, originate or comment on posts). While lurkers may be able to obtain support without providing personal information, Newman 35 suggests DOC users could not be emotionally supported unless they were willing to post their struggles, which may conflict with desires for privacy. In contrast, one study described DOC users who could be emotionally supported by reading content generated by others, 34 supporting the notion that DOC users can maintain privacy as passive participants.
Inactivity
There was very little information about inactivity by means of never starting or stopping DOC use. Mogi 51 found that more than half of DOC communities on Google+ were inactive. While the DOC was used during times of need for additional social support,30,31,37 no studies examined DOC use or inactivity as it related to support from personal networks. Only one study examined why PWD would not use the DOC. In this study focused on adolescents, the most common reasons reported for not using DOCs were because there was no identified need or problem warranting DOC use, no desire to talk about diabetes, or a belief that social networking should not be used for diabetes. 25
5. Research Question 5: What gaps exist in the current DOC literature?
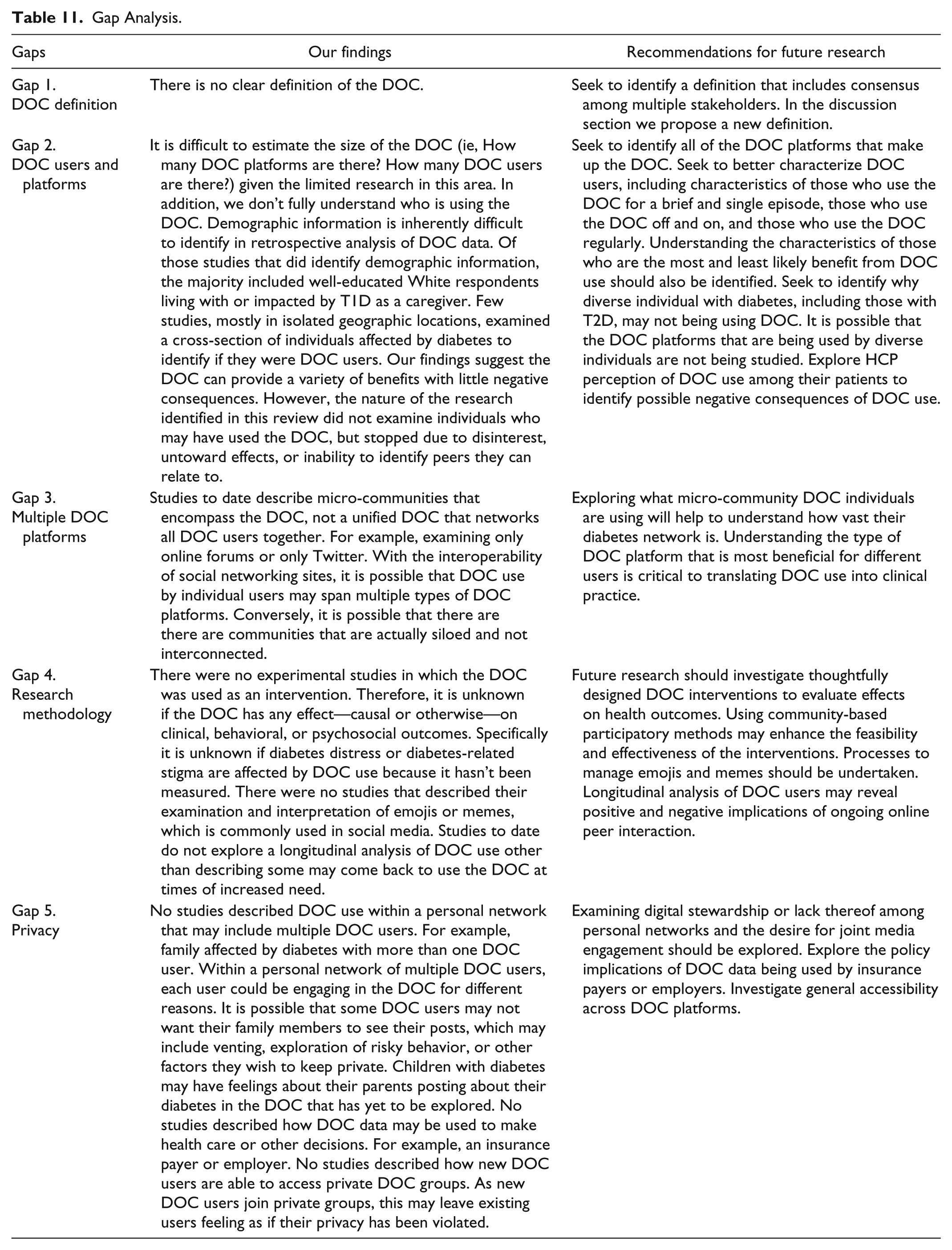
Answering this research question was an iterative process conducted in which the research team members, comprised of clinicians, PWD, caregivers to children with diabetes, and researchers; discussed content and methodological areas of weakness within the body of research reviewed. Five gaps in knowledge emerged: (1) lack of DOC definition, (2) description of DOC users and platforms, (3) use of multiple DOC platforms, (4) research methodology, and (5) privacy. Findings and recommendations for future research are described in Table 11.
Gap Analysis.
Discussion
This scoping review aimed to systematically map and synthesize existing published research focused on organic DOCs and to identify knowledge gaps. We identified a global collection of studies with a variety of methodologies and outcome measures. Research in this topical area is rapidly emerging, however, to date, is relatively descriptive. In addition, there is no consensus of terminology across research in this content area.
Given the lack of consensus on a DOC definition in the included studies, we propose a new definition that reflects our findings: The “DOC” is a user-generated term that encompasses people affected by diabetes who engage in online activities to share experiences and support in siloed or networked platforms. This definition not only lends credence to the term used by communities of interest, but also recognizes the multifariousness of DOCs.
Most studies we reviewed focused on a singular DOC platform without identifying doing so as a methodological limitation. We can assume their epistemological understanding of the DOC is monolithic. A significant finding of this study is that there is no singular DOC, but several distinct groups, resulting in multiple DOCs. Recurrent users were identified by some studies, but not all. A community element may be necessary to understand long-term benefits and consequences of DOC use. Future research on DOC activity and outcomes would benefit from the use of participatory frameworks, such as including users in the design and parameter-setting stages to not only capture a community element, but also increase the social validity and usability of the knowledge produced by the work. 64
There was also a general lack of participant diversity accounted for in the studies. This lack of diversity was found among DOC users by race, education, and diabetes type, though DOC research in Hispanic populations is underway. 65 Although T2D makes up the majority of all types of diabetes, 66 most research identifying diabetes type was focused on T1D, suggesting those with T1D may be more inclined to use the DOC. Perhaps individuals with T1D specifically seek out the DOC because it is more challenging to identify a peer offline. Other types of diabetes, such as latent autoimmune diabetes of adulthood, were only described in two studies21,34 and warrant further examination given the higher possible rates of misdiagnosis. 67 It is possible that individuals with diverse backgrounds, lower income, or T2D may initially come to the DOC, but do not stay because they are unable to identify relatable peers. Individuals with T2D may experience stigma as a result of hostile posts between those with T1D and T2D 34 or “humorous” posts that may be perceived as stigmatizing. 41 There were no studies focused on DOC users who have left the DOC, although one article illuminated why adolescents may not be using the DOC. 25 Future research should carefully examine attrition rates, 68 including reasons, such as adverse outcomes and disinterest. This examination may help to characterize for whom the DOC is most beneficial.
All studies discussed or measured benefits and consequences to DOCs participation in some capacity. One of those measures was A1C. A1C was neutrally or beneficially associated with DOC use. In a randomized control trial of adolescents, A1C was reduced in researcher-developed DOC groups when compared to control. 69 Similarly, in a retrospective cross-sectional study of adolescents and young adults, A1C improved using a researcher-developed DOC group. 70 Therefore, there may be utility in both organic and researcher-driven DOCs. Given that parental stress is linked to worsening A1C in children with diabetes, 71 perhaps the DOC provides a protective factor in neutralizing A1C as parents can solicit and receive support. Among adults, engagement in the DOC may influence both behavioral and psychosocial barriers to self-care, resulting in safer glycemic levels. Alternatively, DOC users may be motivated by social comparison72,73 or influenced by social contagion. 74 Finally, information from peers may provide autonomy support75 when family and friends are not helpful. 76 Lack of biophysical measures of A1C may affect reliability of data. However, consistency between self-reported A1C and registry data has been established.77,78
Shared experience was the most frequently mentioned topic across all studies reviewed. Shared experiences provided DOC users with a sense of normalcy, validating the lived experiences of PWD. DOC users report higher ratings on quality of life measures than non-DOC users, suggesting that DOC use influences users in ways that extend beyond diabetes-specific outcomes. Empowerment was described as an individual measure leading to positive self-management behaviors. Studies did not report collective empowerment of multiple DOC users as it relates to advocacy or activism. While there were multiple psychosocial benefits noted related to DOC use, no studies examined diabetes distress, a known predictor of self-management behaviors. 3
Misinformation was uncommon across several of the studies reviewed. In the context of a community, DOC users appear to be obtaining relevant and credible information as suggested by Apomediation Theory.79,80 In some instances, the DOC corrected misinformation in the online community using a self-policing model. Further, DOC users reported misinformation originating from HCPs. For example, providing information that led someone who was misdiagnosed to a correct diabetes diagnosis—a more common occurrence now that we understand nearly half of T1D cases are diagnosed after age 30. 67 While professional organizations can successfully debunk misinformation online, 81 they can mislead as well. 82
Consequences to DOC use were minimal. However, in certain populations, such as those with diabulemia, DOC use may not be beneficial given that it may threaten recovery. 33 As such, DOC use may not be beneficial for all. In some instances, interactions akin to cyberbullying did occur, which amplified negative consequences, however, this was not common. Notable, some DOC users were unsure if they had been helped or harmed by DOC use, 21 which warrants further study.
Clinical Implications
Overall, DOC use suggests a variety of benefits with low reports of negative consequences. Currently, 1 in 3 diabetes educators recommend DOC participation to their patients. 83 However, we do not know if and how frequently other HCPs (ie, pediatric and adult endocrinologists, primary care providers) recommend DOCs. DOC users are interested in having HCPs read through DOC postings in order to enhance understanding of living with diabetes and the value the DOC has for its users. In the United States, 73% of diabetes educators are engaged in the DOC either actively or passively. 83 The DOC, with minimal costs associated with use, is a relatively accessible solution to the professional recommendations for peer support.8-10
Limitations
It is possible that our search strategy did not identify all articles examining organic DOCs. Searching other databases may have yielded other studies that would have met inclusion criteria. We did not seek to identify how HCPs are using the DOC to interact, learn from, or provide education to PWD. We only included articles written in English. Conference proceedings, which may have provided additional insight to this review, were excluded. While we did not explore the interaction between HCPs and PWD, research suggests HCP-patient interaction on social media is an effective and naturally cost-effective intervention to promote health. 84
Conclusion
This scoping review maps existing research focused on peer-to-peer interaction within organic DOCs. DOCs are relatively accessible resources and spaces for peer support activity that appear to be beneficial to users with minimal harm reported. Future experimental research is needed to understand the impact of DOC use on health outcomes.
Supplemental Material
Appendix_A._Quality_Assessment – Supplemental material for State of the Science: A Scoping Review and Gap Analysis of Diabetes Online Communities
Supplemental material, Appendix_A._Quality_Assessment for State of the Science: A Scoping Review and Gap Analysis of Diabetes Online Communities by Michelle L. Litchman, Heather R. Walker, Ashley H. Ng, Sarah E. Wawrzynski, Sean M. Oser, Deborah A. Greenwood, Perry M. Gee, Mellanye Lackey and Tamara K. Oser in Journal of Diabetes Science and Technology
Footnotes
Abbreviations
A1C, hemoglobin A1C; CMSS, computer-mediated social support; CWD, children with diabetes; DOC, diabetes online community; FDA, Food and Drug Administration; HCP, health care provider; LADA, Latent Autoimmune Diabetes of Adults; M, mean; PWD, people with diabetes; Q&A, question and answer; SD, standard deviation; T1D, type 1 diabetes; T2D, type 2 diabetes.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project is supported by a research award from the American Association of Diabetes Educators.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.