
Abstract
Background:
Diabetes management apps may have positive effects on diabetes self-management. It remains unclear, however, which app features are particularly effective and encourage sustained app usage. Behavior change techniques (BCTs) and gamification are promising approaches to improve user engagement. However, little is known about the frequency BCTs and gamification techniques (GTs) are actually used. This app review aims to provide an overview of BCTs and GTs in current diabetes management apps.
Methods:
Google’s Play Store was searched for applications using a broad search strategy (keyword: “diabetes”). We limited our research to freely available apps. A total of 56 apps matched the inclusion criteria and were reviewed in terms of the features they offer to support self-management. We used a taxonomy comprising 29 BCTs and 17 GTs to evaluate the applications. Two independent raters tested and evaluated each app.
Results:
Interrater agreement was high (ICC = .75 for BCTs; ICC = .90 for GTs). An average of 7.4 BCTs (SD = 3.1) and an average of 1.4 out of 17 GTs (SD = 1.6) were implemented in each app. Five out of 29 BCTs accounted for 55.8% of the BCTs identified in total. The GT most often identified was “feedback” and accounted for 50% of the GTs.
Conclusions:
The potential of BCTs and GTs in diabetes management apps has not been fully exploited yet. Only very restricted sets of BCTs and gamification features were implemented. Systematic research on the efficacy of specific BCTs and GTs is needed to provide further guidance for app design.
The number of people diagnosed with diabetes has been continually increasing over the past decades with current prevalence estimates amounting to 8.8% among adults worldwide, equaling 425 million people with diabetes.
1
Diabetes and its complications impose high social and economic burden on countries and health care systems.
2
In 2012, the estimated total cost of diagnosed diabetes in the United States amounted to $245 billion.
3
To avoid diabetes-associated complications such as cardiovascular disease, neuropathy or nephropathy, people with diabetes have to assume an active role in their treatment, including regular self-monitoring of blood glucose, physical activity, following diet recommendations and insulin injections or intake of medication if required.
4
Successful self-management is a key determinant of treatment outcomes
5
and national and international treatment guidelines are highlighting its significance.4,6 Today, people with diabetes can benefit from a wide range of technical innovations to support daily self-management tasks. Mobile health (mHealth) innovations—wireless mobile devices that support medical and public health practice
7
—have great potential to improve health outcomes in the management of chronic disease.
8
mHealth solutions include smartphone applications (apps) aiming to facilitate symptom control and to enhance diabetes self-management by tailoring support to the needs of people with diabetes (eg, raise motivation). Several studies show positive effects for the use of smartphone apps in diabetes self-management.8-14 Nevertheless, the use of health apps is not widespread,
15
leading to the question how the users’ motivation to engage into app usage can be enhanced. Behavior change techniques (BCTs) may provide suitable strategies. BCTs refer to intervention rationales that aim to motivate people to change health-related behavior.16,17 Positive effects of the integration of BCTs in mHealth interventions have been addressed previously.18,19 A related way to increase patient’s engagement in sustained app usage is “the use of game design elements in non-game contexts”
Methods
Google’s Play Store was searched for freely available applications in February 2018 using a broad search strategy (search term: “diabetes”). Our search yielded 249 initial matches. We applied the following inclusion and exclusion criteria: Apps were eliminated if they were not available in English (n = 44), not categorized into “Medical” or “Health & Fitness” (n = 28) and not developed for people with diabetes (eg, apps for health care professionals, family members, etc; n = 6). Due to the significance of blood glucose monitoring in successful diabetes self-management, we only included apps providing a diary function for blood glucose measurements and excluded apps with informational/educational content only (n = 93). Seventy-eight apps remained and were evaluated. Twenty-two apps had to be excluded during the evaluation process because mandatory registration failed to work (n = 16), usage depended on wearable devices (n = 4), because of problems installing the app (n = 1) and because one application was a duplicate. Fifty-six apps finally remained and were evaluated for diabetes self-management functions and for the implementation of BCTs and GTs.
App Characteristics and Diabetes-Specific Features
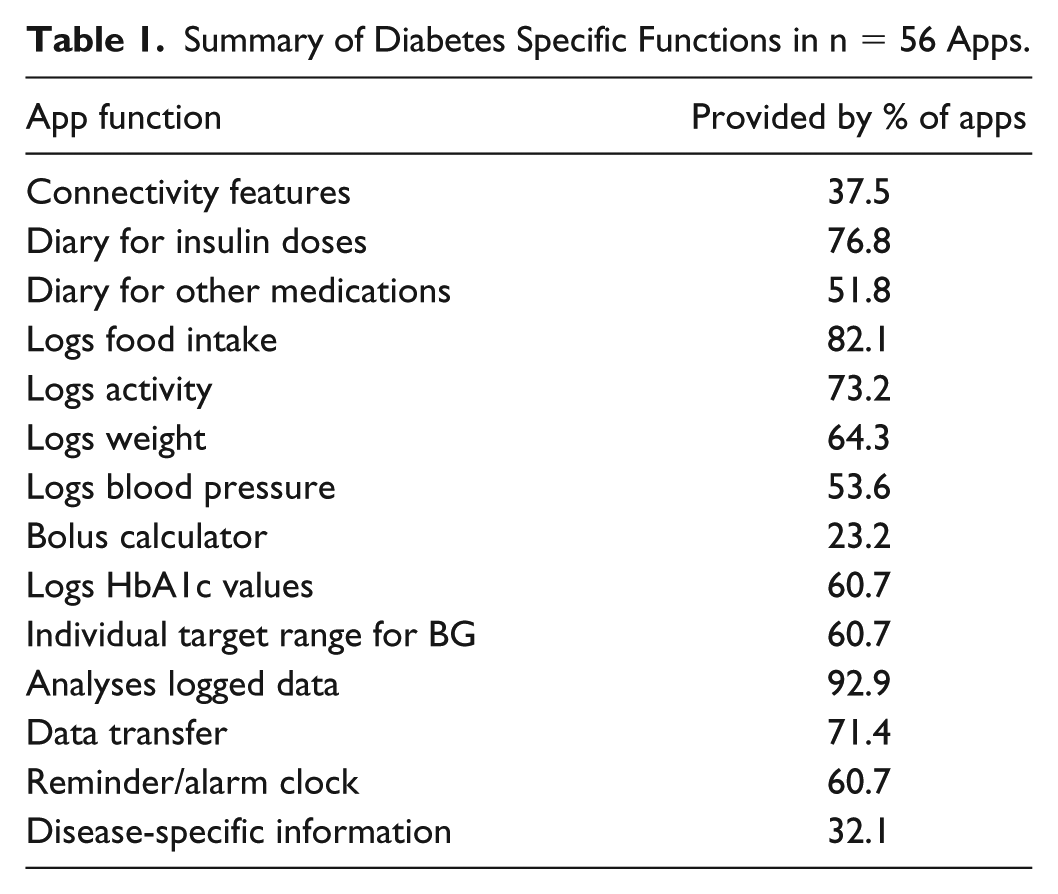
We compiled general information to characterize the available apps: number of installations, number of user reviews, average user rating, embedded advertisements, in-app purchases, source (eg, individual developers or freelancers) and user registration. In terms of diabetes-specific content and functions, we collected the following information: connectivity features with other systems (eg, fitness trackers, integration of diabetes technology), options to record insulin doses, medication, food intake, activity, weight, blood pressure, and HbA1c levels, options to set personal target ranges and reminders, analysis of logged data, data transfer, and disease-related information.
BCT and GT Ratings
We modified an established BCT taxonomy 29 to assess the implementation of 29 BCTs (see Online Appendix A). To assess the implementation of GTs, we used the gamification technique taxonomy proposed by Hoffmann et al 28 that provides detailed descriptions of 17 gamification techniques that can be applied on diabetes self-management apps (see Online Appendix B).
Two trained raters with a background in health psychology and mHealth evaluated the BCTs and GTs independently. Apps were installed on a Motorola Moto E smartphone (Motorola Inc, Chicago, IL, USA) running Android 6.0 and on a Samsung Galaxy S5 smartphone (Samsung Group, Seoul, South Korea) running Android 6.0.1. Each app was assigned a GT score between 0 and 17, representing the number of identified GTs and a BCT score between 0 and 29, representing the number of identified BCTs in the app.
We computed intraclass correlations as an index of agreement between the two raters. Descriptive statistics (mean, standard deviation, range, percentages) were calculated for general app information, diabetes-related functions, and GT and BCT scores.
Results
Key characteristics of the apps are described in detail in Online Appendix C and Online Appendix D. The 56 apps received an average user rating of 4.1 out of 5 (SD = .30). The highest rating was 5 points, the lowest user rating 3.5 points. Of the apps, 37.5% provided in-app purchases and 30.4% contained advertisements. Of the apps, 42.9% required the user to register and to disclose personal information. Table 1 summarizes the distribution of diabetes specific functions.
Summary of Diabetes Specific Functions in n = 56 Apps.
Behavior Change Techniques and Gamification Techniques
The agreement between the two raters was high (ICC = .75 for BCT; ICC = .90 for GT). The diabetes management apps implemented an average of 7.4 out of 29 BCTs (SD = 3.1; min = 2; max = 15). In case of disagreement between the raters, the coauthors discussed the app rating until a consensual agreement was arrived. Figure 1 shows the resulting distribution of BCTs across the 56 apps. Furthermore, an average of 1.4 out of 17 GTs was implemented per app (SD = 1.6; min = 0; max = 9). Discrepancies in the rating were again discussed. Figure 2 shows the resulting distribution of GTs across the 56 apps. Appendices E and F show implemented BCTs and GTs per app as well as the GT and BCT scores per app. Two BCTs (“Self-monitoring of behavior,” “Self-monitoring of outcomes of behavior”) were found in all evaluated applications. Five out of 29 BCTs (“Self-monitoring of behavior,” “Self-monitoring of outcomes of behavior,” “Conserving mental resources,” “Feedback on behavior,” and “Feedback on outcomes of behavior”) accounted for 55.8% of the BCTs identified in total. One GT (“Feedback”) accounted for 50% of the GTs identified in total, while nearly a third of 17 GTs were not listed once (eg, “Avatar”).
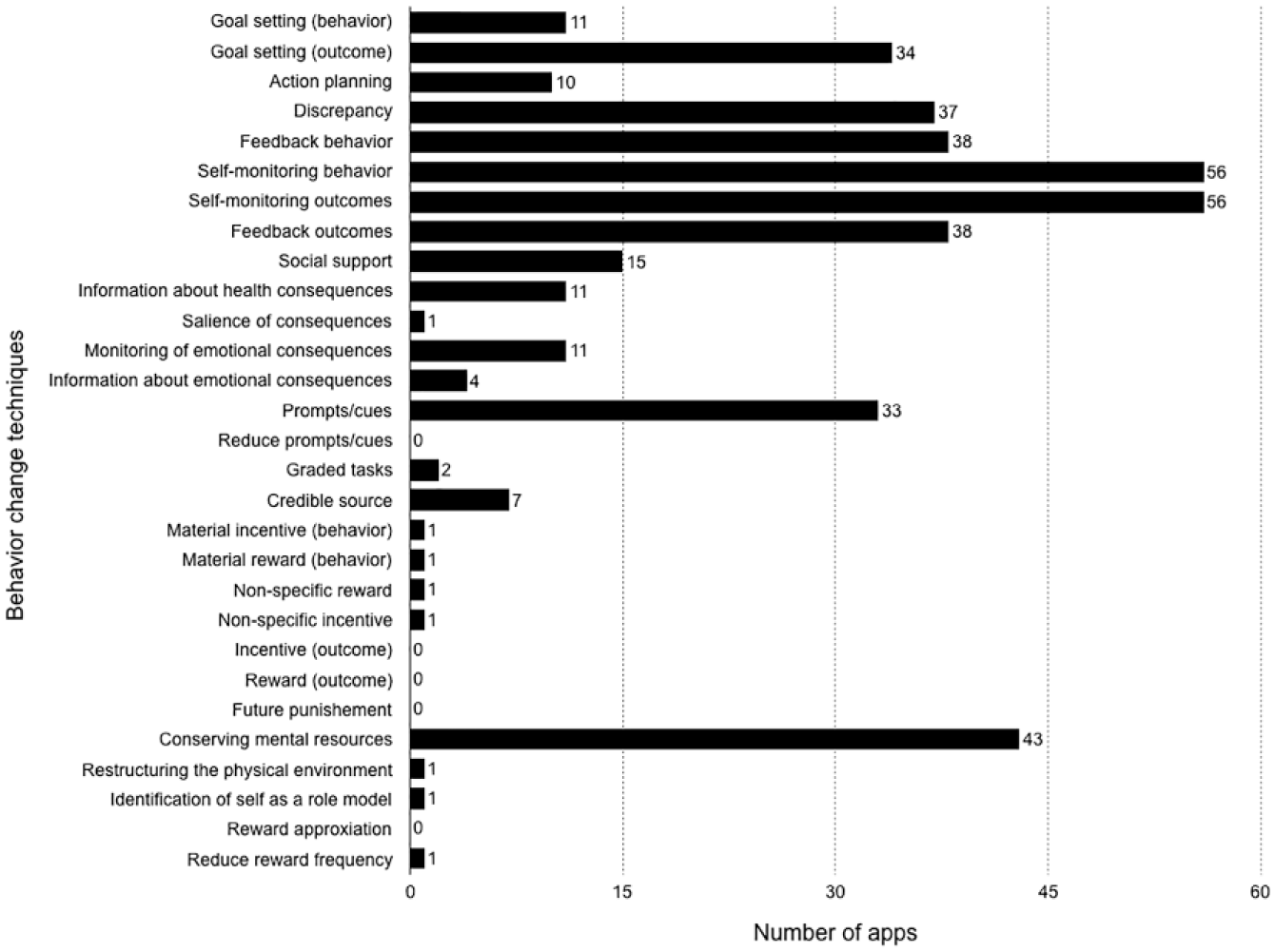
Frequency of BCT use (n = 56).
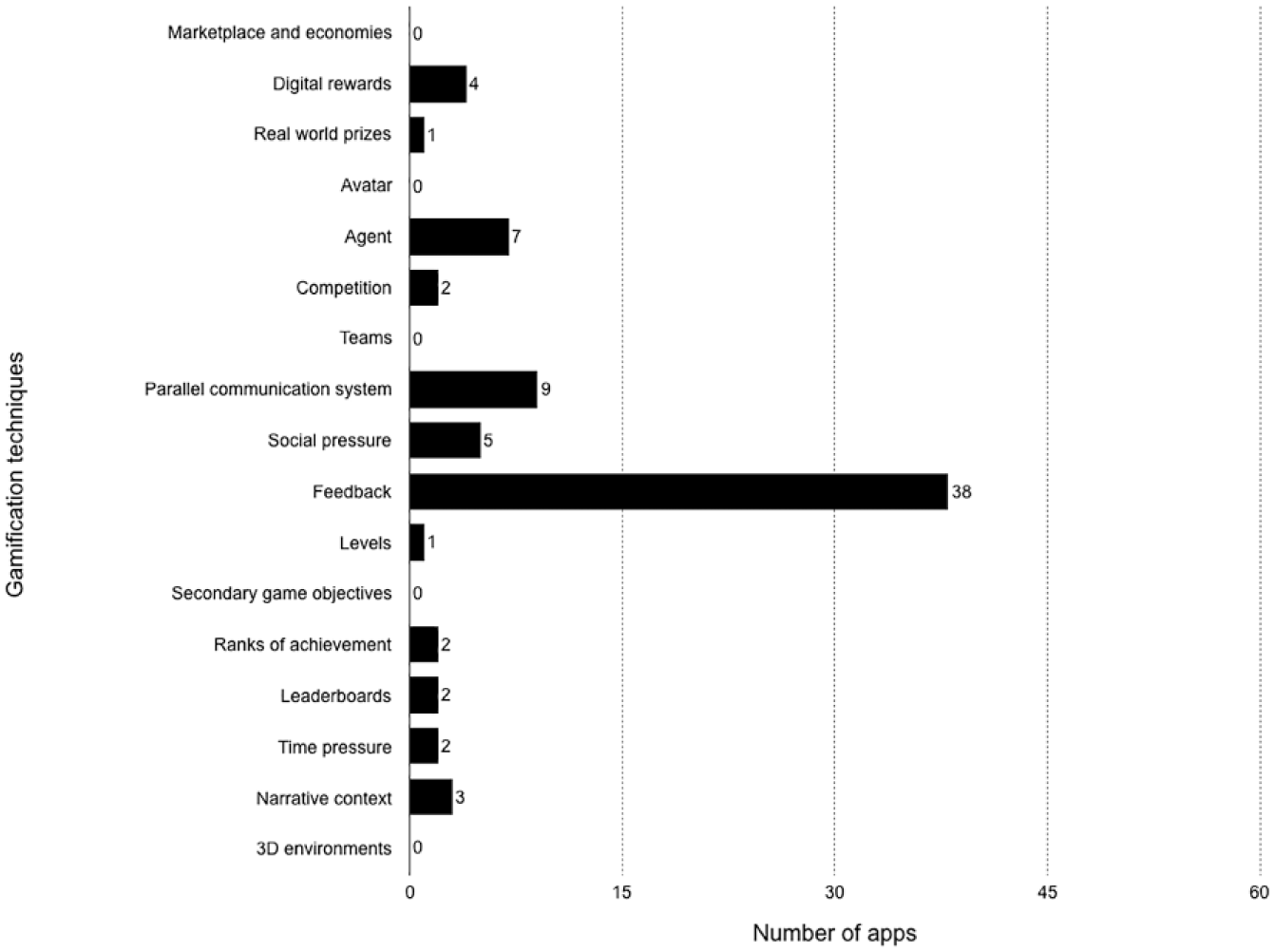
Frequency of GT use (n = 56).
Discussion
The aim of this review was to provide an overview of app functions and BCTs and gamification features in current diabetes management apps. We evaluated 56 freely available self-management apps from Google’s Play Store in regard to the implementation of BCTs and GTs. If BCTs and GTs were used, only a very restricted set of techniques was applied. Our results are in line with previous research on the implementation of gamification features and BCTs in stress management apps, 28 fitness apps 23 and apps for general health behavior change. 30 Results of a stress management app review (n = 26 freely available stress management apps from Google Play Store) showed that the apps included an average of 0.5 out of 17 GTs per app (SD = 0.7; min = 0; max = 2), indicating little to no use of GTs. 28 An average of 2.3 out of 6 GTs was found in n = 132 fitness apps. 23 The authors conclude that gamification features are frequently but unsystematically implemented. Another review on apps for different health-related goals (eg, smoking cessation) examined to which extent app designers used BCTs and GTs to influence user behavior. 30 The authors do not report GT scores but a median of 14 out of 93 BCTs in n = 64 iOS and Android health apps.
In terms of the prominent role of self-monitoring for successful diabetes self-management, it is not surprising that the BCTs with obvious links to self-management tasks (“Self-monitoring of behavior,” “Self-monitoring of outcomes of behavior”) were implemented most frequently (n = 56). The same holds for the two BCTs found in 67.9% of the apps (“Feedback on behavior,” Feedback on outcomes of behavior”) and the most frequent GT (“Feedback,” n = 38) as feedback on logged blood glucose data is a key information for adequate blood glucose control. Especially BCTs and GTs involving rewards or incentives were implemented rarely (eg, “Digital rewards,” n = 4). The frequent implementation of self-monitoring and feedback related techniques as well as the rare use of rewarding features in diabetes management apps is in line with the results of previous health app reviews.23,28,30 The use of incentives should be considered on a more regular basis as the effectiveness of health apps providing rewarding features has been assessed in several studies.21-22
Limitations
We limited our evaluation to smartphone applications from Google’s Play Store and did not include applications for iOS/Apple devices. In addition, the review only includes freely available applications. As 93.5% of Android apps are free, 31 our restriction on freely available apps should not limit our findings substantially. Furthermore, the overall app store supply changes continually and the applications that matched our search term are a mere snapshot. It is at least important to notice that on the one hand, several BCTs and GTs are dependent and not always distinct. Particularly some gamification techniques show content-related overlaps (eg, “Levels”/“Ranks of achievement” or “Teams”/“Social pressure”). On the other hand, there are BCTs and GTs with similar names but different rating criteria, for example, the BCT “Reward (outcome)” and the GT “Digital rewards.” In coding the GTs, the raters particularly paid attention to the game-like character of the rewards (eg, points, badges), whereas the criteria for BCT differ from these game-like features. Hence, apps that qualified the criteria for GT reward mechanisms did not necessarily fulfil the stricter BCT criteria leading to different BCT and GT scores for rewarding functions. Since studies on the effectiveness of gamification features and BCTs in health apps are lacking, we are consequently not able to recommend a minimal set of BCTs/GTs needed to improve user engagement. Nevertheless, a pilot study by Cafazzo et al indicates that the use of a diabetes management app that implemented two gamification principles (digital rewards and socializing through parallel communication systems) increases the frequency of blood glucose checks by 50% among adolescents with type 1 diabetes. 21
Conclusion
This app review provides an overview of app functions, BCTs, and gamification features in current Android diabetes management apps (n = 56). Our review revealed that BCTS and GTs are scarcely used and that their potential has not been fully exploited yet. Since studies usually focus on relatively short periods of active app use, 32 the effects on longer-term user engagement remain unclear. 14 The implementation of BCTs and GTs, however, may provide suitable strategies and should be considered more often. The indication of single BCTs and GTs warrants for more in-depth systematic research, as it seems plausible that not all GTs/BCTs are appropriate for all individuals and all age. The efficacy of GTs/BCTs should be further examined (eg, in randomized controlled trials) to generate scientifically rooted input for app design.
Supplemental Material
Online_Appendix – Supplemental material for Gamification and Behavior Change Techniques in Diabetes Self-Management Apps
Supplemental material, Online_Appendix for Gamification and Behavior Change Techniques in Diabetes Self-Management Apps by Lilli Priesterroth, Jennifer Grammes, Kimberly Holtz, Anna Reinwarth and Thomas Kubiak in Journal of Diabetes Science and Technology
Footnotes
Abbreviations
BCT, behavior change technique; BG, blood glucose; GT, gamification technique; mHealth, mobile health.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.