
Abstract
Background:
Medical practices face challenges of time and cost pressures with scarce resources. Point-of-care testing (POCT) has the potential to accelerate processes compared to central laboratory testing and can increase satisfaction of physicians, staff members, and patients. The objective of this study was to evaluate the effects of introducing HbA1c POCT in practices specialized in diabetes.
Method:
Three German practices that manage 400, 550, and 950 diabetes patients per year participated in this evaluation. The workflow and required time before and after POCT implementation (device: Alere Afinion AS100 Analyzer) was evaluated in each practice. Physician (n = 5), staff (n = 9), and patient (n = 298) satisfaction was assessed with questionnaires and interviews.
Results:
After POCT implementation the number of required visits scheduled was reduced by 80% (88% vs 17.6%, P < .0001), the number of venous blood collections by 75% (91% vs 23%, P < .0001). Of patients, 82% (vs 13% prior to POCT implementation) were able to discuss their HbA1c values with treating physicians immediately during their first visit (P < .0001). In two of the practices the POCT process resulted in significant time savings of approximately 20 and 22 working days per 1000 patients per year (95% CI 2-46; 95% CI 10-44). All physicians indicated that POCT HbA1c implementation improved the practice workflow and all experienced a relief of burden for the office and the patients. All staff members indicated that they found the POCT measurement easy to perform and experienced a relief of burden. The majority (61.3%) of patients found the capillary blood collection more pleasant and 83% saw an advantage in the immediate availability of HbA1c results.
Conclusions:
The implementation of HbA1c POCT leads to an improved practice workflow and increases satisfaction of physicians, staff members and patients.
In diabetes treatment HbA1c is a pivotal pathology test used around the world for the long-term management of patients. Point-of-care testing (POCT) provides a convenient approach for conducting glycated hemoglobin testing outside the laboratory. Several studies demonstrated comparable or also superior outcomes as compared to laboratory testing under controlled conditions.1-6 Considering the fact that medical practices often struggle with time and cost pressure as well as scarce resources, POCT has the potential to optimize the processes taking place in the office. 7 Once properly implemented into the practice workflow, it can accelerate and streamline processes compared to laboratory testing and thus free up resources. Switching from conventional laboratory testing to POCT can shorten the time to decision-making about further treatment as there is less delay due to blood sample preparation and transport. One additional advantage is the immediate availability of test results, allowing a prompt review of results and therapy with the patient obviating the need to schedule further office visits or phone calls. 8 Further positive effects of POCT for HbA1c include better patient compliance to therapy, 9 a higher level of patient satisfaction7,10,11 and a greater patient loyalty, as a result of practice’s reputation for applying state-of-the art technology. 12 In addition to better medical outcomes in terms of improved diabetes management and glycemic control, 13 an optimization of processes can also lead to lower costs and economic benefits.14,15
The objective of this evaluation is to demonstrate the impact of POCT compared to standard laboratory testing with the example of HbA1c measurement in practices specialized in diabetology.
Methods
We performed a pre-post comparison in terms of quantity and quality with regard to HbA1c POCT implementation in medical practices specialized in diabetology. Impact on practice processes and physicians, staff, and patient satisfaction were evaluated. For HbA1c testing in practices the Alere Afinion™ AS100 Analyzer was used.
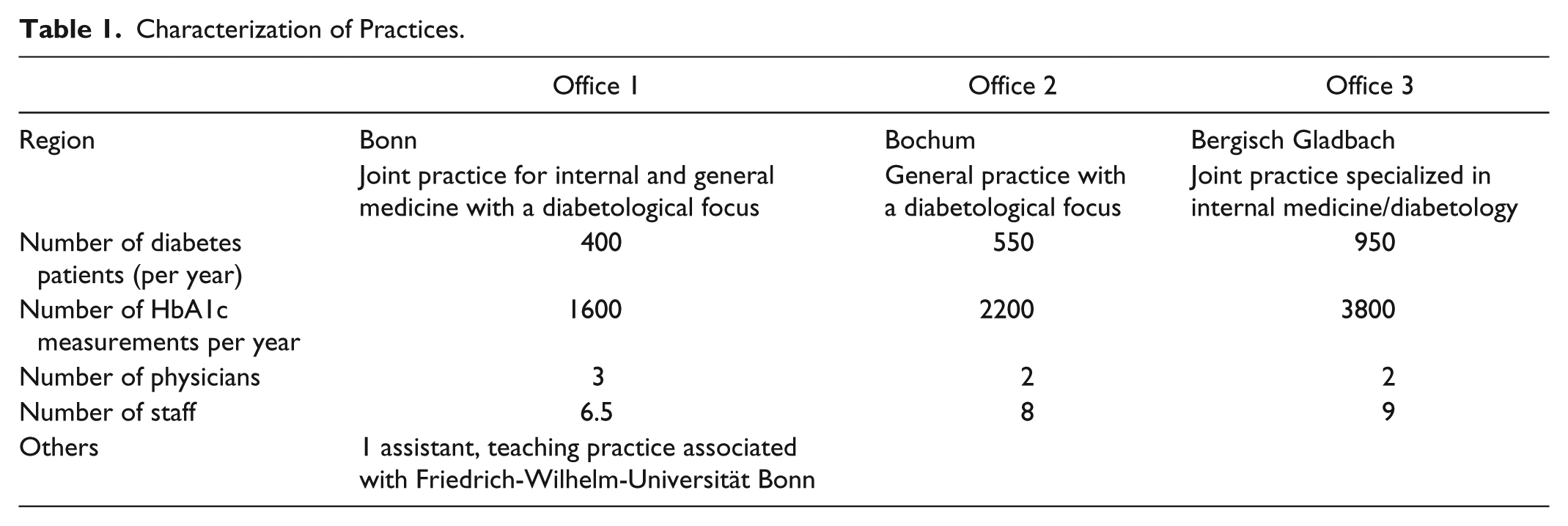
Three offices situated in the German cities Bonn, Bochum, and Bergisch-Gladbach with a total of 7 physicians and 23.5 staff members/physician assistants participated in the eight-month study (April-December 2015). The practices were of different size with 400, 550, and 950 diabetes patients. As guidelines suggest, patients get their HbA1c value measured every quarter, resulting in 1600, 2200, and 3800 HbA1c measurements per year, respectively (Table 1). As a standard of care, two appointments were scheduled with each patient for their quarterly therapy control. At the first appointment, venous blood was sampled and sent to the laboratory. These “lab” appointments were typically scheduled for the early morning. The second appointment was scheduled when lab results are available and physicians can discuss therapy adjustments with the patients.
Characterization of Practices.
To investigate the impact of HBA1c POCT implementation the following methods were applied:
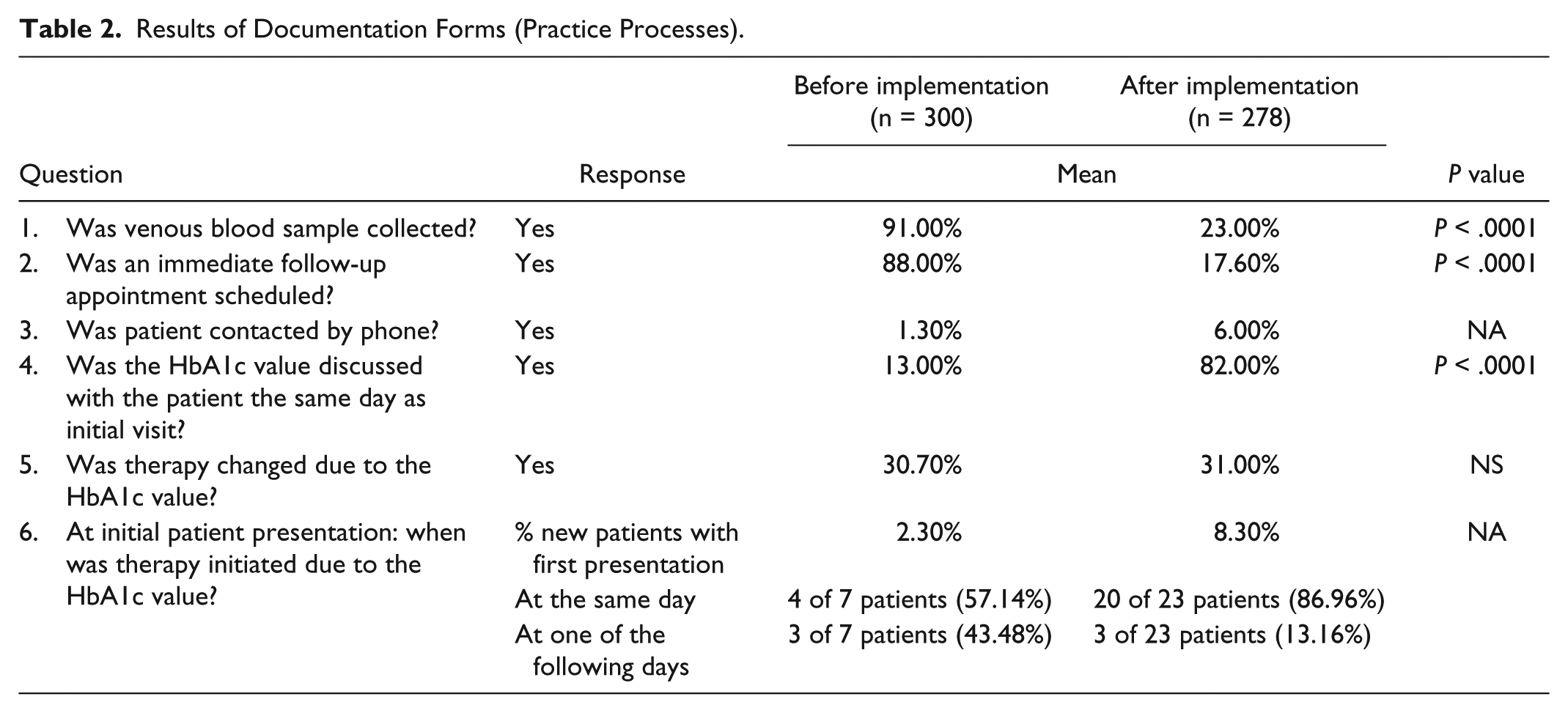
To capture assessment processes for HbA1c determination, physicians were asked to fill out documentation forms concerning participating diabetes patients. The target was to fill out documentation forms for 100 patients per practice before and after implementation of HbA1c POCT each. The documentation form was attached to the patients’ file and should be completed during the patients’ stay in practice. In each case there were six questions with given answers (yes or no / same day or following day) to be answered. The following questions were asked: 1. “Was venous blood sample collected?” 2. “Was an immediate follow-up appointment scheduled?” 3. “Was patient contacted by phone?” 4. “Was the HbA1c value discussed with the patient the same day as initial visit?” 5. “Was therapy changed due to the HbA1c value?” 6. “At initial patient presentation: when was therapy initiated due to the HbA1c value?” (Table 2).
Results of Documentation Forms (Practice Processes).
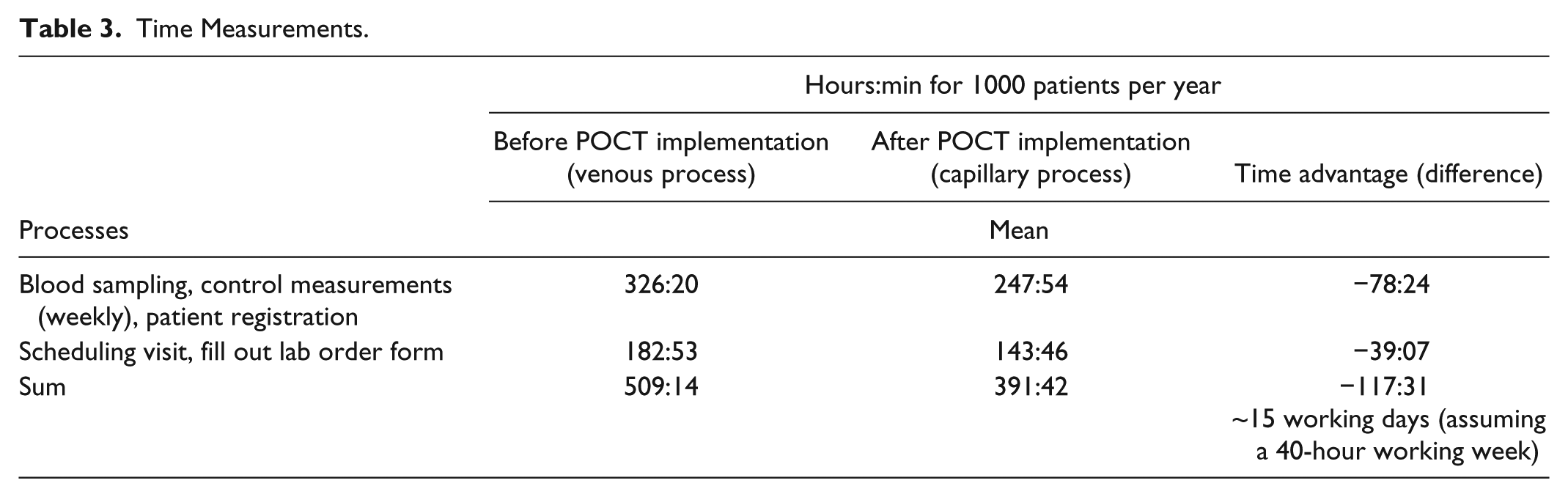
2. To compare the times needed for the processes before and after implementation of HbA1c POCT, time measurements of the following steps have been performed: 1. Venous blood collection: A tourniquet was placed. The procedure ended with completed blood sample preparation for shipment to the external laboratory including labelling test tubes. 2. Filling out laboratory order forms. 3. Capillary blood collection: It started with the opening of the test cartridge foil pouch and ended with the start of the measurement with the Alere Afinion AS100 Analyzer (click on the start button). 4. Patient registration at the reception desk. 5. Scheduling of patient visits at the desk or by telephone. 6. Quality control of the HbA1c test, which is required to be performed weekly in Germany if POCT is used. The manufacturer recommends that a quality control of the HbA1c test should be performed with each new shipment or lot of test kits, after unexpected test results and after training of new staff members quality control. 16
The results were used to calculate the time requirement for 1000 patients a year—expressed in total hours and minutes (Table 3). Venous process included 4 HbA1c measurements per year (quarterly); capillary process included 3 capillary HbA1c measurements with POCT device per year and 1 venous measurement by laboratory testing. It was assumed that at least once per year additional blood parameters are measured which may require laboratory testing. Lipids and the albumin creatinine ratio (ACR) may also be measured with the Alere Afinion AS100 Analyser.
Time Measurements.
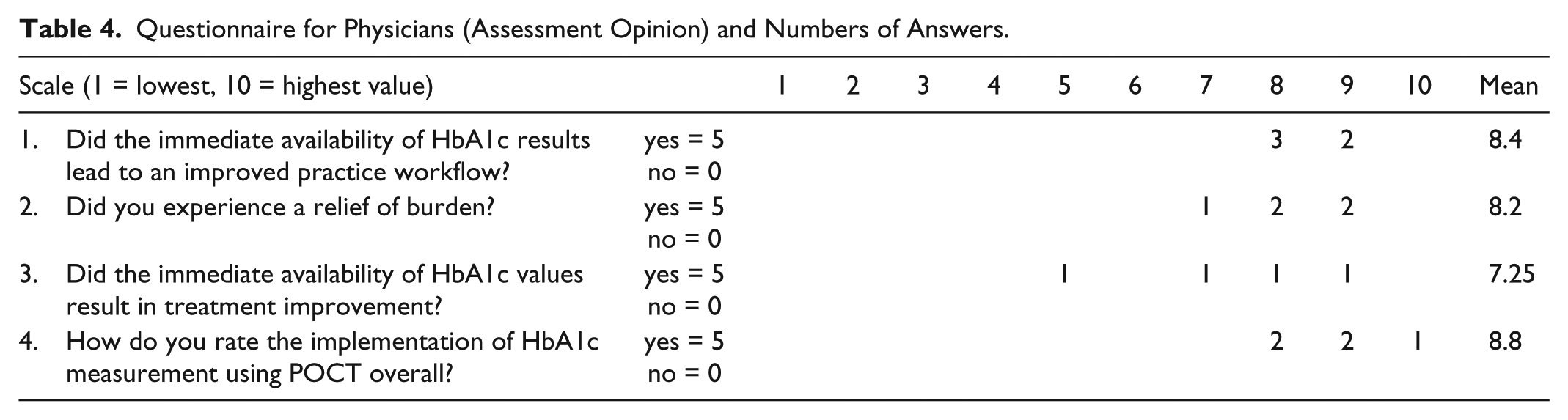
3. To evaluate the impact of HbA1c POCT participating physicians, staff members and patients completed written questionnaires with both open and closed questions. Physicians were asked the following questions: 1. “Did the immediate availability of HbA1c results lead to an improved practice workflow?” 2. “Did you experience a relief of burden?” 3. “Did the immediate availability of HbA1c values result in treatment improvement?” 4. “How do you rate the implementation of HbA1c measurement using POCT overall?” In the case of a yes response, scale ratings (1 = lowest value to 10 = highest value) and short open responses were captured (Tables 4 and 5). Staff members were asked to respond to the following six multiple-choice questions about the HbA1c measurement process and impact of POCT: 1. “How did you experience testing with the Alere Afinion AS100 Analyzer?” 2. “How do you assess the finger-stick capillary blood collection?” 3. “Is there any difference between capillary and venous blood collection in terms of the time needed?” 4. “Did you avoid telephone conversations?” 5. “Has the process for scheduling appointments become easier?” 6. “Did you experience a relief of burden for yourself?” Also, open responses were captured (Table 6). Patients’ opinions were evaluated through written questionnaires and collection of open statements. The following questions were asked: 1. “How did you experience the finger-stick blood collection in comparison to a venous blood collection?” 2. “Which one would you prefer?” 3. “Your HbA1c value is being tested directly in your physician’s office. Do you see an advantage in this approach?”
Questionnaire for Physicians (Assessment Opinion) and Numbers of Answers.
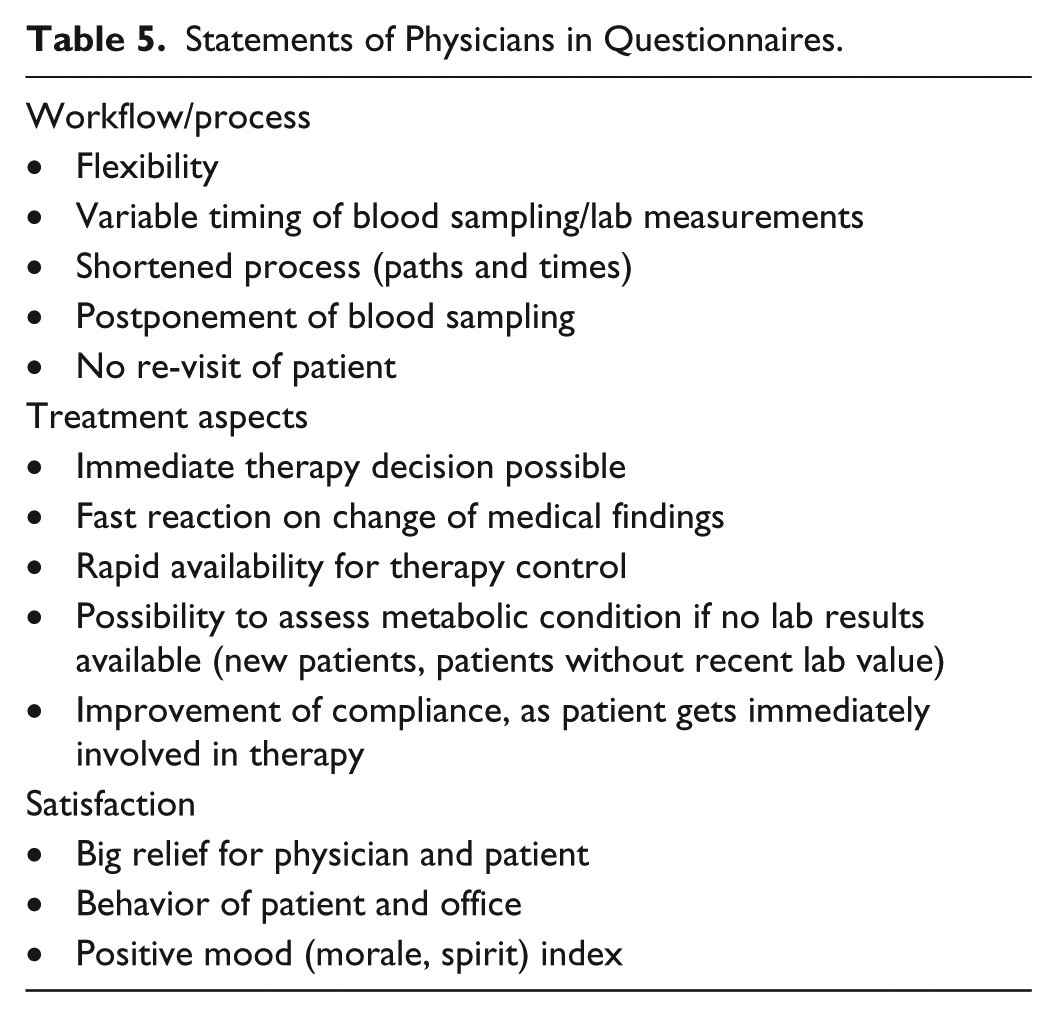
Statements of Physicians in Questionnaires.
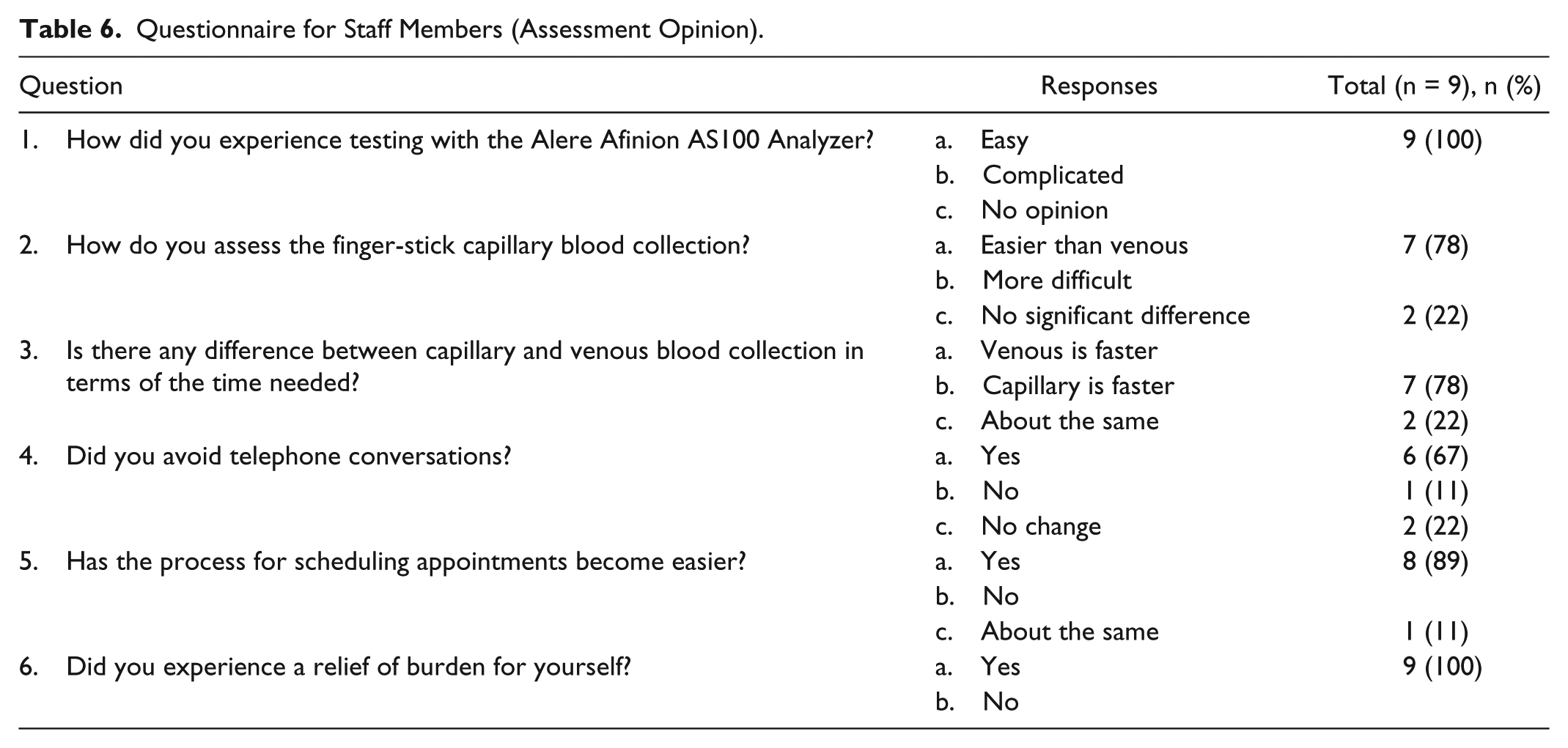
Questionnaire for Staff Members (Assessment Opinion).
Results
Documentation Forms
In total 578 evaluable documentation forms from all practices were analyzed: n = 300 before POCT implementation; n = 278 after implementation (Table 2).
Distinct differences in assessment processes before and after POTC implementation could be observed. The mean numbers of required venous blood collections were reduced by 75% (Figure 1). Before implementation of POCT 91% (95% CI 87.56-94.26) of diabetes patients had venous blood samples taken (9% used direct laboratory testing and presented HbA1c results to practices)—versus 23% (95% CI 18.20-28.42) after implementation of POCT. Also scheduled revisits decreased by 80% after POCT implementation: 88% (95% CI 83.78-91.45) of the patients scheduled a new appointment for discussion of results after testing whereas after POCT implementation only 17.6% (95% CI 13.33-22.62) required a follow-up appointment to be scheduled. Phone calls to inform patients about their laboratory results remained on a relatively low level (1.30% vs 6.00%) (Figure 1).
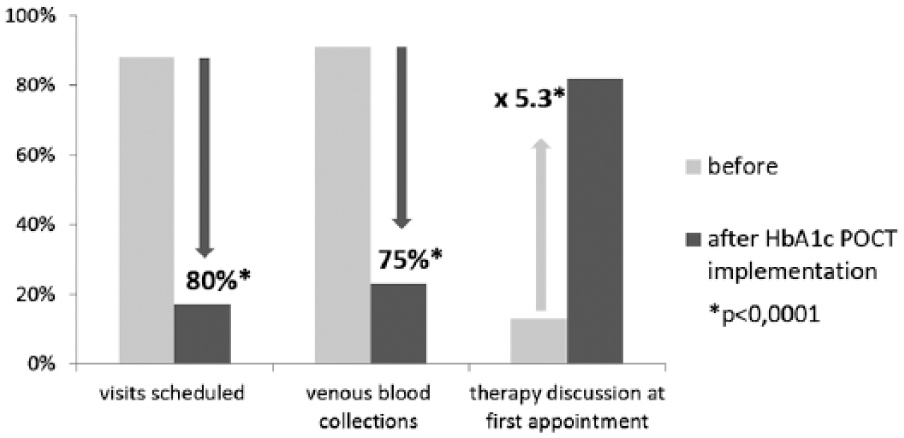
Decrease in numbers of practice processes (comparison before and after HbA1c POCT implementation).
After POCT implementation, physicians discussed HbA1c values with patients more often at the same day (13% compared to 82%; P < .001). The use of HbA1c POCT in this study however did not show an effect on the percentage of patients, who had subsequent therapy changes as a result of their testing (30.7% vs 31%).
The number of patients in the “same day” or “one of the following days” therapy initiation groups was too low to make meaningful conclusions about impacts of POCT (7 vs 23 patients ≙ 2.3% vs 8.3% in the before and after POCT implementation groups). However after POCT implementation immediate therapy initiation for new patients was more frequent (20 of 23 patients) than therapy initiation at a later date (3 of 23 patients). This indicates that the immediate availability of the HbA1c results allows for a faster therapy decision.
Time Measurements
The mean time exposure before rapid test availability projected to 1000 patients per year was calculated at 509:14h (Table 3). After POCT implementation, the amount of time all practices together had to spend for HbA1c measurement and corresponding activities was substantially less: 391:24h for 1000 patients per year. With POCT implementation all practices in aggregate reduced their expenditure on average by 78:25h projected to 1000 patients per year—excluding time spent for scheduling and filling out lab order forms. Including time spent for scheduling and filling out lab order forms the yearly time saving associated with POCT implementation increased to 117:31h per 1000 patients on average. This corresponded with approximately 15 working days per year, based on a 40-hour work week. In two of the practices, the POCT process resulted in significant time savings, approximately 20 and 22 working days (respectively), per 1000 patients per year (95% CI 2-46; 95% CI 10-44). For the third practice, however no data were collected on time required for filling out order forms and visit scheduling. In this practice, the time spent on capillary blood sampling was almost 4 times higher than in the other practices—as such no time savings were associated with POCT implementation. Based on the numbers of diabetes patients and the specific working hour, the Bonn and Bergisch Gladbach practices saved approximately 10 days (400 diabetes patients, 32 hours per week) and 22 days (950 diabetes patients, 38.5 hours per week) per year, respectively.
Questionnaire for Physicians
When questioned whether the direct availability of HbA1c results led to an improved practice workflow, all physicians (n = 5) confirmed that it did (Table 4). The average score of the scale rating was 8.4 out of a possible 10. Open statements provided by the physicians pointed to improvement of “flexibility,” “behavior of patient and office,” “rapid availability for therapy control,” and “variable timing of blood sampling/lab measurements.” When questioned “Did you experience a relief of burden?” and “Did immediate availability of HbA1c values result in treatment improvement?” all physicians answered positively (average scores of 8.2 and 7.25, respectively). Open comments regarding workload included “immediate therapy decision possible,” “postponement of blood sampling,” and “possibility to assess metabolic condition if no lab results available” (Table 5). Open comments on treatment were “fast reaction on change of medical findings,” “no re-visit of patient,” or “improvement of compliance, as patient gets immediately involved in therapy.” The statement that earned the highest average score (8.8) on the physicians’ questionnaire was “How do you rate the implementation of HbA1c measurement using POCT overall?” Scores ranged between 7.25 and 8.8, and corresponding remarks such as “big relief for physician and patient,” “positive mood (morale, spirit) index,” and “shortened process (paths and times)” suggest high satisfaction of participating doctors with POCT implementation (Table 5).
Questionnaire for Staff Members
All staff members (n = 9) agreed that operating the POCT device was simple. 7 of 9 (78%) reported finger-stick capillary blood collection as being easier than venous blood sampling; 2 of 9 (22%) did not report significant difference (Table 6). Most participants (7 of 9, 78%) considered capillary blood collection to be faster than venous blood sampling; 2 of 9 (22%) described the procedure as being similar in terms of the time required.
Other survey questions dealt with change of practice processes through immediate availability of HbA1c value: 6 of 9 (67%) staff members felt that they could reduce telephone conversations, 8 of 9 considered the process for scheduling appointments easier with POCT; all of the assistants experienced a relief of burden for themselves. In addition, open comments on the impact of POCT were mostly positive and ranged from “measurement was easy and safe” and “less laboratory patients and therefore load relief in the laboratory” to “patients had less fear” and “results available within a narrow time frame / short waiting times / patient gets informed immediately.”
Questionnaire for Patients
Of participating patients, 62.1% (n = 298) experienced finger-stick blood collection as more pleasant in comparison to venous blood collection, 26.5% could not see any difference, only 8.1% regarded it as less pleasant (Table 7). Corresponding to this result most patients (49.4%) prefer finger-stick blood collection, only 10.4% prefer venous blood collection (36.9% = it doesn’t matter; 3.3% = missing response). Of patients, 82.6% agreed that there was an advantage to measuring HbA1c values directly in the physician’s office. And 11.7% did not see a benefit (5.7% missing response).
Questionnaire for Patients (Assessment Opinion).
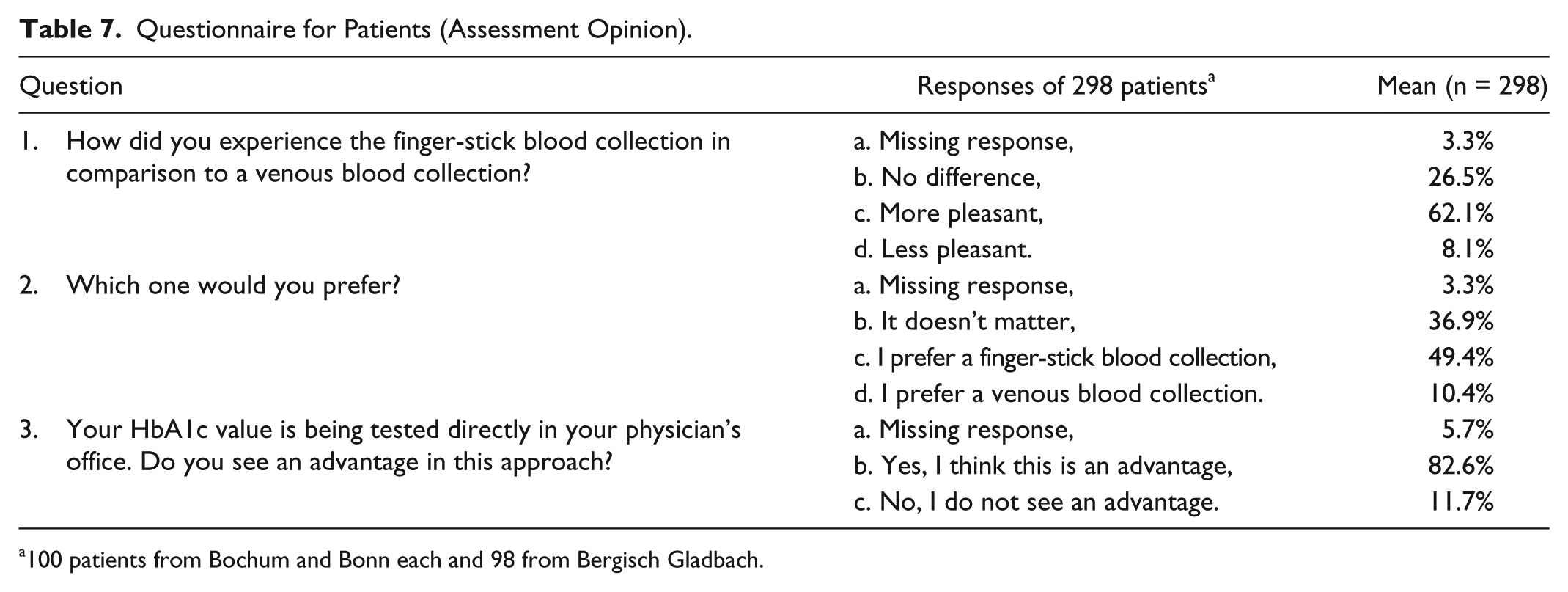
100 patients from Bochum and Bonn each and 98 from Bergisch Gladbach.
Of 298 patients, 124 provided additional information in the form of short open comments. Most of the statements (n = 122, 98%, several statements possible) referred to positive aspects of treatment processes such as “results immediately available,” “faster,” and “direct discussion of results with physician” (n = 84, 68%) or to time saving such as “saves one office appointment” (n = 25, 20%). Another set of responses was related to aspects of comfort (n = 28, 23%) containing statements such as “more pleasant” (n = 10, 8%), “painless” (n = 6, 5%), and “arm vein gets less burdened” (n = 5, 4%).
The majority of interviewed diabetes patients provided a positive response to POCT stating that the measurement was more pleasant and less painful and results were faster available and discussable.
Discussion
The present evaluation demonstrates that the implementation of POCT for HbA1c measurements in practices specialized in diabetology can improve office processes as well as increase satisfaction of physicians, staff members, and patients. It shows a significant acceleration of assessment processes due to a reduction of time-consuming venous blood collections, scheduling tasks and patient revisits. Applying POCT, the number of required venous blood collections in this survey was significantly reduced by 75%. The number of visits scheduled was reduced by 80%. Simultaneously, the numbers of patients, that discussed HbA1c results and therapy directly during the first office visit, increased by 6-fold. This resulted—along with faster procedures in terms of patient registration and paperwork—in considerable time savings for the examined practices (Figure 2). More than 15 working days a year per 1000 patients were saved. Accordingly, physicians and staff members experienced a relief of burden for the office after POCT implementation. The satisfaction of patients also increased. The majority experienced the capillary blood collection as more pleasant and appreciated faster availability of the HbA1c results and less office visits.
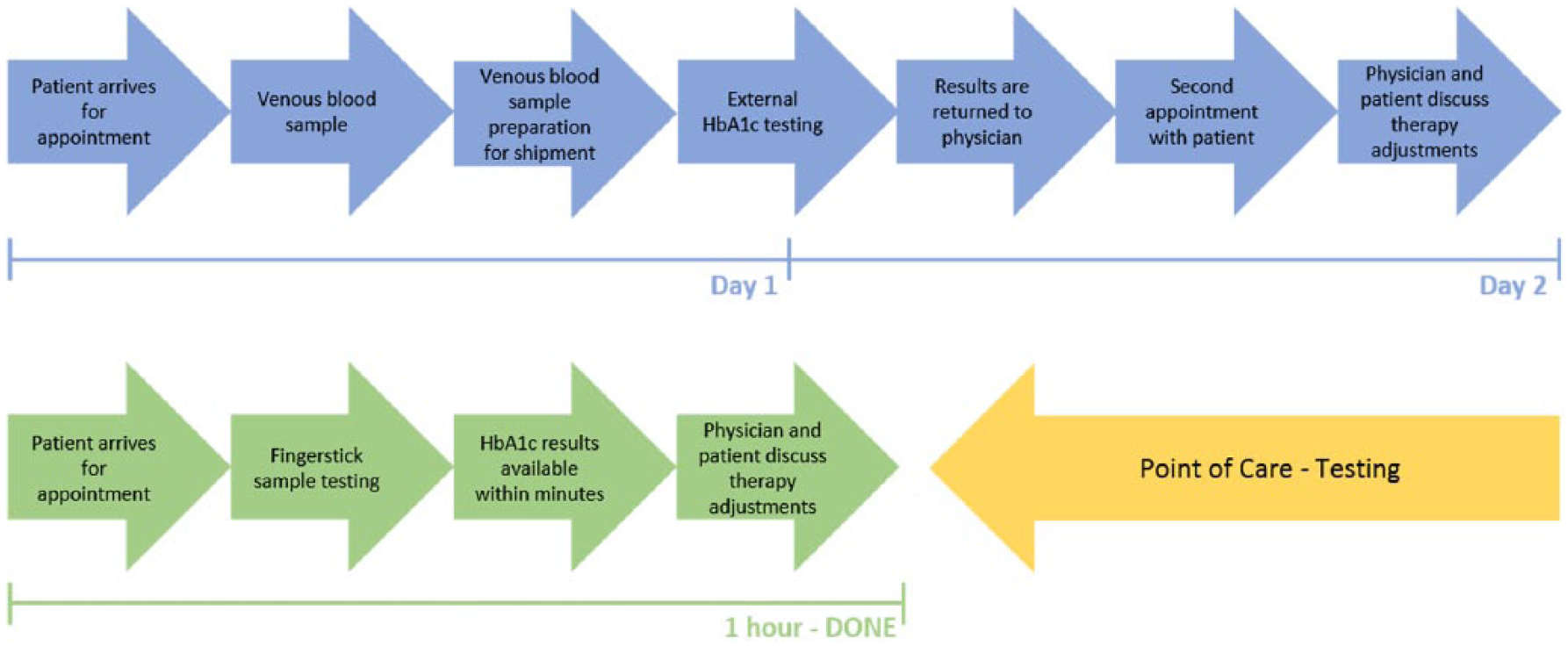
Time required for POCT compared to standard HbA1c measurements.
Up to now most studies concerning HbA1c POCT investigated either the treatment effects1-6, 13 or the quality of measurement in relation to laboratory testing. 17 The advantages regarding workflow of HbA1c POCT compared to laboratory tests were evaluated in an earlier study: Crocker and colleagues observed decreasing numbers of ordered tests, letters and phone calls to patients as well as revisits and concluded in line with our results, that POCT can significantly improve clinical operations with cost reductions through improved practice efficiency. 7 The authors confirmed their findings with a second study, investigating the impact of POCT on practice efficiency in an academic primary care practice. 18 Another investigation of the same group strongly indicates a high level of patient satisfaction with on-site POCT in a primary care setting. 19 In a POCT study of 4968 patients—among them 1262 diabetes patients—patients’ satisfaction and acceptability increased due to faster availability of test results and faster therapy discussions with physicians. 10 Our study confirmed the fact that not only patients but also doctors and staff members see substantial advantages in the implementation and use of HbA1c POCT: POCT mainly based on capillary blood sampling versus laboratory testing based on venous blood sampling is considered to be technically faster and more resource-efficient. This also avoids follow-up appointments for discussing potential therapy changes with diabetes patients. However, our study was limited by the relatively small number of evaluated physicians’ offices. Numbers of surveyed and interviewed doctors and staff members should be increased in future studies. Overall it is of high interest to investigate the impact of POCT on the organizational and medical processes of physicians’ practices specialized in diabetes treatment more closely. Potential cost reductions or revenue growth of practices from the POCT time savings might be of further interest.
Conclusion
The implementation and use of HBA1c POCT leads to an improved and more efficient work flow in outpatient medical practices and can increase satisfaction of physicians, staff, and patients.
Footnotes
Acknowledgements
We thank investigators, doctors, and staff of practices for participating on the study.
Abbreviations
ACR, albumin creatinine ratio; NA, not applicable; NS, not significant; POCT, point-of-care testing.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: KHP is an employee of Sciarc GmbH. SE is an employee of Alere GmbH. OS has given lectures for companies that are involved in HbA1c POCT and is CEO and founder of Sciarc GmbH. PA, KG, GK, AP, MR, and MZ have no conflicts of interest.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was funded by Alere GmbH.