
Abstract
Background:
The aim of this study was to analyze the persistence with oral antihyperglycemic drugs in type 2 diabetes mellitus (T2DM) patients with dementia in Germany.
Methods:
This study included adults with T2DM who were treated with oral antihyperglycemic drugs and were diagnosed with dementia in 1262 German general practices between January 2013 and December 2015 (index date). Dementia cases were matched (1:1) to controls without dementia by age, gender, type of practice, type of residence, physician, and initial antihyperglycemic therapy, using a propensity score method. The primary outcome of the study was the rate of persistence with oral antihyperglycemic drugs in dementia cases and controls without dementia in the year following the index date. Persistence was estimated as therapy time without treatment discontinuation, which was defined as at least 90 days without oral antihyperglycemic therapy. Cox regressions were used to determine the impact of dementia on persistence with oral antihyperglycemic treatment in the entire population and in different subgroups.
Results:
This study included 848 T2DM patients with dementia and 848 T2DM patients without dementia. In the dementia group, 39.2% of patients were men, while the control group included 40.8% men. After 12 months of follow-up, 72.7% of dementia cases and 71.4% of controls without dementia were persistent (P = .291). No significant association was found between dementia and persistence with oral antihyperglycemic drugs in the entire population and in different subgroups (HR ranging from 0.84 to 1.25).
Conclusions:
Dementia did not have a significant impact on persistence with oral antihyperglycemic drugs in T2DM patients in Germany.
Throughout the world, more than 422 million people suffer from diabetes, with 90% of them being affected by type 2 diabetes mellitus (T2DM). 1 In 2012, diabetes and high blood glucose were involved in 1.5 million and 2.2 million deaths worldwide, respectively. 1 With a prevalence of almost 6 million individuals in Germany, 2 T2DM has an important impact on the health and economy of this country. 3
T2DM, a chronic disorder closely associated with age-related physiopathological dysregulation, is mainly found in the elderly. 4 Therefore, many patients with T2DM are also affected by dementia, in particular Alzheimer’s disease and vascular dementia. 5 Various studies have reported low persistence with treatments in people diagnosed with dementia, probably due to the memory loss and lack of concentration associated with the disease.6,7 In 2014, Haider and colleagues discovered that around half of dementia patients discontinued their antidementia medication within the year of initiation. 8 Two years later, Booker et al showed that more than 52% of dementia patients treated with antidepressants stopped medication intake after 6 months of follow-up. 9 Although these findings suggest that treatment persistence is insufficient and needs to be improved in dementia, no study has yet focused on the rate of persistence with antidiabetics in elderly patients diagnosed with dementia.
Therefore, the goal of the present study was to analyze the persistence with oral antihyperglycemic drugs in T2DM patients with dementia in Germany.
Methods
Database
This retrospective study is based on data from the Disease Analyzer database (QuintilesIMS). The database compiles demographical, clinical, and pharmaceutical data obtained in an anonymous format from computer systems used in clinical practices. 10 The quality and exactness of the data (eg, diagnoses and drug prescriptions) are regularly assessed by QuintilesIMS. Using prescription statistics for several drugs and age groups for several diagnoses, the Disease Analyzer database has been found to be a representative database of clinical practices in Germany. 10 Finally, this database has already been used in studies focusing on T2DM.11-13
Study Population
This study included adults with T2DM who were treated with oral antihyperglycemic drugs and were diagnosed with dementia (ICD-10: F01, F03, G30) in 1262 general practices in Germany between January 2013 and December 2015 (index date). To be included, individuals also had to be followed for at least 12 months prior to the index date. After applying similar inclusion criteria, dementia cases were matched (1:1) to controls without dementia by age, gender, type of practice (diabetologist versus nondiabetologist care), type of residence (nursing home versus home-care setting), physician, and initial antihyperglycemic therapy (metformin versus another oral drug; see Figure 1), using a propensity score method.
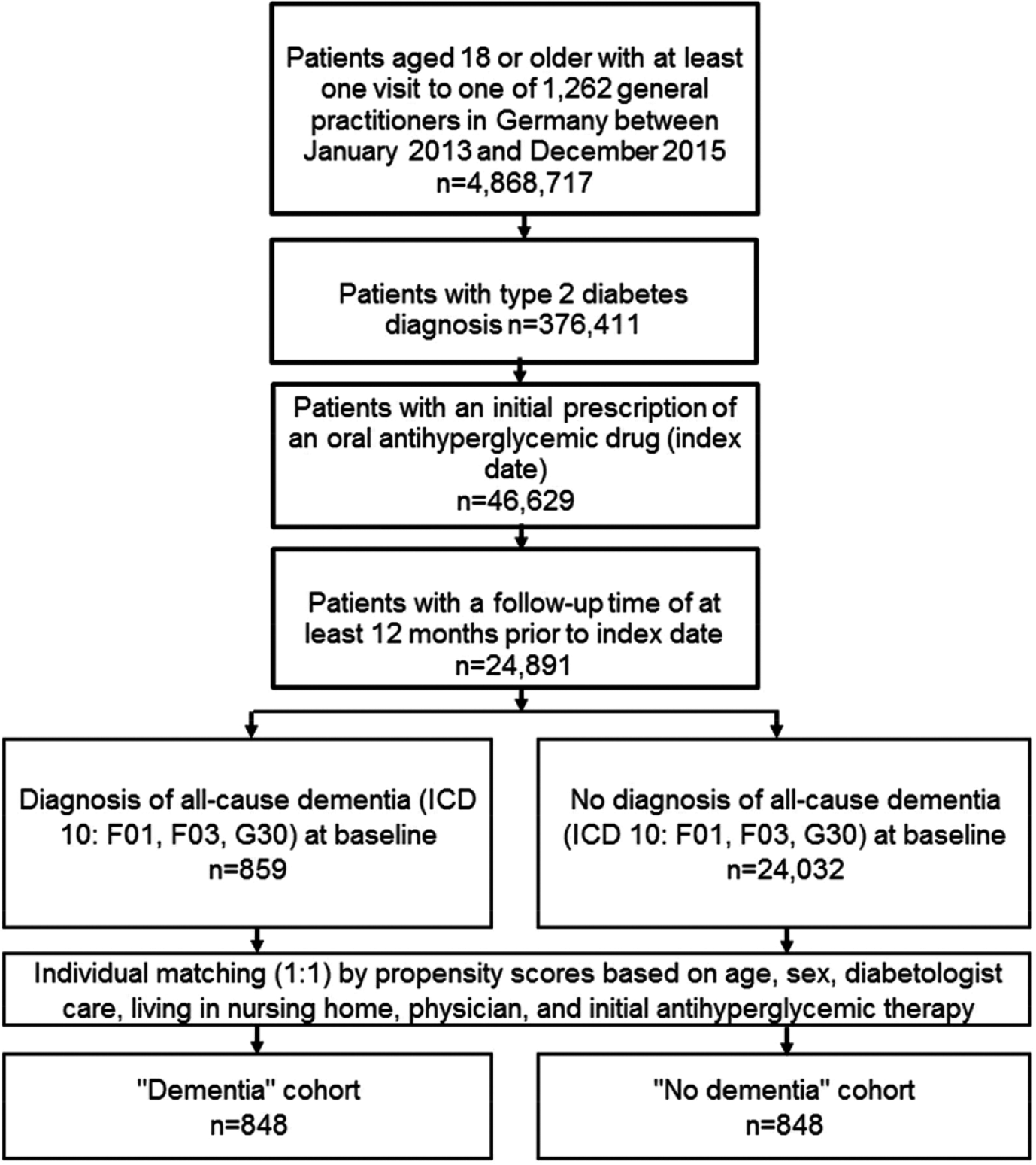
Flow chart of patients included in the study.
Study Outcome
The primary outcome of the study was the rate of persistence with oral antihyperglycemic drugs in dementia patients and controls without dementia in the year following the index date. Persistence was estimated as therapy time without treatment discontinuation, which was defined as at least 90 days without oral antihyperglycemic therapy, defined as at least 90 days between completing their first prescription and receiving the next one. A longitudinal dataset of medication supply was created for each individual patient, and the number of days of drug supply was calculated based on the quantity and dosage information associated with each prescription record. Changes from OAD therapy to insulin or GLP-1 therapy were not considered as OAD therapy discontinuation when the interval between the end of OAD therapy and the next insulin/GLP-1 prescription was less than 90 days. All patients were followed for up to 12 months from their index date.
Independent Variables
Demographic data included age, gender, region (Western versus Eastern Germany), and type of residence. Clinical data included type of care, type of initial oral antihyperglycemic treatment, and six codiagnoses: coronary heart disease (I20, I24, I25), myocardial infarction (I21, I22, I23), stroke including TIA (I63, I64, G45), peripheral artery disease (E11.5, I73.9), hypertension (I10), and hyperlipidemia (E78).
Statistical Analyses
Descriptive statistics were provided, and the differences in patient characteristics (dementia cases versus controls) were assessed using Wilcoxon tests for paired samples or McNemar’s tests. Cox regressions were used to determine the impact of dementia on persistence with oral antihyperglycemic treatment in the entire population and in different subgroups. A P < .05 was considered statistically significant. All calculations were carried out using SAS 9.3 (SAS Institute, Cary, NC, USA).
Results
Patient characteristics are displayed in Table 1. After matching, the study included 848 T2DM patients with dementia and 848 T2DM patients without dementia. In the dementia group, 39.2% of patients were men, while the control group included 40.8% men. The mean age was 77.5 years (SD = 10.0 years) and 76.9 years (SD = 10.6 years), respectively. Hypertension was found to be the most frequent codiagnosis in the two groups (T2DM patients with dementia: 83.4%; T2DM patients without dementia: 84.2%). Figure 2 shows Kaplan-Meier curves for the time to nonpersistence with oral antihyperglycemic drugs in T2DM patients with and without dementia. After 12 months of follow-up, 72.7% of dementia cases and 71.4% of controls without dementia were persistent (P = .291). Of these patients, 5.4% in the dementia cohort and 4.0% in the control group switched to an insulin or GLP-1 therapy within a tolerable time of less than 90 days after ending OAD therapy.
Characteristics of Type 2 Diabetes Mellitus (T2DM) Patients With Dementia and T2DM Controls Without Dementia in General Practices (Disease Analyzer Database, QuintilesIMS).
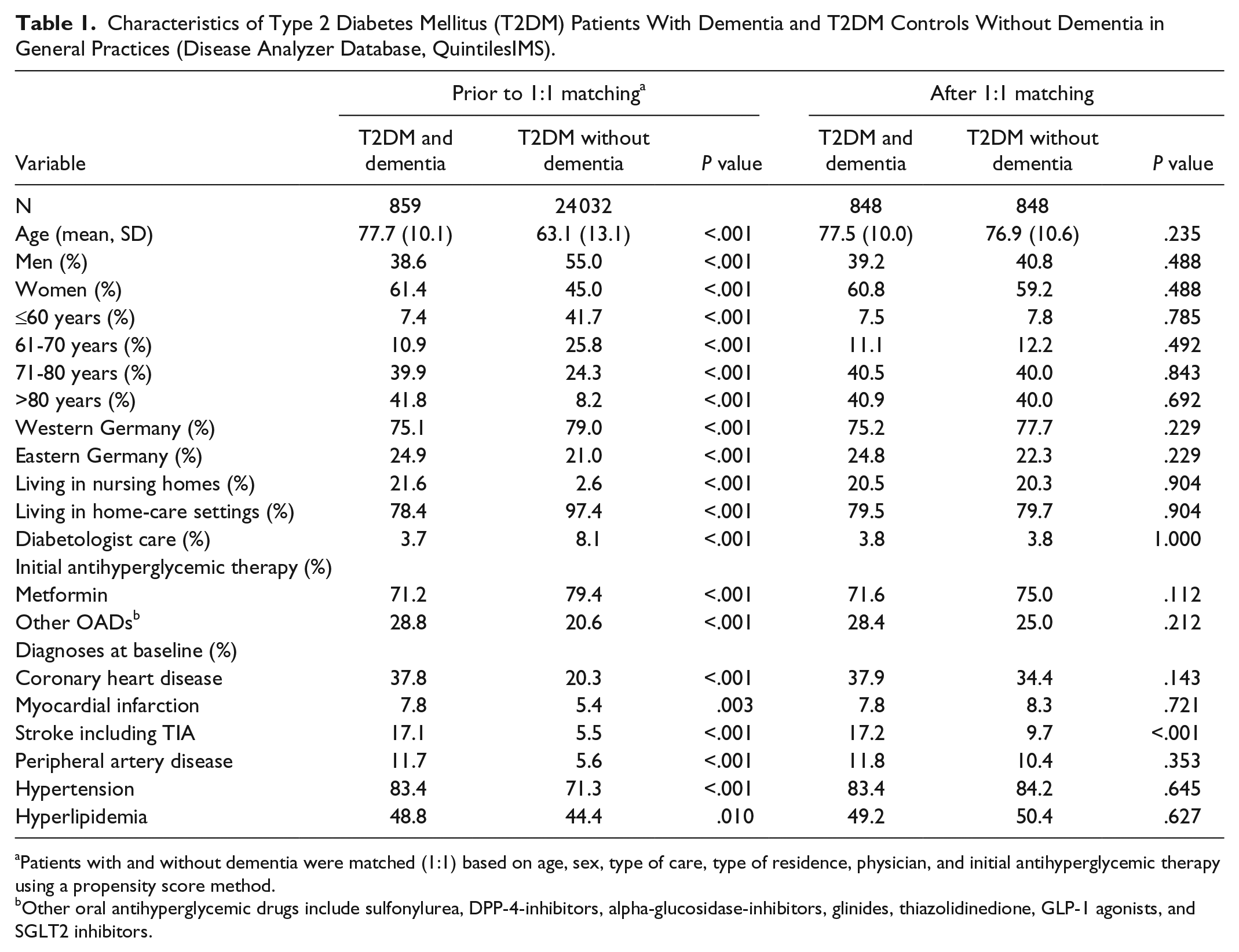
Patients with and without dementia were matched (1:1) based on age, sex, type of care, type of residence, physician, and initial antihyperglycemic therapy using a propensity score method.
Other oral antihyperglycemic drugs include sulfonylurea, DPP-4-inhibitors, alpha-glucosidase-inhibitors, glinides, thiazolidinedione, GLP-1 agonists, and SGLT2 inhibitors.
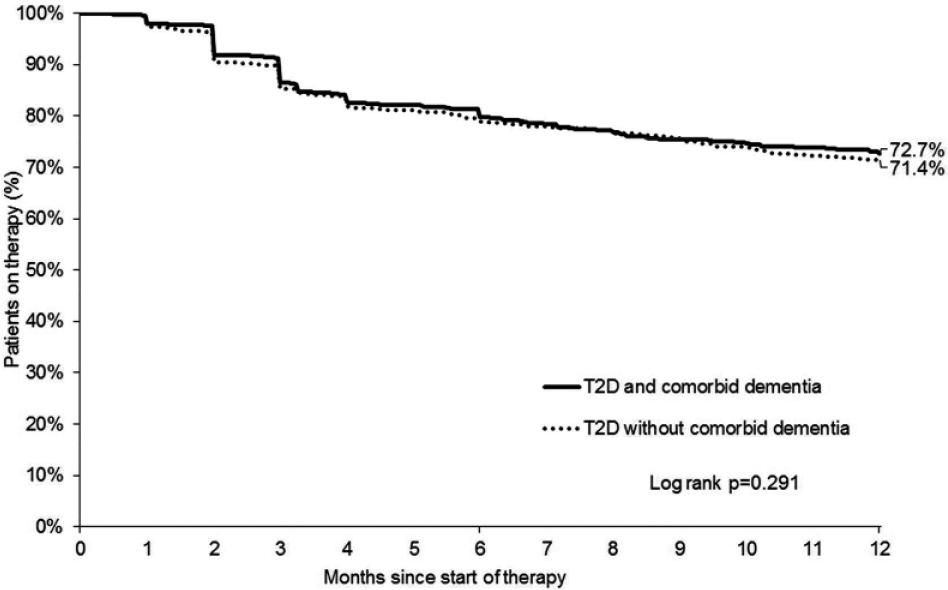
Kaplan-Meier curves for persistence with oral antihyperglycemic treatment in type 2 diabetes mellitus patients with and without dementia in Germany.
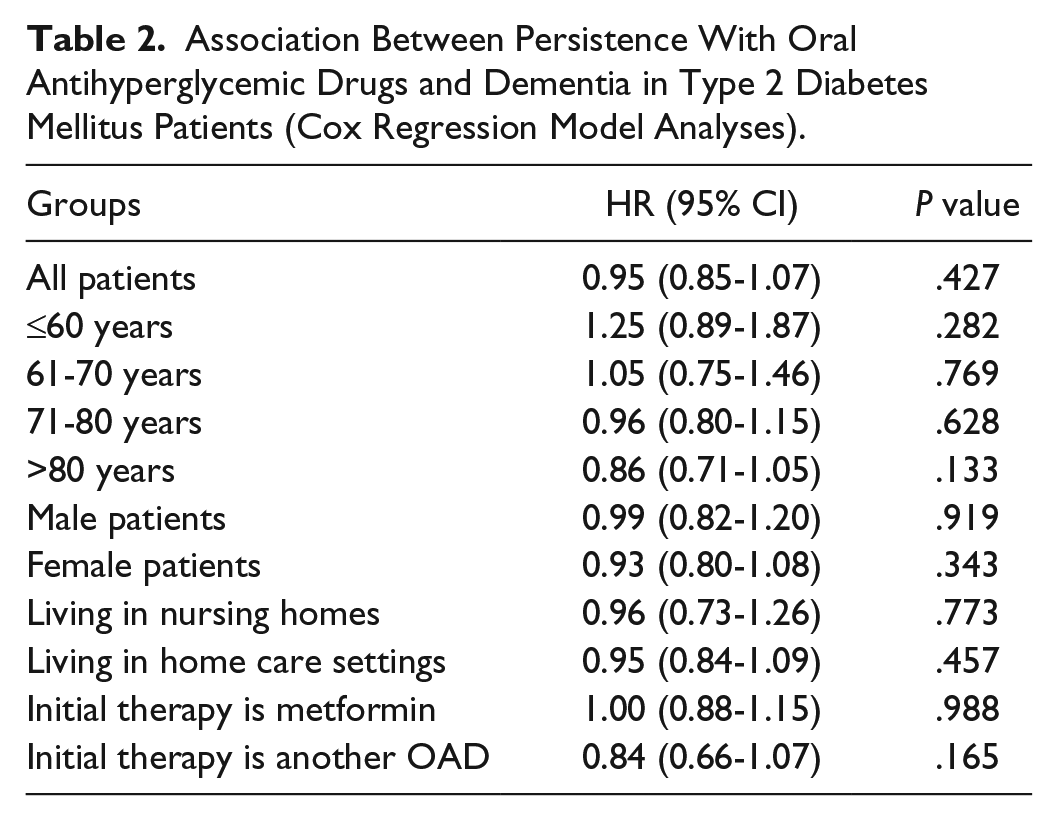
The results of the Cox regression model are displayed in Table 2. No significant association was found between dementia and persistence with oral antihyperglycemic drugs in the entire population or in the different subgroups (HR ranging from 0.84 to 1.25).
Association Between Persistence With Oral Antihyperglycemic Drugs and Dementia in Type 2 Diabetes Mellitus Patients (Cox Regression Model Analyses).
Discussion
The present German study showed that persistence with oral antihyperglycemic drugs was slightly higher than 70% in T2DM patients with or without dementia 12 months after therapy initiation. The subsequent Cox regression analysis further estimated that there was no significant association between dementia and the risk of nonpersistence.
To date, this is the first study to focus on analyzing persistence with oral antidiabetic agents in patients with both T2DM and dementia. Nonetheless, several authors have previously shown that dementia can interfere with treatment persistence. In 2010, Kröger and colleagues discovered in 3369 patients with mild to moderate Alzheimer’s disease that 30.8% and 59.0% of the population discontinued cholinesterase inhibitor therapy 6 months and 3 years after initiation, respectively. 14 Furthermore, based on the results of the Cox regression model, women and individuals with chronic diseases were found to be at a particular risk of early nonpersistence. Later, in 2014, Haider et al estimated that nonpersistence was around 34.0% after 6 months and 58.5% after 12 months of therapy in an Austrian cohort of more than 15 000 individuals affected by dementia. 8 Therefore, these two studies highlight the fact that persistence with antidementia drugs remains low in people with Alzheimer’s disease and other forms of dementia.
Nonetheless, the major finding of the present German study is that dementia did not have a significant impact on persistence with oral antihyperglycemic drugs. This result may be explained by the fact that people with dementia are surrounded by their relatives, potentially leading to proper management of dementia and other comorbid conditions. In a 2004 meta-analysis of 122 studies published between 1948 and 2001, DiMatteo found that family was a determining factor for good adherence to medical treatment. 15 Later, an American study including 164 individuals with diabetes living in inner-city Detroit showed that support from family and friends is positively correlated with better diabetes self-management behavior. 16 In addition to family, medical support is critical for the management and the treatment of diabetes. In 2006, Kim and colleagues investigated the effect of a nurse text messaging service by cellular phone and Internet on glycosylated hemoglobin levels and adherence to diabetes control recommendations. 17 The authors of this Korean study discovered that the use of this nursing strategy was associated with a decrease in HbA1c levels, as well as an increase in antidiabetic drug intake, physical exercise, and foot care adherence. In the case of dementia, as the patient displays mild to severe cognitive impairments, the importance of family, and health professionals is even greater for T2DM management and for optimal control of blood sugar levels.
Retrospective primary care database analyses are generally limited by the validity and completeness of the data on which they are based. The present study was subject to several limitations, which should be mentioned at this point. First, no valid information was provided on diabetes duration. Furthermore, the assessment of complications and comorbidity relied solely on ICD codes entered by primary care physicians. Data on socioeconomic status (eg, education and income) and lifestyle-related risk factors (eg, smoking, alcohol, and physical activity) were also lacking. Unfortunately, the documentation of hypoglycemia was insufficient and could not be used, although hypoglycemia may have an impact on treatment persistence.
Overall, dementia was not significantly associated with persistence with oral antihyperglycemic drugs in Germany. Further studies are needed to gain a better understanding of the role played by friends and relatives in the persistence of the patient.
Footnotes
Acknowledgements
Professional English language editing services were provided by Claudia Jones, MA, Radford, VA, USA.
Abbreviations
ATC, Anatomical Therapeutic Chemical classification system; BMI, body mass index; CHD, coronary heart disease; DPP4i, dipeptidyl peptidase-4 inhibitors; GLP-1, glucagon-like peptid 1; GP, general practitioner; HbA1c, hemoglobin A1c; ICD, International Classification of Diseases; PAD, peripheral arterial disease; SD, standard deviation; SGLT-2, sodium dependent glucose transporter; T2DM, type 2 diabetes mellitus.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: LJ and LAS declare to have no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. Although KK is an employee of QuintilesIMS, he has no conflicts of interest with respect to the research, authorship, and publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.