
Abstract
Bolus advisors that are designed to improve the accuracy of individual bolus doses relative to a meal’s carb content and the current glucose have not substantially changed since they were introduced 15 years ago despite an obvious need for enhancement and innovation. Although some glycemic benefits have been demonstrated, bolus advisors largely ignore the large amounts of clinical data they gather that could have a significant impact on glucose outcomes. Concerns have also been raised regarding the aggressive nature of largely unpublished or poorly explained bolus advisor algorithms. Hypoglycemia and hyperglycemia remain significant risks due to inaccurate bolus advisor settings and the absence of tracking or an inappropriate handling of bolus on board. This review covers common sources for bolus advisor error such as the selection of physiologically inappropriate bolus advisor settings, the use of short duration of insulin action times, poor algorithm logic that tends to cover all carb intake fully, and an excessive reliance on simplistic dosing algorithms. As well as discussing these areas, we provide 21 ways to improve current bolus calculators.
Keywords
A bolus advisor (BA) supports patients with diabetes in the complex processes required to determine optimal insulin doses to cover prandial and corrective bolus insulin requirements. Accuracy of bolus recommendations by the BA relies directly on selection of appropriate personalized settings, accurate glucose monitoring, accurate tracking and accounting of bolus insulin on board (BOB) to minimize insulin stacking, and adequate data collection.1,2 Accuracy also relies indirectly on user and lifestyle factors; however, these aspects are not discussed here other than in reference to potential BA improvements.
It is important for clinicians and users to understand the complexity and limitations of all the devices they use. The manufacturer’s role is to minimize complexity, simplify user interfaces, and remove weaknesses within their devices to ensure a maximum level of safety and effectiveness for the customers who use them. Although widely assumed to be accurate and safe, BAs have been criticized for issues that reduce bolus accuracy and safety.3-5
However, BAs and smart phones also stand at the center of technology-enabled self-management systems that can provide more effective advice for the multiple decisions required each day and for faster clinical interventions than is possible with traditional office visits. Four components help optimize outcomes: (1) patient and device generated health data, (2) analysis, (3) education and adjustment from the analyzed data, and (4) individualized feedback through 2-way communication with the health care team. 6 Integration of BAs into smart phones enables most of these steps, the collection and transfer of the data, analytic capabilities, educational tools, and connectivity to speed up clinical interventions and eventually automate glucose management for patients that require insulin. Efforts are also underway to go beyond math simplification toward suggestions for more phyiologic basal insulin doses and bolus settings that can more directly enhance glucose outcomes.
Providing safe dose recommendations is a primary obligation for any BA. Yet, missteps that increase the risk of hypoglycemic and hyperglycemic events remain relatively common among the users of nearly 100 BAs that are largely untested and frequently unregulated. 7 This leaves health care providers “with the challenge of maneuvering in a field of black boxes that may potentially cause harm to patients.” 3 Most BAs do not reveal the formulas used to determine their bolus recommendations so that clinicians and users remain unaware of how they operate. Like a cart before the horse, some BA algorithms were developed prior to a full understanding of the safety requirements for these devices. We have reached a point where having equivalence with legacy BAs should not be sufficient for regulatory approval.
This review covers common sources for BA errors, especially the use of physiologically inappropriate BA settings and an excessive reliance on poorly understood and poorly explained dosing algorithms. Prevention of hypoglycemia will be a focus because this remains an impediment to improved glucose outcomes with most BAs. An additional section provides multiple areas for BA improvements.
Sources for BA Error
Current BAs suffer from three primary issues: physiologically inappropriate settings, aggressive and nonsequential algorithm logic, and absent or inappropriate BOB tracking or misuse of BOB in calculations. For example, most phone apps do not even track BOB and insulin pump BA algorithms track BOB but most do not subtract BOB from carb boluses or recommend carb intake when it is excessive. Masking residual bolus insulin activity in these ways can generate intermittent “unexplained” hypoglycemia, reduce the clinician’s ability to set physiologically appropriate settings, and hinder the goal of normoglycemia.
Inappropriate BA Settings
Nonphysiological settings for the carb factor (CarbF or I:C ratio) and correction factor (CorrF or ISF) can introduce errors into BA dose recommendations, as well as undermine the benefit of accurate carb counts and accurate glucose monitoring. In one retrospective analysis of the data in 396 insulin pumps, only 38% of these pumps contained CarbF settings that matched their expected distribution shown by the curved R2 line in Figure 1. Of interest, the R2 between actual and expected CarbF distributions did not differ between the low, middle, and high glucose tertiles of 132 pumps each. 8 Also, the CarbF became larger (weaker) in the middle and high glucose tertiles as did the CorrF in the middle tertile. Thus, the relative accuracy of pump settings in this study did not differ for those in better or worse control, but the carb and correction settings became less appropriate as the mean glucose level rose.
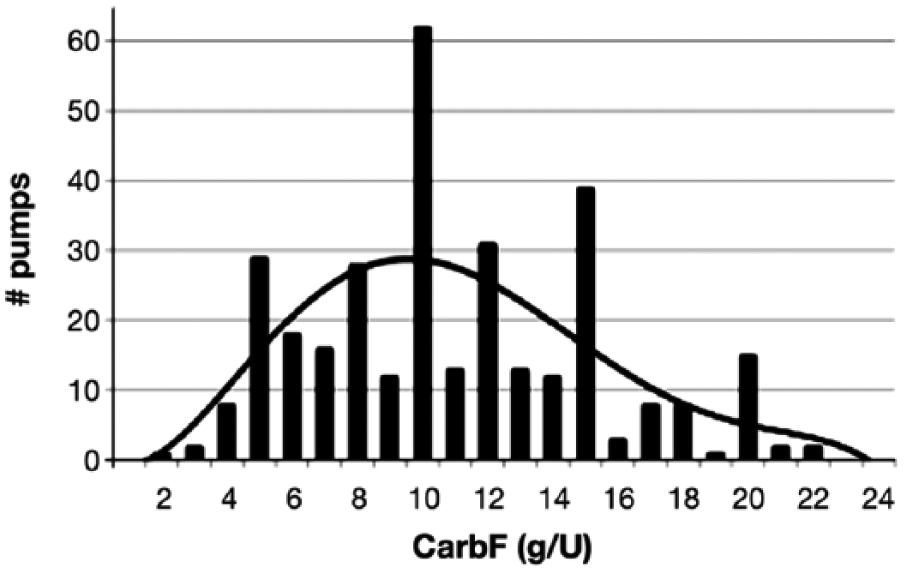
Carb factor settings are often inaccurate. These CarbFs were found in 396 insulin pumps during a routine software upgrade. 9 Only 38% of these CarbFs matched the R2 expected distribution shown by the curved line.
Older CarbF equations such as 300, 450, or 500 divided by the total daily insulin dose (TDD) are often used rather than more exact weight-based equations. Handy CarbF numbers based on multiples of 5 are often selected to ease math calculations, even though the BA performs the calculation and an error of 1 gram in the CarbF can significantly change glucose readings by more than 30 mg/dL after each meal. 5 Initial settings for the CarbF and CorrF are ideally selected from the equations below, and then verified through BGM or CGM testing:


Patient education helps avoid incorrect adjustment of settings in that confusion often causes patients, for instance, to raise CarbFs and CorrFs rather than lower them to treat frequent hyperglycemia. In children prior to puberty, an exact CarbF equation has not been determined, but CarbFs are often slightly higher than in adults. In young children, a CarbF = 3.0 or 3.5 × Wt (lbs)/TDD can be tried. Also, in both children and adults, the CorrF is not determined by a single number such as 1800, but is inversely related to the TDD and also inversely related to any deficit that exists in basal and carb bolus doses, generally measured by the A1c. In other words, 1300/TDD or 1500/TDD may work better for someone with an A1c of 10%, while 2400/TDD may be more appropriate for someone with an A1c of 6.0% where a smaller deficit exists. 11
The appropriateness of basal rates (LAI doses) and CarbFs, the two most critical settings for optimal glucose outcomes, can be quickly optimized from existing retrospective insulin and glucose data within an individual’s BA database. Optimizing glucose levels requires knowing an individual’s A1c or mean glucose level, their significant glucose patterns, TDD, and basal (LAI)/bolus ratio. Once an individual’s total daily dose of insulin (TDD) is reasonably optimized, setting errors become easier to identify in that they tend to generate specific patterns of hyperglycemia and hypoglycemia. 11 Algorithm logic errors, on the other hand, are less obvious in that they generate intermittent hypoglycemia. Other than the A1c, all of these are readily available within the central repository of information, the BA’s dataset.
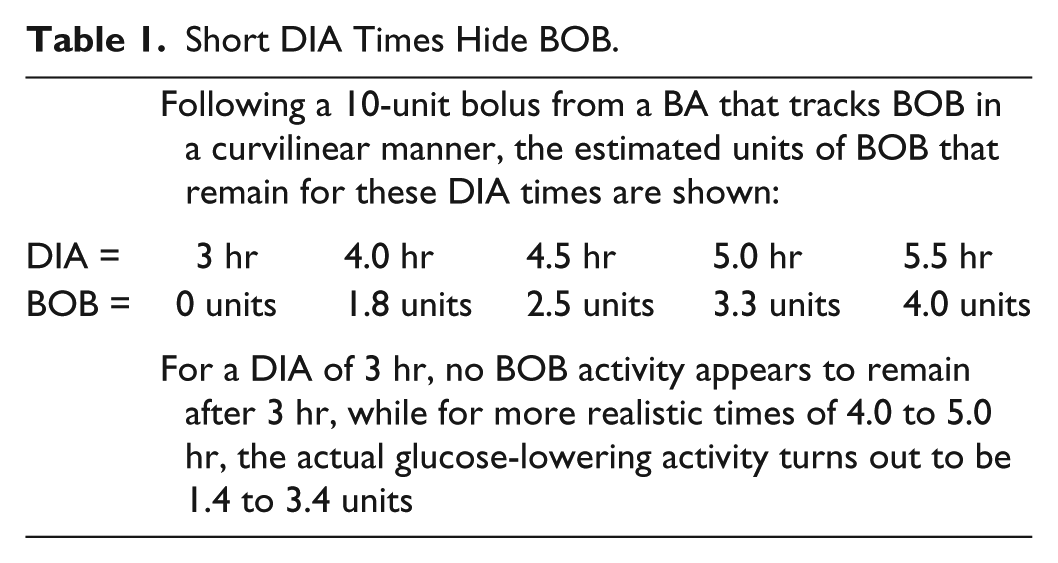
All BA settings must be appropriate but one inaccuracy in particular that often leads to unexplained hypoglycemia arises from the selection of short DIA times. An accurate DIA time setting allows accurate estimates of residual BOB, while an inappropriately short DIA time makes the glucose-lowering activity of a recent bolus appear to be gone as calculated by the BA when bolus insulin is still actively lowering the glucose in the body. Unfortunately, BA users and particularly parents of children with type 1 diabetes realize that shortening the DIA time is a quick way to increase the size of recommended bolus doses. Clinicians themselves may be tempted to shorten DIA times when users complain that an otherwise appropriate DIA time setting prevents them from getting sufficient bolus doses. Unfortunately, the inappropriate selection of the most commonly used DIA time setting of 3 hr masks active BOB and leads to insulin stacking as shown in Table 1.
Short DIA Times Hide BOB.
Exposure to insulin stacking is common. In one study that exemplifies typical usage, pump wearers delivered an average of 5 to 6 carb or correction boluses a day with 64.8% of 201,538 bolus doses delivered within 4.5 hr of each other. 12 A short DIA time introduces a high risk for hypoglycemic events due to the frequency at which insulin stacking may be hidden. A DIA setting of 4 to 5 hr is more physiologically appropriate based on research studies.13,14 Rather than introducing these intermittent episodes of hidden insulin stacking by shortening the DIA, a more appropriate response to hyperglycemia would be to address the actual insulin deficit by increasing basal rates, lowering the CarbF or CorrF, or through improved carb counts or diet choices. This improves the accuracy and safety of bolus doses and eliminates the need to lower the DIA time to “fix” control problems. 13
For some, shorter DIA times may be appropriate when they retain significant residual insulin production that is able to independently lower elevated glucose levels. It can also be required when basal rates or long-acting insulin doses are set artificially low. In the latter case, a more appropriate response would be to correct the deficient basal delivery or LAI dose and select a longer and more physiologic DIA time.
In “artificial pancreas” (AP) pumps that operate largely from an individual’s BA settings, clinicians occasionally advocate the use of short DIA times, such as 2 or 3 hr, along with more aggressive (lower) CarbFs and CorrFs. This assumes that the larger bolus doses generated in this way can be handled by means of basal suspensions. However, this presents a risk when the AP algorithm is offline and the pump is in standalone mode and can no longer offset these larger bolus doses by means of basal suspension. This can introduce serious risk during the frequent interruptions that occur in some individuals who use an AP. We recommend against the use of aggressive BA settings until an AP system can demonstrate it can maintain continuous performance. A safer alternative would be to provide two sets of BA settings that allow a more aggressive one when the AP is operational and a more physiologic one when it is not.
Aggressive and Nonsequential BA Algorithms
The formula used in the first insulin pump BA to simplify math and improve the accuracy of bolus doses provided a simple and relatively safe model for calculation of bolus doses. As shown in equation 3 below, the insulin required to cover the carbohydrates in a meal is added to that required to adjust for the current glucose difference from the target glucose (a positive or negative value) and any residual bolus insulin activity from recent boluses is then subtracted. This equation can be used to determine whether additional insulin is required or whether carb intake may be needed to prevent hypoglycemia. 15

Equation 3 takes into account residual bolus insulin activity to minimize insulin stacking. Clinicians and pump wearers often assume this is the equation used in their BA, but this is not true. For example, the only insulin pumps that follow this equation or a reasonable modification of it are no longer available (Deltec Cozmo and Asante Snap) or are not widely used in the U.S. and Europe (Sooil Dana Diabecare). These modifications address one problem with equation 3 in that strict use would not fully cover an unplanned dessert or second helping consumed shortly after a meal due to apparent excess in the BOB at that time. A few phone and meter BA apps, such as MySugr Pro and Freestyle Insulinx (both only available in the EU), give full bolus coverage for desserts or extra portions that follow a meal bolus. Others are developing more advanced versions that use equations 4a and 4b below to recommend specific carb intake to treat or prevent hypoglycemia when excess BOB is present. Most phone apps, unfortunately, do not yet track BOB and are unable to protect against insulin stacking.
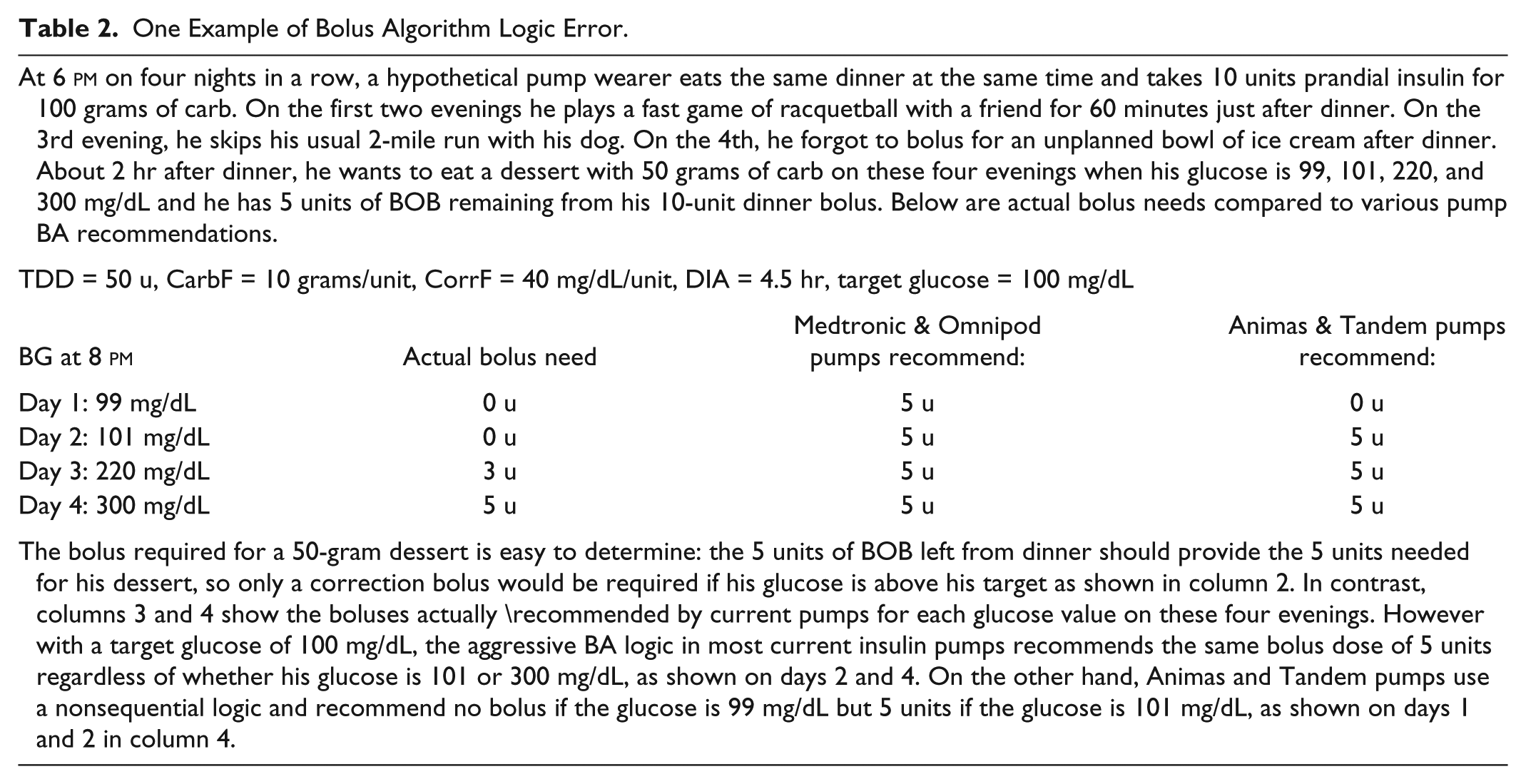
BAs that use aggressive or nonsequential logic can generate serious errors in bolus dose recommendations. For example, in a 2014 review of BA risk management, Rees warned “no advanced BA subtracts excess BOB from a meal bolus when the current BG is above the BG target, that is, they do not follow the logic of equation 3 (similar to equation 3 above) and thereby the patients run the risk of insulin overdosing.” 16 Aggressive and nonsequential BA logic can lead to illogical insulin doses at shown in Table 2.
One Example of Bolus Algorithm Logic Error.
Even when a BA tracks BOB, it is difficult for a user to account for this information if the current BOB is not displayed in context alongside the recommended carb or correction bolus on the screen where the patient makes their final dosing decision. Even when it is displayed, it is unclear to most users how a particular BA takes BOB into account. In other words, if the screen shows 3.0 U of BOB when the glucose is relatively normal, will the BA appropriately subtract 3 U from a carb bolus recommendation (or suggest a specific intake of free carbs), or will the pump wearer be required to subtract this residual insulin himself?
BOB can become excessive and introduce insulin stacking in many situations, such as when increased physical activity lowers the glucose independently of a previous bolus, or when an erroneously high glucose reading is generated by a BGM or CGM, by intake of acetaminophen while on a CGM, or from a finger contaminant. Fredrik Debong, Head of R&D at mySugr, also points out that BOB from correction boluses differs from that from carb boluses and should be tracked separately, such that anytime the BOB from recent correction boluses is in excess relative to the current glucose, it must be subtracted from a planned carb bolus or activate a recommendation for an appropriate intake of free carbs.
BA algorithms that ignore insulin stacking can be frequent sources for unexplained hypoglycemia, as seen in the Sample Case below.
Sample Case: Patient With Frequent Hypoglycemia on Correct Pump Settings
Excessive bolus recommendations can occur when a BA algorithm incorrectly accounts for BOB. In the example below, a pump wearer in her 30s came into a clinic to have her pump settings adjusted because she was experiencing frequent hypoglycemia when she delivered the bolus doses suggested by her pump. However, she was unaware that her pump would recommend full insulin coverage of carb intake and ignore any residual BOB when her glucose was above her target glucose. A sample from her pump download is shown here:
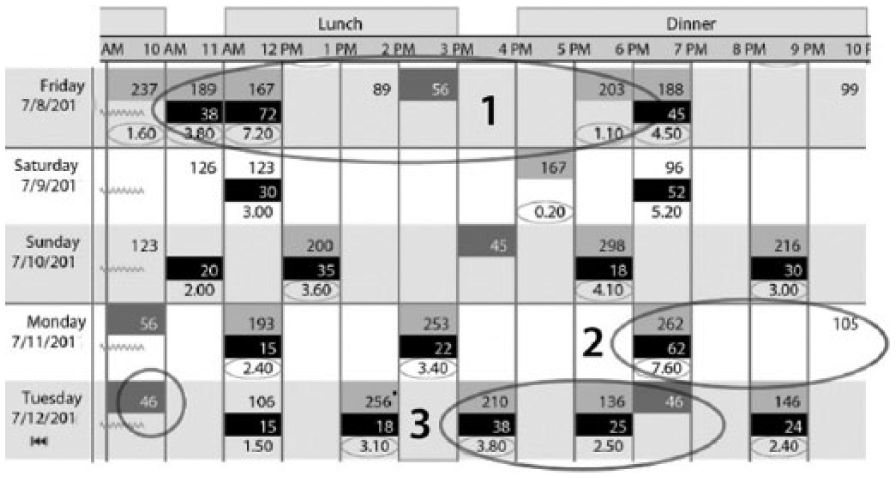
Example 1 shows that her BG had fallen from its peak of 237 mg/dL to 167 mg/dL from 2 boluses (1.6 U and 3.8 U) given in the previous 2 hr. Even so, the pump recommended full coverage (7.2 U) for 72 grams of carb when at least 4 units of BOB remained. Even more alarming, when her glucose reached 89 mg/dL 2 hr later with approximately 4 units of BOB remaining, the pump did not warn her how many carbs she would need to offset this insulin. Consequently, her glucose fell to 56 mg/dL 1 hr later and was followed by a reading of 203 mg/dL 3 hr later from overtreatment of the low glucose because the pump did not recommend how many grams of carb she needed to treat her hypoglycemia.
In example 2, the pump failed to warn her that about 2 units of BOB remained when her bedtime glucose was 105 mg/dL, nor was she informed how many carbs would be needed to compensate for this excess BOB to prevent a low glucose. After likely being hypoglycemic through much of the night, the patient awoke the next morning at 46 mg/dL. (Due to the frequency of her hypoglycemia from these algorithm defects, her stores of adrenal hormones appeared to have been depleted and were insufficient to awaken her earlier in the night.)
In example 3, another bolus overdose occurred when 2.5 units was recommended for 25 grams of carb at a time when the patient’s BG was 136 mg/dL while about 2 U of excess BOB remained from the 3.8 U bolus given 2 hr earlier. The pump did not warn about the excess BOB nor recommend a reduction in the 2.5 units for the carbs that were consumed. As a result of taking the recommended dose, her glucose fell to 46 mg/dL 1 hr later. There are two additional instances of hypoglycemia in her record; one secondary to increased activity (biking) and the second is another example of the aggressive BA algorithm found in most insulin pumps.
In these examples, BOB from recent boluses was not fully accounted for and carb intake was not recommended when BOB became excessive. Once this patient received instruction in how to calculate her bolus doses appropriately using bolus dose equation 3 rather than the pump’s recommended doses, and had a small increase in her CorrF, her frequent hypoglycemia disappeared. Unfortunately, many pump wearers do not have sufficient math skills and the consistent discipline required to override this BA algorithm defect and calculate their own dose. (A short DIA time, discussed earlier, can cause identical problems as these, but this patient’s DIA was set at 5 hr and did not play a role in these excessive bolus recommendations.)
Poor logic in insulin pump BA algorithms creates unnecessary risk for pump wearers and places an additional burden on clinicians to train their patients regarding when and how to safely override erroneous bolus recommendations. Most pump wearers and clinicians often lack the knowledge or time to address this safety issue.
Adaptations for Desserts, Altered Digestion, and Limitations on Carb Intake
As noted above, a period of uncertainty exists for about 90 min following a meal bolus while the impact of the rising glucose from carb digestion remains difficult to balance against the slower glucose-lowering action of the meal bolus. Whether to give a full or partial bolus for an unplanned dessert, a second serving or a later snack depends on its timing, and the current BOB and glucose. Bolus recommendations also need to be modified for low glycemic index foods, meals with a higher fat and protein content, gastroparesis, and concomitant use of an amylin analog or GLP1 agonist. In these situations, BOB may incorrectly appear to be excessive when a minimal elevation is observed in the glucose levels following a meal bolus.
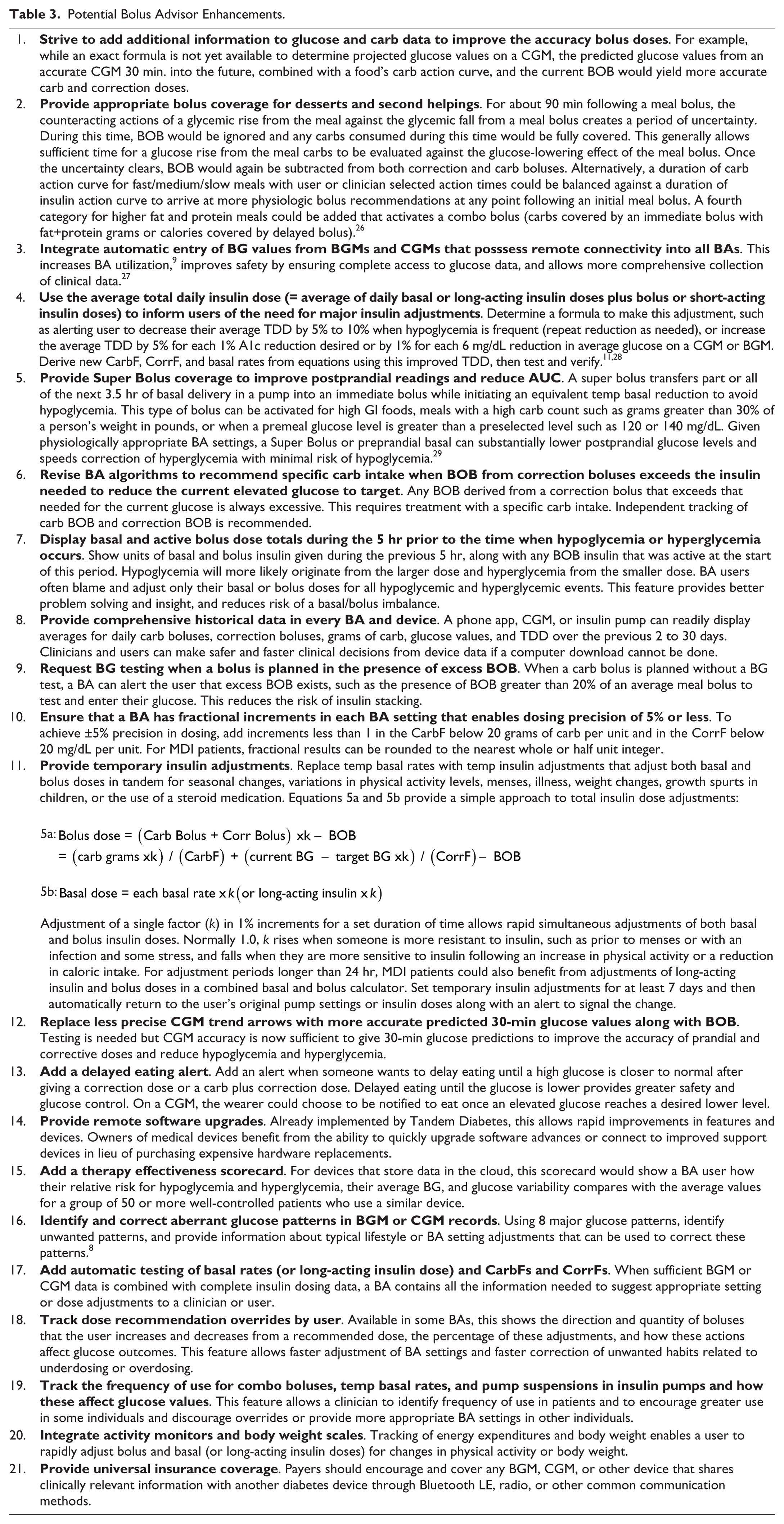
With diabetes and the absence of the pancreas’ remarkable ability to directly deliver insulin to the liver for rapid onset of gluconeogenesis and removal of glucose from the blood, a person becomes far more limited in the maximum number of grams of carb they can consume while still maintaining excellent postprandial control. This maximum is generally equivalent to about 30% of their body weight in lbs. Table 3 reviews many options to improve BAs, including the Super Bolus where basal insulin is delivered preprandially to improve control with larger carb intakes or more quickly reduce hyperglycemia.
Potential Bolus Advisor Enhancements.
A somewhat ignored aspect regarding glucose control is the timing of the insulin bolus with respect to the meal and the duration over which it is delivered. It is well known that the increase in insulin levels circulating in the blood stream after applying the insulin bolus should fit to the increasing demand when carbohydrates started to be are absorbed after a meal. Such a matching of pharmacodynamic properties of the applied insulin with the physiological needs requires that a bolus of insulin be delivered at an appropriate point in time. With current prandial insulins, delivery of an injection or bolus 15 to 30 min before meals when the glucose is relatively normal is generally recommended. Another aspect that may impact postprandial glucose levels is the duration of insulin delivery for meals. For example, an injection of 25 units of insulin could be completed in only a few seconds while some insulin pumps might require a few minutes to deliver the same volume of insulin. Unfortunately, no systematic evaluation has been conducted about the timing of a bolus and postprandial glycemic excursions, so current BCs do not take such factors into account.
Hypoglycemia Prevention and Treatment is Needed
When someone tests their glucose, there is frequently a need for either insulin or carb intake. The BA is in a perfect position to tell them which, yet most BAs provide either no protection or only rudimentary protection against hypoglycemia even when any excess BOB that exists can be clearly identified and a directional trend line from a CGM is also often available. Thus, most BA users are boxing with one hand in the diabetes ring. Any device giving bolus recommendations should also advise the user when free carbs are required to offset excess BOB created either directly by or independently of the BA. Even though all BAs recommend insulin doses, only a handful of the 80+ BAs in meters and phone apps and none in current insulin pumps provide the safety measure of recommending a specific carb intake to compensate for excess BOB.
A glucose reading from a BG meter or a CGM system, potentially enhanced by a CGM’s trend line or projected glucose, can be compared with the glucose-lowering activity of any residual BOB to determine a recommended intake of grams of carb to prevent hypoglycemia, as well as the units of insulin needed when an insulin deficit exists. Equation 4a provides guidance on how to prevent and 4b shows how to treat hypoglycemia with an appropriate quantity of carbs while minimizing overtreatment and its subsequent hyperglycemia.


Absent or Incomplete Glucose Data
Ease of data entry combined with a comprehensive gathering of all clinically relevant information is essential for improved diabetes care. Clinical errors can arise when data is unavailable, becomes biased through incomplete collection, such as when only one of multiple meters in use is downloaded or brought to a clinic visit, or an individual has a habit of testing glucose levels only when they are hyperglycemic or hypoglycemic. Inconsistent entry of glucose data is compounded when a preferred device from one manufacturer does not communicate with another manufacturer’s device, or when a payer does not cover a BGM or CGM that communicates directly with an insulin pump or BA. Manual entry of glucose values introduces major losses in data, distorts an individual’s glucose patterns, and will artificially raise or lower their average glucose. For example, many BA users remain unaware that manual entry of relatively normal glucose readings is required to account for BOB, prevent insulin stacking, and improve bolus safety. Because missing glucose or insulin data compromises clinical decisions, automated collection of all glucose data is required to ensure safety through appropriate bolus doses.
Bolus and Insulin Dose Advisor Improvements and Enhancements
Due to its ability to gather data, the BA is in a unique position to make significant changes in diabetes care. A BA collects nearly all of the critical data needed for a comprehensive analysis of the significant factors that impact glucose outcomes. In insulin pumps, basal insulin data is collected simultaneously with bolus information. Likewise, Bluetooth-enabled insulin pens like Companion Medical’s InPen and Novo Nordisk’s Echo allow collection of all short-acting insulin doses and their timing for people using MDI. When data is automatically collected in phone or meter BA apps, along with manual or Bluetooth entry of long-acting insulin doses, current bolus dose advisors can be transformed into basal and bolus insulin dose advisors (IDA) and allow MDI users and their clinicians to have the same access to clinical data as is currently available for CSII patients.
More than 30 years ago, software programs were introduced to improve glucose outcomes using the information available in BAs. However, they were abandoned due to regulatory concerns.17,18 Steps to integrate problem-solving strategies into BAs are underway and should be strongly encouraged to guide and verify changes in BA settings that provide more accurate bolus and basal dose recommendations.19-23 Telemedicine, as well as new insulin dosing algorithms based on artificial intelligence 24 will at first mitigate errors in BA logic and settings and improve clinician oversight, and eventually reduce data overload and improve glucose outcomes through automation. 25 Although insulin dose titration apps are being designed initially to improve basal insulin doses for people with type 2 diabetes, such as Lilly’s Go Dose and Sanofi’s Voluntis Insulia and My Dose Coach, these are also likely to hasten the development of IDAs for improvement of both basal and LAI insulin doses. Integration of self-correction algorithms for BA settings in partnerships like that of Glooko with Novo Nordisk and IBM Watson will benefit those who use MDI and insulin pumps.
Analysis of existing issues in BAs provides the groundwork for adding features to make BAs safer and more effective for MDI and pump patients. Table 3 displays a variety of potential BA enhancements designed to increase safety and effectiveness of BAs and IDAs. Some enhancements already exist but are not widely utilized or have not been carried as far as they could to provide the best advantage.
Summary
Today’s BAs stand in need of enhancements and innovation. Current BAs focused on the accuracy of individual bolus doses relative to a meal’s carbohydrate content and the current glucose have demonstrated they can improve dose accuracy. Yet safety concerns remain regarding the aggressive nature of largely unpublished or poorly explained BA algorithms. In addition, hypoglycemia and hyperglycemia remain significant risks due to inaccurate BA settings and the absence of tracking or inappropriate handling of BOB. The potential value within the massive quantities of clinical data being collected by BAs remains largely untapped for improvements in glucose outcomes. BAs would benefit from improved and transparent dose algorithms, guided selection of personalized settings, enhancements that add functionality, and a systematic approach that increases safety. We look forward to progress in these areas.
Footnotes
Abbreviations
BA, bolus advisor; BG, blood glucose; BGM, blood glucose meter; BOB, bolus insulin on board or active bolus insulin; CGM, continuous glucose monitors; DIA, duration of insulin action; IDA, insulin dose advisor.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: JW is a consultant for a number of companies developing insulin pumps, bolus advisors, and infusion sets. He is employed by Advanced Metabolic Care and Research, which conducts numerous studies in diabetes devices, AP systems, medications, infusion sets, and insulins. RR has no conflicts to declare. TSB has research support from Abbott, Ambra, Ascensia, BD, Boehringer Ingelheim, Calibra, Companion Medical, Dexcom, Elcelyx, Glysens, Janssen, Lexicon, Lilly, Medtronic, Novo Nordisk, Sanofi, Senseonics, Versartis, Xeris; consulting honoraria from Astra Zeneca, Ascensia, BD, Calibra, Lilly, Medtronic, Novo Nordisk, Sanofi; and speaking honoraria from Abbott, Insulet, Medtronic, Lilly, Novo Nordisk, and Sanofi. LH holds shares in the Profil Institute for Metabolic Research, Neuss, Germany, and ProSciento, San Diego, USA. LH is consultant for a range of companies that develop new diagnostic and therapeutic options for the treatment of diabetes.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.