
Abstract
Background:
Real-time continuous glucose monitoring (rtCGM) improves glycemic control in type 1 diabetes (T1D) patients treated with continuous subcutaneous insulin infusion (CSII). However, the benefits of rtCGM in T1D patients treated with multiple daily insulin injection (MDI) therapy has not been well studied. We explored the effects of rtCGM versus self-monitoring of blood glucose (SMBG) on clinical outcomes within a large T1D population treated with either CSII or MDI therapy.
Methods:
This retrospective, longitudinal analysis utilized datasets from T1D patients enrolled in a commercial health plan to assess changes in HbA1c in 187 naïve to rtCGM users and 6260 SMBG users. Propensity score modeling was used to assess inpatient admissions, emergency room (ER) visits in 1130 patients (565 rtCGM, 565 SMBG). Differences in HbA1c reduction (rtCGM+MDI vs rtCGM+CSII) were evaluated.
Results:
Larger, clinically meaningful HbA1c reductions were seen among rtCGM versus SMBG users: –0.5% (P = .004) versus −0.2% (P < .0001); 0.3% diff in diff, P = .03. All-cause inpatient admissions were lower for rtCGM users: –42%, P = .013. Emergency room visits coded for diabetic ketoacidosis (DKA) were four times higher for SMBG patients than rtCGM patients: 17 versus 4, P = .0318. HbA1c reductions were most notable with rtCGM+MDI versus rtCGM+CSII treatment: –0.6% (P = .01) versus −0.3% (P = .16).
Conclusions:
Use of rtCGM in T1D patients facilitates greater HbA1c improvements and reduced health care system utilization compared with traditional SMBG use regardless of insulin administration method. Treatment with rtCGM in conjunction with MDI confers similar or greater glycemic benefits without the additional costs associated with CSII therapy.
With recent advances in accuracy, reliability and usability, real-time continuous glucose monitoring (rtCGM) is now recognized as a critical component of diabetes self-management among many individuals with insulin-treated diabetes. 1 Unlike traditional blood glucose monitoring systems, which display only “point-in-time” glucose values, rtCGM devices provide numerical and graphical information about the current glucose level, glucose trends and the direction/velocity of changing glucose. Devices with programmable alerts/alarms that warn users of current and/or impending high or low glucose offer additional safety advantages.2-5
Numerous studies have shown that use of rtCGM improves glycemic control in children and adults with type 1 (T1D).3,6-15 Importantly, the benefits of rtCGM are seen primarily in individuals who wear their devices frequently and act appropriately on the glucose data provided.3,6,16-18 Most of the evidence supporting rtCGM use comes from studies conducted primarily in patients using continuous subcutaneous insulin infusion (CSII);7,14,18-21 however, results from a recent study of 20 adult T1D patients suggest that rtCGM may confer the same glycemic benefits to patients treated with multiple daily insulin injection (MDI) therapy. 22
The large financial burden of diabetes is growing and unsustainable, and clinicians are challenged to select treatment regimens that are both efficacious and cost-effective. Although new evidence suggests that rtCGM use in combination with CSII is more cost effective than CSII, alone,23,24 the cost-effectiveness of rtCGM use with MDI therapy is largely unknown. However, given its enhanced decision support and the resulting improvements in glycemic control, rtCGM may be even more cost-effective than CSII because it eliminates the initial and ongoing costs of insulin pump use.
To explore this hypothesis, we analyzed the effects of rtCGM compared with self-monitoring of blood glucose (SMBG) use on clinical outcomes and utilization of health care services within a large population of T1D patients treated with either CSII or MDI therapy.
Methods
Design
This retrospective database analysis assessed the impact of rtCGM (G4 Platinum, Dexcom, Inc, San Diego, CA, USA) compared with traditional self-monitoring of blood glucose (SMBG) in a large cohort of T1D patients. The primary outcome measure was change in HbA1c between and within study groups, according to insulin delivery method (CSII vs MDI). Secondary outcomes included within- and between-group differences in hospitalizations and emergency room (ER) visits.
Data for the study were obtained from the Optum Research Database (Optum, Eden Prairie, MN, USA), which contains eligibility, pharmacy claims, medical claims and laboratory data for more than 14 million enrollees in fully insured and self-funded health care plans. Medical and demographic information, including diagnosis, utilization of health care services (eg, inpatient admissions, emergency room visits, pharmacy costs), age, gender and geographic regions were obtained from health plans’ administrative records for this study.
The identification period for eligible patients was from November 2012 through December 2013. The index date for each patient was the date of the first claim for initiation of either rtCGM or SMBG at a frequency of ≥4 test strips per day. The baseline period for each group was one year prior the index date; whereas, the measurement period was a year following the index date, including the index date itself.
Analysis
The study population included patients with a diagnosis code for T1D, continuous enrollment in the health plan and at least one claim for insulin during the study period. Patients who were pregnant or had prior experience with rtCGM were excluded from all analyses.
The primary analysis included patients who had at least one HbA1c value documented in both the baseline and the measurement periods. Study patients were divided into two groups: patients who initiated rtCGM use (rtCGM group) with the Dexcom G4 Platinum system (Dexcom, Inc, San Diego, CA, USA) and patients documented use of self-monitoring of blood glucose (SMBG group) at a frequency of ≥4 test strips per day within the baseline period as indicated by medical claims. Daily test strip use was calculated as the quantity of test strips dispensed divided by the days until the next prescription fill date. To control for the baseline difference of the two groups, the analysis was also stratified by baseline HbA1c value; thus, baseline matching or continuous enrollment was not required. Changes in HbA1c levels between the rtCGM and SMBG groups, overall and by insulin delivery method (CSII vs MDI), were compared; t-tests were performed to determine the statistical significance of between-group differences.
For the secondary analysis, propensity score matched analysis was performed to reduce selection bias due to imbalances in study covariates. The two groups were extensively matched on baseline per-member per-month (PMPM) medical and pharmacy costs, gender, region, Charlson Index Score and sixteen comorbidity Charlson indices. 25 Patients in the rtCGM group were matched to those in the SMBG group in a 1:1 ratio, based on the resultant propensity score probabilities. However, patients were not matched for HbA1c due to the relatively smaller number rtCGM patients with baseline and measurement period values (Table 1). The number of coded incidents of diabetic ketoacidosis (DKA) and hypoglycemia were calculated.
Demographic Characteristics.
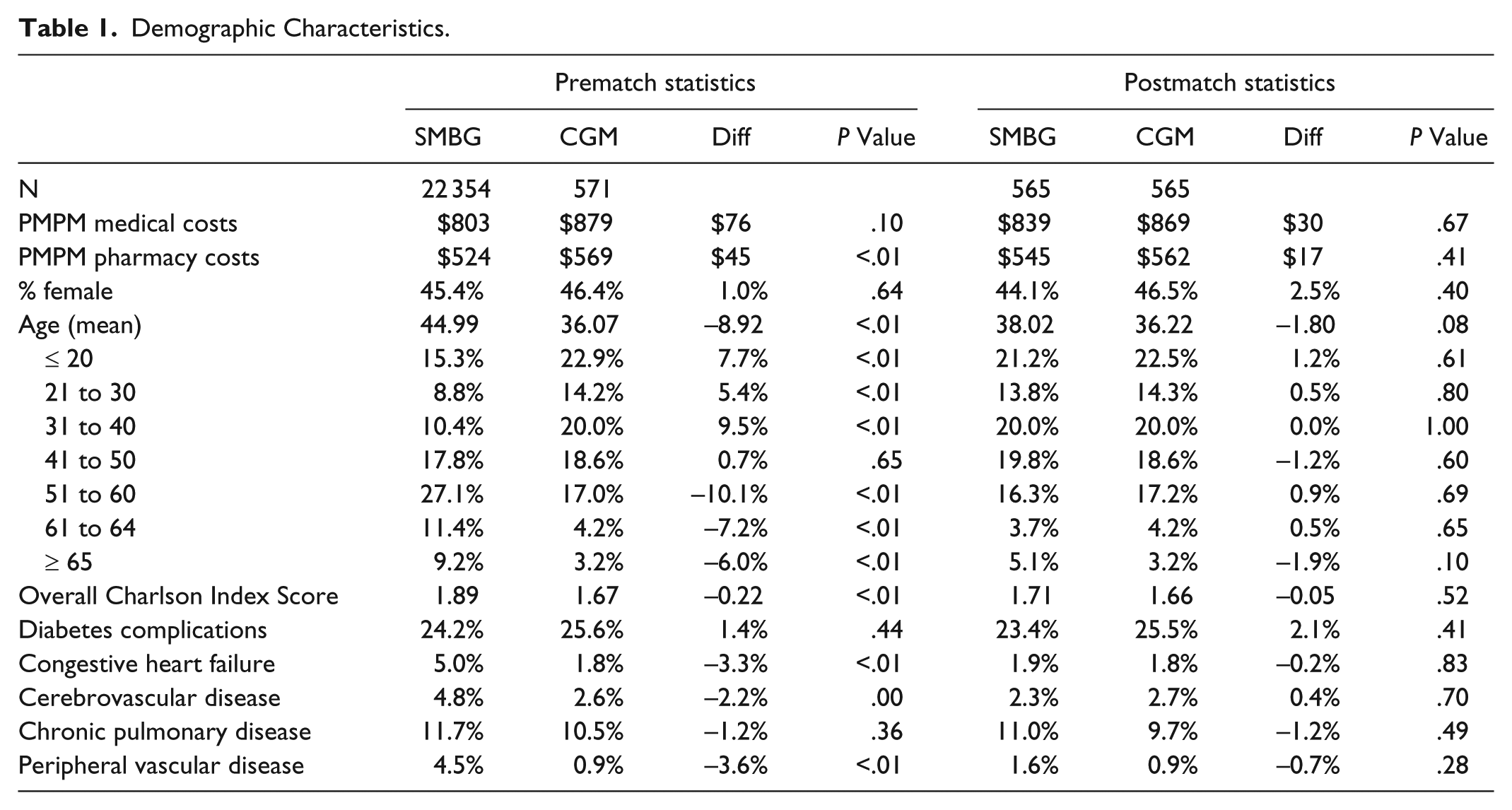
Summary statistics for continuous variables are summarized using mean and SD values. Analyses were conducted using SAS version 9.2 (SAS Institute Inc, Cary, NC, USA).
Results
Primary Analysis
A total of 6467 patients (187 rtCGM; 6280 SMBG) were included in the primary analysis. The distribution of baseline values in the two groups was similar (Figure 1).
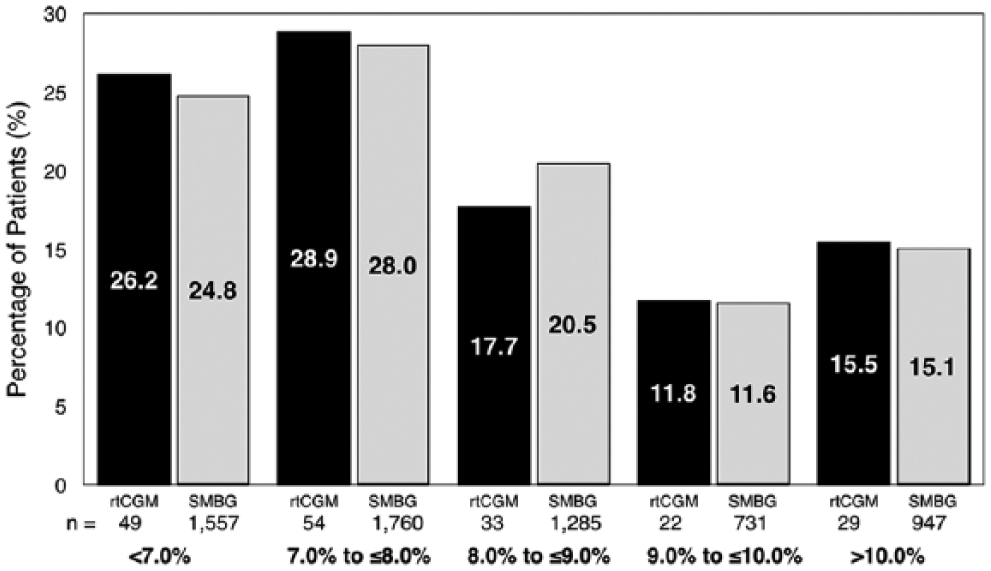
Percentage distribution of baseline HbA1c values.
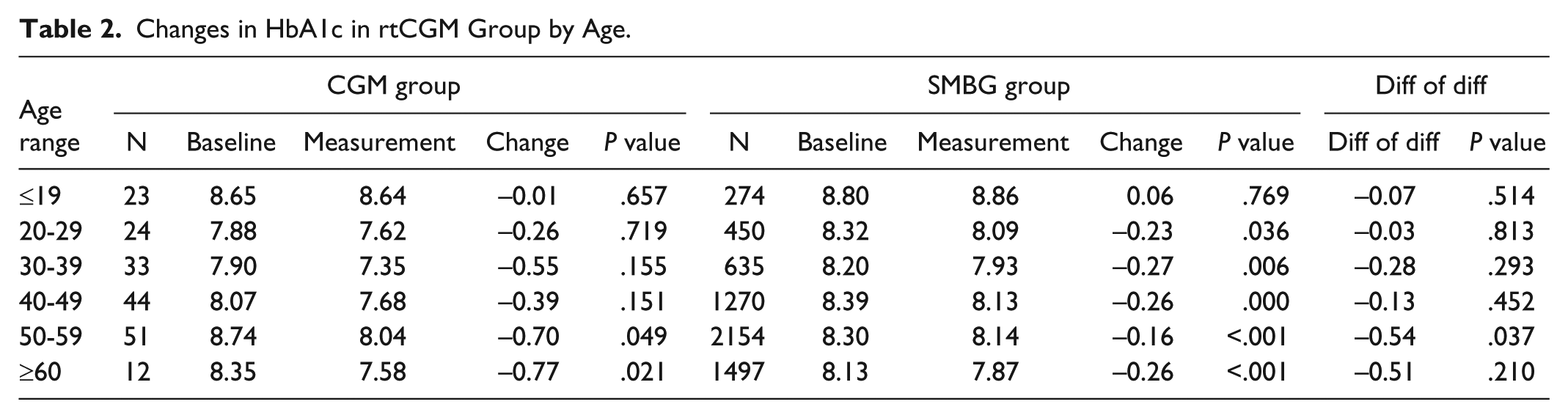
The HbA1c reductions seen in the rtCGM group were significantly greater (P = .0305) and more clinically meaningful compared than the reductions seen in the SMBG group (Figure 2A). The largest HbA1c reduction was seen in older rtCGM users, age ≥50 years (Table 2).
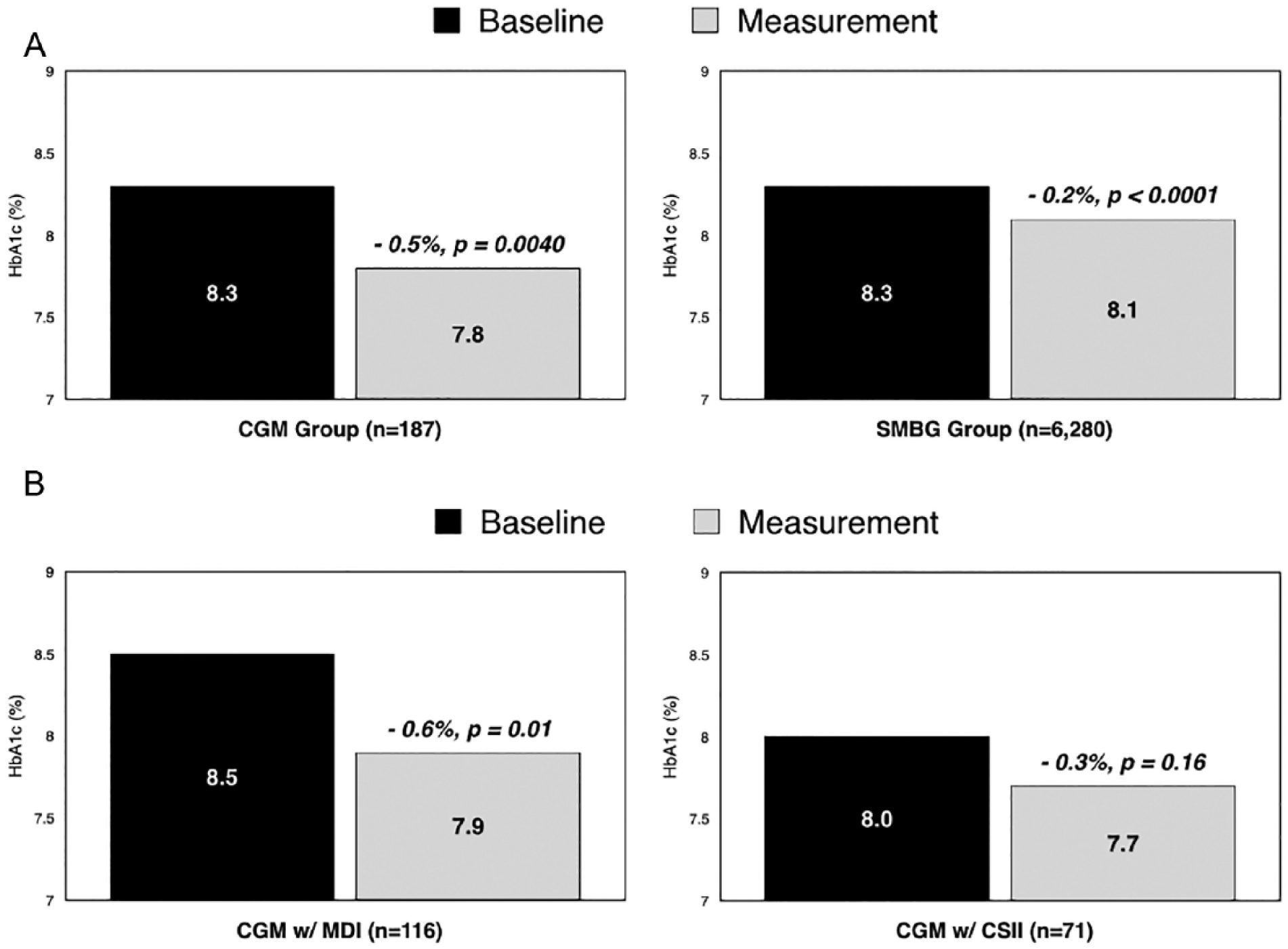
Changes in HbA1c from baseline: CGM vs SMBG (A) and CGM with MDI versus CGM with CSII (B).
Changes in HbA1c in rtCGM Group by Age.
Comparison of change in HbA1c according to insulin administration method showed a clinically significant HbA1c reduction with rtCGM+MDI but not rtCGM-CSII treatment; however, the between-group difference was not statistically significant (P = .06) (Figure 2B).
Secondary Analysis
The secondary analyses included a dataset of 22 925 patients from which 1130 were case matched (rtCGM, n = 565; SMBG, n = 565). No significant between-group differences in medical/pharmacy costs, gender, age, region, or comorbidities were observed. Patient demographics before and after propensity score matching are presented in Table 1.
Health Care Service Utilization
The number of all-cause inpatient admissions among rtCGM patients was significantly lower compared with SMBG patients with notably lower associated costs PMPM (Figure 3A). The number of diabetes-specific inpatient admissions and costs were also notably lower. The number of inpatient admissions coded for DKA among SMBG patients was more than double the number reported for rtCGM patients during the measurement period: 36 versus 16, P = .0675
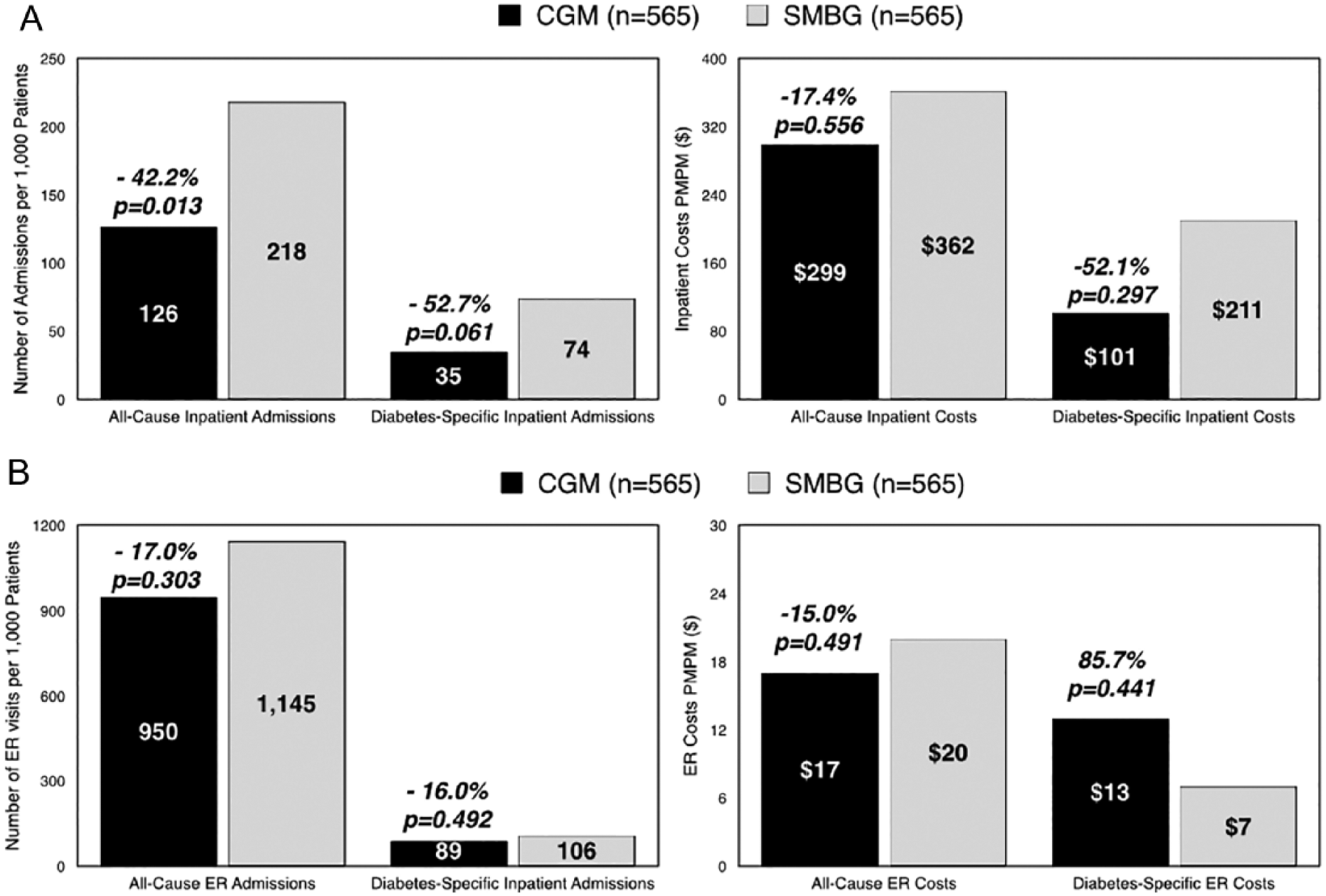
Utilization of health services and costs: Inpatient admissions (A) and ER admissions (B).
The number of all-cause ER visits was notably lower among rtCGM patients versus SMBG patients (P = .303) with associated lower costs PMPM (P = .491) (Figure 3B). The number of diabetes-specific ER admissions was also lower among rtCGM patients versus SMBG patients but with higher associated costs.
The number of ER visits coded for DKA among SMBG patients was more than four times higher than reported for rtCGM patients during the measurement period: 17 versus 4, P = .0318. Similar differences between rtCGM versus SMBG patients were also seen in the number of ER visits coded for hypoglycemia: 2 versus 7, P = .353
Discussion
Several recent studies have shown that use of rtCGM in conjunction with CSII treatment reduces HbA1c levels and occurrence severe of hypoglycemia and/or duration of hypoglycemia in pediatric and adult T1D populations.7,14,18-21 However, recent evidence suggests that rtCGM use in conjunction with MDI treatment may provide the similar glycemic benefits without the additional costs associated with CSII therapy. 22
Our study found that use of rtCGM was associated with reduced HbA1c and utilization of health services compared with SMBG use regardless of insulin delivery method. In addition, rtCGM use was associated with notably fewer inpatient admissions and ER visits coded for DKA and hypoglycemia, which can have long-term effects on patient adherence. For example, as patients quickly learn that hypoglycemic episodes are physically aversive, potentially dangerous and a source of possible social embarrassment, they become fearful of hypoglycemia. 26 In many cases, this fear becomes a key obstacle to intensifying therapy and/or adhering to prescribed insulin regimens,27,28 which often leads to poor metabolic control and subsequent health outcomes. 29
A 2016 report from the T1D Exchange registry showed that among CGM users there was no significant difference in HbA1c levels between CSII and MDI patients. 30 Our findings provide further evidence supporting rtCGM use regardless of insulin delivery method; however, the greater HbA1c improvements seen in the rtCGM-MDI group versus rtCGM-CSII add further support to the willingness of MDI-treated patients to utilize rtCGM data in their self-management. In a recent survey, Pettus and Edelman 2 found that rtCGM-MDI and rtCGM-CSII patients made similar changes in their correction and prandial insulin dosages based on their rtCGM data. Because rtCGM-MDI patients experienced greater HbA1c reductions, but without the added expense of CSII therapy, the cost savings may become an important factor when selecting an insulin administration method (MDI vs CSII).
We recognize that the higher baseline HbA1c levels among rtCGM+MDI users likely contributed to the more notable HbA1c reductions among rtCGM+MDI users. Therefore, although a more reasonable characterization of our findings would be that rtCGM use with either MDI and CSII confers similar glycemic benefits, rtCGM+MDI treatment may be considered more “cost effective” on the basis of this 1-year analysis as it eliminates the initial and ongoing costs of insulin pump use.
A key strength of this study is our utilization of propensity score analysis, which allowed us to identify equivalent comparison groups, 31 thereby facilitating a true comparison between study groups. Another strength of our study design was use of longitudinal analysis used in a real life setting. This approach allowed us to measure the occurrence of change in SMBG acquisition behaviors and subsequent outcomes at the individual level, providing the opportunity to observe individual patterns of change. 32
A key limitation of the study is the small sample size of rtCGM users with pre and post HbA1c test values; a larger sample size would have provided a more robust assessment of the impact of rtCGM use on glycemic control and health service utilization. Another limitation was the design of the study. It is well known that retrospective analyses inherently include confounding variables, which may go unrecognized because of inadequate knowledge of how they interrelate with the outcomes. Although we were able to show associations between treatment modalities and outcomes, we cannot establish causal relationships. In addition, the Optum data set provided no information regarding the socioeconomic, educational characteristics or participation in a formal diabetes self-management education program, all of which could have affected outcomes.
Conclusions
Use of rtCGM in T1D patients facilitates greater improvements in HbA1c and reduced health care system utilization compared with traditional SMBG use regardless of insulin administration method. Treatment with rtCGM in conjunction with MDI confers similar or greater glycemic benefits without the additional costs associated with CSII therapy.
Footnotes
Acknowledgements
The authors wish to thank Stephanie MacLeod, Shirley Musich, Hungching Chan, Mark Holmberg, and Kevin Hawkins for their assistance in conducting the analysis.
Abbreviations
CSII, continuous subcutaneous insulin infusion; DKA, diabetic ketoacidosis; ER, emergency room; MDI, multiple daily insulin injections; PMPM, per-member per-month; rtCGM, real-time continuous glucose monitoring; SD, standard deviation; SMBG, self-monitoring of blood glucose; T1D, type 1 diabetes.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: CGP has received consulting fees from Dexcom, Inc, Insulet Corporation, Roche Diabetes Care, and Sanofi. CG is an employee of Dexcom, Inc. JS has received consulting fees from Dexcom, Inc.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding for this study was provided by Dexcom, Inc, San Diego, CA 92121, USA.