
Abstract
Background:
Depending on available resources, competencies, and pedagogic preference, initiation of insulin pump therapy can be performed on either an individual or a group basis. Here we compared the two models with respect to resources used.
Methods:
Time-driven activity-based costing (TDABC) was used to compare initiating insulin pump treatment in groups (GT) to individual treatment (IT). Activities and cost drivers were identified, timed, or estimated at location. Medical quality and patient satisfaction were assumed to be noninferior and were not measured.
Results:
GT was about 30% less time-consuming and 17% less cost driving per patient and activity compared to IT. As a batch driver (16 patients in one group) GT produced an upward jigsaw-shaped accumulative cost curve compared to the incremental increase incurred by IT. Taking the alternate cost for those not attending into account, and realizing the cost of opportunity gained, suggested that GT was cost neutral already when 5 of 16 patients attended, and that a second group could be initiated at no additional cost as the attendance rate reached 15:1.
Conclusions:
We found TDABC to be effective in comparing treatment alternatives, improving cost control and decision making. Everything else being equal, if the setup is available, our data suggest that initiating insulin pump treatment in groups is far more cost effective than on an individual basis and that TDABC may be used to find the balance point.
For subjects with type 1 diabetes treatment with the glucose-lowering hormone insulin is necessary for survival. In some instances continuous administration through use of an insulin pump (continuous subcutaneous insulin infusion; CSII) is preferred to intermittent administration even though upfront this might be perceived as more costly due to the cost of the pump and supplies. 1 Depending on available resources, competencies and pedagogic preference, the initiation of CSII can be performed either on an individual or group basis. Treatment results and patient preference aside, little is known about the cost-effectiveness of these models.
Controlling cost and increasing the precision of decision making is important in any business.2-4 Activity-based costing (ABC) offers the possibility of absorbing costs in terms of activities and may be particularly suited for service businesses, 5 not least where alternatives for the same service are available. ABC is an advanced cost allocation technique by which cost drivers in terms of activities are identified and to which indirect costs such as overhead are specifically allocated. However, detailed and time consuming measures may be costly and noted as a major barrier to ABC implementation.5,6 Accordingly, so-called time-driven ABC (TDABC) was developed as an alternative to ABC with greater utility.5-8 It requires only that the unit cost of supplying capacity is determined and that the time required performing a transaction is measured, and seems to capture organizational complexity better than traditional ABC by working with multiple time-drivers. 9
Here we applied TDABC in the comparison of initiating CSII in groups to its initiation on an individual basis.
Methods
Data were derived from the Department of Endocrinology at Skåne University Hospital at its two sites in the cities of Malmö and Lund, Sweden, during 2011 and 2012. TDABC was performed as described by Kaplan and Anderson.5,6 Cost drivers were identified and routines timed or estimated at location to compare the treatment initiation alternatives. Cost drivers of the care delivery chain at the service for initiating CSII on an individual (IT) or group basis (GT) were identified by interviews and estimation (Tables 1 and 2). Data were validated by the department secretary responsible for follow-up statistics and the nurse primarily in charge of CSII. Medical quality and patient satisfaction were assumed to be at least noninferior between IT and GT. Overhead costs were allocated differentially based on profession and manager(s). Cost per time unit was calculated straightforward without adjusting for idleness since we did not expect this to be a significant variable, or at least not differ between the alternatives. Rebooking or cancelling appointments in this patient group is rare, and this potential additional labor was not accounted for. The alternatives were compared under open hypothesis generating scenarios and conclusions adjusted for the net effect of differential reimbursement.
Time-Driven Activity-Based Costing Estimate of Insulin Pump Therapy Initiation Based on an Individual Scheme.
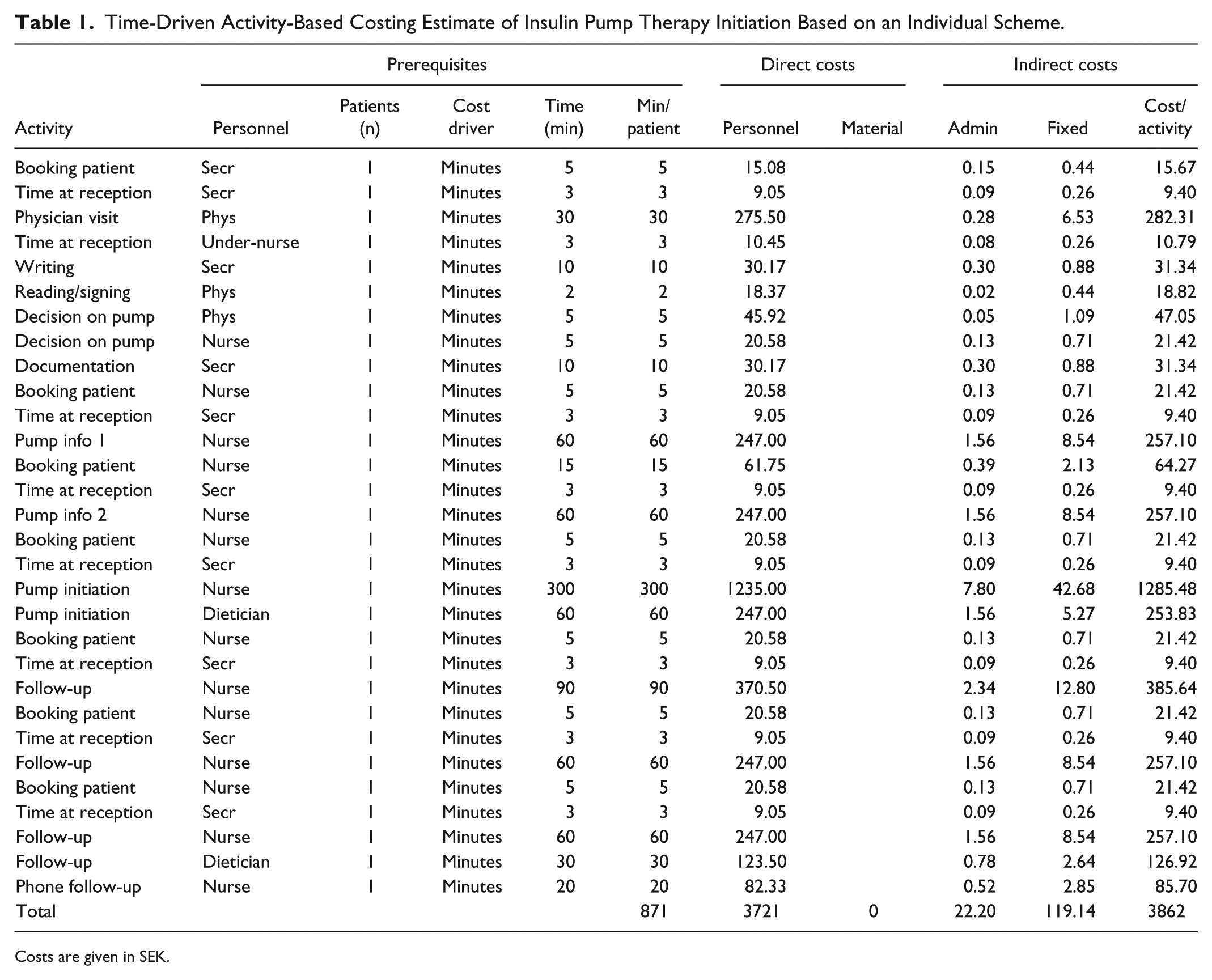
Costs are given in SEK.
Time-Driven Activity-Based Costing Estimate of Insulin Pump Therapy Initiation Based on a Group Scheme.
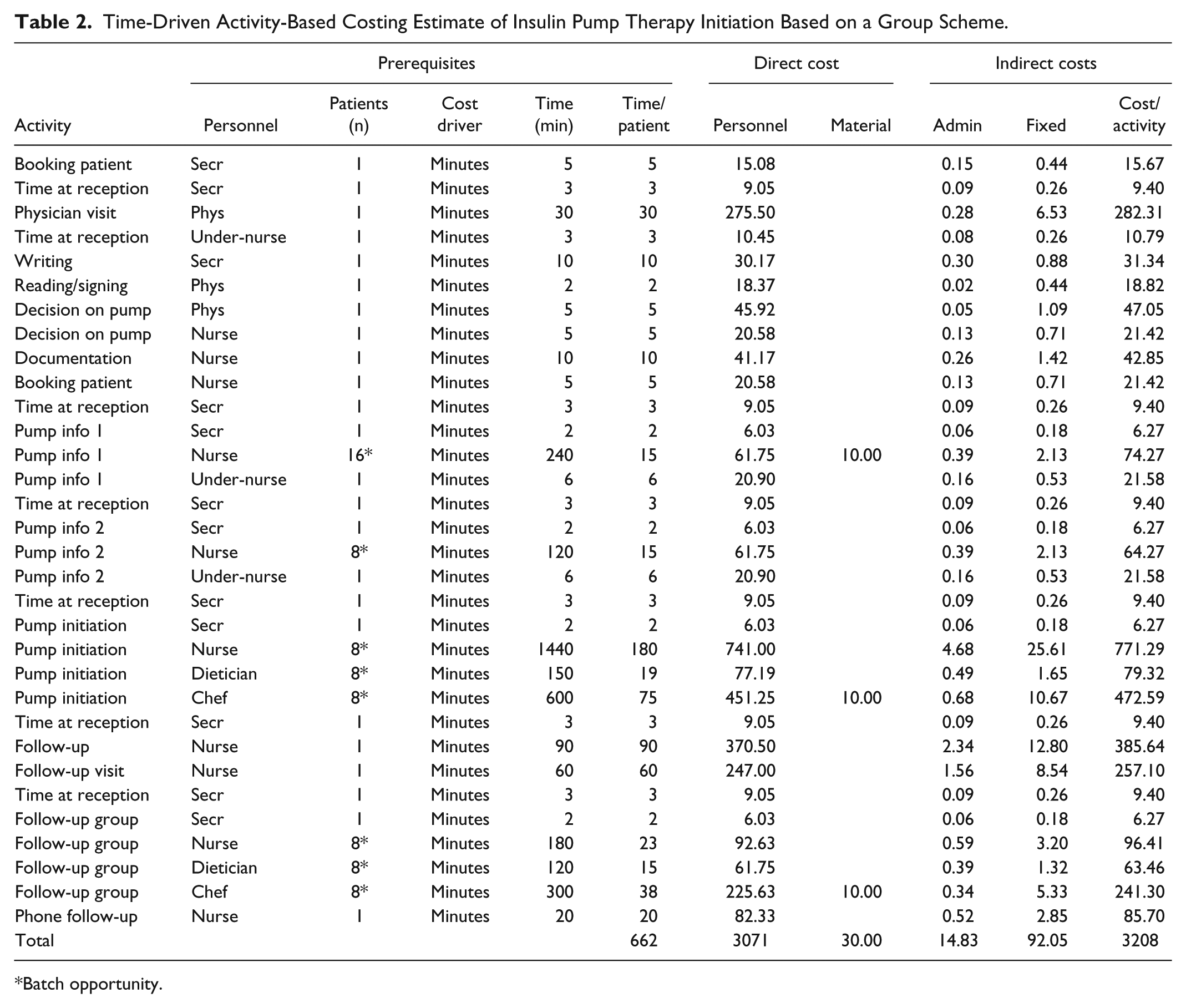
Batch opportunity.
Overhead and Cost Allocation
The following overhead costs from administration were considered: head of department, 20% of wages considered part of the work force and the rest was allocated to each resource (equal to a full-time employee) on a 1:0.8 ratio between physicians and other professionals; deputy head of department, 100% of wages allocated equally to each employee; assistant head of department, 40% of wages allocated equally to each resource; first-line manager outpatient ward Malmö, 70% of wages allocated to all professions but physicians; first-line manager day care ward Malmö, 40% of wages allocated to all professions but physicians; first-line manager outpatient ward Lund, 100% of wages allocated to all professions but physicians; first-line manager medical secretaries in Malmö and Lund, respectively, 40% of wages allocated to each secretary resource. The following overhead costs from fixed costs were considered: Rent, allocated equally per resource (rent is reimbursed on a 1:1 basis, that is, does not add or subtract value but is part of the cost driving structure); personal computers, allocated per resource (each employee has one available work station); telephone costs, allocated equally among employees; financial costs, ditto; education and conference fees, according to fixed scheme per profession (not shown). This allocation meant that overhead from administration was highest among the secretaries and lowest among the physicians, and vice versa for fixed costs. Fixed costs were also more than six times those of the administration (not shown). Costs are given as Swedish krona (SEK); one SEK is approximately equivalent to 0.11 USD.
Results
Initiating Pump Therapy on an Individual Basis
Table 1 describes the activities that were identified for IT initiated CSII. All costs from the initiating physician visit including booking costs to the last nurse follow-up visit were included so as to dilute the effect of the actual initiation with all factual activities surrounding it. This enabled comparisons of similarities and differences between IT and GT, and simulation of alternative or opportunity costs and different scenarios. The activities leading to a complete IT initiation consumed 871 minutes that drove costs differently depending on who was performing the activities and how overhead was allocated to that person (Table 1). Indirect costs constituted only 4% of the total cost of activities and out of the activities those related to the nurse work was by far the most significant. This being said, the 50.000 SEK cost of pump and supplies (first year) greatly outweighed the cost of the activities of about 3.900 SEK that represent a net inflow considering the 16.088 SEK reimbursement for visits in this particular health care setting. The net revenue for IT initiation of CSII was negative at 37.775 SEK per patient.
Initiating Pump Therapy in Groups
Table 2 describes activities for GT initiation of CSII. Similar to IT, all costs from the initiating physician visit including booking costs to the last nurse follow-up visit were included so as to dilute the effect of the actual initiation with all factual activities. Activities leading to a complete GT initiation consumed 662 minutes; 32% less time than IT. However, cost drivers behaved differently according to who was performing the activities and how overhead was allocated to that person (Table 2). Indirect costs constituted only 3.5% of the total cost of activities but there was a 1% shift of costs related to the direct costs that was represented by materials (food during group sessions). Again, out of all activities those related to the nurse work was by far the most significant. In this particular health care system, group session reimbursement is greater than for ordinary visits to compensate for the involvement of multiple professions. Hence, total reimbursement was 20.499 SEK for GT initiated CSII. The net revenue for group based initiation was still negative at 32.710 SEK per patient due to device cost.
Comparisons Between Individually and Group-Based Pump Therapy Initiation
The first difference noted between IT and GT initiation was the use of reception/secretary time. Patients attending groups were routinely doubly registered, first at the reception desk and then at the outpatient ward where sessions were conducted. Up until that point there were no differences between activities or cost drivers between the alternatives. The second major difference was that information about CSII was performed in groups of up to 16 patients which greatly reduced the cost driving effect. By this factor alone the first of two information activities was about twice (but only twice) as costly for IT. If the simple activities related to registrations are reduced this increases to a factor three. Conversely, reducing the number of patients that are informed to between four and five, the GT advantage is completely lost.
Another way to treat this particular cost driver (or composite driver since there are different activities related to the information activity such as booking, reception time, and nurse time) is to consider them batch-wise. Different scenarios were evaluated. Theoretically, cost accumulation may be based on the cost per patient when information sessions are conducted individually or in groups based on the activity cost per patient in full groups of 16 patients. This group cost accumulation is unrealistic since the cost for patients not able to attend and for whom alternative measures have to be taken, should also be taken into consideration. This cost is often very substantial. Nonetheless, these cost accumulation curves serve as base case scenario extremes (Figure 1). If group sessions are conducted only as batches, that is, only when a group of sufficient size can be formed, the generated cost per patient would be the same for GT and IT until a total of (in this case) 16 patients can be booked for the first information group session. Then it would drop substantially, down to the theoretical minimal extreme (Figure 1A). This case is relevant to services with an insufficient number to form full groups. In terms of scale it generates a jigsaw pattern of potential accumulated costs (Figure 1B). More realistically, costs will vary depending on the number of patients that can attend either of the two alternatives. We call this the variable batch scenario (Figure 1A). Again, the alternative cost was calculated as the additional cost to perform the same activity according to the IT base case. Taken together, this set-up generates break-points for when it is (financially) acceptable to deviate from GT in general and group size in particular (Figure 1A) and the financial behavior of scale (Figure 1B). Based on the cost driving data in this study, if the service is able to handle both kinds of treatments, GT will be more cost driving than IT until a group of at least five patients can be formed. Beyond groups of five patients, GT is cost sparing.
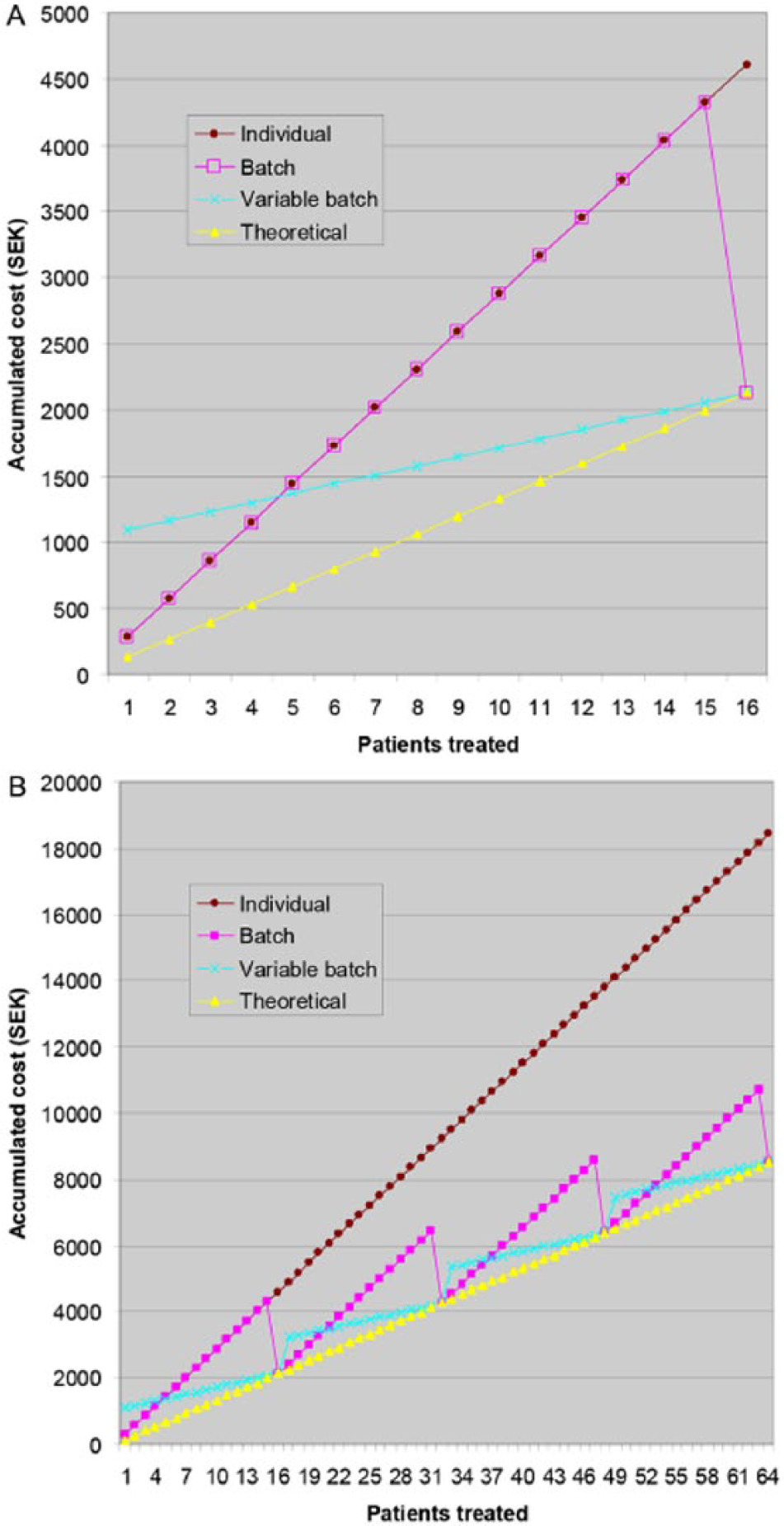
Accumulated costs for informing about insulin pump therapy by individual sessions (Individual), or in groups performed only as full batches (Batch) or in groups of variable size where the remaining patients of a batch receive individual information (Variable Batch) compared to the theoretical lowest accumulated cost for patients receiving information in groups (Theoretical) after the first 16 (A) and 64 (B) patients.
As pointed out above, looking only at accumulated cost allows for cost control but not necessarily improved decision making since this also requires an estimate of the alternative cost. Figure 2 describes one way of acquiring this knowledge by looking at the accumulated batch cost, that is, what it would cost per 16 patients to either IT (stepwise accumulation as in Figure 1) or mixing IT and GT (jigsaw accumulation as in Figure 1). From this it may be determined how much costs are declining as the group-to-individual treatment ratio increases (Figure 2A). Subtracting the stepwise costs from the jigsaw costs results in a curve illustrating the alternative cost. The read-out from these curves is not only that variable batch is less cost driving already when five people are informed as a group and the remaining 11 individually, but also that the curves for variable batch cost and alternative cost converge when this ratio is 15:1 for the first 16 patients. Beyond this point informing in groups allows the opportunity to inform another 16 patients at no additional cost. Taking advantage of this “cost of opportunity” modifies the jigsaw cost of the group alternative as well as the resulting cost of opportunity. For clarity this downward shift of costs as the opportunity cost is realized after the first batch is illustrated in Figure 2B.
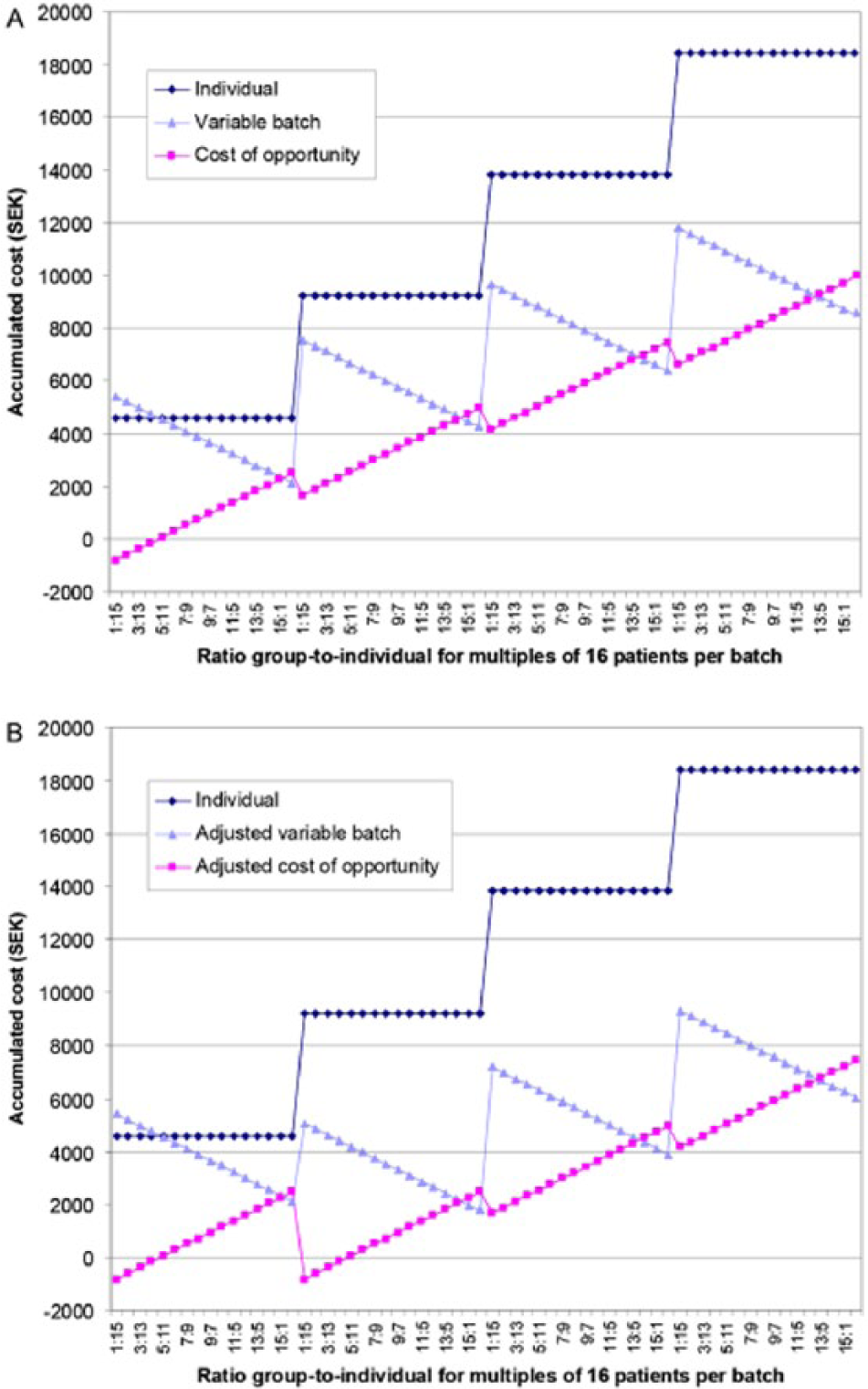
Accumulated costs per batch of 16 patients for informing about insulin pump therapy by individual sessions (Individual), or in groups of variable size where the remaining patients of a batch receive individual information (Variable Batch) where the difference describes the cost of opportunity, here shown either not realized (A) or realized to initiate a second group after the first batch (B).
The last difference was the activities surrounding the actual initiation of CSII and the nature of those activities. The alternatives differ in qualitative terms since GT involves two nurses during the period when pumps are started, a dietician who contributes with how to calculate dose according to caloric load and carbohydrate content, and a chef that prepares standardized meals together with the patients. Still, from initiation to follow-up, GT was 10% less costly than IT in the base case scenario. Both alternatives come with a net financial loss during the first year in the Swedish health care system due to reimbursement rules and the relatively high cost of device and supplies of roughly 50.000 SEK during the first year. The net loss per patient was 5.065 SEK or 20% to the advantage of GT over IT, the majority of this sum being due to differences in reimbursement. 654 SEK per patient came from activity-based cost drivers, equivalent to a 17% decrease in cost per patient.
Discussion
We implemented TDABC to compare alternative health care procedures assumed to have (at least) equivalent effects in qualitative terms but where either costs themselves may be an issue, or methods and measures can be put into perspective in terms of cost and alternate cost. An added advantage of TDABC was the increased decision-making power when it comes to accepting protocol deviations. Here we studied initiating CSII in adult subjects with type 1 diabetes, a time-intensive and expensive exercise, both for patients and health care system. But the approach is naturally implementable for other services and settings as well. By restricting the approach to selected processes we expect that the costs of TDABC can be kept to a minimum while conclusions and experience may be transferred to other activities that may benefit.
One of the most interesting findings was the ability of TDABC to determine when to accept protocol deviations from a financial point of view. This was exemplified by the comparison between informing patients individually, in groups, or as a combination of the two where patients failed to attend group meetings. This choice is very relevant to the real life situation and we view it as an important operational finding. Surprisingly few patients had to attend the group sessions for them to be cost effective even though this generated an alternate cost, only five out of 16 patients where the remaining 11 would have to be offered individual sessions. Furthermore, with greater efficiency, here a group-to-individual treatments ratio of 15 to one, comes a cost of opportunity that is equivalent to initiating a second group at no additional cost. Conversely, for smaller services it should also be possible to understand at what cost GT comes and to explain to management why this may not always be the most cost effective alternative.
It is well known that conventional cost accounting has a tendency to undercost low-volume services or products and overcost high-volume ones and it is possible that ABC and TDABC alleviates this problem.10,11 The implementation of TDABC itself seems highly appropriate since all the cost drivers that were identified and could be traced to the relevant activities were multiples of time spent performing a task. Differentiating between batch-wise and unit-wise work does add complexity to the analysis but is basically not different in terms of what drives the cost. The important issue is that there should be a cause-effect relationship concerning cost objects, drivers and indirect costs. 11 This relationship may come naturally from the context, for example, health care setting, available staff, and patient volume.
There are some limitations to our study. First, it is likely that not all cost drivers were identified and that at least some time measures or estimates were biased. This would lead to insufficient accuracy.6-8 In fact, since the allocated overhead, normally an advantage of using ABC, was relatively low this particular benefit may not be apparent in the current case. In general though, ABC is considered more accurate (but also more costly in performing) than conventional cost allocation. 11 Second, from a relative point of view and for reasons of transparency, all identified costs were included in this analysis. From the service perspective however, this may not be necessary since no saving or losses can be made on, for example, rent for which this particular department is fully reimbursed, or even for the pump devices themselves since they come with a separate budget. This problem may be overcome by grouping some cost drivers once their internal relationship have been determined, and separating others from the analysis. For example, once the supply chain of the service has been identified this may be viewed as one optimized package or activity consisting of a secretary, a nurse, and a physician; sometimes referred to as determining the standard full-cost-per-service unit.11,12 An inherent limitation is also the lack of separating practical from theoretical capacity which is often estimated at 80-85%.5,6 We did not include this aspect since our main objective was to compare methods. It is also possible that idleness differs consciously or unconsciously between working individually and on a group basis. We do not expect that this would alter the confirmation of the intuitive belief that group-based approaches are more cost effective than individually based approaches. Last, one may argue that since in this particular case the majority of the total cost can be traced to the device and the majority of the net difference in cost can be traced to differences in reimbursement it may not be worthwhile to set up TDABC. While this may be true for some processes the argument works both ways and is not applicable. Sometimes skilled people are more expensive than their working material, sometimes it is the other way around. For insulin pumps as for other high tech devices one might expect competition to drive prices down significantly already in the next few years as their use becomes more widely implemented. In addition, it is likely that adequately informed managers act far more quickly in adjusting services than does the prevailing global reimbursement system diagnosis related groups. 11
It is important to acknowledge that we did not asses or compare the clinical effectiveness of initiating pump treatment individually or in groups. In fact, although recognized by many in clinical practice as potentially more effective due to the added benefit of group dynamics and peer support, we are not aware of any randomized studies addressing this comparison.13,14 Evidence suggesting the superiority and/or advantages come from both randomized trials 15 and observational studies following adult patients that initiated CSII in a setting very similar to the one described here for one year. 1 The ongoing Relative Effectiveness of Pumps Over multiple daily injections (MDI) and Structural Education (REPOSE) study is comparing MDI and CSII initiated in a similar manner as reported here using a modified Dose Adjustment For Normal Eating (DAFNE) structured education course which is soon to report two year data will shed further light on the effectiveness of the concept. 16 We also want to stress that the size of the groups in this report was merely evaluated from a resource perspective. In clinical practice, groups of 5-8 subjects, as is the case in the REPOSE study, are probably more common and realistic in real life practice. In addition, the example we chose here pertains to the situation for an adult population, and cost drivers in a pediatric setting may be very different. These knowledge gaps deserve further investigation.
In conclusion, we found that TDABC can be productively implemented both to compare alternative treatment protocols, and to seek ways to make these more cost efficient. It may help managers focus on value-adding activities and limit non-value-adding ones, something that is greatly called for in any business. It is also likely that TDABC increases cost control and improves decision making in such businesses.
Footnotes
Abbreviations
ABC, activity-based costing; CSII, continuous subcutaneous insulin infusion; GT, group treatment; IT, individual treatment; SEK, Swedish krona; TDABC, time-driven activity-based cost allocation.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: MR holds a position as adjunct professor at Lund University but is a full-time employee of Novo Nordisk A/S.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was funded by the Swedish Research Council