
Abstract
Diabetes is a highly prevalent disease also implicated in the development of several other serious complications like cardiovascular or renal disease. HbA1c testing is a vital step for effective diabetes management, however, given the low compliance to testing frequency and, commonly, a subsequent delay in the corresponding treatment modification, HbA1c at the point of care (POC) offers an opportunity for improvement of diabetes care. In this review, based on data from 1999 to 2016, we summarize the evidence supporting a further implementation of HbA1c testing at POC, discuss its limitations and propose recommendations for further development.
One and a half decades ago, the worldwide prevalence of diabetes was 171 million, while the prediction was 366 million patients by 2030. 1 More recent estimates point to more than 640 million people being affected by this disease by 2040. 2 With clear links to multiple comorbidities such as cardiovascular disease (including hyperlipidemia, coronary artery disease, and stroke),3,4 renal disease, (chronic renal insufficiency, dialysis and transplantation), infections, malignancy, and functional impairment, diabetes places a tremendous financial burden on both patients and health care systems. In 2012 the American Diabetes Association (ADA) estimated total economic cost of diabetes care in the United States at $245 billion, 5 accounting for more than 1 in 5 of all health care dollars spent.
Glycated hemoglobin A1c (HbA1c) testing plays a key role in the management of diabetes. 6 Guidelines on HbA1c testing frequency and treatment modifications aim at supporting the achievement of glycemic targets. However, low adherence to these recommendations among adult patients with type 2 diabetes has been reported. 7 Even when no clear explanation has been found as to why this is the case, the rapid availability of HbA1c testing results has been shown to facilitate diabetes management. 7 In response to this, HbA1c testing at the point-of-care is currently increasing. The ADA recommends point-of-care (POC) testing for HbA1c to offer the opportunity for more timely treatment changes, while the International Diabetes Federation (IDF) recommends determination of HbA1c either at the POC or in the laboratory before clinical consultation.6,8 The aim of this paper is to present current evidence supporting the utility of HbA1c testing at POC and to summarize its usefulness for diabetes management optimization. We will also discuss potential risks while presenting potential venues for implementation and risk mitigation.
Background: Rationale for HbA1c Testing
HbA1c measurement has for decades been considered one of the most important laboratory medical advances in diabetes care. Its implementation in clinical practice in the 1970s represents a milestone in follow-up and treatment guidance of patients with diabetes. 9 Soon thereafter, both landmark studies of the Diabetes Control and Complications Trial (DCCT) in type 1 diabetes 10 and the United Kingdom Prospective Diabetes Study (UKPDS) in type 2 diabetes 11 emphasized the role for HbA1c in diabetes management. 7 A link between HbA1c and diabetic complications was confirmed and the need for adequate glycemic control underscored. 9
HbA1c values represent average glycemic control over the past 2-3 months and account for both preprandial and postprandial blood glucose levels. Regular HbA1c measurement is recommended by international guidelines for all patients with diabetes for the assessment of glycemic control6,12,13 by providing information on long-term glycemic status and reliably predicting risk for diabetes-related complications.6,14-20 However, even though glycemic control has been shown to be significantly related to adherence to HbA1c testing frequency and treatment modification recommendations, compliance to these recommendations is observed in only about 3% of patients. 7
A major challenge in successful diabetes management is addressing poor glycemic control. According to NHANES (National Health and Nutrition Examination Survey), only 63.7% of the patients with diagnosed diabetes met their individual goal for HbA1c. 21 Approximately 50-60% of patients with HbA1c levels above target are either not adherent to their diabetes care plan or are not on an aggressive enough care plan to intensify glycemic control. 22 Delays in treatment escalation are reported to cause not only long (>12 months) periods of hyperglycemia, but also to diminish the chance of success once therapy is eventually intensified. 22
Good glycemic control is a prerequisite for prevention and reduction of complications. Given the importance of good glycemic control in general health outcomes, regular HbA1c testing is recommended for all patients with diabetes. 6 HbA1c testing should be performed based on the clinical situation and treatment strategy. In general, patients with stable glycemia should have at least biannual testing, while patients with unstable glycemia or unmet glycemic targets should be tested every 3 months. 6 As indicated by the ADA, the implementation of HbA1c testing at POC provide an opportunity for more timely treatment modifications. 6
HbA1c Testing at POC
Why POC HbA1c Testing?
One potential disadvantage of traditional HbA1c laboratory testing is that results are not available at the time of the patient visit due to the turnaround time required for testing and reporting. Thus, health care providers have to communicate the test result and treatment modifications sometime after the patient’s visit. This delay in communicating results can delay intensification or modification of treatment and reduce patient adherence to the treatment plan. 23 Previsit HbA1c testing (taken some days before the clinical visit), can be inconvenient and costly for patients due to the extra time and cost invested and lost in a second visit, 24 moreover patients often arrive for clinical consultation without having visited the laboratory as instructed. For a comparison on time costs of POC testing versus lab testing, see Figure 1.
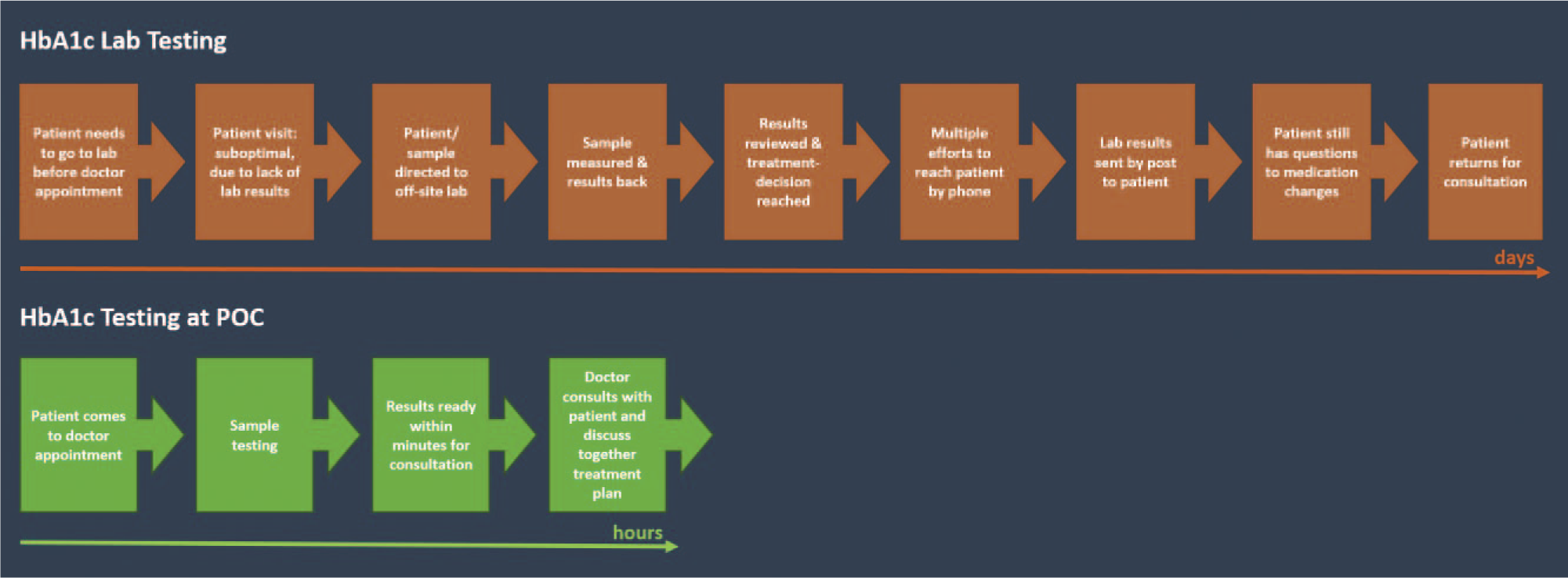
Comparison process duration between lab testing and POC testing.
POC testing is defined as “testing at or near the site of patient care wherever that medical care is needed.” 25 The intention of POC testing is to facilitate immediate medical decisions and therefore, to improve patient outcomes. 25 The rapid availability of HbA1c results permits the discussion of the results face-to-face, and has the potential to improve patient-doctor dialogue and patient satisfaction, thereby facilitating improved glycemic control. 26 HbA1c testing at POC was shown to potentially improve diabetes management if undertaken within an adequate comprehensive quality management system. 11
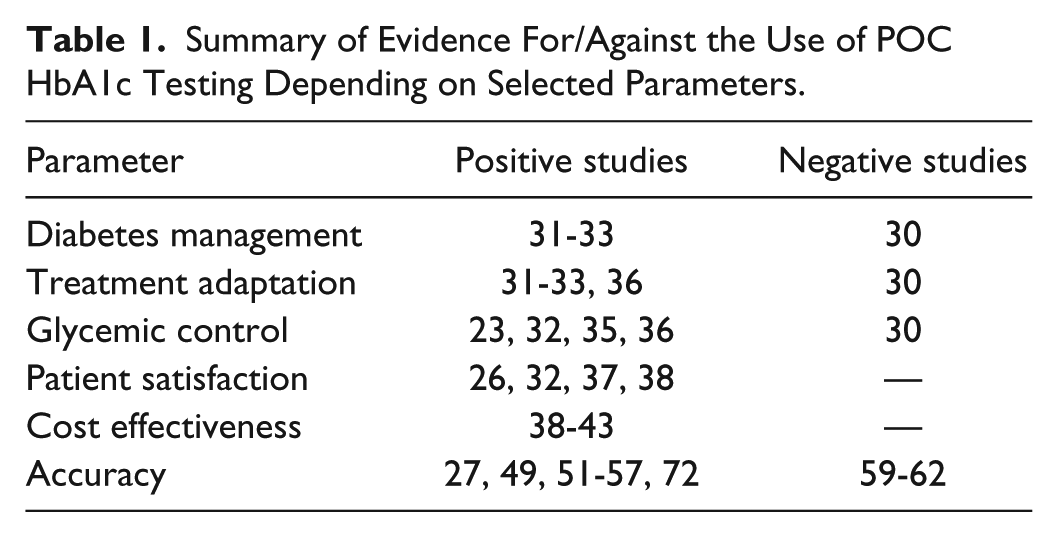
To assess the current knowledge on HbA1c testing at POC, a literature research including PubMed/Medline, EMBASE, and Cochrane library was conducted. Keyword sets combined primarily “HbA1c” and 1 of the following terms: “point of care” and “point of service.” The list of titles and abstracts contained 621 articles, which were reviewed for relevance. The span of literature reviewed covers from the end of the 1990s (1999) to the present year (2016). With regard to the progressive improvement of measurement systems, 27 more recent publications were preferred as far as possible. We included all publications fulfilling a set of quality criteria including patient number, statistical method/bias.28,29 A summary of the reviewed evidence on POC can be found in Table 1.
Summary of Evidence For/Against the Use of POC HbA1c Testing Depending on Selected Parameters.
Strong Evidence Supports POC Positive Effects on Glycemic Control and Patient Satisfaction
Although a 2011 meta-analysis concluded that there was a lack of evidence supporting the use of POC HbA1c testing for diabetes management, the limited number of studies included in the meta-analysis (n = 7), together with the heterogeneity of patient groups and trial designs, precluded a thorough analysis. Therefore, the conclusions reached by the aforementioned article are disputable. 30
a. Improved diabetes management/treatment adaptation
A range of studies have demonstrated the benefits of POC HbA1c testing for improved diabetes management and glycemic control. In a trial with 597 people with type 2 diabetes visiting a neighborhood primary care clinic, prompt availability of HbA1c results was associated with an increasing frequency of treatment intensification and a decrease in HbA1c levels. 31 Beneficial effects of rapid HbA1c analysis on diabetes management were also reported by a randomized study conducted at an outpatient facility. More than 1000 patients with type 2 diabetes were randomly assigned to a “rapid” group (HbA1c results immediately available) or a conventional group (measurements available after the patient left the clinic). Not surprisingly, over 2-7 months of follow-up, diabetes management was more appropriate in the “rapid” group (79 vs 71%; P = .003), which was mainly attributable to a less frequent treatment escalation in patients with ≤7% HbA1c levels (10 vs 22%, P < .0001). In patients of the POC group with HbA1c results >7%, the therapy was slightly more frequently intensified (67 vs 63%; P = .33). In conclusion, rapid availability of HbA1c results facilitates diabetes management. Since the beneficial effects on HbA1c profile in the “rapid” group were found to be independent from the decision to intensify treatment, other factors such as enhanced provider and/or patient motivation might be involved. 32 As emphasized by the authors, rapidly available HbA1c results facilitate identification of patients with good metabolic control (HbA1c levels ≤ 7%) and, therefore, mitigates potential hypoglycemia risk from inappropriate treatment escalation. 32
To evaluate the potential effects of the implementation of POC HbA1c testing in a primary care setting, data from 164 patients with type 2 diabetes in a primary care setting were reviewed. 33 Data were collected 6 and 3 months before POC testing implementation, and again at 3 and 6 months after implementation. Documentation of adherence to guideline compliant HbA1c testing frequency by health-care providers increased from 65.9% and 68.3% (6 and 3 months before implementation) to 82.9% and 95% (3 and 6 months after implementation). 34 There was also a reduction in mean HbA1c from 8.1% (6 months preimplementation) to 7.7% (6 months postimplementation) (P = .008). Attending to these results, HbA1c testing at POC can potentially contribute to an improved adherence to guideline recommended testing frequency. Furthermore, the possibility to provide and discuss HbA1c results face-to-face has the potential to improve patient-doctor dialogue and patient satisfaction, thereby facilitating glycemic control. 26
b. Improved glycemic control
A randomized controlled trial in 201 insulin-treated patients (type 1 or type 2 diabetes) showed an association between prompt availability of HbA1c results and a significant improvement of glycemic control. 23 In 100 patients, HbA1c results were available at the beginning of the visit, whereas for the 101 control patients results were provided by the laboratory after consultation. The favorable effect of rapidly available HbA1c results on glycemic control was detected at 6-month follow-up (–0.57 ± 1.44%; P < .01) and persisted for another 6 months (–0.40 ± 1.65%, respectively; P < .01). Conversely, patients in the control group had no significant HbA1c changes. 23 Since no change of total insulin dose was appreciated, the immediate feedback of HbA1c results may possibly facilitate appropriate insulin regimen adjustments.
An even more sustainable benefit of readily available HbA1c results at the POC was demonstrated in a large, retrospective, cross-sectional study based on more than 16,000 HbA1c analyses. Significant HbA1c improvements associated with POC testing were detectable even after 3.5 years. 35
POC also resulted in glycemic control improvement in a pilot-study set in an urban community health center from a low-income and low empowerment zone. 106 patients with diabetes were enrolled, of whom 69 had both pre- and post-POC implementation data. The trial evaluated the implementation of finger-stick HbA1c testing at POC. 36 This intervention was associated with an HbA1c testing rate increase from 73.6 to 86.8% (P = .40) and was well accepted by both nurses and physicians. Comparison of pre- and postintervention results revealed a significant decrease in HbA1c levels (7.84 vs 8.55%; P = .004). 36 This finding corresponded to an increase in treatment escalation in patients with HbA1c values >8.0% from 28.6 to 53.8% (P = .03). The positive outcome was mainly credited to the opportunity for immediate face-to-face counseling once the POC HbA1c results were known. 36
c. High patient satisfaction
Further to the positive effects on glycemic control that are associated with the use of POC, there are also reports of increased patient satisfaction and motivation. For instance, in the framework of a large multicenter, randomized, controlled trial assessing the extent of POC testing in Australian general practices, patient satisfaction was assessed via questionnaire. 37 Patients randomized to POC testing reported higher satisfaction levels with the sample collection process (P < .001) and more confidence in the process (P < .001). Moreover, according to patients assessments, POC testing was able to enhance their relationship with their physician (P = .010). 37
Subjective perceptions of health-care providers and patients regarding POC testing impact on diabetes management were examined in a qualitative study based on in-depth interviews. 26 All interviewees agreed that an improved opportunity for treatment adoption provided by the rapid availability of HbA1c results was an important advantage of POC testing. A positive reception of HbA1c testing at POC by both patients and physicians was reported.23,38 Furthermore, POC testing was regarded as offering an excellent opportunity to enhance patient’s diabetes education and motivation. 26
Higher patient satisfaction might also be a result of the decreased patient revisits associated with POC implementation. Up to 61% reduction in patient revisits has been reported with implementation of POC testing. 39 A lower frequency of patient visits may contribute to a substantial reduction in annual diabetes care costs for patients. 38 In addition, from a patient’s perspective, revisits may also involve other inconveniences and/or additional costs due to travel, parking, copayments, and potentially lost wages. 39
Emerging Evidence Supports POC Cost-Effectiveness
Despite the wealth of studies focusing on effects over glycemic control and/or patient psychological well-being, there is relatively little published evidence on the cost-effectiveness of POC.38-42 Even when it seems clear that the unit cost of POC tests is higher than testing at a central laboratory, 40 the reduction of patient revisits associated with HbA1c POC testing may result in a reduction in health care costs. 38 In a recent study, HbA1c testing at POC was found to be cost-effective in a primary care setting. 39 POC testing resulted in increased operational efficiency in primary care practice. With POC testing implementation the total test number/per patient visit decreased (-21%; P < .0001), as did telephone calls to patients (-89%; P < .0001), the number of results letters mailed to patients (-85%; P < .0001), and the number of follow-up visits for an abnormal laboratory result (-61%; P = .002). 39 In agreement with this result, the analysis of approximately 300 cases showed significant potential financial savings opportunities for primary care practices with the adoption of POC testing. 39 With increased focus on pay for performance and accountability for care, improved glycemic control associated with POC testing may lead to cost savings through reduced complications and in-hospital admissions. A considerable potential for cost savings due to HbA1c testing at POC was also reported in a budget impact analysis for Ontario, Canada. 43 Regardless of present evidence, calculating cost-effectiveness for POC testing remains an open question, especially considering the multilevel impact of diabetes management. 27
POC Analytical Accuracy and Performance: Room for Improvement
An important issue regarding POC HbA1c testing evaluation is that while some systems have been shown to have acceptable analytical performance not all have.27,34,44,45 So far, the insufficient evidence for analytical performance of HbA1c testing devices in diagnosis of diabetes has limited their use in this application. In fact, in the past decade only hospital laboratory HbA1c instruments have been recommended for use in diabetes diagnosis and to date only a handful of these have been cleared by the US FDA for this use. 46
With the endorsement of HbA1c for diagnostic use and the tightening of the NGSP criteria in recent years, 47 POC technology has experienced strong development, improving both hardware and software of POC devices,27,48 so much that a review of an external quality assurance survey in Norwegian general practice offices and hospital laboratories, showed very good results for certain POC testing devices. 34 Over the course of 6 years, about 60%–90% of general practices using POC testing met the quality specifications both for truthfulness (≤6.0%) and imprecision (≤0.3%) in diabetes diagnostics. This was comparable and even slightly higher than the 54-84% of the hospital laboratory methods, which met the same quality specifications. There is growing evidence for a high quality of analytical performance. Moreover, analysis of POC results has demonstrated a strong correlation between values obtained from capillary and venous blood samples. 49 Furthermore, a moderate quality evidence for a positive correlation between HbA1c testing at POC and lab results was also reported by an evidence-based analysis of studies published between January 2003 and June 2013. 50 High accuracy and precision of HbA1c testing at POC with different devices has been repeatedly reported,51-57 making POC a useful aid in diabetes management. 58
However, several studies of the analytic performance of various POC HbA1c systems have found significant differences in performance. While some POC methods have a high quality performance, others might meet the criteria for precision but not for bias, or simply result inferior to laboratory systems.59-61 Therefore it is important to evaluate the performance of POC systems in independent evaluations of analytical performance to understand the clinical utility and potential risks of various POC methods.
Further factors that might limit POC HbA1c accuracy are more related to measuring HbA1c itself. For instance, certain blood related illnesses (anemia), which affect red blood cell life span can impact HbA1c results. In addition, race/ethnicity might also affect HbA1c results (for example, African Americans might have higher HbA1c levels than non-Hispanic whites despite similar fasting glucose levels), although this is ontroversial.62,63 In children, HbA1c has been shown to significantly correlate to mean blood glucose. Similarly as for different ethnicities, so far the ADA has not differentiated its recommendations for HbA1c depending on age.62,63 Importantly, these considerations are not unique to POC HbA1c testing methods and can affect central laboratory results as well.
Despite the above, some POC HbA1c systems can achieve the analytical quality specifications for diagnosing diabetes mellitus, while their performance has demonstrated analytical quality equivalent to that of hospital laboratory systems. 34 The remarkable improvement of analytical performance of POC devices for HbA1c testing in recent years, together with the development of new diagnostic materials 64 or the miniaturization of devices 48 argue in favor of an expansive diagnostic potential in the near future. 65
A further consideration for POC testing success is the implementation of appropriate quality control measures. Participation in external quality control programs or proficiency testing (EQA, external quality assessment)66,67 is a possibility and can assist in monitoring quality of results. It is critical to follow the manufacturer’s instructions in the use of external quality control materials for regular quality control surveillance. Although CLIA waived tests have been shown to have a significant correlation with lab tests,68,69 several reports on the use of waived tests have pointed to the need for proper personnel education to ensure the reliability of the results of POC testing. 70 Therefore, adequate training and continuous personnel education is recommended to ensure POC reliability.
Necessary Future Developments
The great expansion and serious consequences of the diabetes epidemic creates a growing need for innovative diagnostic tools. The ADA already includes in its treatment guidelines a recommendation toward regular prediabetes testing.6,62 However, despite the positive impact on glycemic control and patient satisfaction of POC HbA1c testing for monitoring patients with diabetes, POC HbA1c is not yet recommended by the ADA for identification of prediabetes or diabetes diagnosis. 62 To that end, an agreement on evaluation parameters that include both accuracy and patient centered outcomes in an integrated approach might be warranted. 27 A new method to incorporate multiple test attributes in evaluating POC tests was presented at the NIH-IEEE 2015 Strategic Conference on Healthcare Innovations and Point-of-Care Technologies for Precision Medicine (9-10 November, 2015, Bethesda, USA). This method aims at outlining and visualizing the balance between the benefits and harms associated with tests, the multiple attributes of POC tests, the interactions that potentially occur between these attributes, and impacts on individual and population health outcomes. 71 The aforementioned innovative evaluation approach together with continued focus on accuracy and cost-effectiveness will advance the use of HbA1c testing at POC in the management and diagnosis of patients with prediabetes/diabetes.
Conclusion
HbA1c testing at POC
increases compliance with recommendations for HbA1c testing frequency and treatment adoption
improves clinical outcomes
facilitates patient education and motivation
improves patient’s quality of life
appears to contribute to cost/time savings both for health-care professionals and patients
in the future, may prove useful for increased early detection of prediabetes/diabetes and thus the prevention of diabetes-associated complications
All the advantages mentioned above make HbA1c testing at POC a highly advantageous technique for diabetes management. Indeed POC testing of HbA1c is recommended by the ADA for monitoring patients with diabetes. Continued evidence of the accuracy improvements of various POC systems and cost-effectiveness evaluations, together with the implementation of effective quality control measures will support the expansion of these POC testing systems as the methods of choice for HbA1c testing in daily practice.
Footnotes
Acknowledgements
We thank Matthew J. Thompson and Gillian Parker for their input and comments, which greatly improved the present article.
Abbreviations
BG, blood glucose; ISO, International Organization for Standardization; NGSP, National Glycohemoglobin Standardization Program; pO2, partial pressure of oxygen; POC, point of care.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: OS has acted as member of advisory boards and/or given lectures under support from Abbott, Astra Zeneca, Bayer Healthcare, Boehringer-Ingelheim, Eli Lilly, Medtronic, Novartis, Roche Diagnostics, Sanofi; and is CEO and founder of Sciarc GmbH. JBC has no conflicts of interest to disclose. JW has not reported any conflicts of interest.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Generation of the article was supported by an unrestricted grant from Alere GmbH.