
Abstract
The number of US patients using diabetes technology is increasing, and sophisticated technologies continue to emerge. Patients using diabetes technology require access to providers prepared to offer care in this rapidly changing field. The authors sought to identify factors important to both patients using diabetes technology and providers caring for such patients. They redesigned the Diabetes Technology Clinic at an academic group practice in response to the needs of patients and providers. Ongoing analysis of best practices, patient experience, and provider feedback is essential to structuring diabetes technology clinics to meet the complex needs of patients requiring diabetes technology. To our knowledge, this is the first report describing a systems engineering approach to develop a diabetes technology clinic.
From 2010 to 2015, the number of people in the United States using insulin pumps increased from an estimated 400,000 to 525,000. 1 Sophisticated diabetes technologies continue to emerge, including sensor-augmented insulin pumps and low-glucose insulin suspend systems, representing a further step toward closed-loop systems. Studies show that use of diabetes technology improves clinical outcomes and patient satisfaction. Furthermore, the ease of technology use has led to improved diabetes management.2,3 Experts anticipate that technology improvements will result in more patients adopting the technology.
Continuous glucose monitors, insulin pumps, and first-generation closed loop control systems have evolved rapidly over the past 15 years. Incorporation of these technologies into clinical practice and patient self-management has been challenging. Clinics have needed to develop new education practices for patients using diabetes technology. While diabetes technology’s effect on education practices has been studied, less study has addressed how to structure clinics to serve patients using diabetes technology. In a previous benchmarking study, the authors identified a lack of clinics focused on incorporation of diabetes technology and determined a need to establish a best practice. 4 Clinical care of patients who use diabetes technology is not currently standardized. 5 The American Diabetes Association insulin pump standards of care emphasize the importance of skilled, consistent providers to care for the patients who use diabetes technologies to manage their diabetes. 5
In 2006, the Diabetes Technology Clinic (DTC) at Mayo Clinic was founded in recognition of the need for a clinic focused on people with diabetes who use technology for effective disease management. The DTC care team includes physicians, nurse practitioners, registered nurse certified diabetes educators (CDEs), dietitians and clinic support staff. To accommodate the expected increase in patients requiring diabetes technology-focused care, the DTC partnered with a health systems engineer from Mayo Clinic’s Management Engineering and Internal Consulting team to redesign the DTC.
Methods
Benchmarking and Team Assembly
National benchmarking was conducted to identify best practices to serve diabetes patients who use technology. 4 Following the benchmarking findings, the DTC assembled a multidisciplinary team to identify opportunities to improve the DTC. The Mayo Clinic Institutional Review Board gave exemption status to the study.
Process Mapping
The DTC patient visit process flow was mapped through direct observation and care team interviews. The process maps begin with scheduling the patient visit and end with patient dismissal.
Provider Interviews
DTC and referring providers were interviewed by the health systems engineer and the DTC nurse practitioner. The goal of these interviews was to elicit feedback on the current DTC processes and identify themes for improving the DTC for patients, the care team, and referring providers.
Patient Experience
DTC patients were surveyed to learn about the patient experience and how to improve the care provided. According to Browne et al, 6 patient experience data “can reveal system problems . . . that have major quality and efficiency implications.” The survey was designed with input from the Mayo Clinic’s survey research center, to identify DTC patient satisfaction elements most closely associated with overall patient experience and likelihood to recommend the clinic to other patients. The paper survey was mailed to 349 patients who had visited the DTC within the past year.
Results
Process Mapping
Evaluation of the current-state process identified several standardization and flow issues. The first issue was that processes varied by provider. Opportunity existed to standardize these processes to allow predictability for patients, care team members, and referring providers. The second issue was that device download was a process constraint. Educating patients to download at home, as well as streamlining download at the clinic could eliminate the delay of report readiness for provider review in advance of meeting with the patient.
Provider Interviews
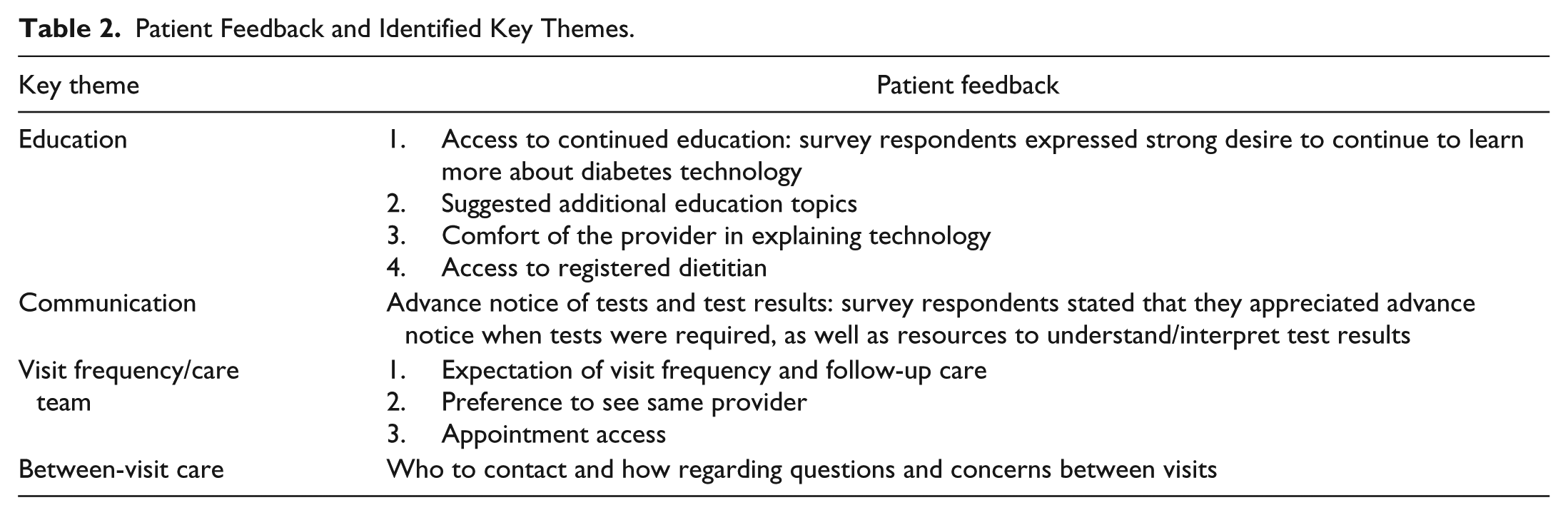
Interviews with representatives of the DTC care team and referring providers identified several central themes for improvement (Table 1). The providers shared opportunities to improve the clinic flow from the point of ordering services and scheduling patient appointments to after-visit follow-up. Communication with the referring provider regarding ongoing care and follow-up with the patient was also identified as an element to improve care for DTC patients. The team used this feedback to identify, test, and implement clinic improvements.
Provider Feedback and Identified Key Themes.
Patient Experience
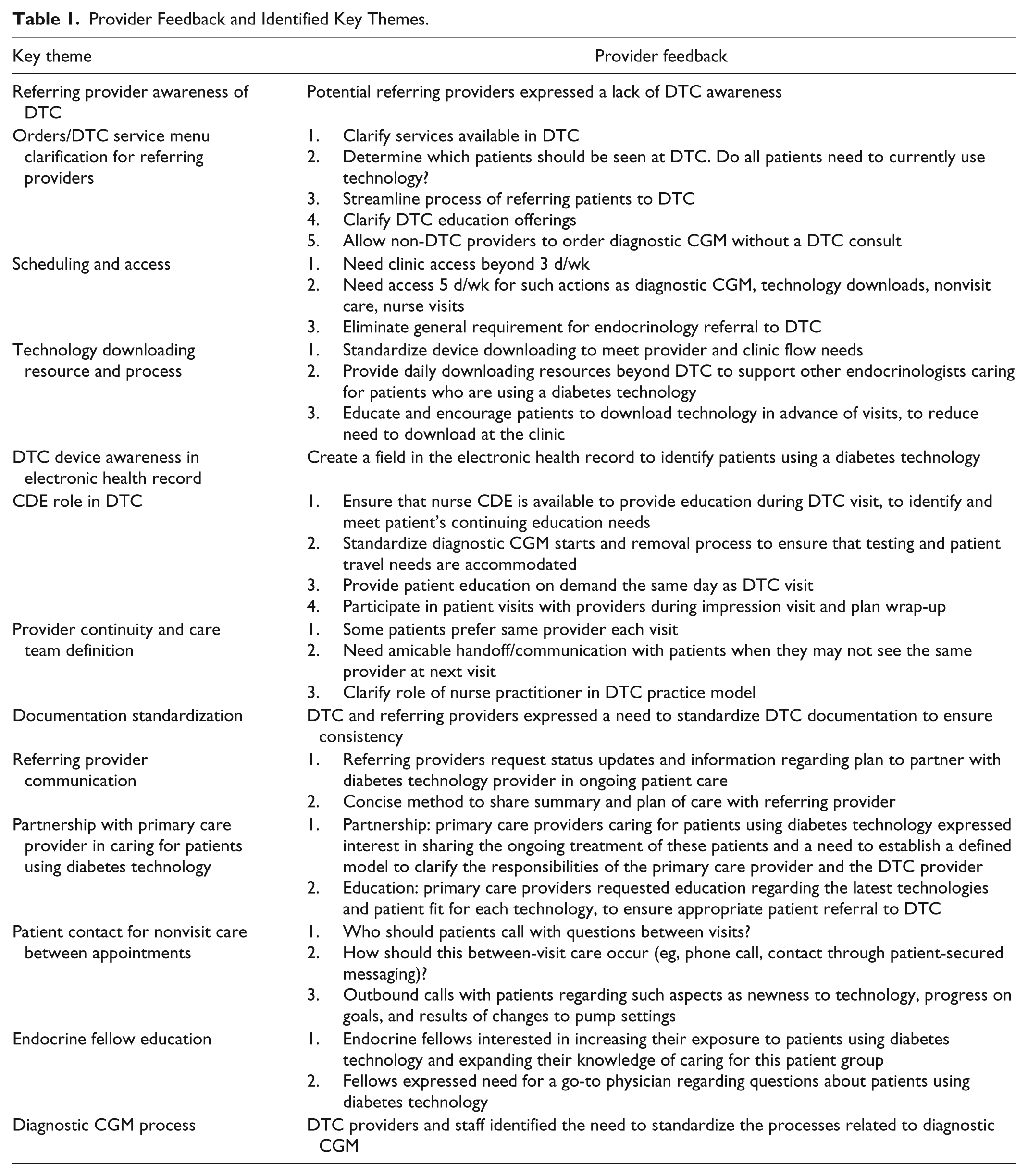
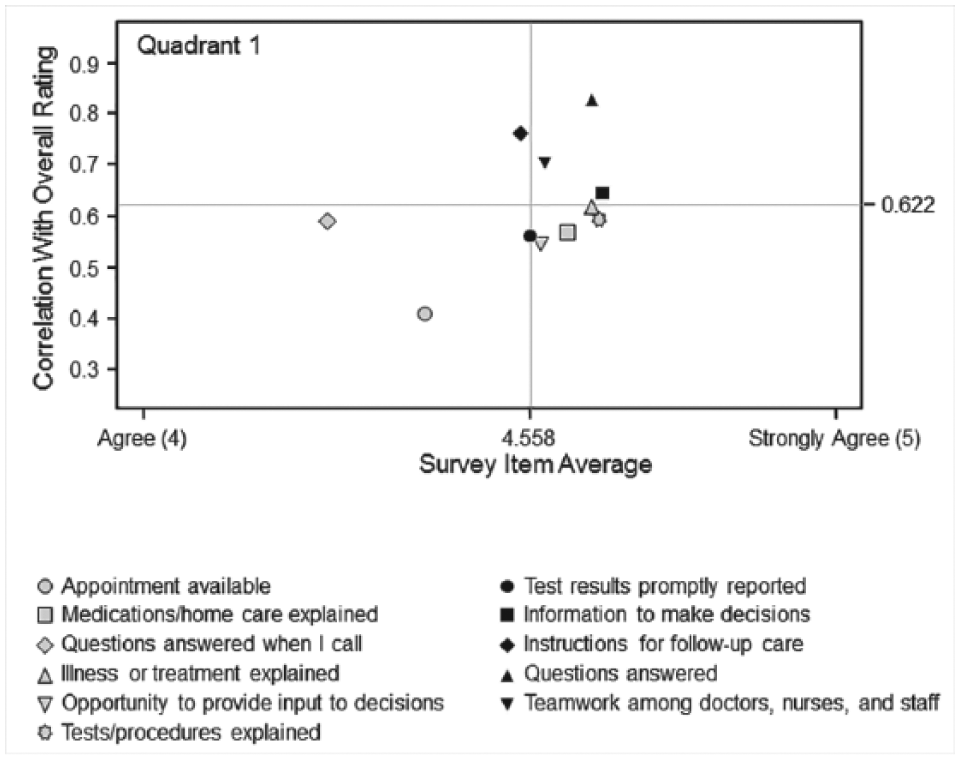
The response rate for the patient satisfaction survey was 49.6%. Patient and family feedback was essential to ensure that the DTC met the needs of its patients. The element identified by respondents as most closely associated with overall experience was that patients were provided instructions for follow-up care (Figure 1). The elements most associated with their likelihood to recommend the DTC to other patients were that patient questions were answered when they contacted the DTC between appointments and that they were provided instructions for follow-up care (Figure 2).
Associations with rating for overall experience. Graph identifies which survey items are most associated with the rating. The item in quadrant 1—instructions for follow-up care—has lower-than-average satisfaction levels. Items having higher-than-average correlation with the survey item are listed below the y-axis.
Associations with likelihood to recommend. Graph identifies which survey items are most associated with overall rating. Items in quadrant 1—questions answered when I call and instructions for follow-up care—have lower-than-average satisfaction levels. Items having higher-than-average correlation with the survey item are listed below the y-axis.
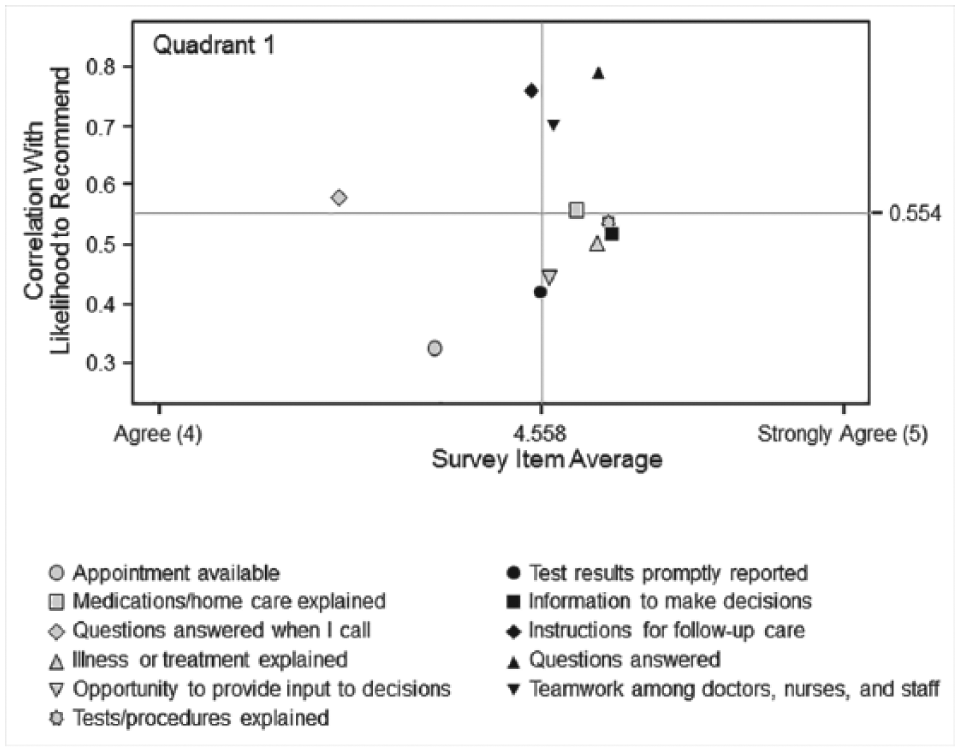
The project team carefully reviewed the comments provided by patients and patient families (Table 2). Patients expressed interest in continuing to learn strategies to use their technology to best manage their diabetes. Education was sufficient when patients were new to the technology, but they wanted continued learning from experts. Patients also suggested additional education topics related to incorporating technology use with their lifestyle, as well as the latest developments in diabetes technology.
Patient Feedback and Identified Key Themes.
Patients shared that they wanted to understand the expectations related to the necessary frequency of face-to-face visits with a DTC provider, and they expected access to appointments that met their needs. The survey responses indicated patients require consistency and desire to see the same provider each visit. They expect to leave a visit with a clear understanding of next steps, the expectations for follow-up care, and whom to contact with questions between visits.
Interventions: Acting on the Feedback
The project team synthesized the learning from benchmarking, process flows, and provider and patient feedback to identify necessary changes to improve DTC processes.
Awareness
Several interventions were implemented to improve awareness of the DTC and its services available. DTC providers conducted referring provider presentations about current diabetes technologies and research, determining patient fit for technology and diagnostic CGM. The DTC published clinic overview articles in provider newsletters, and developed a DTC overview YouTube video (https://www.youtube.com/watch?v=DP6MaaSk__Y). A brochure was designed that addressed commonly asked questions, current diabetes technologies, care team members, clinic visit expectations, and contact information. Creating awareness of the DTC was an essential first step to ensuring that patients and providers use the expertise available within the DTC.
Access
The team next addressed DTC access improvement opportunities. This included clarifying that the clinic cares for patients currently using or interested in using diabetes technology and that consult and education appointments could be scheduled without a referral. Diagnostic CGM with expert interpretation is available without a DTC consult. DTC appointment access was expanded from 3 days to 5 days per week with 2 additional physicians and 1 additional nurse practitioner, which resulted in improved appointment availability.
Clinic Processes
Several clinic improvements were implemented to improve patient flow (Figure 3). The patient intake process was modified to document diabetes technology information in the electronic health record. The nurse CDE completes the diabetes technology device downloads and the downloading process was standardized to ensure necessary reports were available during the patient visit. The insulin pump reports include 30 days of glucose values, and the reports are available electronically during the patient visit. Printed copies of the reports are provided based on provider and patient preference. The IT team maintains required download equipment. The nurse CDEs receive training from the software vendors, and the download procedures are documented and available for staff reference. Patient education was developed to teach patients how to download their insulin pump at home, with the goal of reducing the need to download at the clinic. The patient education material emphasized the importance of uploading their device at home between visits and was designed to accommodate any device selected by the patient by including the download instructions for multiple software options to accommodate patient device preference.
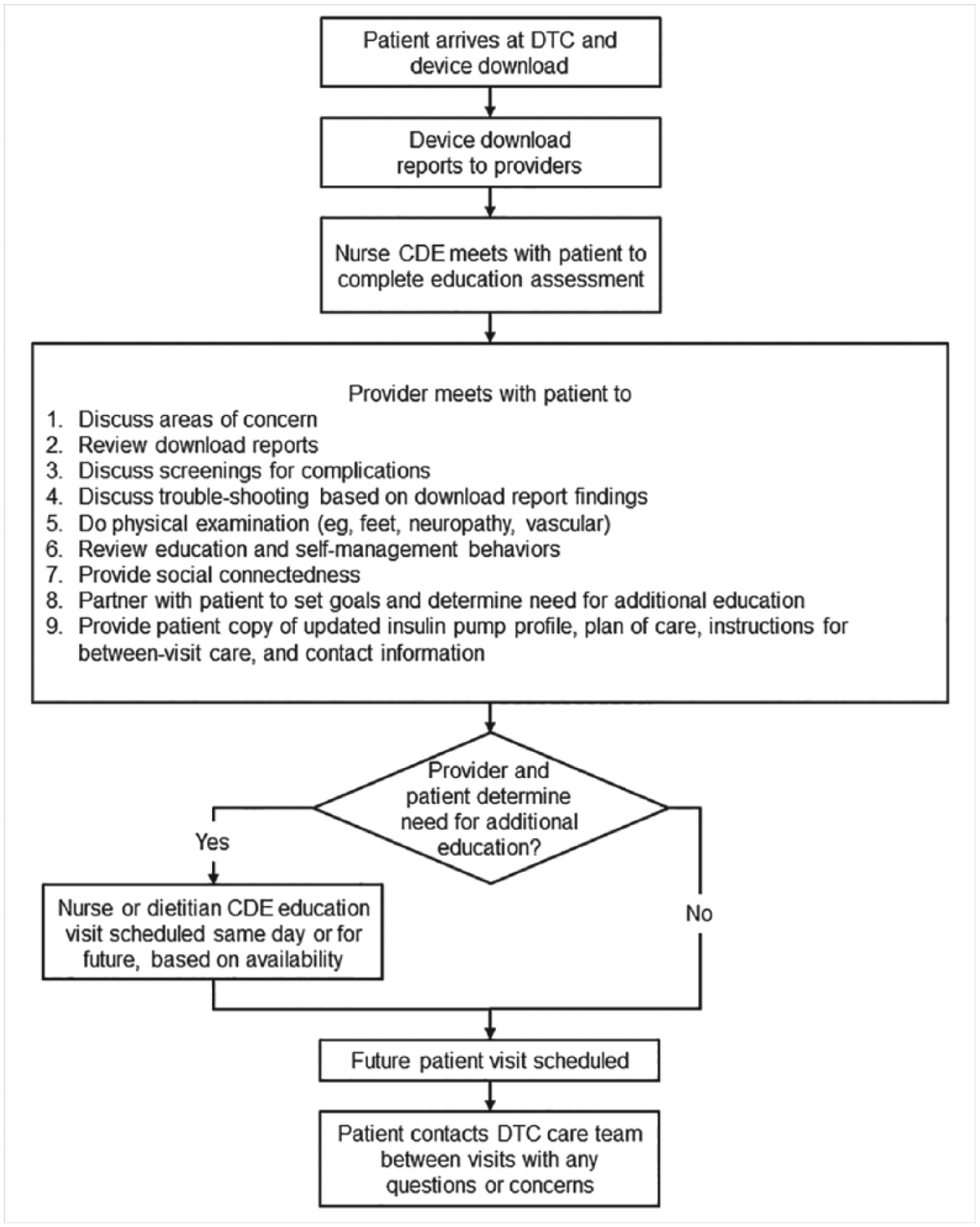
DTC visit flow.
To address patient and provider requests for ongoing patient education, new patient visits begin with a nurse CDE education assessment. The assessment results are shared with the provider and patient to determine education needs. Nurse and dietician CDE resources are available for patient education as determined by the provider and the patient. New educational materials were developed based on topics requested by patients.
Consistency
Patients and providers expressed a preference for provider visit consistency, so the DTC care team worked to ensure that established patients are scheduled with nurse practitioners to provide continuity. Exceptions are based on patient complexity, but the goal is to provide consistency when possible. The DTC has developed materials to support patient awareness of the team. A DTC brochure explains the care team, and team photos in all examination rooms facilitate conversations regarding the role of each member of the team. Physicians also introduce the nurse practitioner who will see the patient at the next appointment to provide a warm handoff.
After-Visit Follow-up
Patient and referring provider feedback included the need for clear understanding of the visit outcomes and next steps. Templates were created to ensure consistent visit and plan of care documentation in the electronic health record. Patients can access the information through the clinic’s patient online services; providers can view it through the provider portal. DTC and referring providers confer regarding ongoing plans to care for patients. The DTC care team partnered with the medical center’s primary care practice to develop a model of caring for primary care patients currently using or interested in using diabetes technologies.
Between-Visit Care
To address the patient need for standardized between-visit care, the DTC created a clinic brochure designed to address common patient questions and provide contact information. The care team reviews this information with patients to explain how to contact the DTC providers between visits. Materials were developed to educate patients on how to download their device at home between visits, as needed in support of care between visits. Patients calling after DTC hours are connected with the endocrine fellow.
Diagnostic CGM Processes
In response to provider feedback, the DTC team revised and standardized several diagnostic CGM processes (Figure 4). The DTC provider of the day ensures daily CGM interpretation using a standard documentation template and tag in the electronic health record. The DTC also implemented a remote return process to allow patients to wear the CGM for the required minimum time.
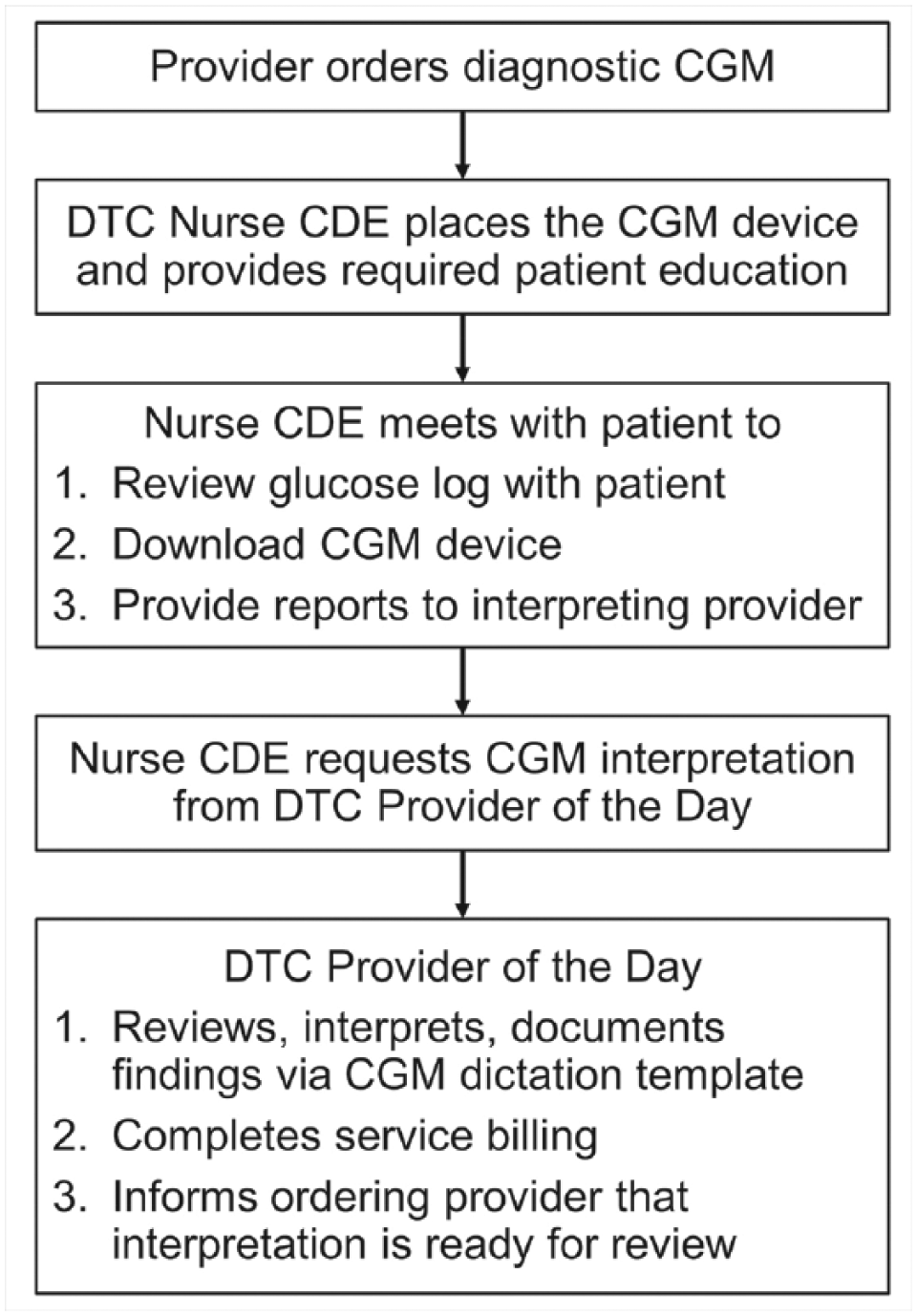
DTC diagnostic continuous glucose monitor process flow. Flow of the diagnostic CGM process.
Provider Training
The Endocrine Fellowship Program provided feedback to improve training opportunities within the DTC to teach future diabetes technology experts. An annual workshop on diabetes technology was designed for the fellows to meet this identified learning need. Endocrine fellows now see DTC patients to enhance the fellows’ diabetic technology training. The fellows also have access to the DTC provider of the day for any diabetes-technology-related question.
Discussion
Literature is limited about the needs of patients using diabetes technology, as well as the clinics and providers focused on caring for patients using diabetes technology. The needs of patients using diabetes technology are distinctive and require individualized care. Feedback from patients and providers, best practice benchmarking, and current-state process analysis resulted in a substantial redesign of the DTC practice, with the goal of better meeting the needs of patients and providers.
A limitation of this work is the lack of a follow-up patient satisfaction survey and provider interviews to determine the effect of the clinic redesign. The team also identified several improvement opportunities that have not yet been addressed: (1) CDE participation in visit care plan discussion, (2) outbound patient calls to determine goal progress and the results of pump setting changes, and (3) improved testing and results communication. The DTC discussed in this article is one example, and there is an opportunity to investigate the scalability of diabetes technology clinics for practices of all sizes.
The diabetes technology practice is a continually evolving and complex system for patients and those caring for them. Use of diabetes technologies involves a blending of patient involvement, an afferent arm with use of an insulin pump, an efferent arm with the use of continuous glucose monitor, or any combination of these. Individualized care will continue to be an important component of future use of diabetes technology. New diabetes therapeutic technologies are being tested by industry and by consortia funded by the National Institutes of Health. Current providers need to incorporate new competencies, and fellowship programs need to increase educational activity in this niche practice. Patients need more awareness, and technology use needs to be expanded for appropriate populations, such as patients with new-onset type 1 diabetes and after total pancreatectomy. They also need access to skilled, consistent care tailored to meet their distinctive needs. Continued care using both the multidisciplinary team and between-visit connected care is central to these efforts. Much work lies ahead for diabetes technology programs in the coming years.
Footnotes
Abbreviations
CDE, certified diabetes educator; CGM, continuous glucose monitoring; DTC, Diabetes Technology Clinic; IT, information technology.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: AMC was supported by the Department of Medicine, Mayo Clinic, Rochester, MN. PS was supported by the Division of Endocrinology, Mayo Clinic, Rochester, MN. YCK is supported by National Institutes of Health grant DK85516.