
Abstract
Fear of hypoglycemia is a major concern for many patients with type 1 diabetes and affects patient decisions for use of an artificial pancreas system. We propose an alternative way for prevention of hypoglycemia by issuing predictive hypoglycemia alarms and encouraging patients to consume carbohydrates in a timely manner. The algorithm has been tested on 6 subjects (3 males and 3 females, age 24.2 ± 4.5 years, weight 79.2 ± 16.2 kg, height 172.7 ± 9.4 cm, HbA1C 7.3 ± 0.48%, duration of diabetes 209.2 ± 87.9 months) over 3-day closed-loop clinical experiments as part of a multivariable artificial pancreas control system. Over 6 three-day clinical experiments, there were only 5 real hypoglycemia episodes, of which only 1 hypoglycemia episode occurred due to being missed by the proposed algorithm. The average hypoglycemia alarms per day and per subject was 3. Average glucose value when the first alarms were triggered was recorded to be 117 ± 30.6 mg/dl. Average carbohydrate consumption per alarm was 14 ± 7.8 grams. Our results have shown that most low glucose concentrations can be predicted in advance and the glucose levels can be raised back to the desired levels by consuming an appropriate amount of carbohydrate. The proposed algorithm is able to prevent most hypoglycemic events by suggesting appropriate levels of carbohydrate consumption before the actual occurrence of hypoglycemia.
People with type 1 diabetes (T1D) may experience hypoglycemia (blood glucose concentration [BGC] < 70 mg/dl) episodes that may be caused by insulin doses that are too large in relation to the BGC, reduced food intake, extensive physical activity, or slow absorption of currently available “fast-acting” insulins. 1 Fear of hypoglycemia is a major concern for many patients and affects patient decisions for use of an artificial pancreas (AP) system. Various strategies have been proposed for predicting BGC to be implemented in an AP system for prevention of hypoglycemia.2-16
Most of the developed AP systems are based on subcutaneous glucose measurement and subcutaneous insulin infusion. 17 Even though studies have shown that some hypoglycemia episodes can be prevented by suspension of insulin infusion,2,5 insulin as the only manipulated variable in an AP system may not be sufficient to prevent all hypoglycemia episodes. Glucagon has been used as the second control action to prevent hypoglycemia.18-25 Glucagon increases glucose by stimulating adenylate cyclase to produce increased cyclic AMP, promoting hepatic glycogenolysis and gluconeogenesis. This antihypoglycemic effect requires preexisting liver glycogen stores. 26 When hypoglycemia occurs, the predicted insulin infusion is suspended and glucagon is infused to elevate BGC. Although glucagon works well to prevent low glucose concentration, there have been occasions where administration of only glucagon was not sufficient to fully prevent hypoglycemia in almost all reported studies and additional rescue carbohydrates (CHO) were needed. Glucagon is more difficult to work with than insulin due to its inability to remain stable in solution, though there has been research into creating improved glucagon formulations.27,28
An alternative is to use CHO to prevent hypoglycemia. Several factors influence glycemic response to food, including food form, degree of cooking and processing (particle size, degree of hydration), ripeness, macronutrient composition, fiber, antinutrients (eg, amylase inhibitors), amount of food or CHO consumed at 1 time, type of sugar (glucose, fructose, sucrose, lactose) or starch (amylose, amylopectin, resistant starch), meal frequency, rate of ingestion, and physiologic effects.29-32 Any of these factors, alone or in combination, will impact the overall rate of digestion and absorption and subsequent glycemic response. When hypoglycemia is detected, providing a small amount of CHO regardless of source or type can help. 31 Depending on the level of blood glucose detected and the rate blood glucose is decreasing, providing a rapidly absorbable form of CHO (dextrose tablets or gels, juice, etc) can quickly increase blood glucose levels. Addition of complex CHO can prevent the hypoglycemia episode from recurring.30,31 Administration of glucagon can help to prevent hypoglycemia if the patient has sufficient glycogen stores, but, if not, then fast-acting CHO should be provided if the patient is responsive.
We propose a new algorithm for real-time suggestion of CHO based on early detection of hypoglycemia potential for prevention of low BGC in patients with T1D. We have already reported a multivariable hypoglycemia early alarm (HEA) system that was able to predict most hypoglycemia episodes 25-30 minutes in advance. 13 This HEA system is integrated with a new CHO suggestion algorithm. The proposed algorithm suggests specific amounts of CHO to be consumed for prevention of low BGC. The algorithm has been tested on 6 subjects in 3-day-long clinical experiments.
Participants and Methods
Study Participants
The experiments were performed at the University of Chicago (UOC) Clinical Research Center (CRC) over a 3-day period. Six subjects (3 male and 3 female, age 24.2 ± 4.5 years, weight 79.2 ± 16.2 kg, height 172.7 ± 9.4 cm, HbA1C 7.3 ± 0.48%, duration with diabetes 209.2 ± 87.9 months) participated in the study. Subjects were provided 2 continuous glucose monitoring (CGM) (Dexcom G4 PLATINUM) devices, a BodyMedia SenseWear armband, 33 and a Zephyr chestband. 34 The subjects had a CGM placed prior to the study, and the study MD had begun to remotely monitor subject blood glucose before the study began then continuously during the study. Continuous data collection from the subjects started on Day 1 and insulin delivery via AP algorithm continued for 60 hours. Data were collected and transmitted to a laptop computer every 5 minutes. Plasma glucose concentration was measured every 30 minutes using the YSI 2300 STAT (Yellow Springs Instrument, Yellow Springs, OH). All 3 days, subjects had 2 personalized exercise sessions (morning and afternoon), to include aerobic, resistance or interval exercises in the same sequence for all subjects according to the individual’s fitness level. Exercise intensity was calculated based on subjects’ exercise stress tests. According to the Karvonen formula, 35 the subjects’ target heart rate (HR) training zone was calculated. The formula uses maximum and resting HR with the desired training intensity to get a target HR (((maximal HR - resting HR) × 65 to 85% intensity) + resting HR). For interval training, moderate intensity is 60-70% of HR reserve and high intensity is 85-90% of HR reserve. Subjects were monitored for hypo- and hyperglycemia during this time and discharged from the CRC approximately 2 hours following disconnection from the algorithm. Daily dietary needs (8 meals and 2 snacks) and 2 nights sleeping accommodations were provided by the CRC. Participants received a 1d-cycle rotating menu each day for 3 days customized to individual food preferences. Prior to admission for the study, participants were interviewed by phone to plan the study diet. CHO intake was kept very similar to their usual intake. Daily calories were divided among breakfast (25%), lunch (30%), dinner (35%) and evening snack (10%). The caloric content and macronutrient composition of consumed meals, snacks and beverages were calculated using Food Processor SQL (version 10.15.41, ESHA Research, Salem, OR). Participants were not required to eat 100% of meals and were only allowed to eat food provided by the CRC Metabolic Kitchen. Any food that was not consumed was weighed back. Foods consumed (type and amount) and physical activity, were logged throughout the study period.
Methods
Glucose predictions are obtained by using a multivariable time-series models where glucose concentration is expressed as a function of past glucose concentration and physical activity signal readings and infused insulin amounts by using an ARMAX model structure: 13

where



where
Based on measured glucose values, 5 different phases are defined (Figure 1). For each phase, 3 different speeds of glucose decrease (S: slow, N: normal, F: fast) are defined as:


where
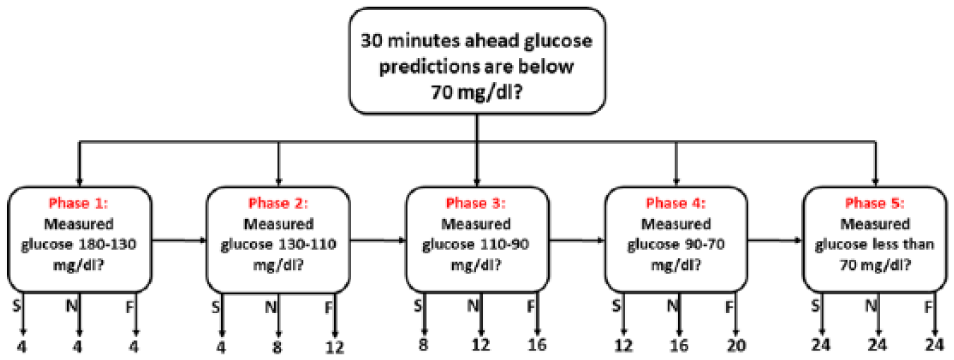
Hypoglycemia detection based CHO suggestion flowchart (values are shown in grams).
With every new measurement, 30-minutes-ahead glucose predictions are compared with 70 the mg/dl mild hypoglycemia threshold (80 mg/dl during exercise). If the predicted values are below the threshold, the last measured glucose value is used for determination of the phase interval. At the same time, the speed of glucose reduction is obtained using equations (5) and (6). Once the phase and the speed of reduction are calculated, specific amounts of CHO (Figure 1) are suggested to patients for consumption. Only 1 CHO suggestion is done in 1 phase (except phase 5) until glucose levels decreases to the next level.
Results
The proposed algorithm has been tested on 6 subjects (one experiment per subject) over 3-day-long closed-loop experiments. When hypoglycemia potential is detected, subjects were notified and the algorithm suggested some amounts of CHO to be consumed according to the flowchart in Figure 1. However, subjects were free to eat CHO amounts different than the suggested amount or not eat.
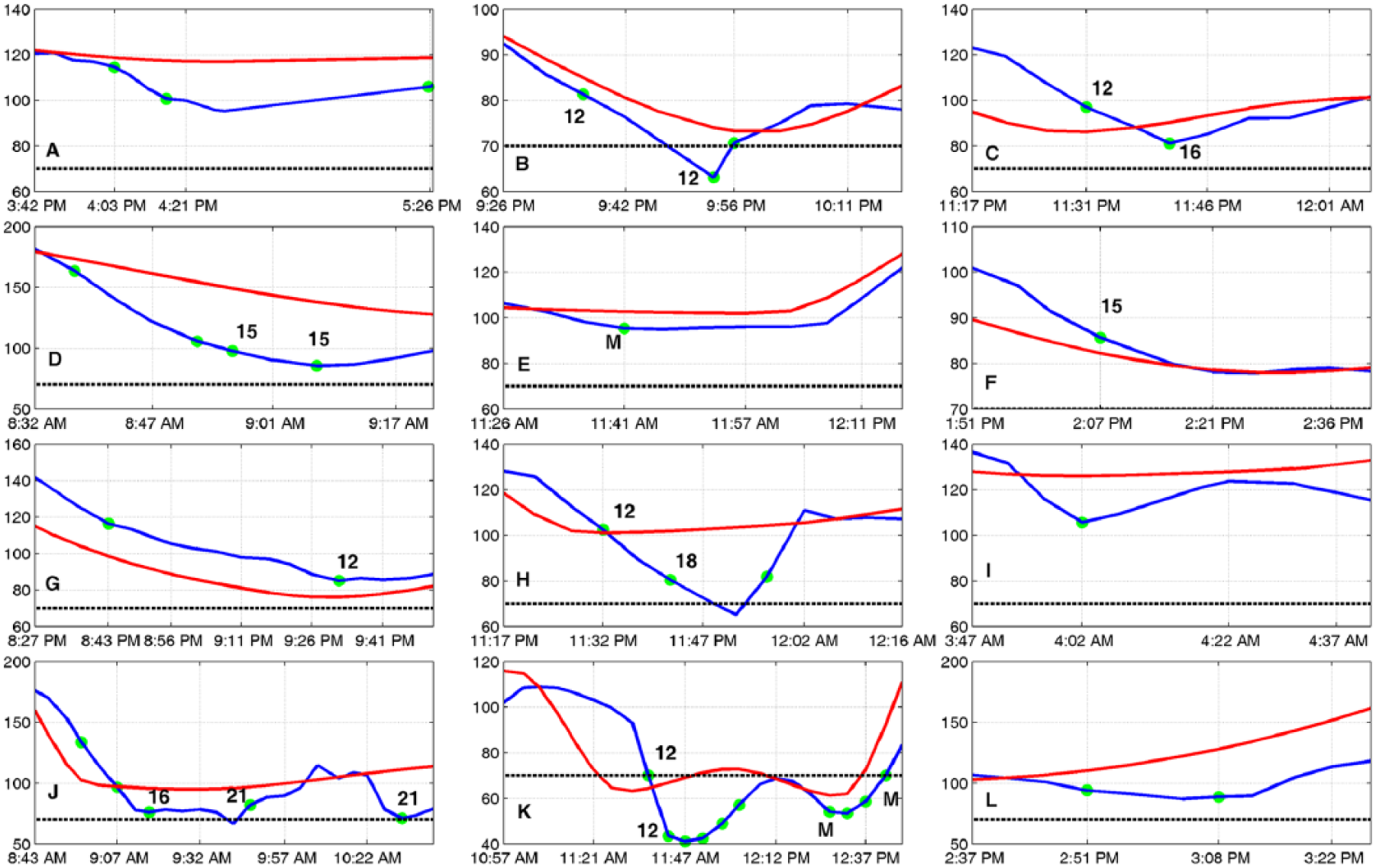
In the first experiment, hypoglycemia alarms were issued during 6 time periods throughout the 3-day experiment and CHO were suggested by the algorithm (Figure 2). Overall, 15 times (10.9 ± 8.9 gram, total 163 gram) different CHO amounts were taken. A mild hypoglycemia occurred on only 1 occasion. This might have been prevented if the subject had consumed the suggested CHO amount when the first alarm was issued (Figure 2B). Average glucose value was 132 ± 29.2 mg/dl when the first hypoglycemia alarms were issued.
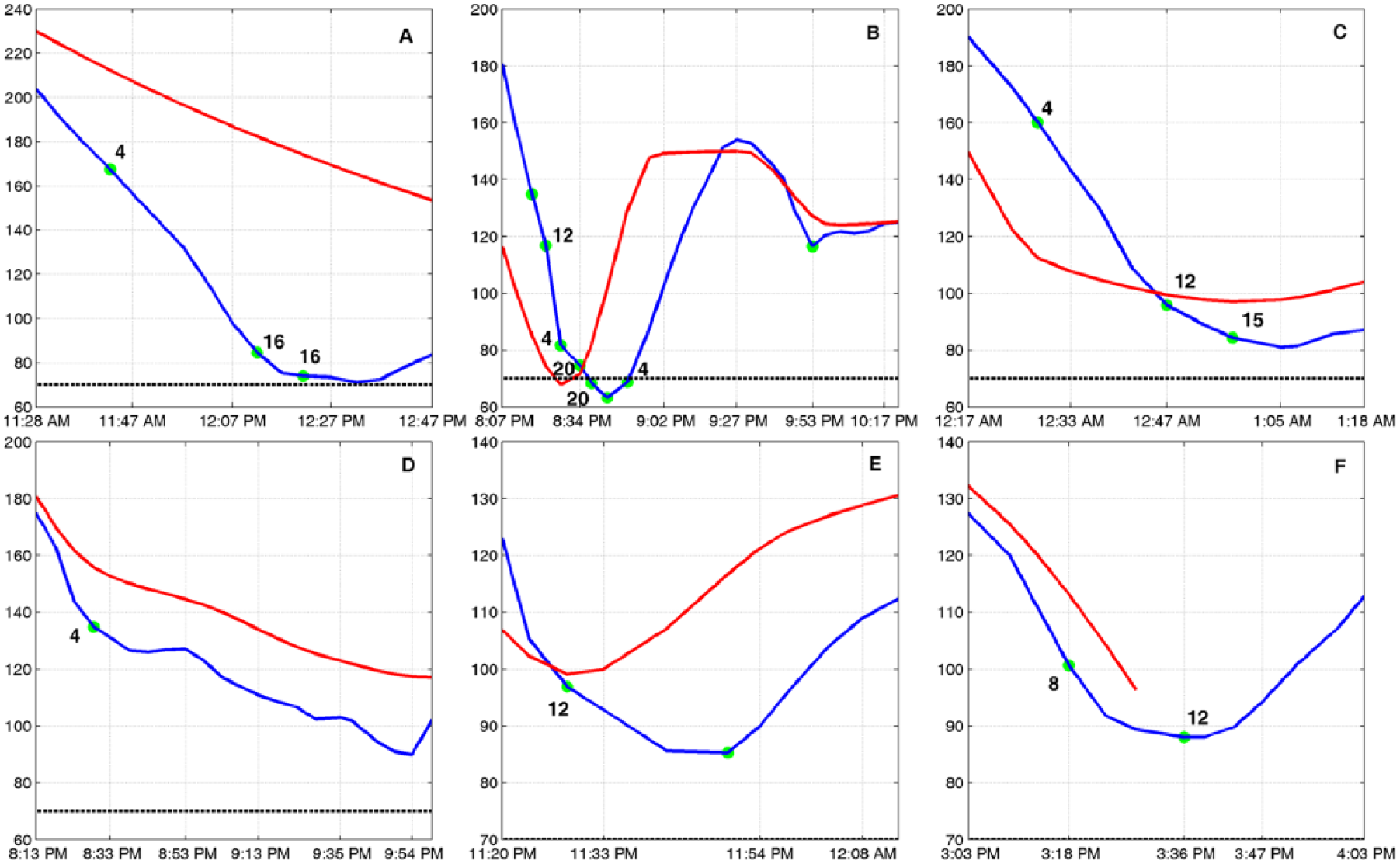
Results of experiment 1. Blue line: CGM; red line: interpolated YSI; dashed black line: mild hypoglycemia threshold; green circle: hypoglycemia alarms with their verified CHO amounts (M: regular meal).
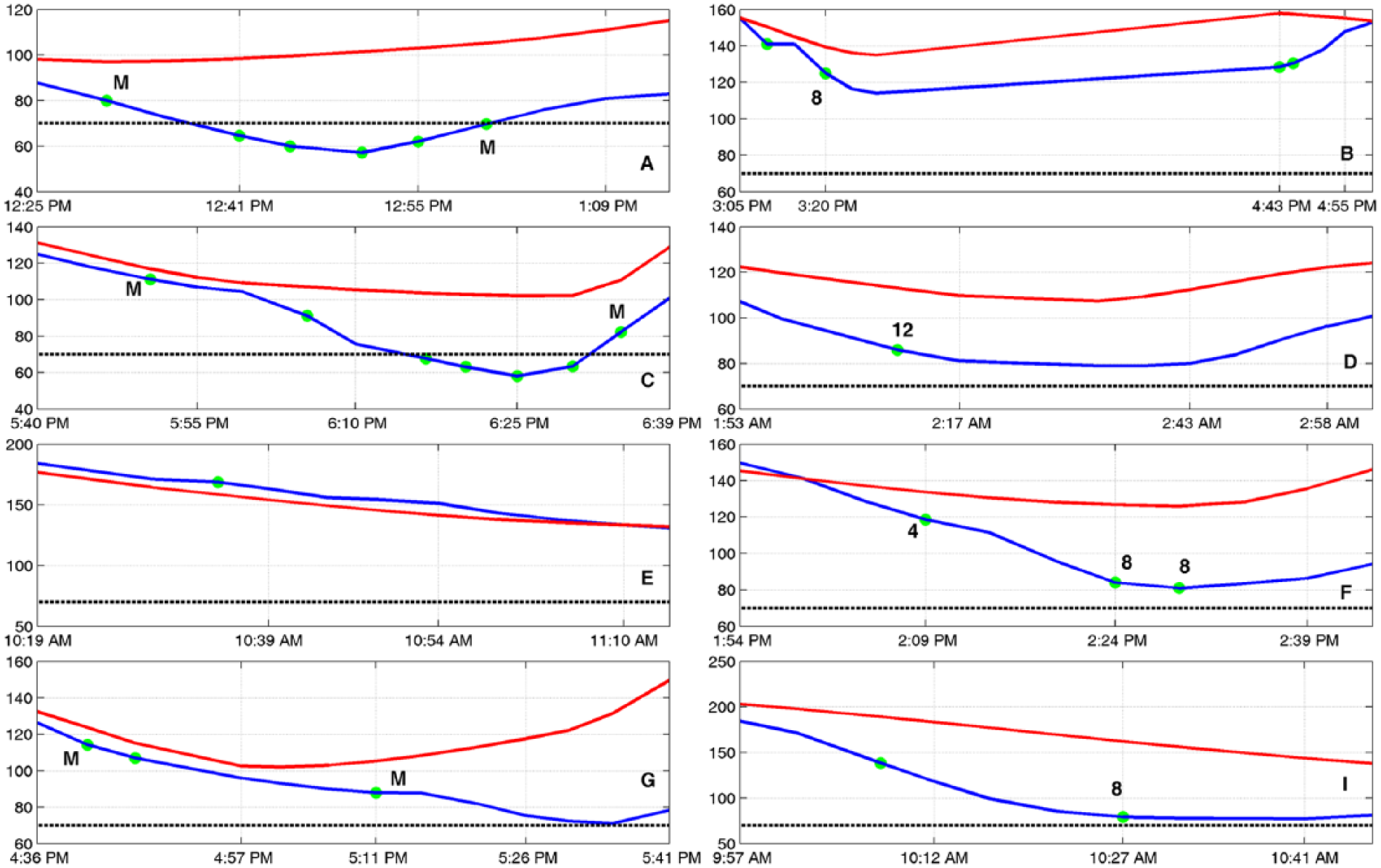
The second experiment had 4 potential hypoglycemic periods (Figure 3). CHO were taken 8 times (14 ± 17.8 gram, total 112 gram) during the 3-day experiment. The first hypoglycemia alarm was issued during the exercise session on the first day and administration of 8 grams of CHO was suggested. However, the actual response to the alarm was a CHO amount that was much more than the suggested amount. This was caused by an inaccurate finger-stick measurement during the exercise period which showed the glucose value to be 33 mg/dl. Later, this reading was found to be wrong when YSI values were obtained from laboratory. The next hypoglycemia alarms occurred close to lunch time (green circles without number), and the subject preferred not to consume the suggested CHO amounts and wait for lunch. During the later period (Figure 3C) there was a sharp decrease in CGM readings, due to disconnection from CGM sensor. In the last period, CHO amounts are suggested at higher glucose values because, the subject was in an exercise session. This is done automatically by the algorithm for prevention of exercise-induced hypoglycemia by suggesting CHO at an earlier stage by using exercise information from the Bodymedia Sensewear armband. Average glucose concentration was recorded to be 146 ± 19.7 mg/dl when a hypoglycemia alarm was triggered.
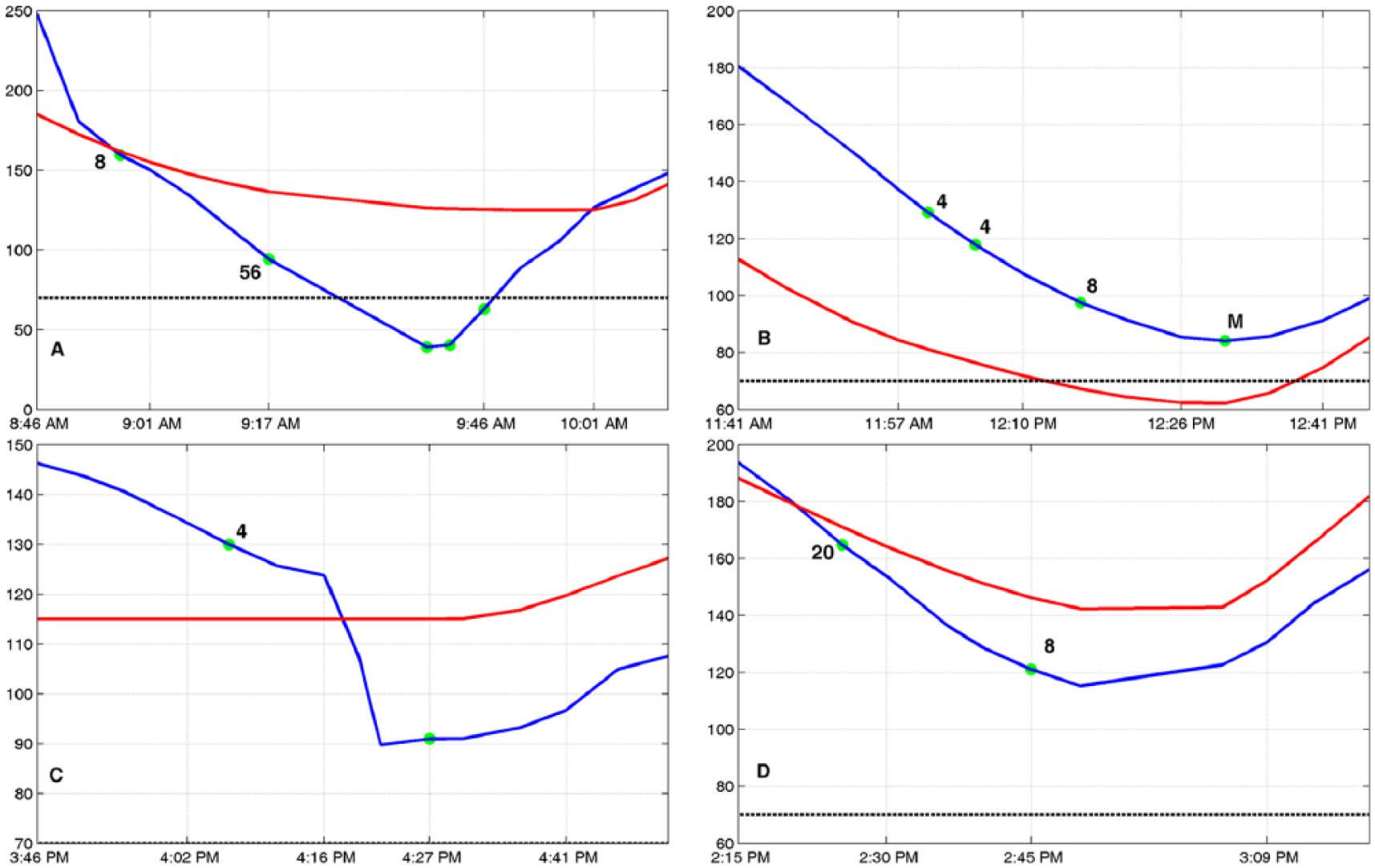
Results of experiment 2. Blue line: CGM; red line: interpolated YSI; dashed black line: mild hypoglycemia threshold; green circle: hypoglycemia alarms with their verified CHO amounts (M: regular meal).
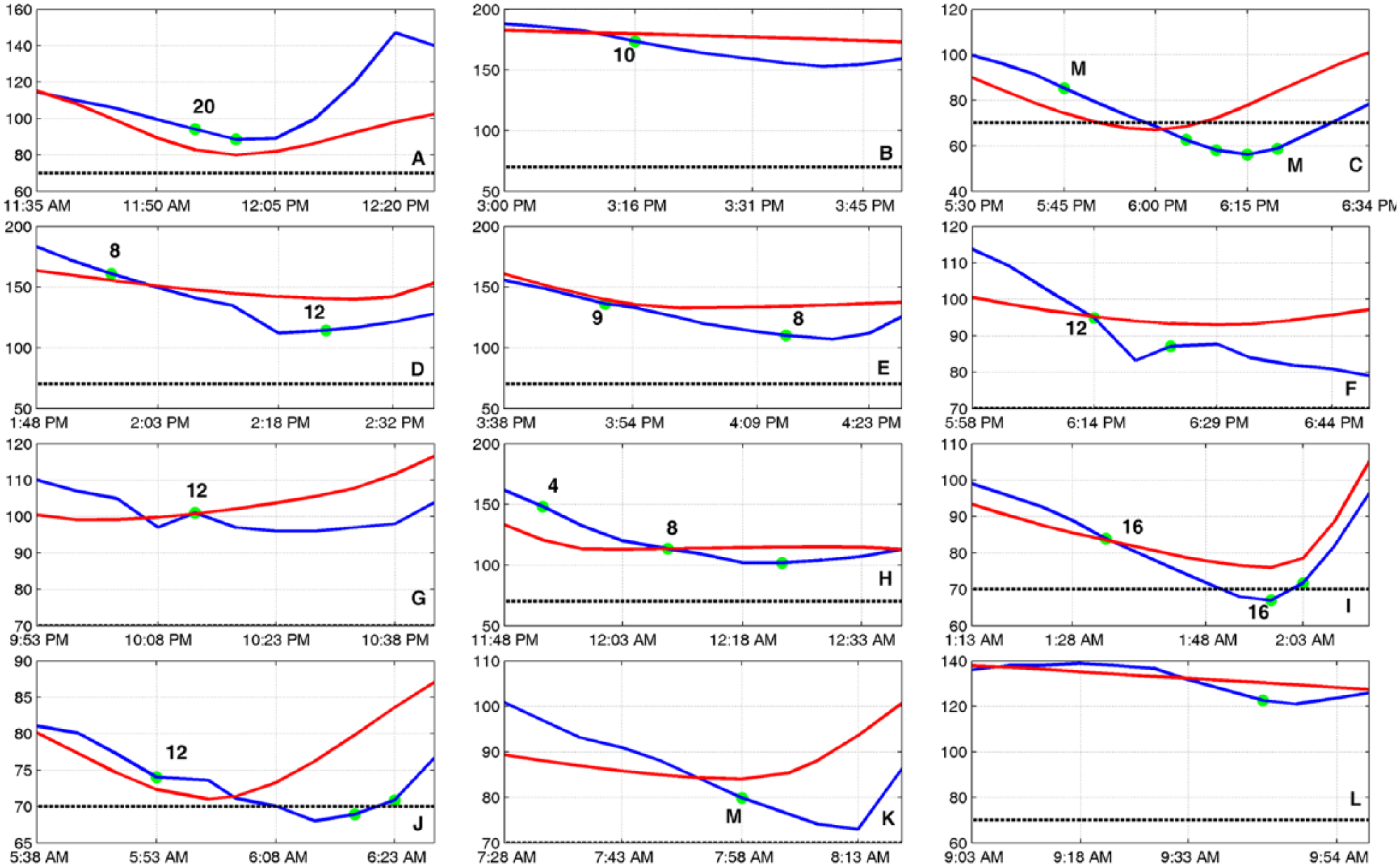
Overall, 18 times (19 ± 5.2 gram, total 345 gram) CHO were taken during 12 different time instances for experiment 3 (Figure 4). Since no limitation was made on the amount of suggested CHO amounts, subjects used their own preferences to modify the suggested amounts, which resulted in relatively higher amounts of consumed CHO in this experiment. Two of the hypoglycemia alarms overlapped with meal times and the subject preferred no additional CHO besides lunch. In all experiments, the alarms during the meal periods (green circles between 2 M) were ignored and no additional CHO were provided. There was only 1 true hypoglycemia (TH) (YSI < 70 mg/dl) episode that could not be prevented. One possible reason for this hypoglycemia might be sensor accuracy (Figure 4). Average glucose concentration was 116 ± 31.9 mg/dl at the time of the first hypoglycemia alarms.
Results of experiment 3. Blue line: CGM; red line: interpolated YSI; dashed black line: mild hypoglycemia threshold; green circle: hypoglycemia alarms with their verified CHO amounts (M: regular meal).
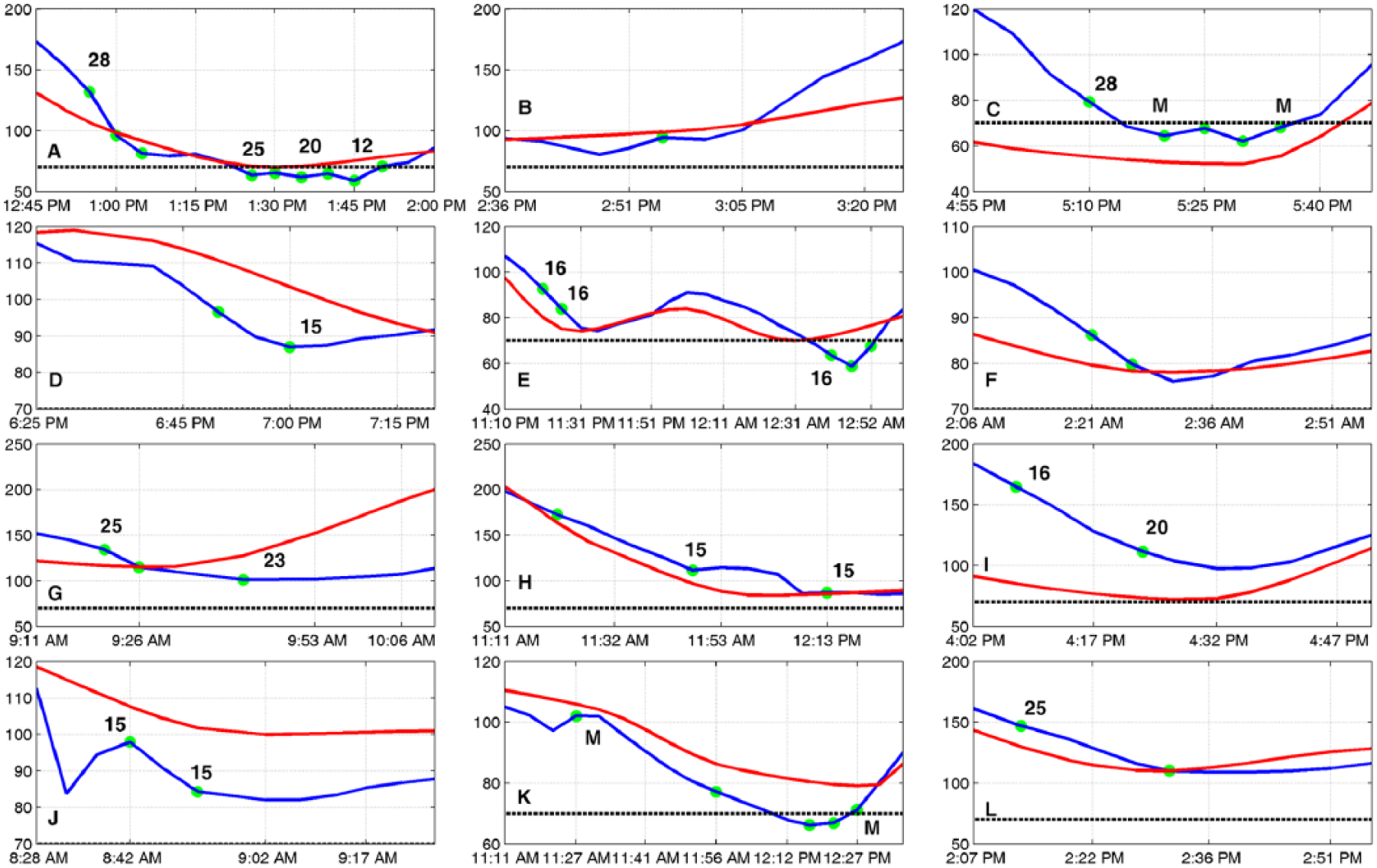
Experiment 4 had 12 different hypoglycemia alarm periods (Figure 5). During the 3 days of the experiment 15 CHO (14 ± 3.2 gram, total 221 gram) were consumed. There was only 1 case where the proposed algorithm was not able to predict hypoglycemia in advance (Figure 5K). This is most probably because of the sudden directional change in glucose readings at around 11:30
Results of experiment 4. Blue line: CGM; red line: interpolated YSI; dashed black line: mild hypoglycemia threshold; green circle: hypoglycemia alarms with their verified CHO amounts (M: regular meal).
There was no TH during experiment 5 (Figure 6). At 6 different times, the algorithm gave a hypoglycemia alarm where 3 of these times overlapped with meal times and no additional CHO were provided. Overall, 6 times CHO (8 ± 2.3 gram, total 56 gram) were consumed. Average glucose concentration at the time of the first hypoglycemia alarms was observed to be 119 ± 29.4 mg/dl.
Results of experiment 5. Blue line: CGM; red line: interpolated YSI; dashed black line: mild hypoglycemia threshold; green circle: hypoglycemia alarms with their verified CHO amounts (M: regular meal).
Figure 7 shows the results from the last experiment where hypoglycemia alarm was triggered in 12 different periods and most of them were treated with CHO. Thirteen times suggested CHO amounts (11 ± 4.2 gram, total 147 gram) were consumed by the subject. No TH was observed and average glucose at the time of the first alarms was measured to be 112 ± 34.4 mg/dl.
Results of experiment 6. Blue line: CGM; red line: interpolated YSI; dashed black line: mild hypoglycemia threshold; green circle: hypoglycemia alarms with their verified CHO amounts (M: regular meal).
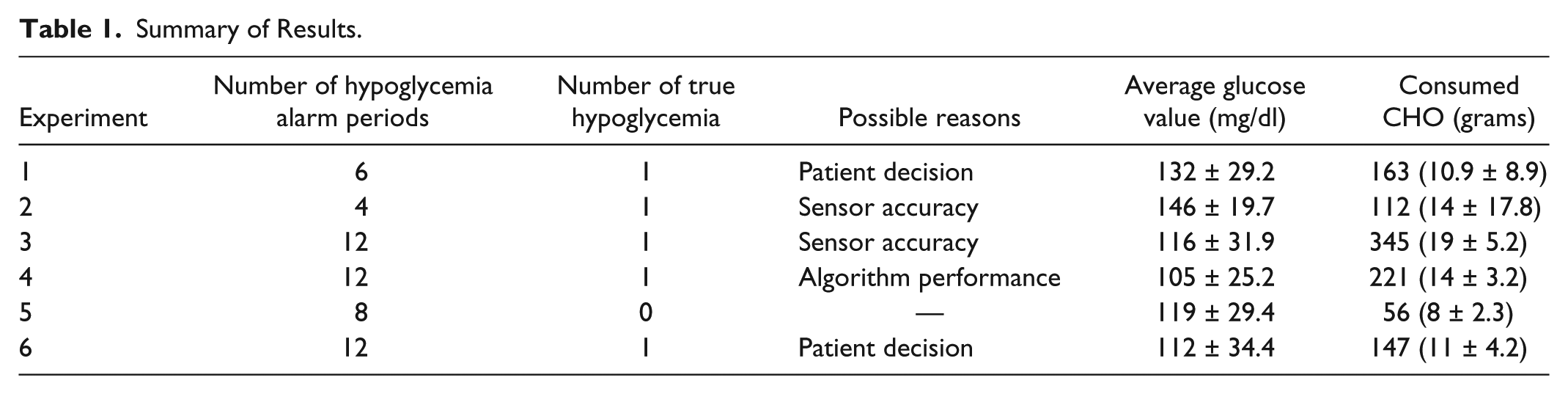
Table 1 summarizes all the results where overall 5 TH was seen during all 6 experiments. There was only 1 hypoglycemia per experiment. Out of 5 TH, only 1 is considered to be missed by the algorithm as the rest are due to either patients’ decision or sensor inaccuracy.
Summary of Results.
Discussion of Results
In this study, we propose an alternative for prevention of hypoglycemia by issuing predictive hypoglycemia alarms and encouraging the patients to consume CHO in a timely manner. We have already developed a multivariable AP control system for patients with T1D. 36 The developed system has several modules such as an adaptive controller, 1 an HEA system, 13 a meal detection and bolus calculator,37,38 a physical activity classifier, 34 and a fault detection module. 39 The ultimate goal is to add other modules to the multivariable AP system to provide a fully automated and safe environment for people with T1D. Hypoglycemia is one of the main concerns of people with T1D for using an automated system and the proposed method provides a simple and effective intervention based on 30-minutes-ahead prediction of hypoglycemia.
Our results have shown that most low glucose concentrations can be predicted in advance and the glucose levels can be raised back to the desired levels by consuming appropriate amount of CHO. There were only few cases where TH occurred. However, some of these hypoglycemia episodes might be due to sensor accuracy or subject CHO consumption preferences. The suboptimal performance of CGM devices has been discussed in many studies.40-43 However, this problem is being addressed by device manufacturers, and the availability of CGM systems with higher accuracy and reliability are expected in the near future.
The CHO amounts that are shown in Figure 1 are defined based on generalized clinical experiences. One may modify the suggested amounts in the flowchart for a specific subject offline before the algorithm is used in an automated mode. This way, the suggested amount will be more subject-specific which would prevent low CHO suggestions that may not prevent the occurrence of hypoglycemia and high CHO suggestions that may induce hyperglycemia.
Although, the proposed method was shown to be able to prevent most of low glucose values, it still has some limitations. For example, patients may not be aware of a given alarm during sleep. Hypoglycemia during sleep can be prevented by setting the controller to be more conservative 36 or shutting down the insulin pump. 2 Our multivariable AP system already has both rules as a safety module to prevent hypoglycemia during sleep when patients are not aware of low BGC and are not responding to an alarm given by the algorithm.
Conclusions
The proposed algorithm is able to prevent most hypoglycemic events by issuing predictive hypoglycemia warnings and suggesting appropriate levels of CHO consumption before the actual occurrence of hypoglycemia. The CHO amounts that are suggested can be personalized based on subject-specific preferences and metabolic information to customize the CHO to users offline before the algorithm is used for prevention of large deviations in glucose levels.
Footnotes
Abbreviations
AP, artificial pancreas; BGC, blood glucose concentration; CGM, continuous glucose monitoring; CHO, carbohydrates; CRC, Clinical Research Center; HEA, hypoglycemia early alarm; HR, heart rate; TH, true hypoglycemia; T1D, type 1 diabetes; UOC, University of Chicago; YSI, Yellow Springs Instrument.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Institutes of Health under grant NIH/NIDDK 1DP3 DK101077 and Juvenile Diabetes Research Foundation under grant 3-PDF-2016-175-A-N