
Abstract
Background:
Continuous glucose monitoring (CGM) is today provided by various techniques. This study aims to compare two different CGM-systems: the FreeStyle Libre subcutaneous continuous glucose monitoring system (SC-CGM) and the Eirus intravascular microdialysis continuous glucose monitoring system (MD-CGM) in patients undergoing cardiac surgery.
Methods:
A total of 26 patients were equipped with both the SC-CGM and the MD-CGM systems. The SC-CGM system was placed subcutaneously in the left upper-arm and the MD-CGM system was placed in the superior vena cava. Reference blood glucose values were obtained by analyzing arterial blood in a blood gas analyzer. Reference glucose values were then paired with glucose values from both CGM-systems and analyzed for accuracy.
Results:
In all, 514 paired MD-CGM/arterial blood gas glucose values and 578 paired SC-CGM/arterial blood gas glucose values were obtained. Mean difference (SD) for the MD-CGM system was 0.9 (15.1) mg/dl and for the SC-CGM system −43.4 (20) mg/dl. ISO criteria (ISO15197:2013) were not met by either CGM system. In the Clarke error grid, all paired samples were within the zones AB for the MD-CGM system, and 94% in zone A. For the SC-CGM system, 99.1% of the paired samples were within zones AB, and 18.9% in zone A. Both the MD-CGM and the SC-CGM systems were reliable and used without complications.
Conclusions:
These results indicate that the Eirus intravascular microdialysis system monitors glucose continuously with superior accuracy compared to the FreeStyle Libre subcutaneous glucose monitoring system, which repeatedly measured a glucose value that was lower than the reference method.
Glycemic control (GC) in critically ill patients is an important aspect of the treatment conducted in intensive care units (ICUs) worldwide. Initially, primarily hyperglycemia was targeted after van den Berghe and colleagues demonstrated a substantial mortality benefit using a tight blood glucose target in their landmark study from 2001. 1 Subsequent research has since then expanded the concept of GC to not only target hyperglycemia, but also to minimize the incidence of hypoglycemia and glycemic variability, as these aspects also have been linked to increased mortality and morbidity.2-5
Glucose monitoring in the ICU have special demands requiring both speed and accuracy. The golden standard of blood glucose analysis is to measure plasma glucose by the hospital laboratory, which often utilizes a glucose oxidase method. However, this is generally too time-consuming in the ICU-setting, where blood glucose is mostly analyzed intermittently by either handheld point-of-care (POC) glucometers or blood gas analyzers. POC glucometers have repeatedly been found to lack in accuracy when used in critically ill patients.6,7 Blood glucose analysis by analyzing an arterial blood sample in a blood gas analyzer has been extensively assessed with demonstration of excellent accuracy and performance in the ICU 8 and is thus by many considered the standard method for blood glucose monitoring in these patients. 9 Today there are several commercially available systems that provide continuous glucose monitoring (CGM) in critically ill patients.10-12 CGM may be advantageous to intermittent analysis, as both hypo- and hyperglycemia with certainty are not missed. Furthermore, the use of CGM may also reduce nurse workload and save economic costs. 13
There are several different CGM systems in use today that employ various techniques, ranging from more invasive systems placed inside a vessel to less invasive subcutaneous systems. Subcutaneous CGM systems have been tested in several studies, of which most have demonstrated a good performance in critically ill patients,12,14,15 but the accuracy has also been found to be low and inadequate. 16 It may be argued that placing a glucose-monitoring sensor subcutaneously can be disadvantageous in some clinical scenarios that may occur in the ICU setting, such as hypoperfusion. A recent study investigated the association between impaired microcirculation and sensor accuracy in cardiac surgery patients, but could not demonstrate a connection. 17 In general, more invasive glucose-monitoring techniques tend to be more accurate. 18 Intravascular microdialysis is a method that has been shown to be useful and accurate for CGM in critically ill patients.19,20 The system utilizes a microdialysis membrane located on a catheter placed in a central vein, that also provides a central venous access.
This study aims to evaluate and compare the accuracy and reliability of 2 different CGM-systems: the Eirus intravascular microdialysis continuous glucose monitoring (MD-CGM) system and the FreeStyle Libre subcutaneous glucose monitoring (SC-CGM) system.
Material and Methods
Patients and Setting
In all, 26 patients undergoing cardiac surgery on cardiopulmonary bypass at the Karolinska University Hospital, Stockholm, Sweden, between October and December 2015 were included. Patients had to be >18 years of age and scheduled for elective cardiac surgery. Exclusion criteria were ongoing infection, a state of high risk for blood coagulation and unfit anatomy for safe insertion of a central venous catheter (CVC). All patients provided written consent for participation after having received oral and written information about the study. The study was approved by the Regional Ethics Committee of Stockholm.
CGM Systems
The Eirus intravascular microdialysis system (Maquet Critical Care, Solna, Sweden) consists of a microdialysis triple-lumen catheter (TLC) that is a standard CVC with an integrated microdialysis membrane located proximally to the infusion holes. The length of the catheter is 16 cm and the diameter 7Fr. The microdialysis membrane is placed in a central vein and perfused with sodium chloride, creating a dialysate fluid with the same glucose concentration as in the bloodstream. The catheter is connected to a sensor that continuously measures the glucose concentration of the dialysate fluid using the glucose oxidase method. The sensor is further connected to a monitor that displays the glucose concentration as a numerical value and a trend graph, with a time lag of 5 minutes (the time it takes to perfuse the system). An illustration of the microdialysis system is provided in Figure 1. The catheter is approved for use for up to 30 days. The microdialysis system needs to be calibrated every 8 hours by manually entering a reference glucose value into the monitor.
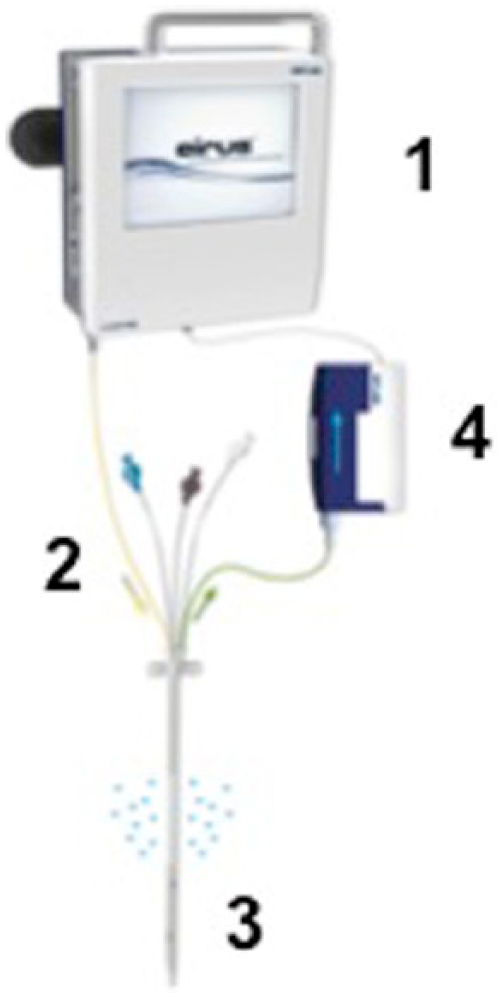
The Eirus intravascular microdialysis system, consisting of (1) the monitor, (2) the microdialysis catheter with (3) the microdialysis membrane at its distal end, and (4) the sensor that continuously analyzes the glucose concentration of the dialysate fluid.
The FreeStyle Libre (Abbott Diabetes Care Inc, Alameda, CA, USA) SC-CGM system consists of a small sensor (approximately 2 cm diameter) that is placed subcutaneously in the upper arm, also utilizing the glucose oxidase method for glucose analysis. A special sensor-reader is used to scan the sensor within a distance of 1-4 cm, to acquire knowledge of the blood glucose concentration. In addition, the sensor automatically analyzes the blood glucose concentration every 15 minutes and stores this information. The sensor needs to be scanned at least every 8 hours and is approved for use for 14 days. The system requires a 1-hour warm-up period after the sensor is inserted before blood glucose can be analyzed. The sensor is precalibrated by the manufacturer and recalibration is not possible. The sensor-reader may also be used as a POC glucometer, analyzing a capillary blood sample utilizing special test strips. An illustration of the sensor and the sensor-reader is provided in Figure 2.

The FreeStyle Libre subcutaneous continuous glucose monitoring system, consisting of (1) the sensor-reader and (2) the sensor.
The Eirus intravascular microdialysis system has previously been used and evaluated by us in the same type of patients included in this study, 19 that is, patients undergoing cardiac surgery, as well as by others who have evaluated the system in patients undergoing abdominal surgery, 20 and have been found to be useful and reliable in the ICU-setting. However, the FreeStyle Libre system was developed for use in stable out-clinic patients with diabetes, and has previously (to our knowledge) only been tested such patients. 21 Although the system has demonstrated good accuracy, its performance and suitability in the ICU is unknown. Technical details of both systems are specified in Table 1.
Technical Specifications of Both the Eirus Intravascular MD-CGM and the FreeStyle Libre SC-CGM Systems.
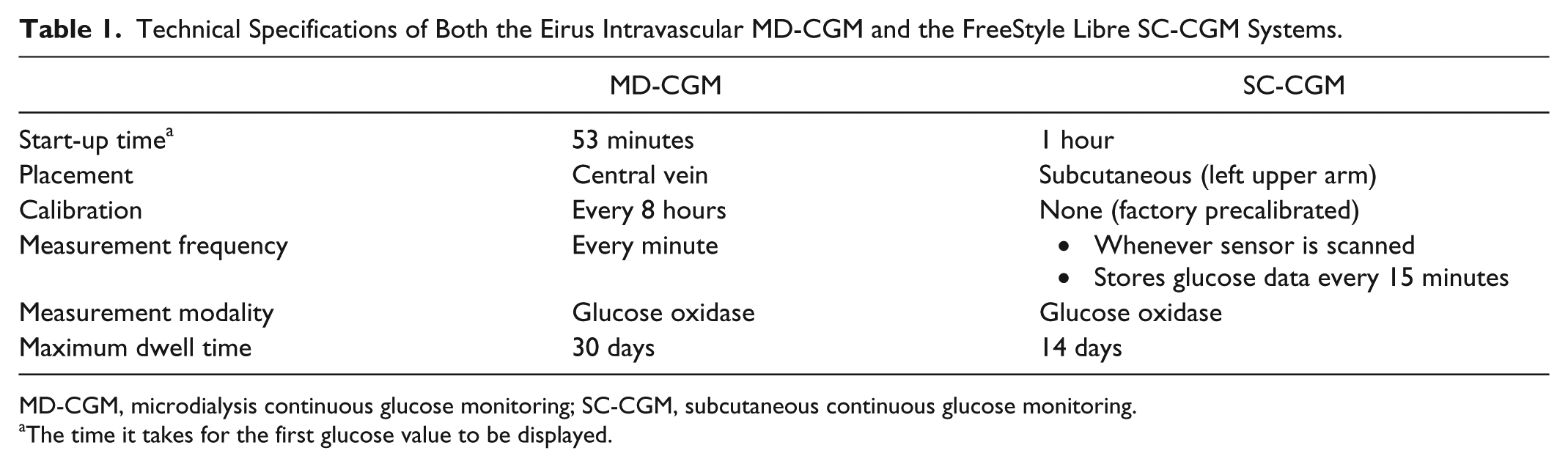
MD-CGM, microdialysis continuous glucose monitoring; SC-CGM, subcutaneous continuous glucose monitoring.
The time it takes for the first glucose value to be displayed.
Study Protocol
The SC-CGM system was set up as follows: the sensor was placed subcutaneously in the left upper arm the day before planned surgery, as recommended by the manufacturer (personal communication). The subcutaneous sensor was scanned with the sensor-reader every 4 hours (needs to be performed at least every 8 hours in order not to loose glucose data). The MD-CGM system was set up as follows: the microdialysis catheter was placed in the superior vena cava in the operating room after the patient was under general anesthesia and then connected to the microdialysis sensor and monitor. Perfusion of the microdialysis membrane was then begun and the initial blood glucose value displayed on the monitor after approximately 30 minutes. After calibration of the microdialysis system, CGM was initiated. Subsequent calibration was performed every 8 hours. Reference blood glucose values were obtained every hour by sampling arterial blood that was analyzed using a blood gas analyzer (ABL800 FLEX, Radiometer Medical, Copenhagen, Denmark). In addition, a capillary blood sample was analyzed using the POC function of the FreeStyle Libre sensor-reader every 4 hours. Neither the MD-CGM nor the SC-CGM systems were used to guide treatment with insulin. Both CGM-systems were removed the day after surgery. No postoperative anticoagulation was administered to the patients during the study period, as this is never initiated during the first 24 hours after surgery at our clinic. The microdialysis-catheter was used for all drug administration in the postoperative period. Patients received insulin infusions or injections as needed, aiming for a blood glucose range of 90-180 mg/dl during and after cardiac surgery. By clinical routine, all patients received 5% glucose infusion (1 ml/kg/h) postoperatively.
The time when the reference arterial blood gas glucose value was obtained was documented, and this reference value was then paired with the respective glucose value measured by the MD-CGM and the SC-CGM systems. POC glucose values were also compared with reference arterial blood gas glucose values. The MD-CGM system provides a glucose value every minute, while the SC-CGM system stores the glucose value every 15 minutes. To match the arterial blood gas glucose value taken at a specific time with the correct SC-CGM glucose value, a glucose level time course was plotted using the SC-CGM glucose values. The SC-CGM glucose value was then extracted from this graph. No correction for time lag was made.
Data Analysis
The accuracy of both CGM systems was evaluated by analyzing the mean glucose values, the mean difference between test and reference method as well as calculating the median and mean absolute relative difference (MARD). To further assess the glucose monitoring accuracy, Bland-Altman analysis 22 was performed as well as evaluation for International Organization of Standardization (ISO) criteria for blood glucose analyzing devices. ISO criteria (ISO15197:2003) require that 95% of the test glucose values to be within ±20% of the reference value if the reference value is >74 mg/dl or within ±14 mg/dl if the reference value is less than 74 mg/dl. 23 The criteria were updated in 2013 (ISO15197:2013), requiring 95% of the test glucose values to be within ±15% of the reference value if the reference value is >99 mg/dl and within ±14 mg/dl if the reference value is less than 99 mg/dl. 24 We have in this study evaluated the test glucose values according to the ISO criteria from 2013.
Error grid analysis (EGA) using the Clarke model was also performed to estimate the clinical accuracy of the CGM systems. The Clarke EGA plots paired glucose samples in 5 different zones. 25 Values in zone A are within 20% of the reference value and have no clinical implications. Values in zone B exceed 20% difference from reference value but lead to appropriate clinical decisions. Values in zone C may lead to unnecessary but harmless corrections. Values in zone D and E represent overestimation of hypoglycemia (failure to detect) or underestimation of hyperglycemia that may lead to incorrect clinical actions. In short, the more values in zone A and B the more clinical accuracy of the test method. The Clarke EGA has been criticized for its use in evaluation of blood glucose monitoring accuracy in the ICU since it was not developed for use in critically ill patients, nor does the original Clarke EGA make considerations for CGM. An updated version of the EGA that does consider continuous monitoring exists, but since it is difficult to perform and to interpret and since our reference method was measured intermittently, 26 we chose to use the original Clarke EGA.
All analyses were performed using either Microsoft Excel (Microsoft, Redmond, WA, USA) or SPSS version 23 (IBM, Armonk, NY, USA).
Results
During the study period from October to December 2015, 26 patients were included in the study. Out of these 26 patients, 24 patients had successful glucose monitoring with both the MD-CGM and the SC-CGM systems. The FreeStyle Libre system could be inserted and functioned well in all patients, while the initiation of the Eirus intravascular microdialysis system failed in 2 patients. In 1 patient this was due to late start of surgery (no personnel available to commence the system) and in the other patient this was due to malfunction of the microdialysis catheter most probably due to damage during insertion. Thus, glucose data was available from 24 patients. Characteristics of these patients are presented in Table 2.
Patient Characteristics
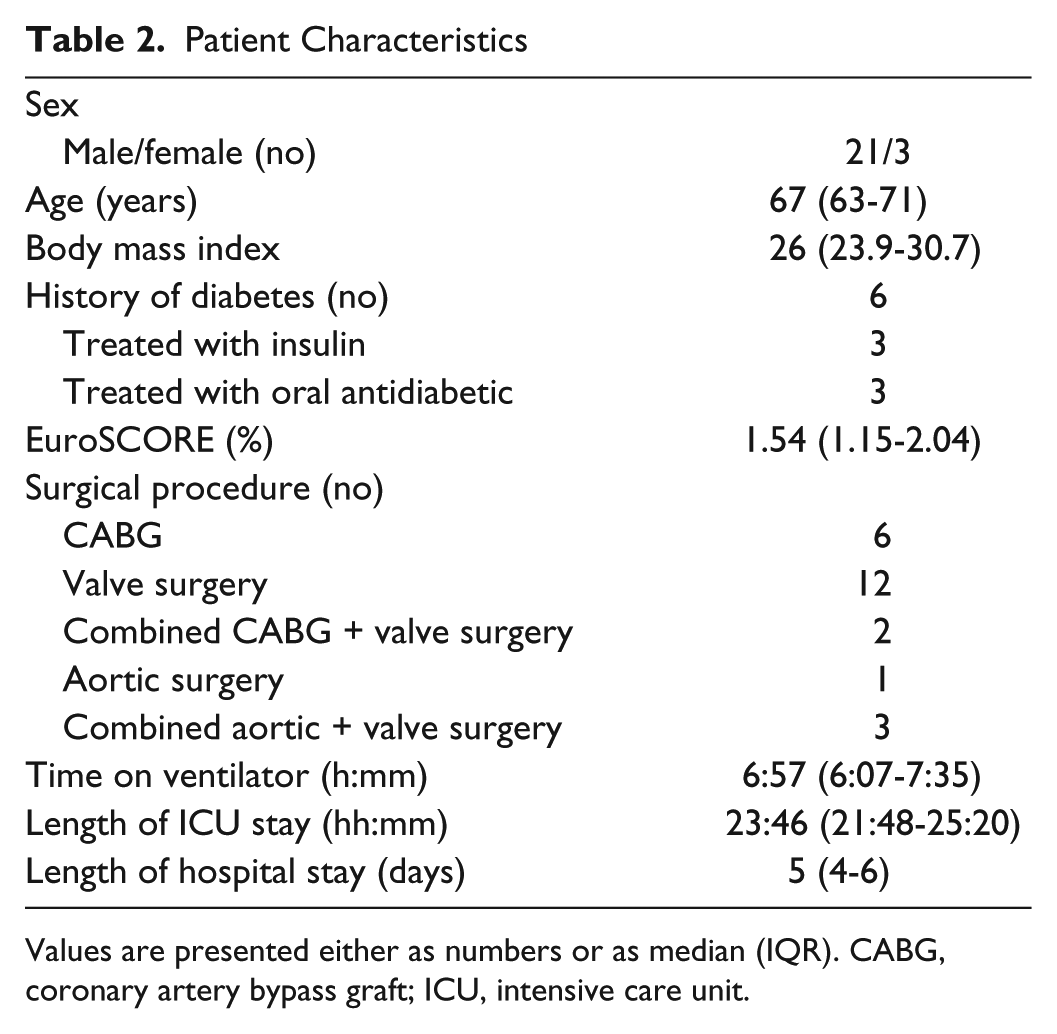
Values are presented either as numbers or as median (IQR). CABG, coronary artery bypass graft; ICU, intensive care unit.
Glucose was continuously monitored with the MD-CGM system for a mean (SD) of 26 (5) hours. The intravascular microdialysis system was reliable and no problems were experienced with insertion, except in the patient described above. After insertion of the microdialysis catheter, it took an average of (SD) 53 (11) minutes before the first glucose value was displayed on the monitor. In 1 patient, there were difficulties with the calibration procedure on 1 occasion resulting in no reliable glucose values for 2 hours. When calibration could be performed, the system functioned as usual. Otherwise, calibration was performed without difficulties. No complications were observed while using the MD-CGM system, including no blood clotting of the microdialysis membrane and no interference during drug administration. The microdialysis system performed CGM without interruptions in 2 patients. In the remaining 22 patients there were data gaps, median number of gaps (range) was 3 (1-8). The data gaps had a mean duration (SD) of 13 (19) minutes, and the median (range) was 10 (1-141) minutes. The data gap of 141 minutes was in the patient with the calibration complication detailed above for about 2 hours. The data gaps occasionally occurred at the time when the arterial blood gas was analyzed, thus resulting in a missed paired point in the accuracy analyses.
Glucose was continuously monitored with the SC-CGM system for a mean (SD) of 47 (7) hours. All FreeStyle Libre subcutaneous sensors functioned well and there were no problems with the insertion procedure. In 1 patient the sensor had to be replaced due to excessive sweating causing the first sensor to detach.
The mean (range) duration of data collection was 23.7 (21-24) hours. Mean (SD, range) reference glucose value during the study period was 147 (31, 63-288) mg/dl, and corresponding values for the MD-CGM system was 148 (34, 63-292) mg/dl and for the SC-CGM system 102 (32, 40-207) mg/dl. As demonstrated by these numbers, the SC-CGM system often measured lower glucose values than the reference method.
A total of 514 paired MD-CGM/reference and 578 SC-CGM/reference glucose samples were available for accuracy analysis. The reasons why there were more SC-CGM/reference samples were that the SC-CGM system was commenced before the MD-CGM system (the day before surgery) and that initiation of the MD-CGM system was more time-consuming. The accuracy of both CGM-systems is detailed in Table 3. The MARD for individual MD-CGM systems ranged from 2.5% to 12.6% and the MARD for individual SC-CGM sensors ranged from 12.0% to 52.1%. A time course of glucose levels from a single patient, as measured by all the different techniques used in this study is illustrated in Figure 3. This figure displays that both the MD-CGM and the SC-CGM systems followed the trend of the true blood glucose concentration (as measured by analysis of an arterial blood gas) very well, but the SC-CGM repeatedly underestimated the blood glucose value. The trend graph displays the same feature in all patients.
Results From Accuracy Analysis of the Eirus Intravascular Microdialysis and the FreeStyle Libre Subcutaneous CGM Systems.
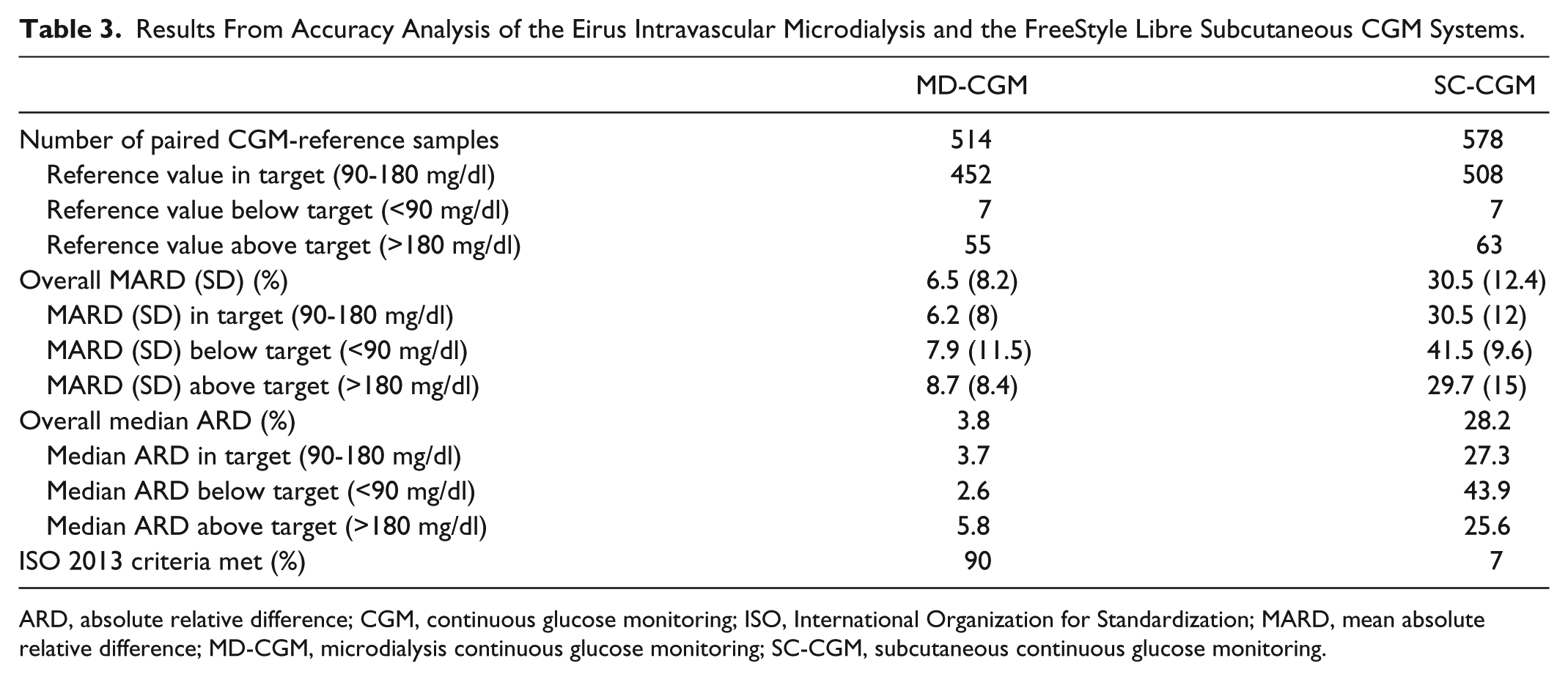
ARD, absolute relative difference; CGM, continuous glucose monitoring; ISO, International Organization for Standardization; MARD, mean absolute relative difference; MD-CGM, microdialysis continuous glucose monitoring; SC-CGM, subcutaneous continuous glucose monitoring.
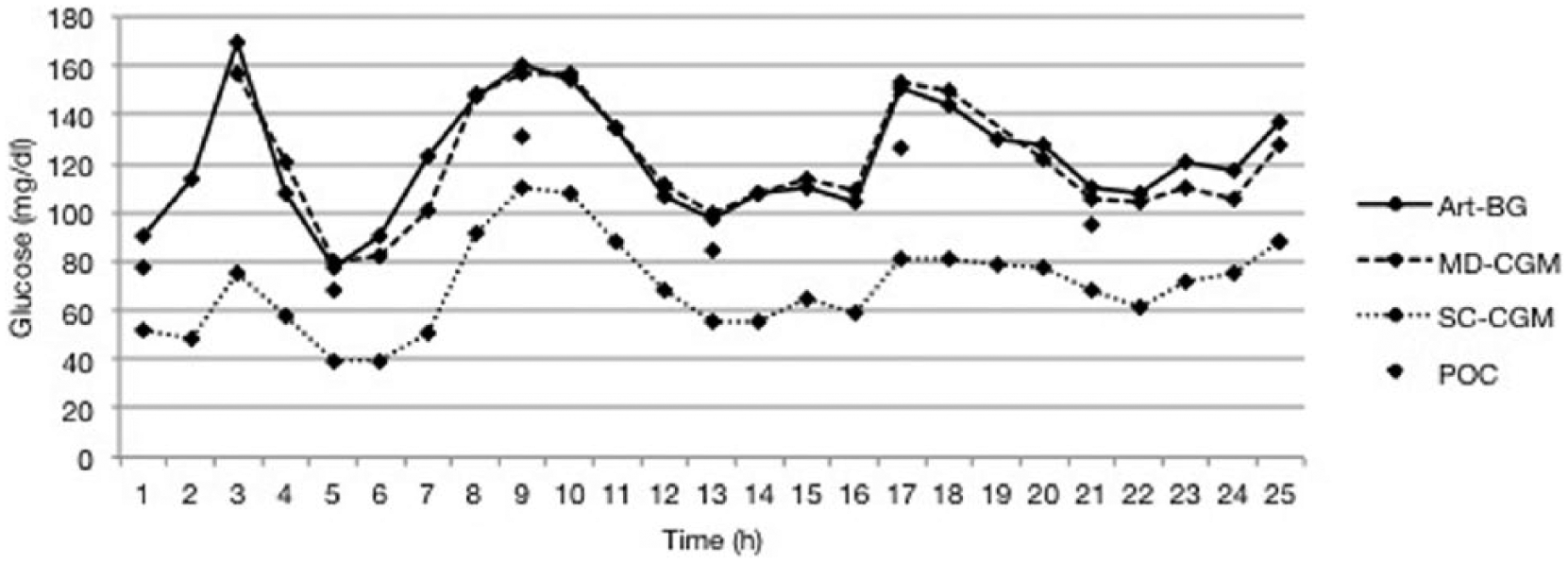
The time course of glucose levels in a single patient. The MD-CGM glucose values followed the reference method (Art-BG) very well. The SC-CGM and POC glucose values also followed the trend of the reference method, although lower glucose values were measured. The MARD of this patient was 5.03% for the MD-SCG system, 42.8% for the SC-CGM system, and 17.4% for the POC function of the sensor-reader. Art-BG, arterial blood gas; MD-CGM, microdialysis continuous glucose monitoring; POC, point-of-care glucometer; SC-CGM, subcutaneous continuous glucose monitoring.
Of the reference glucose values, 87.9% were within the target blood glucose range in the ICU (90-180 mg/dl). Only 7 reference glucose values were below this range, and only 1 of these was classified as being in the hypoglycemic range (ie, <74 mg/dl). That specific reference glucose value was 63 mg/dl and the corresponding MD-CGM value was 62.8 mg/dl and the SC-CGM value was 40 mg/dl. There was no difference in accuracy of the MD-CGM system in or above target blood glucose range, as illustrated by similar MARD values (Table 3). In addition, the difference in MARD between the various blood glucose ranges was not found to be statistically significant in a Kruskal-Wallis test, P = .119. However, the SC-CGM system improved precision with higher reference glucose values (MARD above target 29.7%, in target 30.5% and below target 41.5%). This improvement was found to be significant in a Kruskal-Wallis test, P = .016.
The POC function of the FreeStyle Libre sensor-reader was used to measure blood glucose on 157 occasions. The mean (SD, range) of the POC glucose values was 125 (31, 52-241) mg/dl and the mean (SD, range) of the paired reference glucose values was 140 (32, 63-232) mg/dl. The overall MARD was 12.3%.
Bland Altman analysis is illustrated in Figure 4. Mean difference (SD) was low for the MD-CGM system, 0.9 (15.1) mg/dl and higher for the SC-CGM system, –43.4 (20) mg/dl. The upper and lower limits of agreement were 29 and −27 mg/dl for the MD-CGM system and −4.5 and −82 mg/dl for the SC-CGM system. The negative mean difference and limits of agreement of the SC-CGM system imply that the system repeatedly measured a lower glucose value than the reference method. The POC function of the FreeStyle Libre sensor-reader had a mean difference (SD) of −15 (14) mg/dl. There was no visual trend toward more imprecision ranging from lower to higher blood glucose concentrations. The MD-CGM system did not meet the ISO criteria from 2013, as 90% of the paired values fell within that standard (required 95%). For the SC-CGM system, 7% of the glucose values were within the ISO 2013 criteria.
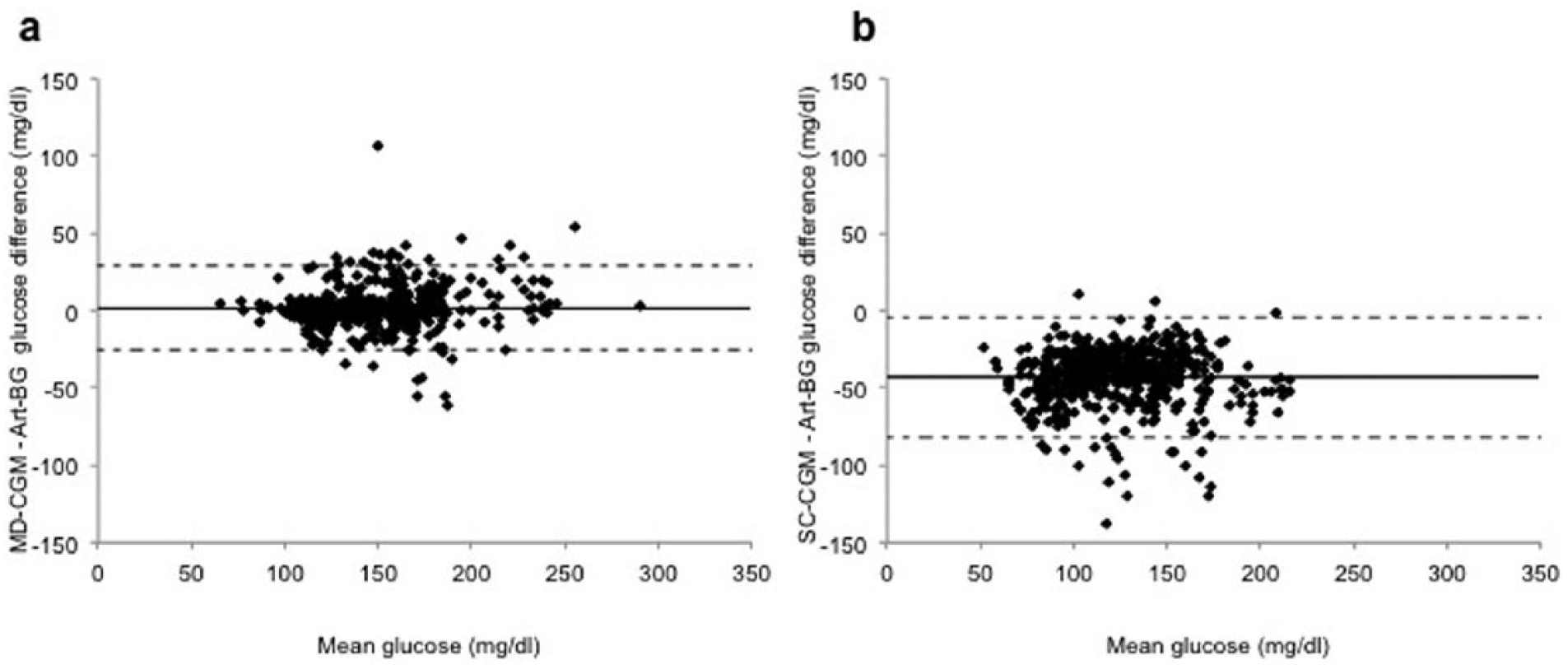
Bland Altman analysis of (a) MD-CGM versus reference glucose values and (b) SC-CGM versus reference glucose values. The difference between the CGM-systems and the reference glucose values are plotted against the average glucose value. The solid line represents the mean difference (MD-CGM 0.9 and SC-CGM −2.41mg/dl) and dotted lines represent the limits of agreement (mean difference ± 1.96 SD). Art-BG, arterial blood gas; MD-CGM, microdialysis continuous glucose monitoring; SC-CGM, subcutaneous continuous glucose monitoring.
The clinical accuracy as assessed by the EGA was good for the MD-CGM system with 100% of the paired samples within zones A and B (no altered clinical action), and 94% within zone A (Figure 5). The EGA of the SC-CGM system revealed 0.9% of the paired samples (n = 5) within in zones C, D or E implying that if treatment with insulin had been guided using these 5 glucose measurements, possibly incorrect clinical actions would have been taken. The remaining 99.1% of the paired samples were within zones A and B, with 18.9% within zone A.

Clarke error grid analysis of (a) MD-CGM versus reference glucose values and (b) SC-CGM versus reference glucose values. The different zones of the error grid represent various significances (see text for full explanation). Samples in zones A and B imply that the test glucose monitoring method would not have resulted in a different clinical action compared to the reference glucose monitoring method. MD-CGM, microdialysis continuous glucose monitoring; SC-CGM, subcutaneous continuous glucose monitoring.
Discussion
In this study we have used and compared 2 different CGM systems in patients undergoing cardiac surgery, the more invasive Eirus intravascular microdialysis system and the less invasive FreeStyle Libre subcutaneous system. Analysis of arterial blood in a blood gas analyzer was used as the reference method. The MD-CGM system was shown to be more accurate and precise for glucose monitoring compared to the SC-CGM system. The POC function of the FreeStyle Libre sensor-reader was more accurate than its CGM function, but still inferior to the MD-CGM system. However, the impact on GC has not been assessed for neither glucose monitoring method as this was not the aim for this study.
The accuracy results from the MD-CGM system were in line with those from our previous studies, also evaluating the same MD-CGM system in patients admitted to the ICU after cardiac surgery.19,27 The MD-CGM system has further been used by another researcher group and validated in patients undergoing abdominal surgery. 20 In addition, the accuracy was similar to that of another intravascular device measuring glucose continuously using a fluorescence technique.11,28 The microdialysis system was found to be consistent and effective, with no altering clinical action taken if the system had been used to guide treatment of blood glucose concentrations. No interference with clinical care was observed. The MD-CGM system was reliable, with the set up and insertion procedure being easy in all but 1 patient, in who damage to the microdialysis catheter occurred during insertion. There were data gaps in 22 patients, but these were often short (minutes) although sometimes unfortunately occurring when the reference glucose value was measured.
The SC-CGM system was very reliable and measured glucose completely without interruptions, and there were consequently no data gaps. The accuracy was worse compared to other SC-CGM devices used in cardiac surgery patients. 12 The reasons for this poor outcome were neither the focus nor the aim to explore further in this study, and to what degree this is due to impaired microcirculation in these patients remains unanswered. The impact of reduced microcirculation was recently evaluated using another SC-CGM device in patients undergoing cardiac surgery, but no relation was demonstrated to sensor function. 17 Figure 3 demonstrates that the SC-CGM glucose values followed the trend of glucose analyzed by an arterial blood gas, suggesting that impaired microcirculation is not the reason why the SC-CGM system often reported a lower glucose value than the reference method. If the microcirculation were in fact affecting the SC-CGM system, the glucose analysis would probably be more static. If it was possible to recalibrate the FreeStyle Libre system, this could potentially improve the glucose monitoring truthfulness. The FreeStyle Libre was developed for use in stable out-clinic patients and its performance in the ICU has up until now not been known. It is possible that adjustments to optimize its use in the ICU-setting could further improve the accuracy. The accuracy of the POC function of the FreeStyle Libre sensor-reader was better than the CGM function of the same system, but still not as good as the microdialysis system.
The two CGM systems used in this study did not only differ in accuracy, they also differ in some important technical details. The FreeStyle Libre is minimally invasive and the sensor can easily be inserted. The intravascular microdialysis system is more invasive and requires central venous access for insertion. This leads to that the startup of the microdialysis system is more time-consuming and complex. However, in critically ill patients a central line is often required, which means that the microdialysis system would not be an additional invasive procedure in these patients. Another principal difference is how continuous the glucose monitoring is executed. The FreeStyle Libre system analyzes blood glucose every 15 minutes, which is the definition used to define CGM by the CLSI (Clinical Laboratory Standards Institute). Although the FreeStyle Libre system is continuous by definition, it may be argued that it performs glucose monitoring in an automated intermittent manner when compared to the intravascular microdialysis system, which analyzes glucose every minute. Another technical difference is the way the glucose concentration is displayed. The glucose value analyzed by the FreeStyle Libre system is visible on the sensor-reader screen and the sensor-reader thus needs to be picked-up, turned on and the sensor needs to be scanned every time the attending staff wants to know the blood glucose concentration. While the microdialysis system takes longer to set up, it does not require any additional workload after startup besides the calibration procedure every 8 hours, and the glucose value is continuously displayed on the monitor as a numerical value and a trend graph. We believe that these technical features of the intravascular microdialysis system makes it more clinically useful and perhaps more intuitive as the glucose trend is always visible, facilitating the interpretation of the glucose monitoring. In addition, following the glucose trend diminishes the need for absolute point accuracy, as each individual glucose value becomes less important if put in context of a trend.
There are several limitations to this study. For one, the study was performed in a specialized setting on patients undergoing cardiac surgery. It is plausible that the accuracy could differ if the CGM systems were used in other patient categories. A further limitation was the lack of hypoglycemic glucose values, implying that the CGM systems were solely evaluated and compared in normal to high blood glucose concentrations. There was only 1 reference glucose value that was in the hypoglycemic range, and this is not sufficient to argue that the hypoglycemic accuracy was adequately evaluated. However, the accuracy of the MD-CGM system in hypoglycemia has previously been evaluated in an animal model with as good results as in higher blood glucose concentrations. 29 Furthermore, we cannot comment on the function of either CGM system beyond 24 hours, as glucose monitoring was ceased at that point.
Conclusion
This study has demonstrated that the Eirus intravascular microdialysis system may safely be used for CGM in patients undergoing cardiac surgery and that it is more accurate than the FreeStyle subcutaneous CGM system. The microdialysis system was also superior in accuracy compared to the POC function of the FreeStyle Libre sensor-reader that analyzes capillary blood. These results support using a more invasive CGM technique in critically ill patients admitted to ICUs due to the importance of accurate glucose monitoring.
Footnotes
Abbreviations
CGM, continuous glucose monitoring; CVC, central venous catheter; EGA, error grid analysis; GC, glycemic control; ICU, intensive care unit; ISO, International Organization of Standardization; MARD, mean absolute relative difference; MD-CGM, microdialysis continuous glucose monitoring system; POC, point of care; SC-CGM, subcutaneous continuous glucose monitoring system.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: AFC and JL were cofounders of Dipylon Medical AB, which was later acquired by CMA Microdialysis AB and subsequently sold to Maquet Critical Care.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the Mats Kleberg Foundation and the Signe and Olof Wallenius Foundation.