
Abstract
Background:
Ambulatory care underwent rapid changes at the onset of the COVID-19 pandemic. Care for people with diabetes shifted from an almost exclusively in-person model to a hybrid model consisting of in-person visits, telehealth visits, phone calls, and asynchronous messaging.
Methods:
We analyzed data for all patients with diabetes and established with a provider at a large academic medical center to identify in-person and telehealth ambulatory provider visits over two periods of time (a “pre-COVID” and “COVID” period).
Results:
While the number of people with diabetes and any ambulatory provider visit decreased during the COVID period, telehealth saw massive growth. Per Hemoglobin A1c, glycemic control remained stable from the pre-COVID to COVID time periods.
Conclusions:
Findings support continued use of telehealth, and we anticipate hybrid models of care will be utilized for people with diabetes beyond the pandemic.
Introduction
The identification of diabetes as a risk factor for severe disease from COVID 1 led to increased concerns and prioritization of care for people with diabetes, including access to care, self-management, and glycemic control. There was an understanding that diabetes care needed to continue, even if in-person visits were not an option.
Prior to the pandemic, diabetes care was delivered almost exclusively through in-person visits. Synchronous video visit use was limited as the Centers for Medicare and Medicaid Services (CMS) only reimbursed video visits when they occurred at a health care facility in a rural area designated as a Health Professional Shortage Area. As a result, data on the use of telehealth as a component of diabetes management are limited. Available studies are generally small in size with short-term interventions, and while heterogeneity makes direct comparisons challenging, findings are primarily positive.2 -4
At the onset of the COVID pandemic, health care systems quickly pivoted to telehealth to address and manage known risk factors while keeping patients and providers safe.5,6 Since much of outpatient diabetes management involves taking a history, reviewing glucose data and laboratory results, and discussing potential changes to the treatment regimen, it is particularly amenable to telehealth.
At an academic health system located in a Midwestern U.S. state, care for people with diabetes was quickly transformed into a hybrid model to help maintain continuity of care. In-person visits, synchronous video visits (herein referred to as telehealth), phone calls, and asynchronous messaging via a secure patient portal were all utilized. The purpose of this study was to expand upon the body of evidence regarding the integration of telehealth into diabetes management as a consequence of the COVID pandemic. We do so by identifying if provider access differed for patients with an established source of care with the health system during the COVID time period relative to established patients in the pre-COVID period. We also described the frequency of telehealth use and differences in diabetes control between the two time periods.
Methods
Study Design and Study Data
This historical, cross-sectional study included patients with a diagnosis of diabetes. Included patients also had established a source of care based on having at least one ambulatory visit with a primary care or specialty provider in clinics owned and operated by the health system. The study protocol was reviewed and approved by the University of Nebraska Medical Center’s Institutional Review Board. This study used a limited data set of electronic health record (EHR) data on in-person or telehealth ambulatory provider visits from March 16, 2017, through March 15, 2021.
Study Timeline and Study Groups
Two groups were identified for 1-year study periods representing a pre-COVID period (March 16, 2019, to March 15, 2020) and a COVID period (March 16, 2020, to March 15, 2021) (Supplemental Appendix Figure A1). Included patients had at least one ambulatory visit for any reason and a documented diagnosis of diabetes in the EHR (ICD-10-CM SNOMED CT) during the 2-years prior to the start of the specific study period using a previously validated computable phenotype from the U.S. National Library of Medicine’s Value Set Authority Center. 7 Full definitions are available in the supplemental material (Supplemental Appendix Table A1). Patients could be in one or both study periods.
Dependent Variables
The primary dependent variable was the occurrence of at least one ambulatory provider visit during the study period. Ambulatory provider visit delivery method (in-person vs telehealth) was also captured, and patients were categorized as having all in-person visits, one or more telehealth visits, or no provider visit.
Hemoglobin A1c (A1c) values were captured during each study period as a measure of glycemic control. When patients had more than one A1c value in the study period, the mean of the values was reported. In addition, it was identified if patients had any A1c value <8.0% or a value >9.0% during the study period.
Independent Variables
Independent variables for baseline demographic and clinical data were identified for each study period to describe the groups, and included age, payer type, sex, and race. Age was based on age at the beginning of the period of interest. Other baseline characteristics were pulled from the patient’s ambulatory visit closest but prior to in the start of the specific study period. Socioeconomic data (income, education level, and rurality) and Internet access were assigned to patients based on their zip code of residence at the time of the data pull using American Community Survey 2019 5-year estimates. 8
Statistical Analyses
As the study period groups were not independent, only descriptive statistics were used to present baseline characteristics and unadjusted results by time period. Mean values are presented ± standard deviation (SD). No steps were made to impute missing data, given then small rate of missingness for baseline characteristics (<1% for all variables except insurance type, which was <6%, in which case we created a separate category for missing insurance type). Thus, for all descriptive statistics, percentages were calculated using the nonmissing data within each variable as the denominator. For a subgroup analysis looking at patients who had at least one visit during the COVID period, chi-square tests were used to test the association between visit modality over the period (telehealth only, in person only, or a hybrid of both in person and telehealth) and glycemic control outcome variables.
Multivariable regression analysis using a generalized estimating equation (GEE) with robust standard errors was conducted using a log link and Poisson distribution to generate the adjusted relative risk (aRR) of patients having an ambulatory provider visit during the COVID period relative to the pre-COVID period, controlling for patient characteristics. The GEE approach accounted for the correlation within patient using a compound symmetry working correlation matrix structure. Adjusted relative risks were presented with 95% confidence intervals (95% CIs), which were Bonferroni adjusted for explanatory variables with more than two subgroups. The same modeling technique was also used to determine the aRRs for time period as it related to having either a high or low A1c, for patients who had A1c values.
As a sensitivity analysis to assess for potential model overfitting, models which were more parsimonious were generated for each outcome by first modeling age as a continuous variable (either linear or quadratic, when significant), and removing preferred language due to its smaller subgroup sizes and association with other variables in the model (ie, race and ethnicity). After running this initial reduced model, any additional explanatory variables that had a main effect P value of more than .05 were removed in a sequential fashion. Then, the aRRs were compared between the full and reduced models. Statistical analyses were performed using SAS version 9.4 (SAS Institute Inc., Cary, NC, USA).
Results
A total of 30 871 patients with diabetes were included in the pre-COVID group and 32 500 in the COVID group. Overall, 25 765 (68.5%) patients were included in both study period groups. Baseline characteristics for each time period are described in Table 1. The mean age in both groups was 61 ± 16 years, and 54% were female. The groups were predominantly white (78.8%) and non-Hispanic (~93.5%), and a majority (~50%) had Medicare coverage. Mean baseline A1c for both periods was 7.4%.
Baseline Characteristics of Patients With Diabetes Established With Health System Providers by Study Period.
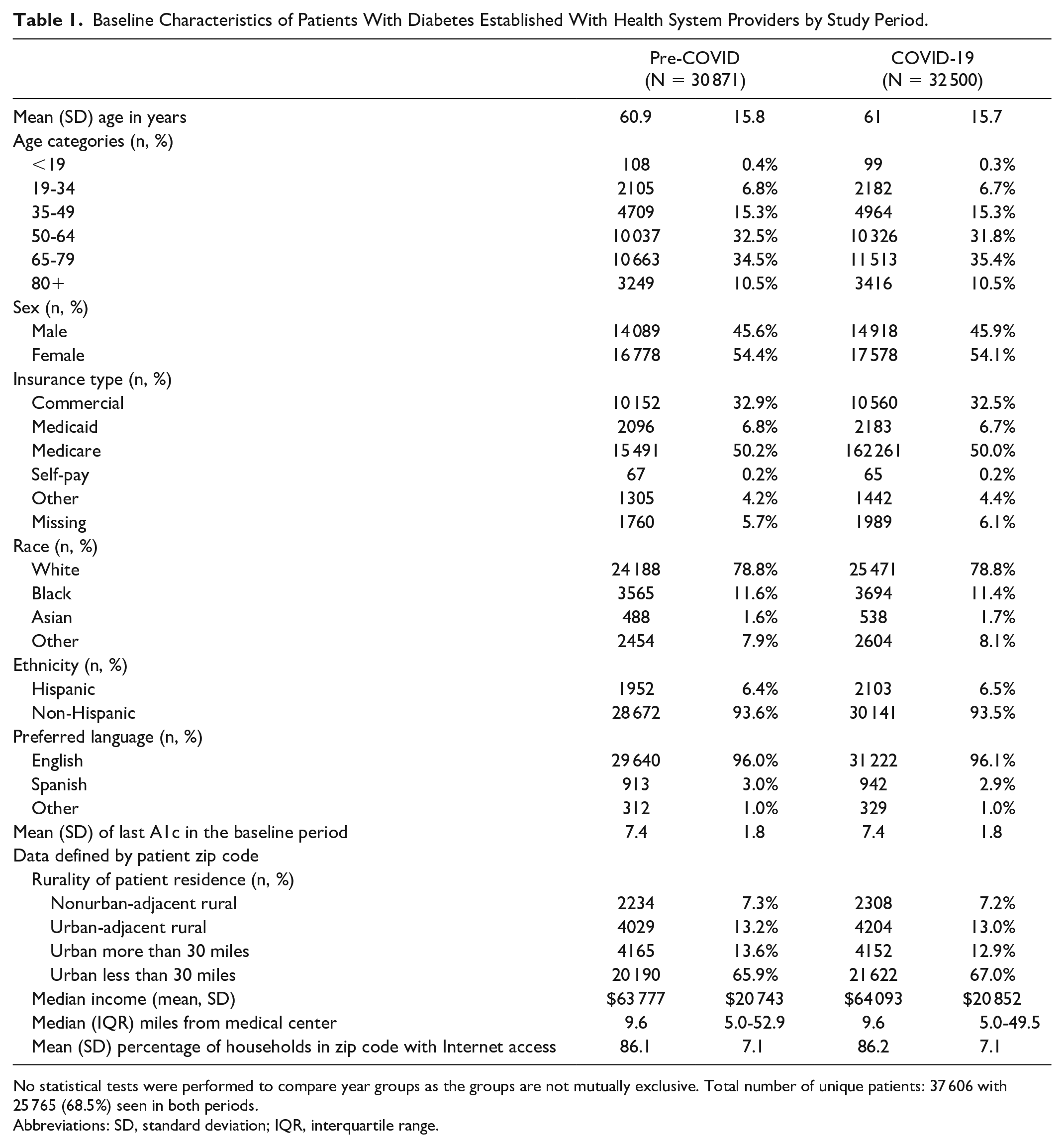
No statistical tests were performed to compare year groups as the groups are not mutually exclusive. Total number of unique patients: 37 606 with 25 765 (68.5%) seen in both periods.
Abbreviations: SD, standard deviation; IQR, interquartile range.
Provider Visits During COVID
The percentage of patients with an ambulatory provider visit was 67.1% in the pre-COVID and 64.6% in the COVID period. In multivariable regression analyses, patients were less likely to have any provider visit (in person or telehealth) in the COVID period compared with the pre-COVID period (aRR 0.91, 95% CI 0.902, 0.916), controlling for demographic and clinical characteristics. Other factors associated with having a provider visit included age, with most age groups having a lower risk of having a visit relative to those age 50 to 64 years. Being female and having Medicare coverage versus commercial insurance were associated with a higher risk of having a visit. However, self-pay and Medicaid insurance were associated with a lower risk of having a visit during the COVID period. Patients whose preferred language was not English, nonurban patients, and those living more than 30 miles from the medical center were also less likely to have had a visit in the COVID period (Supplemental Appendix Figure A2).
Telehealth Use
Few included patients had a telehealth provider visit pre-COVID (0.8%). In the COVID period, 32.8% had at least one telehealth visit (Figure 1). As with baseline characteristics, inferential statistics were not performed as the study period groups were not mutually exclusive.
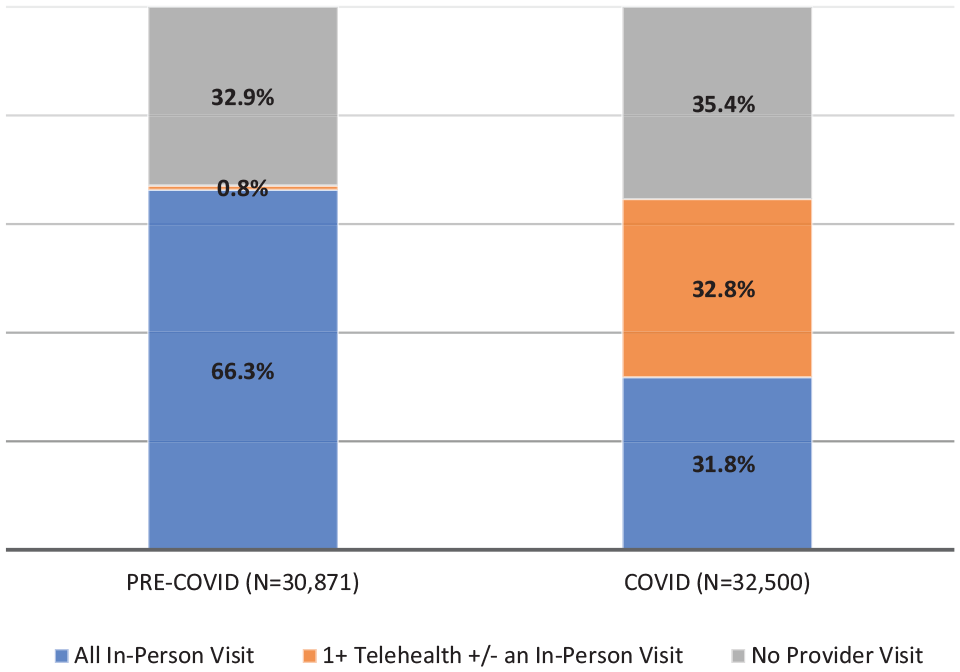
Proportion with ambulatory provider visits by any telehealth or all in-person for patients with diabetes during COVID and pre-COVID study periods.
Glycemic Control
The proportion of patients with an A1c value recorded in the EHR during the study period was 41.7% during pre-COVID and 38.5% during the COVID period (Supplemental Appendix Table A2). Mean A1c during the pre-COVID period for patients with A1c data was 7.38% (1.65) versus 7.41% (1.76) in the COVID period. These values differed very little from the mean baseline A1c for the corresponding study period.
Most patients in the Pre-COVID and COVID periods had at least one A1c of <8.0% (78.9 and 78.3% respectively). The risk of having an A1c <8.0% during COVID was slightly less than the pre-COVID (aRR 0.98; 95% CI 0.97, 0.99). Fewer than 20% of each group had an A1c during the study period >9.0% (19.1 and 18.6%, respectively), and the risk of having an A1c >9.0% did not differ between the COVID and pre-COVID study periods (aRR 0.98; 95% CI 0.94, 1.02) (Supplemental Appendix Table A2).
To further investigate glycemic control, patients with at least one visit during the COVID period were grouped by their visit modality for the period: telehealth only, in person only, or hybrid. As hybrid was defined by having at least one visit of each type, their mean number of visits during the period (8.4 ± 7.2) was higher than patients in the in person only (3.3 ± 3.2) and telehealth only (2.1 ± 3.1) groups. There were significant associations between visit modality and both A1c less than 8% (P = .02) and A1c greater than 9% (P = .01). For both outcomes, the only telehealth group had the lowest percentage of patients out of the three modalities: A1c < 8% (73.2% vs 78.5% [hybrid] and 78.5% [in person only]) and A1c > 9% (16.4% vs 19.7% [hybrid] and 17.6% [in person only]).
Sensitivity Analysis
After performing the sensitivity analysis for the aRRs for time period for each of the outcomes, it was noted that the aRR estimates and associated 95% confidence intervals did not change by more than 0.001 between the full and final reduced model for any of the outcomes.
Discussion
This study is unique in that it includes over 30 000 people with diabetes seen in a large academic health care system in the United States. At the time of this study, little data existed in the literature regarding access to care for people with diabetes. Since this time, there has been extensive literature published on the effects of COVID on diabetes management, but to our knowledge, none have focused on how COVID affected access to care as well as glycemic control in people with type 1 or type 2 diabetes.9 -12 Similarly published studies were conducted outside the United States, or focused on the effect of COVID and use of telehealth on glycemic control in a single cohort. In addition to glycemic control, we examined access to care for both the overall group as well as those utilizing telehealth.
In this retrospective analysis of patients with diabetes, ambulatory provider visits declined, as expected. We also identified that key patient factors may have influenced access to provider care, including gender, language and insurance type. While access to provider care declined overall, the proportion of patients with at least one telehealth visit increased substantially in the pre-COVID period (0.8%) to a third of all patients during the COVID period, demonstrating a substantial effort to maintain care continuity during the first year of the pandemic.
Furthermore, concerns about poor diabetes control during COVID were not observed in those with documented A1c values, as the proportion with A1C >9.0% was similar between time periods. However, the proportion of patients with A1c <8.0% was similar between periods.
Findings from existing literature are mixed relative to glycemic control during COVID. A systematic review of glycemic control during lockdown in people with diabetes showed that people with type 1 diabetes tended to have improved glycemic control while those with type 2 diabetes tended to have worsening control. 13 However, this systematic review did not include U.S.-based studies. Studies based in numerous countries have now shown that people with diabetes utilizing telehealth were able to maintain diabetes control when compared with the prepandemic period.9,10,12,14
A potential explanation for our findings of stable glycemic control in those with A1c data is the health system’s model of care. All primary care clinics in our health system utilize a patient centered medical home model, which provides multidisciplinary team-based care with a population health focus. Concerns regarding poor outcomes for people with diabetes may have triggered care teams to be more proactive with patient outreach during times of high COVID transmission in the community.
Stable glycemic control is also suggestive of continued diabetes medication access. Many payers passed and our health system promoted pandemic-related policies allowing for 90-day prescription fills and for community pharmacies to mail prescriptions to patients.15 -17 Thus, even if patients delayed a provider visit, these medication-related policy changes may have allowed people with preexisting diabetes to continue their medication regimens.
In this study, half of patients with a provider visit had at least one telehealth visit. Prior research has shown that people with diabetes utilizing telehealth during the pandemic had similar quality measures, including glycemic control, compared with prepandemic values, while those not utilizing telehealth showed a decrease in quality measures. 10 Stable glycemic control despite a decreased number of in-person visits supports the concept that diabetes management is amenable to remote interventions.
The results of this and other recent research have implications for care delivery. Findings support telehealth’s ability to facilitate efforts to “meet the patient” to optimize care and outcomes in “normal” times, not just in times of disruption. This study highlights an opportunity for telehealth to facilitate improved access to diabetes care, close care gaps, and address clinical inertia. Given these advantages and opportunities, we anticipate that health systems and providers will continue to use hybrid models to manage diabetes care, with regular in person visits supported by interim telehealth visits.
Limitations
A strength of this study is that it was based on a large data set from an academic health center with a wide geographic catchment area. However, there are several limitations that warrant mention. As a historical cross-sectional study, results are subject to confounding bias. This includes unmeasured confounders that likely differed between the time periods such as adherence to lifestyle recommendations. In addition, we used a pre-post design with time-based groups that were not identical or mutually exclusive. While this more accurately reflects the diabetes population in each period, the groups lack independence. Thus, only descriptive statistics were performed on baseline characteristics. However, multivariable methods appropriate for groups that lack independence were performed to identify the relative risk of having a provider visit and of attaining glycemic quality targets.
To assess glycemic control, we relied on A1c data captured in the EHR, which was missing for over half of the patients in each time period. We are aware that many lab tests were postponed during the COVID period to mitigate risk. Laboratory A1c draws may have been replaced by home A1c testing or by continuous glucose monitoring data, which were not captured in the EHR. Furthermore, patients with A1c data in the EHR in the COVID period may differ from those who did not. Other limitations with our data set include lack of information about prior health-seeking behavior and long-term history such as diabetes duration and historical glycemic control. We also did not collect data on asynchronous portal messaging, medications lists, use of diabetes technology, and reason for visit, which may have affected outcomes. Finally, study groups consisted of patients with an ambulatory visit in our health system with a diagnosis of diabetes but was not limited to patients specifically receiving diabetes care by our health system. Thus, the study likely includes patients whose diabetes was managed outside our health system, contributing to missing outcomes data. Similarly, children with diabetes are underrepresented in this study as many are managed by providers affiliated with a separate children’s hospital.
Conclusion
The increased utilization of telehealth with stable glycemic control during the COVID-19 pandemic indicates that at a population level, utilizing telehealth for diabetes care was not likely detrimental. Given current signals from payers that they will continue to reimburse for telehealth beyond the public health emergency, the way we care for people with diabetes is well poised for change.
Supplemental Material
sj-docx-1-dst-10.1177_19322968231162866 – Supplemental material for In-Person and Telehealth Provider Access and Glycemic Control for People With Diabetes During the COVID-19 Pandemic
Supplemental material, sj-docx-1-dst-10.1177_19322968231162866 for In-Person and Telehealth Provider Access and Glycemic Control for People With Diabetes During the COVID-19 Pandemic by Leslie Eiland, Proleta Datta, Kaeli Samson, Jerrod Anzalone, Anthony Donovan and Carrie McAdam-Marx in Journal of Diabetes Science and Technology
Supplemental Material
sj-docx-2-dst-10.1177_19322968231162866 – Supplemental material for In-Person and Telehealth Provider Access and Glycemic Control for People With Diabetes During the COVID-19 Pandemic
Supplemental material, sj-docx-2-dst-10.1177_19322968231162866 for In-Person and Telehealth Provider Access and Glycemic Control for People With Diabetes During the COVID-19 Pandemic by Leslie Eiland, Proleta Datta, Kaeli Samson, Jerrod Anzalone, Anthony Donovan and Carrie McAdam-Marx in Journal of Diabetes Science and Technology
Supplemental Material
sj-docx-3-dst-10.1177_19322968231162866 – Supplemental material for In-Person and Telehealth Provider Access and Glycemic Control for People With Diabetes During the COVID-19 Pandemic
Supplemental material, sj-docx-3-dst-10.1177_19322968231162866 for In-Person and Telehealth Provider Access and Glycemic Control for People With Diabetes During the COVID-19 Pandemic by Leslie Eiland, Proleta Datta, Kaeli Samson, Jerrod Anzalone, Anthony Donovan and Carrie McAdam-Marx in Journal of Diabetes Science and Technology
Supplemental Material
sj-docx-4-dst-10.1177_19322968231162866 – Supplemental material for In-Person and Telehealth Provider Access and Glycemic Control for People With Diabetes During the COVID-19 Pandemic
Supplemental material, sj-docx-4-dst-10.1177_19322968231162866 for In-Person and Telehealth Provider Access and Glycemic Control for People With Diabetes During the COVID-19 Pandemic by Leslie Eiland, Proleta Datta, Kaeli Samson, Jerrod Anzalone, Anthony Donovan and Carrie McAdam-Marx in Journal of Diabetes Science and Technology
Footnotes
Abbreviations
A1c, Hemoglobin A1c; aRR, adjusted relative risk; CMS, Centers for Medicare and Medicaid Services; EHR, Electronic Health Record; GEE, generalized estimating equation.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: LE: ProventionBio, Sanofi, Roche, and Cecelia Health. PD, KS, JA, AD, and CMM report no conflicts of interest.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Institute of General Medical Sciences, U54 GM115458, which funds the Great Plains IDeA-CTR Network, and the UNMC Clinical Research Analytics Environment (CRANE). CRANE was supported by funding from the National Institute of General Medical Sciences, U54 GM115458, and the Patient-Centered Outcomes Research Institute, PCORI CDRN-1306-04631. The content is solely the responsibility of the authors and does not necessarily represent the official views of the NIH or PCORI. The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.