
Abstract
This study evaluated the associations between depressive symptoms, emotion dysregulation and bulimic symptoms in youth with type 1 diabetes (T1D) in the context of the diagnosis and treatment of T1D. Study participants were 103 youth in 2 distinct groups: newly diagnosed (New) or transitioning to pump therapy (continuous subcutaneous insulin infusion [CSII]; “Pump”), who completed questionnaires regarding symptoms of depression, emotion dysregulation, and bulimia. Glycemic control (A1c), height, weight, and questionnaires were evaluated within 10 days of diagnosis (n = 58) or at education/clinic visit before starting insulin utilizing CSII (n = 45). In the newly diagnosed group, only depression accounted for significant variance in bulimia scores (β = .47, P < .01). For the group with disease treatment experience (Pump), but not for the newly diagnosed group (New), greater depressive symptoms and emotion dysregulation were associated with greater bulimic symptoms. Depressive symptoms and emotion dysregulation, an indicator of poor coping/behavioral control, could help explain adoption of disordered eating behaviors in youth with T1D who are transitioning to pump therapy.
Adolescents with type 1 diabetes (T1D) report elevated rates of disordered eating behaviors (DEB), most commonly bulimic symptoms such as binge eating and purging.1-5 Of particular concern is purging via glucosuria (glucose excreted through the urine) due to underdosing insulin, which is linked with poor health outcomes such as retinopathy, neuropathy, and premature mortality.6,7 In addition, individuals with T1D engaging in DEB have poorer glycemic control with hemoglobin A1c levels as much as 2% higher than non-eating-disordered individuals with T1D.2,8 Thus, disordered eating is associated with significant morbidity in T1D patients, making identification of risk factors a priority.
Both depressive symptoms and emotion dysregulation are independently associated with higher rates of disordered eating in the general population.9-11 It is unknown how the combination of these psychological risk factors is associated with development of DEB in the context of diabetes onset and treatment for youth with T1D. 12 These 2 contextual factors, onset and treatment method, appear to be especially important variables to consider when developing and testing models of risk for DEB in T1D. The initial onset and diagnosis of a chronic illness in and of itself may increase risk for psychological factors associated with DEB, such as depressive symptoms. Regarding treatment type, DEB occurs in similar rates across insulin treatment modalities (eg, multiple daily injections [MDI] vs continuous subcutaneous insulin infusion [CSII]).13,14 Youth on CSII with DEB are more likely to discontinue CSII use as compared to youth without DEB. 13 However, a recent study demonstrated that following 6 months of CSII treatment, DEB symptoms were reduced. 15 Thus, from the sparse literature available on this topic, it appears that the function or presentation of DEB symptoms, although not frequency, may vary depending up on the treatment context. The goals of this study are to examine the association of depression and emotion dysregulation to DEB in 2 samples of youth with T1D; those who have been newly diagnosed, and those who are transitioning to CSII. As these 2 groups are experiencing different psychological realities (adjusting to a new diagnosis vs management of an ongoing, chronic, disease), the relationship of depression and emotion dysregulation to DEB may vary within each group.
Approximately 15% of adolescents with T1D report symptoms of depression, almost twice the rate of healthy controls and depression is significantly associated with acute (eg, diabetic ketoacidosis) and chronic (eg, macrovascular problems) diabetes-related complications.16,17 Depression has been hypothesized as a risk factor for the development of DEB, 18 and studies show that depression significantly predicts DEB in the T1D population.19,20
Emotion regulation has been conceptualized as processes by which individuals moderate their emotions in response to demands placed on them by their environment.21-23 For patients with T1D, their environment includes treatment of their disease. Persons who are emotionally dysregulated have been found to engage in maladaptive behaviors in response to negative emotions. 24 Emotion dysregulation 22 is associated with disease related stressors, nonadherence, and DEB in adolescents with T1D.25,26 Emotion regulation may be especially relevant to youth who have been living with T1D because of the physiologic factors associated with the disease itself such as hypoglycemia. Indeed, studies have reported that hypoglycemia contributes to failures in self-regulation and the experience of negative mood states.27,28 T1D youth who are newly transitioning to pump therapy may have had the experience of unsuccessful regulation of blood glucose with insulin injections, which increases hypoglycemia. 15 Thus, it is reasonable to expect that youth living with T1D prior to transition to insulin pump may demonstrate increased emotion dysregulation, which in turn is associated with increased risk for DEB.
The relationships between these known psychosocial risk factors for DEB: depressive symptoms and emotion dysregulation have not been simultaneously studied in youth with T1D, and very few studies at all have examined youth with T1D who have been newly diagnosed versus transitioning to CSII. Examination of risk for DEB in each of these groups permits elucidation of the putative contributions of disease onset and treatment-related risk for DEB in the T1D population, which has not previously been examined. We hypothesized that age matched newly diagnosed youth (New) would endorse similar levels of bulimic symptoms compared to youth with established disease (CSII), replicating previous studies.13,14 Although we recognize that these 2 groups of youth have qualitatively distinct experiences with T1D, we wished to demonstrate replication of previous studies on frequency of DEB in these 2 groups, as this topic has been understudied. We hypothesized that pump youth would endorse greater depressive symptoms secondary to difficulty controlling glycemia and/or weight, consistent with previous studies. 13 Between group differences in endorsement of emotion dysregulation was not a priori hypothesized, as there is so little empirical data on this topic. We examined the relative contribution of both depressive symptoms and emotion regulation to endorsement of bulimic symptoms in both groups. As described above, we hypothesize that emotion regulation may contribute significant variance to DEB in those individuals newly transitioning to pump therapy, due to both risk for hypoglycemia and the stress of living with a chronic illness. Finally, we hypothesized that bulimic symptoms in both groups would be associated with elevated A1c.
Methods
Participants
In all, 103 youth were originally enrolled. Two Pump patients were dropped from analyses because 1 was found not to be 10 years old at baseline assessment and 1 did not begin CSII use. Thus, our final sample included 101 participants (54.4% female) between the ages of 10 and 17 years (mean = 12.8, SD = 2.1). The majority of the sample (75%) was Caucasian and consisted of 58 New (newly diagnosed) participants and 45 Pump (transitioning to pump) participants.
Procedures
Inclusion criteria included being between the ages of 10 and 17, either a new diagnosis of T1D or individuals with T1D who were beginning pump therapy and the participation of an eligible caregiver (person with whom the child/adolescent spends at least 50% of his or her time and had responsibility for overseeing diabetes management). Exclusion criteria included not actually initiating pump therapy, having a co-occurring untreated chronic illness affecting weight (eg gastrointestinal or adrenal disorder), severe psychiatric illness (eg, bipolar disorder), and pregnancy. Eligible participants were recruited for this cross-sectional study and entered in sequential fashion at 3 different sites: Georgia Health Sciences University in Augusta, Georgia; Emory University in Atlanta, Georgia; and Joslin Diabetes Center in Boston, Massachusetts. IRBs at the 3 participating institutions approved the protocol. Following written informed consent/assent, participants and parents completed surveys.
Children and their parents were enrolled within 10 days of initial diagnosis of T1D or 10 days of initiating pump treatment. Once eligible participants were identified, staff referred them to a site-specific research assistant who conducted an eligibility screening and obtained informed consent/assent. Baseline assessment, which was conducted during a home visit, clinic visit, or in the hospital, provided data for the current study. New participants were evaluated within 10 days of initial diagnosis to capture endorsement of bulimic symptoms associated with disease onset without the effects of treatment. Pump participants received their baseline evaluation prior to actual insulin administration utilizing the pump, reflecting levels of bulimic symptoms before pump treatment.
Measures
Eating Disorder Inventory–III (EDI-III)
The EDI-III is a 91-item self-report measure of clinically relevant cognitions and behaviors specific to DEB. It consists of 12 independent standardized subscales: Drive for Thinness, Bulimia, Body Dissatisfaction, Low Self-Esteem, Personal Alienation, Interpersonal Insecurity, Interpersonal Alienation, Interoceptive Deficits, Emotional Dysregulation, Perfectionism, Ascetisism, and Maturity Fears. Participants rate their level of agreement with items on a 6-point Likert-type scale (ranging from “always” to “never”). Questions ask the individual to evaluate himself or herself in the present, indicating how often they exhibit specified symptoms (“I experience marked mood shifts”; Emotion Regulation scale), behaviors (“I eat and drink in secrecy”; Bulimia scale), and cognitions (“I think about overeating”; Bulimia scale). Subscales used for these analyses were the bulimia and emotion dysregulation subscales. 29 The bulimia subscale consists of 8 items with scores ranging from 0 to 32. Higher endorsement on the bulimia scale indicates more DEB. The emotion dysregulation scale consists of 8 items with scores ranging from 0 to 32. Higher endorsement of items on the emotion dysregulation scale indicates poor coping in response to negative mood. Internal consistency was acceptable for the bulimia subscale (α = .83) and body image dissatisfaction subscale (α = .80) in the current sample. Acceptable convergent validity for the EDI-III has been established in prior studies. 30
The Children’s Depression Inventory (CDI)
The CDI is used to assess cognitive, affective, and behavioral signs of depressive symptoms in children and adolescents aged 6-17 years old during the previous 2 weeks. The CDI self-report measure consists of 27 items and has 5 subscales, including negative mood, interpersonal difficulties, ineffectiveness, anhedonia, and negative self- esteem. For the purposes of this study, a total score was calculated. A total score of ≥13 is indicative of clinically elevated depressive symptoms. Internal consistency for the CDI ranges from .71 to .89 and the test retest coefficients range from .74 to .83. 31 In the current study, reliability for the CDI was acceptable, α = .80.
Hemoglobin A1c
Laboratory values were obtained from the participants’ medical charts. Because participants were recruited from 3 sites, assay methods were not standardized. However, site was used in all analyses as a covariate to account for potential variation in values (as well as other possible site based differences). All sites used the methods that were standardized to the DCCT assay. 32
BMI
Height and weight were obtained from the participants’ charts or measured at the time of the study visit. Height (to the nearest 0.1cm) and weight were assessed 3 times, and averaged, if obtained by a research assistant. Age and sex-adjusted BMI (BMI z-score standard deviation [z-BMI] based on the Centers for Disease Control and Prevention [CDC] growth charts) were calculated. 33
Length of illness
Time since diagnosis and baseline evaluation was assessed via medical chart review.
Data Analytic Strategy
Analyses were conducted using PASW Statistics 18, Release Version 18.0.0 (D3 SPSS, Inc, Chicago, IL, 2009, www.spss.com). Bivariate correlations were examined between all variables in each group. In addition, demographic variables, such as ethnicity and site, were compared between each group using independent t-tests and chi-square analyses. Independent samples t-tests were also used to compare the rate of bulimic symptom endorsement and z-BMI in each group. To examine the relative contributions of depressive symptoms and emotion regulation to bulimic symptoms, we conducted hierarchical linear regressions. Two models were tested: 1 for newly diagnosed participants, and 1 for participants transitioning to CSII. Participant sex, age, z-BMI, A1c, and site were entered in the first step. Only data from participants with a concurrent A1c value (n = 87) were analyzed in regression models (Pump = 43, New = 44). Of note, there were no differences between participants included in analyses with A1c values versus those who were not included because they did not have A1c data. Length of illness, depressive symptoms, and emotion dysregulation were entered in the second step. The interaction of depression and emotion dysregulation was entered in the third step of the model. To reduce multicollinearity impacting interaction terms, following the recommendations of Cohen, 34 CDI scores and emotion dysregulation scores were centered. Finally, simple slope analyses were conducted to probe significant interactions. 35
Results
Table 1 provides participant characteristics and questionnaire results by group. The Pump group had significantly higher mean z-BMI (t = 3.12, P < .05) and a greater proportion of Caucasian participants (χ2[100] = 9.59, P < .01) than the New group. Regarding site differences, patients from Georgia Health Sciences University (GRU) and Joslin differed significantly on symptoms of bulimia: GRU participants had significantly higher z-BMI, A1c, and endorsed higher levels of bulimic symptoms (t = 2.76, P < .01). Bivariate correlations for the New and Pump participants are presented in Table 2.
Descriptive Statistics of Major Study Variables.
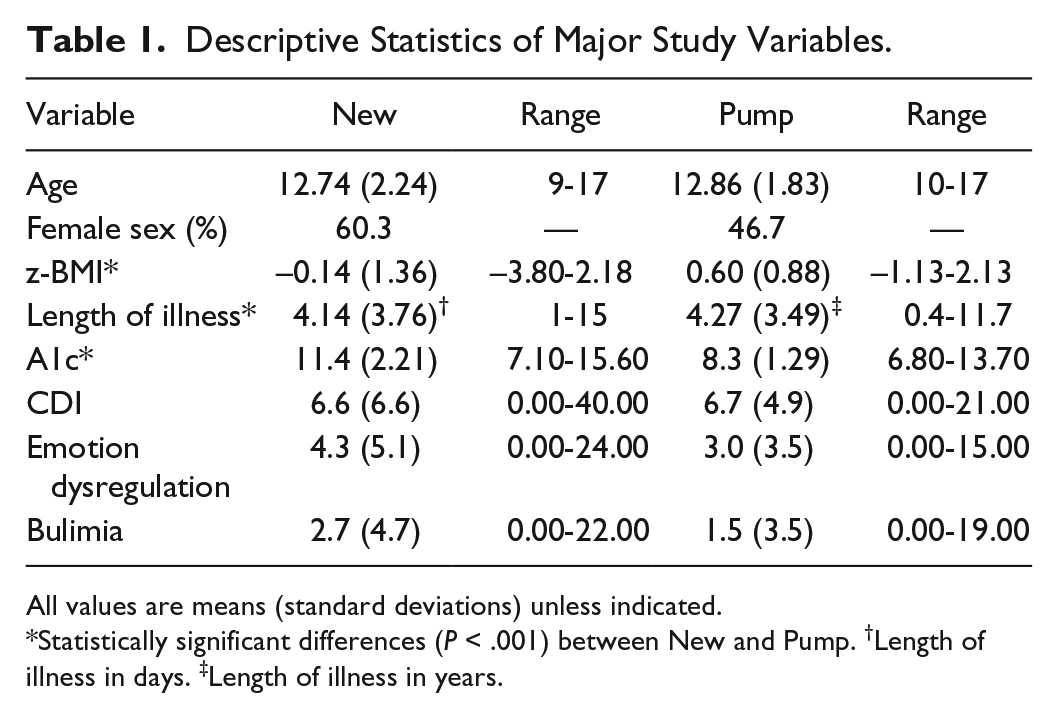
All values are means (standard deviations) unless indicated.
Statistically significant differences (P < .001) between New and Pump. †Length of illness in days. ‡Length of illness in years.
Correlations of Major Study Variables for Combined Sample: New (n = 58) and Pump (n = 43).
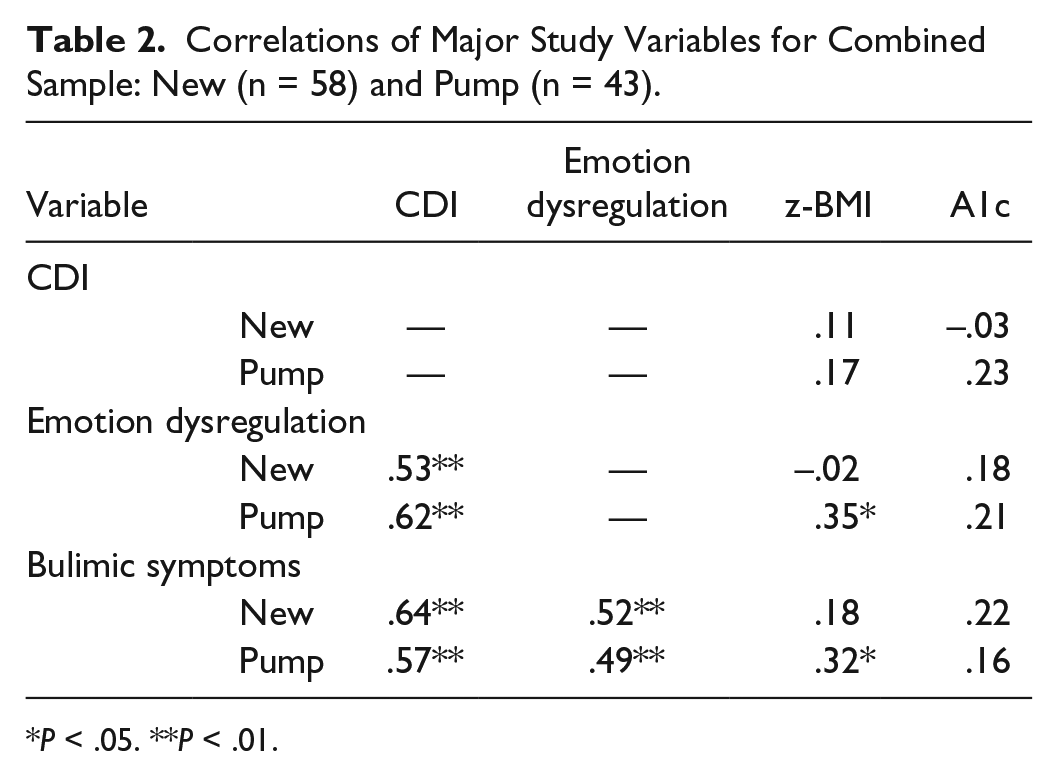
P < .05. **P < .01.
Regression of Depressive Symptoms and Emotion Dysregulation in the Newly Diagnosed Group
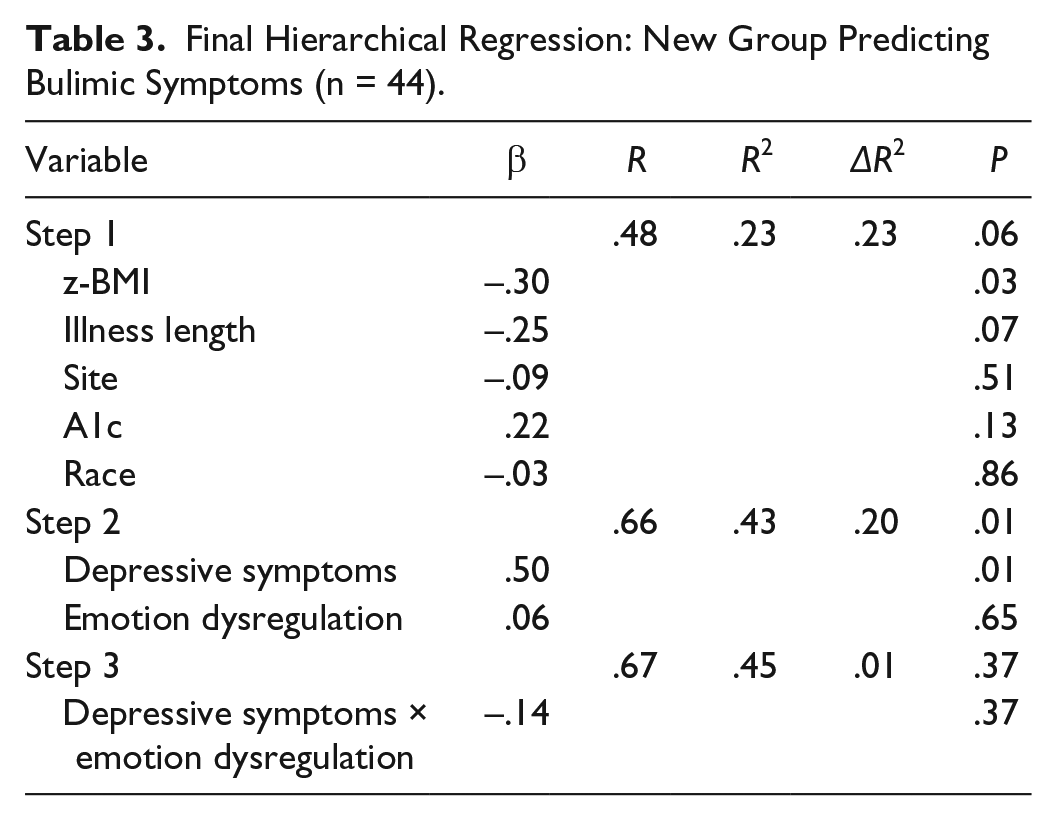
In the last step of the model for the New group (R2 = 45%) (which included all variables), z-BMI contributed significantly to endorsement of bulimic symptoms (β = –.30, P < .03) such that lower z-BMI in newly diagnosed youth was associated with higher endorsement of bulimic symptoms. Examination of the beta weights indicated that depression had a significant, unique effect on bulimic symptoms (β = .50, P < .001). Emotion dysregulation and site were not significant predictors of bulimic symptoms, and there were no significant interaction effects (see Table 3).
Final Hierarchical Regression: New Group Predicting Bulimic Symptoms (n = 44).
Regression of Depressive Symptoms and Emotion Dysregulation in the Pump Transition Group
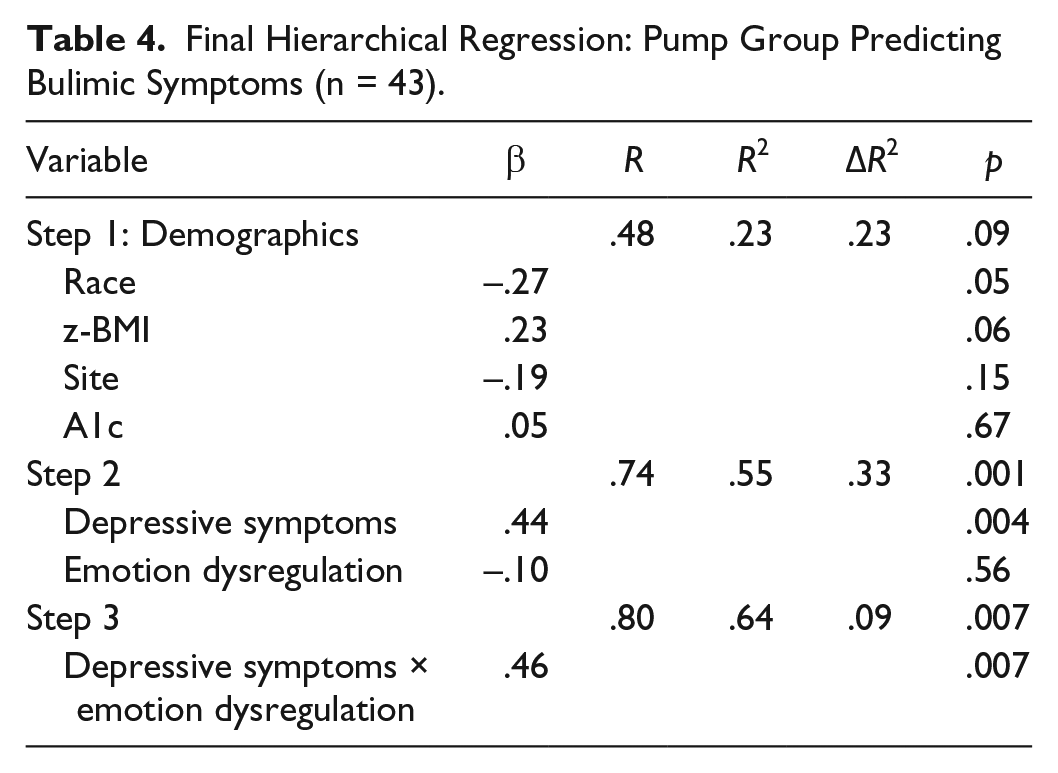
The regression model was replicated in the Pump group (R2 = 64%, P < .007). Site (β = –.34, P < .04) and z-BMI score (β = .34, P < .03) made significant contributions to bulimic symptoms in the first step of the model. When psychological risks were added to the model, race became significant (β = –.32, P < .03), site remained significant, but z-BMI became nonsignificant. In the final model, the interaction between depressive symptoms and emotion dysregulation contributed significant unique variance to bulimia scores (β = .46, P < .007). Simple slopes were tested for the relationship of depressive symptoms to bulimic symptoms at levels of emotion dysregulation at 1 standard deviation below the mean, at the mean, and 1 standard deviation above the mean. This analysis revealed that at low levels of emotion dysregulation, depressive symptoms were not associated with bulimic symptoms (t = 1.52, p = .14). However, at mean (t = 3.52, P < .001) and high (t = 3.14, P < .003) levels of emotion dysregulation, depression was significantly associated with bulimic symptoms. Pump youth with high levels of both depressive symptoms and emotion dysregulation endorsed the highest rates of bulimic symptoms (see Table 4 and Figure 1).
Final Hierarchical Regression: Pump Group Predicting Bulimic Symptoms (n = 43).
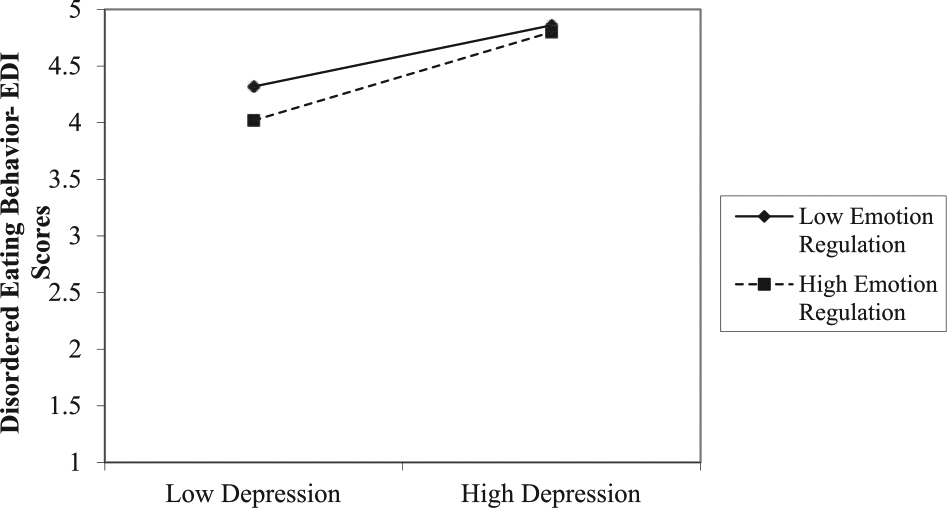
Interaction of depressive symptoms, emotion regulation, and disordered eating behavior.
Discussion
This study examined associations between z-BMI, bulimic symptoms, depressive symptoms and emotion dysregulation in 2 distinct groups: patients who were newly diagnosed with T1D and established patients transitioning to a pump regimen. Replicating previous studies, there were no statistically significant differences between the 2 groups on endorsement of bulimic symptoms.13,14 For youth with treatment experience about to transition to pump, the influence of depressive symptoms was moderated by emotion dysregulation such that the interaction between higher depressive symptoms and emotional dysregulation amplified adoption of DEB. This implies that established patients with T1D with higher BMI who are experiencing greater depressive symptoms and emotion dysregulation are more likely to engage in DEB.
Since hypoglycemia is associated with negative mood states and poor emotion regulation,27,28 the interaction of these mechanisms could help to explain the link between poor glycemic control/negative health consequences associated with DEB.2,8 For established patients, loss of residual β-cell function could be expected to make glycemic and weight control more difficult. 36 Furthermore, weight gain is a common side effect of insulin treatment that can promote weight concerns. 37 For youth with depressive symptoms and emotion dysregulation, they may be more likely to engage in DEB.15,27 A recent study demonstrated that DEB decreased over 6 months in a sample of youth who had transitioned to an insulin pump suggesting that the insulin pump may help mitigate DEB and normalize eating patterns. 15 Our findings suggest the importance of screening for DEB in youth with T1D, particularly during this transition from MDI regimens to an insulin pump. This period of time after the individual has been living with the illness and managing using an MDI regimen appears to be a time of risk for DEB, particularly with a higher BMI, and concurrent depressive symptoms and emotion dysregulation.
There are several implications of these findings regarding treatment of bulimic symptoms in youth with T1D. In individuals without diabetes, emotion regulation skill building has been shown to be effective in decreasing bulimic symptoms.38,39 Studies suggest binge eating serves as an emotion regulation process by which binging serves to decrease negative affect.8,9 However, in addition to experiencing negative emotion (ie, higher rates of depressive symptoms), individuals with T1D also experience a dysregulation of appetite and satiety due to hormonal deficits (eg, amylin), excessive insulin, and fluctuations in blood glucose. 12 Current findings that depressive symptoms and loss of control over emotion regulation both contribute to endorsement of bulimic symptoms suggest education regarding expected loss of cues regarding hunger and satiety related to disease processes may reduce associated distress, helping to prevent adoption of bulimic symptoms as a maladaptive coping mechanism. 40 Cognitive behavioral therapy (CBT), which has been found to be effective in patients with eating disorders but without diabetes, 41 could prove effective in this population. Importantly, CBT would need to be modified to address the physiology of disease processes and treatment effects. Specifically, treatment should focus on promotion of more flexible eating patterns (while adhering to T1D treatment regimen), and decreasing the frequency of underdosing insulin. CBT would also need to address the role of diabetes distress within the context of DEB in youth with T1D. Current recommendations for treatment of co-occurring DEB and T1D include the use of a multidisciplinary team approach (eg, endocrinologist, nurse educator, dietician, and psychologist/social worker). 42 Furthermore, patient may require inpatient hospitalization to ensure medical stability prior to initiating outpatient treatment with a multidisciplinary team. 42
Given the cross-sectional nature of our analyses, results should be interpreted with caution since cross-sectional data cannot determine directionality or causality. Another weakness of the current study was due to lack of experience with diabetes treatment (our New group), a diabetes-specific measure of DEB, such as the Diabetes Eating Problems Survey-Revised (DEPS-R), 43 could not be used with the New group for their baseline evaluation. Although we used a well validated screening measure, the EDI-III, this measure is not normed in youth with T1D and is a weakness of the current study. Other limitations of the current study included no measurement of within group differences in regimen behaviors (eg, dosage/frequency of insulin administration) as these indices were in flux. We also did not directly measures β-cell function, which could address issues regarding ease of management and control of appetite. It is also likely that youth desiring a pump are not representative of all youth with T1D. It is important to note that although we hypothesized that the mechanisms of action between increased depressive symptoms and emotion dysregulation include hypoglycemia, this hypothesis was not tested in this study. Thus, future studies need to examine such variables in conjunction with DEB, depressive symptoms, and emotion dysregulation. Finally, it may have been that our New and Pump groups were underpowered to find significant associations within and between groups as they were small samples. It remains, however, that these data suggest evaluation of depressive symptoms and emotion dysregulation in youth with T1D as they transition to pump would be helpful when ascertaining the risk for DEB in this population, and provide opportunity for targeted intervention.
Results from this study present novel information regarding the roles of depressive symptoms and emotion dysregulation on bulimic symptoms in boys and girls who are newly diagnosed with T1D and youth with T1D before transitioning to pump. Youth who have been living with T1D and are about to transition to pump appear to be more vulnerable to DEB when they have concurrent depressive symptoms and emotion dysregulation. Future prospective studies are needed to test the contributions of emotion dysregulation and depressive symptoms to the development of bulimic symptoms in youth over the course of the disease. As noted by Colton et al, 1 DEB symptoms tend to increase with age in those patients who develop them. The current study is an important first step in understanding the effects of depressive symptoms and emotion dysregulation on risk for DEB in youth with T1D in the context of disease onset and treatment.
Footnotes
Abbreviations
A1c, hemoglobin A1c; CBT, cognitive behavioral therapy; CDC, Centers for Disease Control and Prevention; CDI, Children’s Depression Inventory; CSII, continuous subcutaneous insulin infusion; DCCT, Diabetes Control and Complications Trial; DEB, disordered eating behavior; EDI-III, Eating Disorder Inventory–III; GRU, Georgia Health Sciences University; MDI, multiple daily injections; New, newly diagnosed; Pump, transitioning to pump regimen; T1D, type 1 diabetes; z-BMI, body mass index z-score.
Authors’ Note
DLYH was at the Georgia Regents University when the work for this article was performed. The findings and conclusions in this article are those of the authors and should not be construed to represent the views of the Office of Behavioral and Social Science Research or the National Institutes of Health.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by American Diabetes Association grant 07-08-CR66, DLYH (PI).