
Abstract
Objective:
Adherence to type 1 diabetes management declines as children enter adolescence. For youth, psychosocial variables including mood and interpersonal relationships play a large role in diabetes maintenance. The current study assessed the unique and interactive roles diabetes family conflict and depression have on insulin bolusing behaviors for youth ages 10-16 years.
Methods:
Ninety-one youth-parent dyads completed a survey assessing family conflict and depression. Mean daily blood glucose levels, mealtime insulin bolus scores (BOLUS), and glycated hemoglobin (HbA1c) were collected from the medical record as outcome variables.
Results:
Parent-reported diabetes-related family conflict and youths’ endorsed depression both significantly predicted insulin bolusing behavior, R2 = .13, F(2, 88) = 6.66, P < .05. The interaction of diabetes family conflict and youth depression played a significant role in youths’ bolusing behaviors, above and beyond that which was predicted by conflict and depression separately, R2 = .18, Fchange(1, 87) = 4.63, P < .05. BOLUS was negatively related to youths’ hemoglobin A1c, r = –.556, P < .001 and mean daily blood glucose levels, r = –.428, P < .001.
Conclusions:
Among depressed youth, mealtime insulin BOLUS scores declined with greater diabetes-related family conflict, while there was no change in BOLUS scores among depressed youth living in families reporting less conflict. Findings underscore the importance of screening for depression and family conflict in youth experiencing or at risk for poor adherence to mealtime insulin and higher HbA1c levels.
Adolescence and preadolescence can be an especially difficult time for patients with type 1 diabetes mellitus (T1DM) who are not only encumbered with the academic and social demands inherent in these developmental periods, but also managing T1DM.1,2 Frequently, hormonal changes during puberty result in varying blood glucose levels and insulin needs, 3 requiring youth to make frequent BG observations and adjust accordingly. Likewise, these developmental periods bring about change in those responsible for managing T1DM, as parents begin to pass primary responsibility to their children. 4 This shift in responsibility can interfere with a youth’s relationship with his or her parents, causing family conflict and declines in diabetes outcomes. 5 In fact, numerous studies have shown that increased levels of diabetes family conflict are associated with higher glycated hemoglobin (HbA1c) levels,6,7 less frequent blood glucose monitoring, 8 and poorer overall glycemic control. 9
Youth diagnosed with T1DM have also been shown to be more at risk for depression, 2 which is predictive of poorer adherence, especially if there is also a higher level of family conflict reported.10-12 While technology may play a role in mediating the relation between psychosocial factors and adherence, research is still needed in this area.13,14 Common devices used in T1DM management are blood glucose monitors and insulin pumps. 15 Several studies have already shown relations between youth psychosocial and social functioning and their adherence to frequency of blood glucose monitoring, a popular objective measure of T1DM adherence. 8 Furthermore, at least 1 study has demonstrated the mediating effect blood glucose monitoring has on family conflict and HbA1c. 16 However, comparatively less research is available examining relations between psychosocial and social functioning and youths’ adherence to insulin. Appropriate insulin use is a key component of diabetes management. 3 Moreover, studies now show that youths’ adherence to mealtime insulin boluses is more strongly related to their HbA1c levels than frequency of blood glucose monitoring. 17 Taken together, these suggest a need for research on factors that impact behaviors surrounding insulin and dosing. Recently, an objective measure of youths’ mealtime insulin use was validated making it possible to conduct this formative research. 17 Therefore, the aim of this study was to investigate the effects diabetes-related family conflict and youth depression have on insulin use in youth with T1DM. Specifically, investigators hypothesized that patients with high levels of either family conflict or depression would demonstrate less frequent mealtime insulin use. A second hypothesis was that high levels of depression and family conflict would have an interactive effect on youths’ mealtime insulin use.
Method
Participants, Recruitment, and Inclusion Criteria
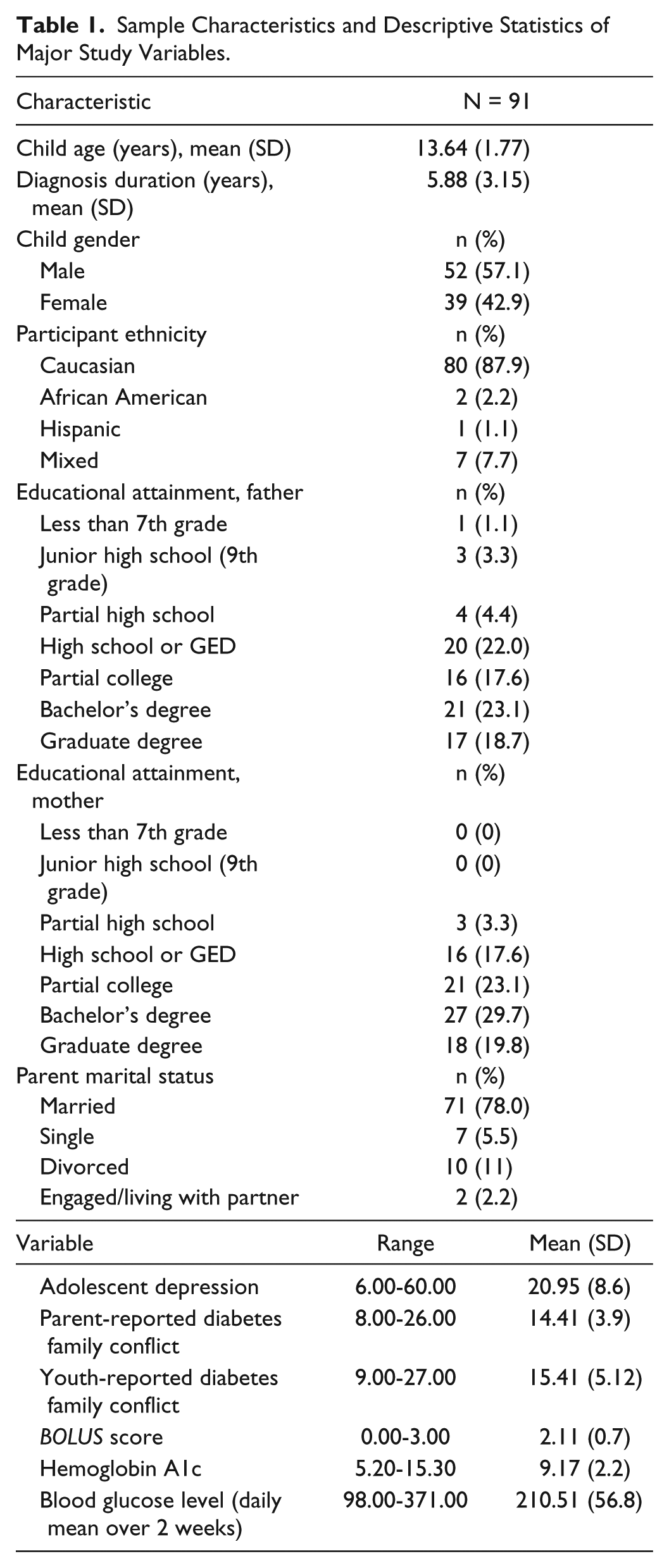
The sample was selected from a larger subset of 137 parent-youth dyads. Parent-youth dyads were eligible to participate in the larger study if youth were between the ages of 10-16 years old (an age range selected to ensure inclusion of youth transitioning from preadolescence to adolescence), youth had been diagnosed with T1DM for at least 6 months, and the family was English speaking. Families were excluded if youth had a diagnosis of developmental delay (ie, autism, cerebral palsy, or intellectual disability) or if youth or parents reported hospitalization within the last year for a psychological disorder. Parent-youth dyads were recruited from pediatric diabetes clinics affiliated with 2 large metropolitan hospitals during a clinic visit. For the current sample, families (N = 91) were selected because the youth was using an insulin pump for daily diabetes management. There were no systematic differences between the current sample and the larger subset of 137 parent-youth dyads. See Table 1 for sample demographic characteristics.
Sample Characteristics and Descriptive Statistics of Major Study Variables.
Procedure
The study was approved by the Institutional Review Boards at Children’s Mercy Kansas City and the University of Kansas Medical Center. Following recruitment and informed consent and youth assent, parent-youth dyads accessed a secured internet study website to separately complete measures of depression and family conflict via iPads during a routine diabetes clinic appointment. HbA1c, mean daily blood glucose levels, and insulin pump data were obtained during that same clinic appointment from a medical chart review or device downloads, respectively. Parent and youth were both compensated $25 for their participation.
Measures
Youth Depression
The Center for Epidemiologic Studies–Depression Scale (CES-D) 18 is a 20-item questionnaire that assesses for depressive symptoms. Responders indicate the frequency with which they experienced each symptom on a scale of 0 (none of the time) to 3 (all of the time) over the past week. Scores range from 0 to 60, with scores over 16 suggesting some difficulty with depression and scores over 21 suggesting the possibility of major depression. The scale has been validated for use with children and adolescents. 19 The reliability coefficient in the current sample was .80, indicating good internal consistency.
Diabetes-Related Family Conflict
The Diabetes Family Conflict Scale (DFCS) 20 is a recently revised 19 item questionnaire that measures perceptions of family conflict. Parents and adolescents independently completed the questionnaire. They were asked to indicate the frequency of occurrence of items using a 3-point Likert-type scale (1 = never argue, 2 = sometimes argue, and 3 = always argue). Only the 9 items specific to diabetes care on the Direct Management Tasks subscale were used in the present analyses. The reliability coefficients for this subscale were .88 and .96 for parents and youth, respectively, indicating good internal consistency.
Bolus Behavior
Youths’ mealtime insulin BOLUS score was calculated from their insulin pump records. Consistent with established scoring procedures, 17 youth received 1 point for each mealtime bolus occurring between 0600 and 1000, 1100 and 1500, and 1600 and 2200, for a total possible of 3.0 points per day. These daily scores were then averaged over 14 days to calculate the BOLUS score.
Demographic Information
Youth reported their age, gender, ethnicity, and time since diabetes diagnosis. Parents reported on their education level, marital status, employment status, and job type. Means, standard deviations, and frequencies were calculated for all the demographic variables.
Results
The statistical analyses were performed using Statistical Package for the Social Sciences (SPSS) Software Version 23 (2014, IBM Corp, Aramonk, NY). Prior to analysis, data were screened to ensure that assumptions of univariate and multivariate analysis had not been violated. Preliminary analyses showed a mean HbA1c of 9.17 ± 2.16% and a mean daily blood glucose of 210.5 ± 56.8mg/dl for youth. Youths’ average BOLUS score was 2.12 ± .7, suggesting they only dosed for slightly over 2 meals per day. Sixty-nine youth (75.8%) scored equal to or greater than 16 on the CES-D, with 35 (38.4%) scoring above the clinical cutoff score of 21. The mean HbA1c and parent-reported diabetes family conflict for the current sample was similar to those found in other studies.8,16 See Table 1 for descriptive statistics of the other main variables.
Preliminary bivariate correlations (see Table 2) showed that the mealtime BOLUS was inversely related to youths’ HbA1c, r = –.556, P < .001 and mean daily blood glucose levels, r = –.428, P < .001, suggesting that better adherence to mealtime insulin use was related to better glycemic control (ie, glucose levels decrease). Correlations also showed that while youth age was inversely related to the mealtime BOLUS score, r = –.286, P < .01 and HbA1c, r = .371, P < .01, it was not significantly related to youth depression or parent and youth reporting of diabetes family conflict. Neither ethnicity nor sex were related to BOLUS score. Thus, age, sex, and ethnicity were not controlled for in the study’s main analyses.
Pearson Coefficients of Study Variables.
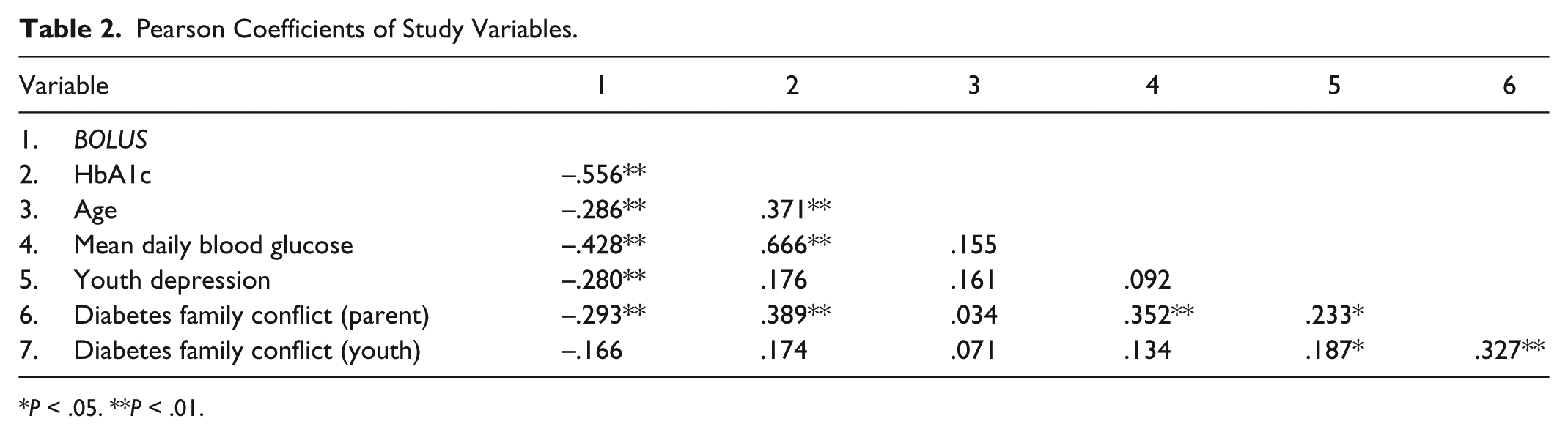
P < .05. **P < .01.
Hypothesis 1 was examined via Pearson correlations. While the mealtime BOLUS score did not relate to youth-perceived diabetes family conflict, results showed that it was inversely correlated with both youth depression, r = .280, P < .01 and parent-endorsed diabetes family conflict, r = –.293, P < .01, lending support to the hypothesis.
Because significant correlations were observed between the variables, multicollinearity statistics were examined for the main study variables prior to running the primary regression analysis. These were within the normal range (VIF = 1.073; Tolerance = .932). Therefore, to test hypothesis 2, a multiple regression analysis was conducted to predict youths’ bolusing behaviors based on their level of depression and parents’ endorsed level of diabetes family conflict. The results indicated that depression and parent-perceived family conflict accounted for a significant amount of youth bolusing behavior variability, R2 = .13, F(2, 88) = 6.66, P < .05. A second regression was conducted to determine whether or not there was an interactive effect of depression and family conflict on youths’ bolusing behaviors and this regression was also significant, R2 = .18, Fchange(1, 87) = 4.63, P < .05 (see Figure 1). Specifically, youth with higher levels of depression showed greater decline in their mealtime BOLUS score as parent-perceived diabetes family conflict increased (P < .05), while there was no change in mealtime BOLUS scores for depressed youth with low parent-perceived diabetes family conflict. See Table 3 for the regression coefficients.
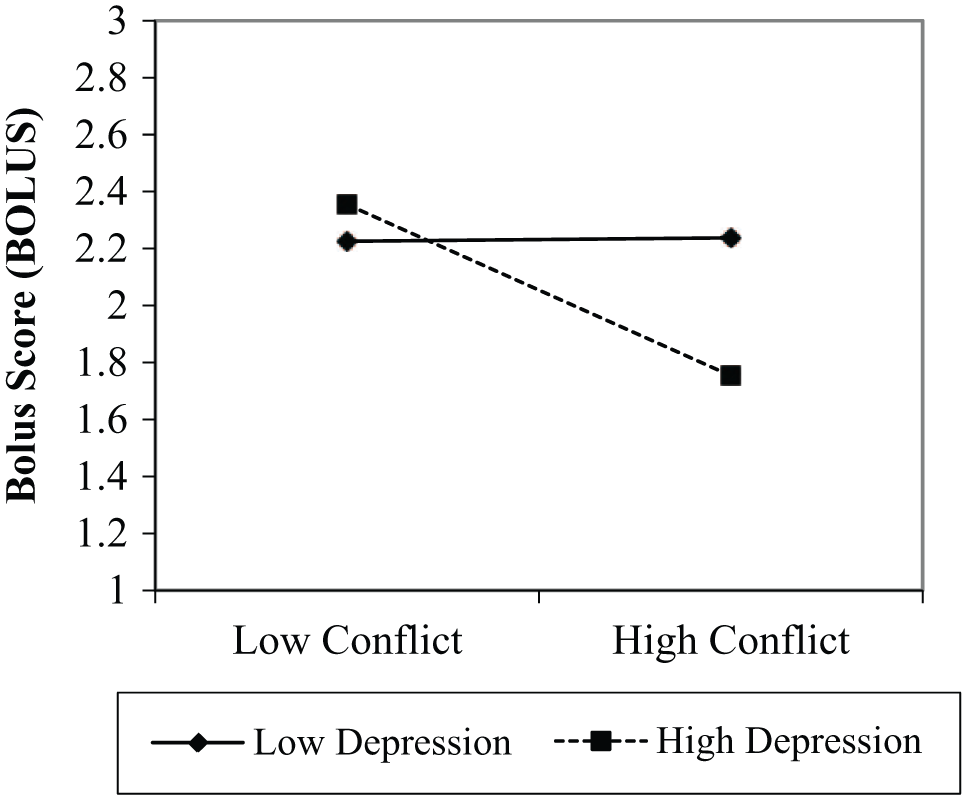
Interaction of youth depression and diabetes family conflict on BOLUS score.
Results of Regressing Centered Youth Depression and Diabetes Family Conflict on BOLUS score.
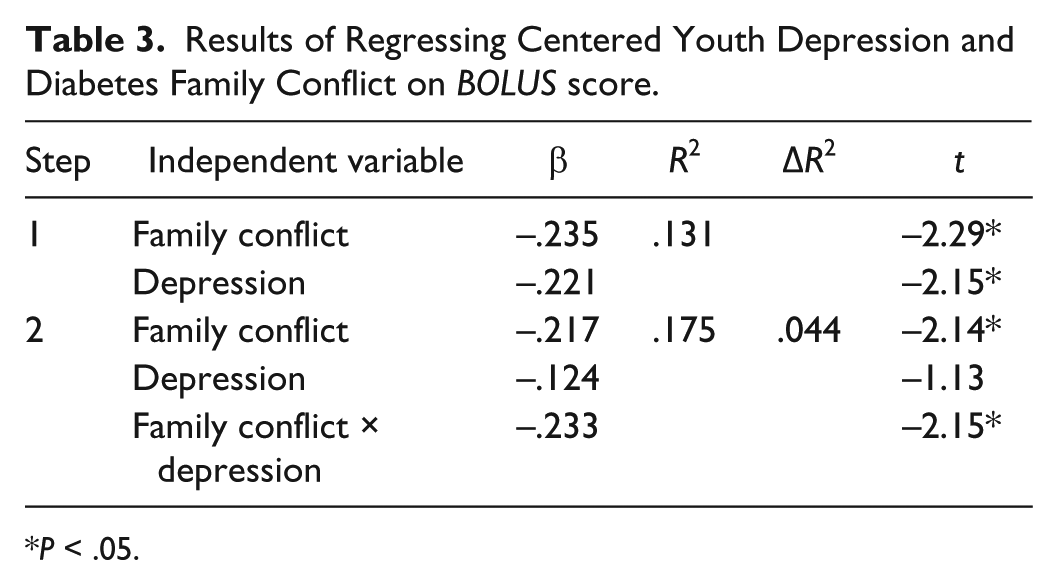
P < .05.
Discussion
While data collected by the T1 Diabetes Exchange suggests that a majority of youth in the United States use an insulin pump for daily management, 21 the research examining psychosocial and social predictors of insulin adherence has lagged behind. The current study begins to address this gap by examining the associations of family conflict and youth depression to youths’ adherence to mealtime insulin bolusing. Findings demonstrated that both parent-perceived diabetes family conflict and youth depression resulted in worse adherence to youth mealtime bolusing. Results also showed that these variables had an interactive effect, suggesting that youth with high levels of depression and who lived in a family where parents perceived a high degree of diabetes family conflict demonstrated worse adherence behavior than youth with high depression and low parent-perceived family conflict. Specifically, in the presence of high depression and high family conflict, youth adherence dropped by almost 1 full mealtime bolus per day. However, findings also demonstrated that even in low conflict environments, youth with depression tended only to bolus for 2 meals per day, which is suboptimal. One potential caution in our results is the relatively low percentage of variability in youths’ BOLUS score accounted for by depression and family conflict. Yet we would assert our findings are still significant because depression and family conflict are both modifiable and because past research has shown a 1.5% decrease in youths’ HbA1c level for every 1-point increase in youths’ BOLUS score, 22 indicating that a decrease in family conflict and youth depression could have a potentially important clinical impact in youth.
Our present results are consistent with previous research showing that depression and diabetes family conflict both result in poorer HbA1c levels.2,10,12 In addition, our results are consistent with the studies which have shown a relation between depression, family conflict, and poorer adherence, as measured by frequency of BG checks and self-report.8,10,12 However, our focus on youths’ adherence to insulin use may improve on these past studies by providing a more accurate measure of adherence. Unlike frequency of BG checks, measuring adherence using the mealtime BOLUS score may be more accurate because youth are more likely to have their insulin pumps with them when they attend clinic, but could forget to bring all of their glucometers to clinic potentially leading to gaps in these data and seemingly lower adherence rates. Similarly, because the mealtime BOLUS score is an objective measure of adherence, it is unlikely to be vulnerable to response bias, which is a problem with self-report.
One unexpected finding was the lack of an association between youths’ perception of diabetes family conflict and their BOLUS score. It is unclear why this occurred, especially considering the significant correlation between youths’ and parents’ conflict scores. One potential explanation could be that parents, when completing the DFCS, focused on any conflict that arose from reminding their child to bolus at a meal, thus making their conflict scores more directly related to the BOLUS. However, it is also possible youths’ perception of family conflict was simply independent of their adherence and a product of some other psychosocial or developmental factor leading to the lack of relation between these 2 variables. It is important to note that youth-perceived family conflict showed more variability than parent-reported conflict. Although it was still normally distributed, the greater variability could also have reduced its association to a behavior as specific as bolusing, leading to the lack of significant relationship.
Implications for Treatment
The current study provides additional impetus for routine clinical screening of depression and intervention especially if high family conflict is also detected. As increased family conflict is often a symptom of youth depression, we would suggest that providers initially target depression in their regular screenings. Medical providers who identify youth with combined depression and family conflict should do all they can to address conflict and poor communication during medical visits, while providing families with a referral for mental health treatment. Health care teams should also work together to use problem-focused strategies to reduce depression and conflict for at-risk families. Improvements in adherence that result from such interventions could be maintained by setting appropriate behavioral goals during clinic visits and providing reinforcement to families.
Another important implication is the use of the mealtime BOLUS as an objective measure of diabetes adherence. Because of the specificity of the BOLUS, providers could directly target interventions to promote increased adherence to mealtime bolusing overall or even target better adherence to specific meals for which youth appear to have more difficulty remembering to bolus. Doing so could allow for setting more realistic and attainable short-term goals that would provide families with frequent feedback, as opposed to waiting months for a new HbA1c. The mealtime BOLUS is simple to calculate and easy to deploy in a clinic setting. It can also be a good predictor of youths’ clinical outcomes because of its closer relation to current and future HbA1c than frequency of BG monitoring.17,22
Strengths, Limitations, and Future Research
A strength of the study is that the clinics from which the sample was recruited do not require youth to have a predetermined HbA1c level to obtain an insulin pump. This allowed for maximum variability in adherence and HbA1c levels in our sample and likely reduced the risk of bias related to a selective sample. Another strength is our use of an objective measure of youth adherence by employing the mealtime BOLUS, which has also been previously shown to be valid and reliable in youth.17,22 That being said, this study only included youth on insulin pumps, so the results may not generalize to youth using a pen or syringe for daily insulin use. Another limitation is the homogeneous sample. Although the sample was large, the majority of participants identified as non-Hispanic white, which limits generalizability to other ethnic groups. Nevertheless, the current sample was demographically similar to the clinic from which it was drawn and the general US population, which has a higher rate of T1DM in non-Hispanic white individuals than in minority groups. 23 Therefore, future research is needed to recruit participants of varying ethnic and racial backgrounds to attain better generalizability. This study may be limited by its use of self-reported depression and family conflict because self-report is vulnerable to reporting bias. Indeed, there is some concern of a reporting or selection bias, as the majority of youth self-reported either mild or moderate depressive symptoms on the CES-D. Future research is needed to provide additional confirmation of the relation between family conflict, youth depression, and diabetes adherence, perhaps using a different measure of youth depression. Finally, this study is limited because of its cross-sectional design, which prevents an examination of causation among the study variables.
Conclusions
This study finds that youth who experience high levels of depression and live in families with a higher level of diabetes-related family conflict are more at risk for poor adherence to mealtime bolusing than youth who struggle with depression alone. This is the first study to assess depression and family conflict in relation to the BOLUS score, and findings provide impetus for further research into psychosocial variables that impact bolusing behavior. Providing appropriate psychological referrals and brief conflict reduction interventions would benefit youth who struggle with depression and especially youth with depression who also live in highly conflicted family environments.
Footnotes
Acknowledgements
The authors would like to acknowledge all of the families who volunteered to participate in the current study.
Abbreviations
BOLUS, mealtime insulin bolus score; CES-D, Center for Epidemiologic Studies–Depression Scale; DFCS, Diabetes Family Conflict Scale; HbA1c, glycated hemoglobin; T1DM, type 1 diabetes mellitus.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors would like to acknowledge funding from the University of Kansas Diabetes Institute.