
Abstract
Keywords
The prevalence of depression in patients with type 1 diabetes mellitus (T1D) is increasing toward a global epidemic. Depression is associated with poor self-care, erratic dietary adherence, higher risk of microvascular disease as well as premature mortality. 1 Selective serotonin reuptake inhibitors (SSRIs) are commonly used for treatment, but they are linked to a greater risk of diabetes and related complications. 2
We describe a 26-year-old female with chronic anorexia and bingeing who had been prescribed high doses of 2 SSRIs for several years. A weight gain of 10 pounds and elevated serum glucose levels signified onset of T1D. She was treated with a sliding scale of Lantus and Humalog insulin, but her blood glucose showed wide variations. She became overwhelmed with depression and confined herself to a treatment center.
At the initial presentation, she was an ectomorphic, menstruating female with BMI of 22. There was no family history of diabetes. Insomniac and inattentive since latency years, she had found temporary relief by bingeing or running. Her resting state blood pressure was 91/57 mm/Hg and the pulse rate was 53 beats/minute. Cognitive exams showed sub-optimal function. Her fasting blood glucose (FBS) was at 438-mg/dl and glycated hemoglobin (HbA1c) at 119 mmol/mol (13%).
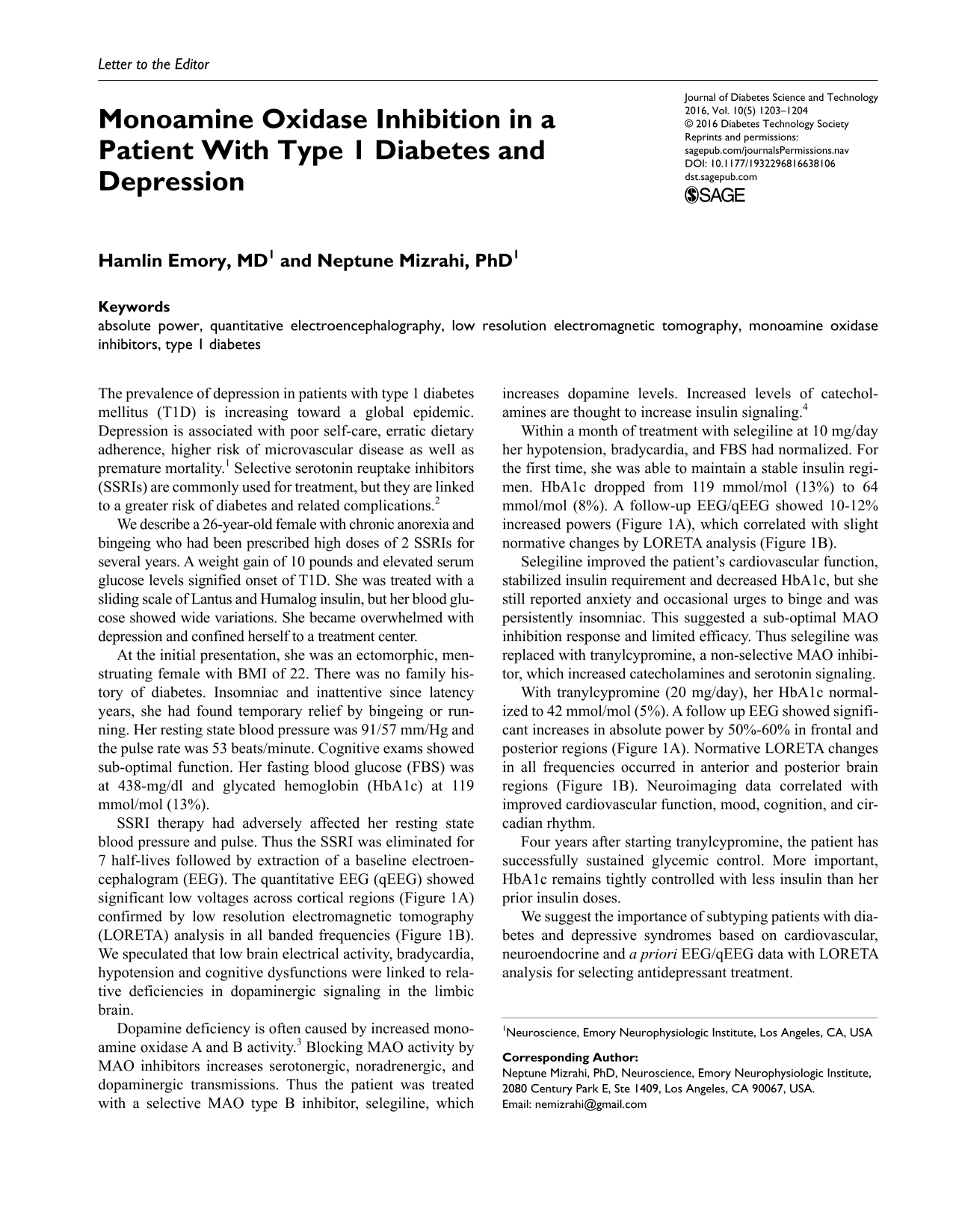
SSRI therapy had adversely affected her resting state blood pressure and pulse. Thus the SSRI was eliminated for 7 half-lives followed by extraction of a baseline electroencephalogram (EEG). The quantitative EEG (qEEG) showed significant low voltages across cortical regions (Figure 1A) confirmed by low resolution electromagnetic tomography (LORETA) analysis in all banded frequencies (Figure 1B). We speculated that low brain electrical activity, bradycardia, hypotension and cognitive dysfunctions were linked to relative deficiencies in dopaminergic signaling in the limbic brain.
qEEG and LORETA analysis before and with MAO inhibitors treatment. (A) Graph showing differences in qEEG absolute power defined as the total power in the EEG frequency bands at each electrode. Z-scores show the differences between baseline and treatment with selegiline or tranylcypromine. (B) Three-dimensional images showing current density in Talairach space obtained by LORETA for baseline (BL), selegiline (SLG), and tranylcypromine (TCP). Differences in 7 frequency bands (delta: 1 Hz, theta: 7 Hz, alpha1: 8Hz, alpha2: 10 Hz, beta1: 18 Hz, beta2: 21 Hz, and beta3: 29 Hz) are shown. Blue areas correspond to brain’s reduced elecrical ctivity and red areas correspond to increased electrical activity. A, anterior; P, posterior.
Dopamine deficiency is often caused by increased monoamine oxidase A and B activity. 3 Blocking MAO activity by MAO inhibitors increases serotonergic, noradrenergic, and dopaminergic transmissions. Thus the patient was treated with a selective MAO type B inhibitor, selegiline, which increases dopamine levels. Increased levels of catecholamines are thought to increase insulin signaling. 4
Within a month of treatment with selegiline at 10 mg/day her hypotension, bradycardia, and FBS had normalized. For the first time, she was able to maintain a stable insulin regimen. HbA1c dropped from 119 mmol/mol (13%) to 64 mmol/mol (8%). A follow-up EEG/qEEG showed 10-12% increased powers (Figure 1A), which correlated with slight normative changes by LORETA analysis (Figure 1B).
Selegiline improved the patient’s cardiovascular function, stabilized insulin requirement and decreased HbA1c, but she still reported anxiety and occasional urges to binge and was persistently insomniac. This suggested a sub-optimal MAO inhibition response and limited efficacy. Thus selegiline was replaced with tranylcypromine, a non-selective MAO inhibitor, which increased catecholamines and serotonin signaling.
With tranylcypromine (20 mg/day), her HbA1c normalized to 42 mmol/mol (5%). A follow up EEG showed significant increases in absolute power by 50%-60% in frontal and posterior regions (Figure 1A). Normative LORETA changes in all frequencies occurred in anterior and posterior brain regions (Figure 1B). Neuroimaging data correlated with improved cardiovascular function, mood, cognition, and circadian rhythm.
Four years after starting tranylcypromine, the patient has successfully sustained glycemic control. More important, HbA1c remains tightly controlled with less insulin than her prior insulin doses.
We suggest the importance of subtyping patients with diabetes and depressive syndromes based on cardiovascular, neuroendocrine and a priori EEG/qEEG data with LORETA analysis for selecting antidepressant treatment.
Footnotes
Abbreviations
BMI, body mass index; FBS, fasting blood glucose; HbA1c, glycated hemoglobin; LORETA, low resolution electromagnetic tomography; MAO, monoamine oxidase; qEEG, quantitative electroencephalography; SSRIs, selective serotonin reuptake inhibitors; T1D, type 1 diabetes.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.