
Abstract
Youth with chronic illnesses have the greatest risk for a decline in their health management during transition-age. Because of this demonstrated and well-known issue, research has focused on how to improve the transition of care process. Despite the increasing number of technological devices on the market and the advances in telemedicine modalities available to patients with type 1 diabetes (T1D), the utilization of technology is still suboptimal among patients of transition-age (ages 13-25). This article reviews the available resources, patterns of use in transition-age youth, and explores opportunities to advance technology use in transitioning patients with T1D from pediatric to adult care.
Keywords
The objective is to review current use of technology in patients with type 1 diabetes (T1D) transitioning from pediatric to adult care and discuss the potential to improve transition process outcomes. Acknowledging the important psychological development of this transition period, this article specifically reviews the current and promising future use of technology for day-to-day management of diabetes (eg, use of insulin pumps and continuous glucose monitors [CGMs]) and the use of technology in health care delivery and patient-provider communication (telemedicine) in this population.
What Is Transition of Care, and Why Is It Important?
Transition from pediatric to adult care is a process rather than an event. 1 Transfer of care is the actual event whereas transition has been defined as a “purposeful, planned process that addresses the medical, psychosocial, educational and vocational needs of adolescents and young adults as they grow up learning to live with their lifelong medical condition.” 2 In the diabetes literature, the transition process has become a focus of considerable research, as health care management during and after the transfer of care tends to be challenging as demonstrated by poorer health outcomes. 3 There is broad consensus that a lack of effective transition from pediatric to adult diabetes care may contribute to fragmentation in health care, decreased frequency of clinical follow-up, and adverse outcomes in young adults with T1D, however empirical data are limited on best practices in the transition process especially within the United States. 4
Another challenge is the variability in age range cited in transition literature. 5 The variation is often related to whether the research is addressing interventions for the transition process, often taking place as early as age 13 or the actual transfer of care which is commonly achieved during “emerging adulthood or age 18-25.”1,6,7 For this article, we reviewed articles focused on technology use in youth with T1D age 13-25 years, as it is the population most often defined as “transition-aged youth.” This definition is consistent with the theories of Arnett and the recent discoveries in the field of neurophysiology, which point out that prefrontal cortex continues to mature until the age of 25.7,8
There have been several attempts to improve the transition process by increasing education and support, adjusting clinic visits, and creating teams to target the transition-age population and transfer of care. Some programs have provided both clinic-based and online support groups with access to medical providers as well as peers that focused on providing information and support to improve the transition process.9,10 Another focus has been changes to the actual clinic visits by offering joint or transition clinics.11-13 A third approach involves a health care staff member who helps coordinate the transition period.14-17 These various approaches9-17 have shown limited and variable improvements with adjustment to and acceptance of T1D, improvements in A1c, reduction in short-term health complications, engagement with services, and successful transfer of care from pediatric to adult providers. A more robust transition process has been recommended given the potential short- and long-term effects on health outcomes and variability with current attempts. 1
Current State of Glycemic Control in Transition-Age Population: The Case for a Multifaceted Approach to Transition Care
Importance of optimal glycemic control for long- term outcomes has been long established: the landmark Diabetes Control and Complication Trial’s study population initially included subjects aged 13-39 and compared rates of diabetes complications between those receiving intensive insulin therapy with an A1c of 7.2% to those receiving standard care treatment with an A1c of 9.1%. 18 Long-term follow-up of this cohort demonstrated metabolic memory; participants in the intensively treated group during adolescence and young adulthood had lower rates of complications more than 20 years after the conclusion of the interventional part of the study. 19 Using technological devices with the potential to improve metabolic control in the transition-age becomes even more relevant in the light of this finding, as optimized control during this period has profound future implications.
It is uncommon for transition-age patients to achieve A1c goals: just 17% of adolescents (ages 13-17) and 14% of emerging adults (ages 18-25) are currently reaching ADA-recommended A1c targets. 20 The T1D Exchange data show insulin pump use attenuated the age-related A1c increase during adolescence, highlighting its potential to improve outcomes in this group. 21 Unfortunately, there is little discussion in the published literature regarding the role of diabetes devices specifically in the transition process, aside from referencing historical problems with compliance of first generation real-time CGM in this age group. Studies are needed to specifically assess the impact of the addition of diabetes devices in the transition age.
The presence of patient psychosocial stressors is another important determinant to successful transition from pediatric to adult care. 22 Psychosocial factors impacting diabetes management have been identified as depressive symptoms, 23 anxiety or avoidance, 24 learning difficulties, 25 diabetes burnout, 26 life satisfaction, perceived stress, global well-being, 22 combinations of life transitions/change, diabetes self-efficacy, and demonstration of diabetes self-management. 27 Research continues to demonstrate that untreated psychosocial stressors are a moderator of optimal diabetes management. 22 In addition, roughly two-thirds (65%) of transition-age youth indicate they have experienced at least 1 unfavorable medical outcome due to suboptimal access to medical care. 28
In particular, lack of access to mental health professionals for transition-age youth with psychologicalcomorbidities is often cited as a major barrier to care in this age group. 4 Thus, the process of improving outcomes for transition-age youth should focus on both improving metabolic control and on timely identification and treatment of psychological comorbidities.
Diabetes technologies are increasingly being used in patients of all ages, although perhaps transition-age youth are best positioned to incorporate it seamlessly into their daily lives. Technology use is widespread among adolescents in the United States, with the average usage time of all forms of media at 7 hours 38 minutes daily. 29 In addition, 95% of American adolescents use the Internet, 74% have their own computer, and 77% have a mobile phone and report use of instant messaging daily. 30 Technology has been integrated into diabetes management in various ways including decision-making software, communication between patient and provider, and analysis of the disease. 31
Technological advancement and development of numerous devices has made significant improvement in the ability to manage diabetes,18,32 however it is unknown which patients are best suited for certain devices or technologies and how factors such as psychological well-being may affect successful use. Researchers have recommended treatment methods which involve support people (family, friends, coworkers, and health care providers), ongoing assessment of the patients’ skills and understanding of the technology and treatment recommendations, as well as barriers that may arise throughout treatment (psychological disorders, diabetes burnout, diabetes-related family conflict). 33 Today, there is a potential for technology to target all of those areas to facilitate an improved transition process. In this article, we aim to review the current state of technology use in transition-age youth with T1D and to discuss its potential to improve the outcomes during the transition process.
Use of Technology Impacting Day-to-Day Management in Transition-Age Youth With T1D
Use of diabetes devices including insulin pumps and CGM is increasing overall; yet large studies such as the T1D Exchange Registry report utilization by adolescents and young adults (age 13-25) lower than any other age.20,34 A recent review of 3 large multicenter registries (including sites in the United States, United Kingdom, Germany, and Austria) reports that in a pooled analysis, insulin pump use in children and adolescents was associated with statistically and clinically significant lower mean hemoglobin A1c, supporting the notion that pump therapy may be superior to multiple daily injections in this population. 35
The dynamic environment of diabetes technology development inherently makes published reviews of device outcomes and utilization rates challenging. New device models and upgrades are released in rapid succession and quantification of outcomes on a large-scale will likely lag behind the most recently released technology. Unfortunately, insurers often make reimbursement decisions using historical data that may not represent the current state. 36 For example, large health insurers often cite lackluster adherence to consistent CGM use in early CGM trials37,38 (eg, 30-55% subjects used CGM ≥6 days/week) to categorically deny coverage for those devices in transition-age youth, thus limiting our ability to assess its efficacy. In part, these decisions may explain the lower rates of technology utilization by a population that has otherwise wholeheartedly embraced technology integration in their day-to-day lives. Further analysis of initial studies revealed a CGM dose-dependent improvement in A1c across all age groups, including adolescents and emerging adults, exemplifying technology is effective in those who use it consistently.38-40 Understanding factors affecting the patient’s decision to consistently use a device will be key to enhancing usability and acceptance in the transition-age population.
The perceived advantages and disadvantages of diabetes technologies vary across age groups with respect to convenience and effectiveness as it relates to day-to-day diabetes management. 41 In the T1D Exchange Registry, those ages 13-25 were approximately twice as likely (6.2%, vs 3.0% in <13 years old and 3.4% in >25 years old) to discontinue pump use over the course of a 1-year follow-up than both younger and older participants. 42 Reasons for discontinuing CGM use also varied by age: Transition-age youth were more likely to cite problems with insertion, adhesives, and interference with sports and activities than younger or older participants (personal communication detailing age-specific responses to survey data presented in suppl 3 of reference). 43 Surveys of both current and former CGM users illustrate perceived beneficial aspects such as improved sense of safety, motivation and confidence to manage diabetes, and avoidance of serious hypoglycemia but also report problems with accuracy, usability, intrusiveness, alarms, and insurance issues leading to inconsistent use or discontinuation altogether.44-46 Device features and educational programs that succeed with younger children or older adults may fail in the transition-age group. Unfortunately there is still a paucity of literature specifically examining barriers to technology use and acceptance in transition-age youth.
The frequency of diabetes care visits decreases at the time of transfer of care, 47 and under those circumstances technology may serve to link the patient and provider during a time frequently punctuated by travel for education or early career obligations. Patients transferring from pediatric to adult diabetes care providers who use insulin pumps are less likely to be lost to follow-up and report greater treatment satisfaction and improved glucose variability.48,49 With the integration of devices and health care technology a provider may be able to access data from the insulin pump or CGM upload via a web-based portal for a patient who is physically unable to attend an office-based appointment. Some of these services are becoming reimbursable and may be suitable for providing significant aspects of diabetes care remotely (eg, while a patient is attending college).
Technology Use in Health Care Delivery and Patient–Provider Communications (Telemedicine) in Transition-Age Youth With T1D
Diabetes is largely a self-managed condition. Patients are supposed to implement a comprehensive care plan to self–manage personal and environmental factors pertaining to their condition and contact with the medical provider is frequently limited to regular appointments commonly spaced several months apart. Recent technology improvements in disease monitoring and insulin delivery have provided patients and providers with an opportunity to collect and analyze large amounts of data and make frequent changes to the regimen to optimize treatment outcomes. In this new environment, the traditional model of quarterly office visits to the provider as a mainstay of therapy is becoming obsolete, and new models of communication and health care delivery facilitated by technology are being explored.
Telemedicine, defined as “any remote communication of health care information and services between patients and health care providers using telecommunication,” 50 presents a unique opportunity for transition-age youth with T1D to engage in diabetes management using the tools with which they are familiar and comfortable.
Existing evidence generally supports the effectiveness of telemedicine services in the area of behavioral health in adolescents with T1D. Delivery of Behavioral Family Systems Therapy–Diabetes (BFST-D) by videoconferencing was found to be a viable option for addressing nonadherence and suboptimal glycemic control in adolescents with T1D in a randomized controlled trial conducted over a 12-week period. 51 However, most of the research in this field still consists of preliminary studies or descriptions of feasibility of an intervention rather than controlled randomized clinical trials of effectiveness. Even though videoconference-enabled 1-on-1 visits and group visits with health care providers are becoming a more widespread option in many areas of medicine, to date there is no literature evaluating its use in transition-age patients with T1D.
A recent study by Kumah-Crystal et al found increased frequency of use of the selected technologies (eg, mobile applications, social technologies, and glucose software) in patients with higher A1c. They subsequently postulated that adolescents in poorer glycemic control may be primed to achieve greater improvements in health outcomes by using the technology to problem solve in a reactive manner. 52 A meta-analysis reviewed a number of telemedicine interventions including text messaging, phone and video consultation, remote blood glucose and disease monitoring, mobile phone applications and computer software. 50 Authors noted statistically significant improvement in A1c values in 3 studies, even though a trend toward improvement was observed in 10 of the 15 studies reviewed. Mobile phone support for sick-day management was associated with lower hospital admission rates for diabetes complications. Users reported high levels of satisfaction with telemedicine modalities, and most wanted to continue using them after the studies were completed. The authors bring up a number of challenges to telemedicine use: the need to log on to a portal or a website rather than using personal devices (health care privacy), lack of integration with the existing electronic health records databases, and the lack of personalized technology options that may be more attractive to adolescents. 50 Interventions combining technology with the clinician and parental involvement were found to be the most successful, but the current lack of reimbursement for those services may be limiting the availability to patients. 53
Two other systematic reviews found limited evidence that mobile phone messaging interventions may provide benefit in supporting the self-management of long term illnesses 54 and that the interventions could improve treatment adherence and metabolic outcomes. 55
Unfortunately, most of the studies on usage of telemedicine modalities in youth with T1D lack adequate descriptions of methodology, are limited by inadequate sample sizes, and lack reporting of long-term outcomes. There is limited information on acceptability and the costs and risks of studied interventions, therefore conclusions cannot be widely disseminated.53-55
Despite the growing recognition of the values of technology in management of chronic disease, telemedicine modalities have not been applied widely to the transition process between the pediatric and adult settings. Most interventions used to prepare adolescents with chronic disease for transition still tend to be disease-focused and delivered in-person, increasing the cost and decreasing availability and efficiency. Huang and colleagues recently evaluated a generic (across disease) approach to transition of adolescents to adult care, in a randomized controlled trial that included 81 patients with diagnoses of inflammatory bowel disease, cystic fibrosis, or T1D (N = 34). 56 The intervention group received a 2-month intensive intervention delivered via the Internet and text messaging which provided disease management and a skill-based intervention followed by a 6-month review period. Intervention recipients demonstrated significant improvements in all targeted outcomes including disease self-management and health related self-efficacy. In addition, the number of patient-initiated communications between intervention group participants and their health care team increased significantly compared with the control group. Authors emphasize that the baseline health literacy affected outcomes according to treatment group. In contrast, age and disease group did not have such effect on outcomes over time. Disease status, functional performance and quality of life did not significantly change over the study period by treatment group. As technology continues to advance, systems that integrate input from a variety of patient-driven mobile applications with a protected, web-based portal suited for use by several categories of users may become more widely available and will ultimately serve as a solution to a number of barriers listed above (eg, Mobil Diab [Infokom, Neubrandenburg, Germany], Glooko [Palo Alto, CA], and Tidepool [Palo Alto, CA]). 57
Online Communities—Support or Distraction?
For today’s generation of adolescents, online social networking is one of the basic ways of connecting with others. At the same time, web-based programs are increasingly utilized as a mechanism by which to incorporate social, interactive, and guided behavior change processes in chronic disease areas including diabetes. Ho and colleagues reviewed the features of 18 online communities specific to diabetes and available to adolescents with T1D. 58 Diabetes-related blogs as well as groups that exist within other social networks not focused on health (eg, Facebook) were excluded from their analysis. The results of the review indicated that, even though many sites were successful in incorporating a number of evidence-based features relevant to improvement in diabetes self-management, they exhibited a general lack of guidance and oversight for discussions and activities available on those sites. Authors found that less than half of those communities were certified by the Health On the Net Foundation, a nonprofit accredited by the Economic and Social Council of the United Nations that evaluates trustworthiness and reliability of health-related sites. Even more concerning, the online communities included in the review did not have a process to verify a diabetes diagnosis (eg, via clinician verification). There is a need for outcome data to reliably guide patients and clinicians in use of such sites.
The Promise of Technology: Where Do We Go From Here?
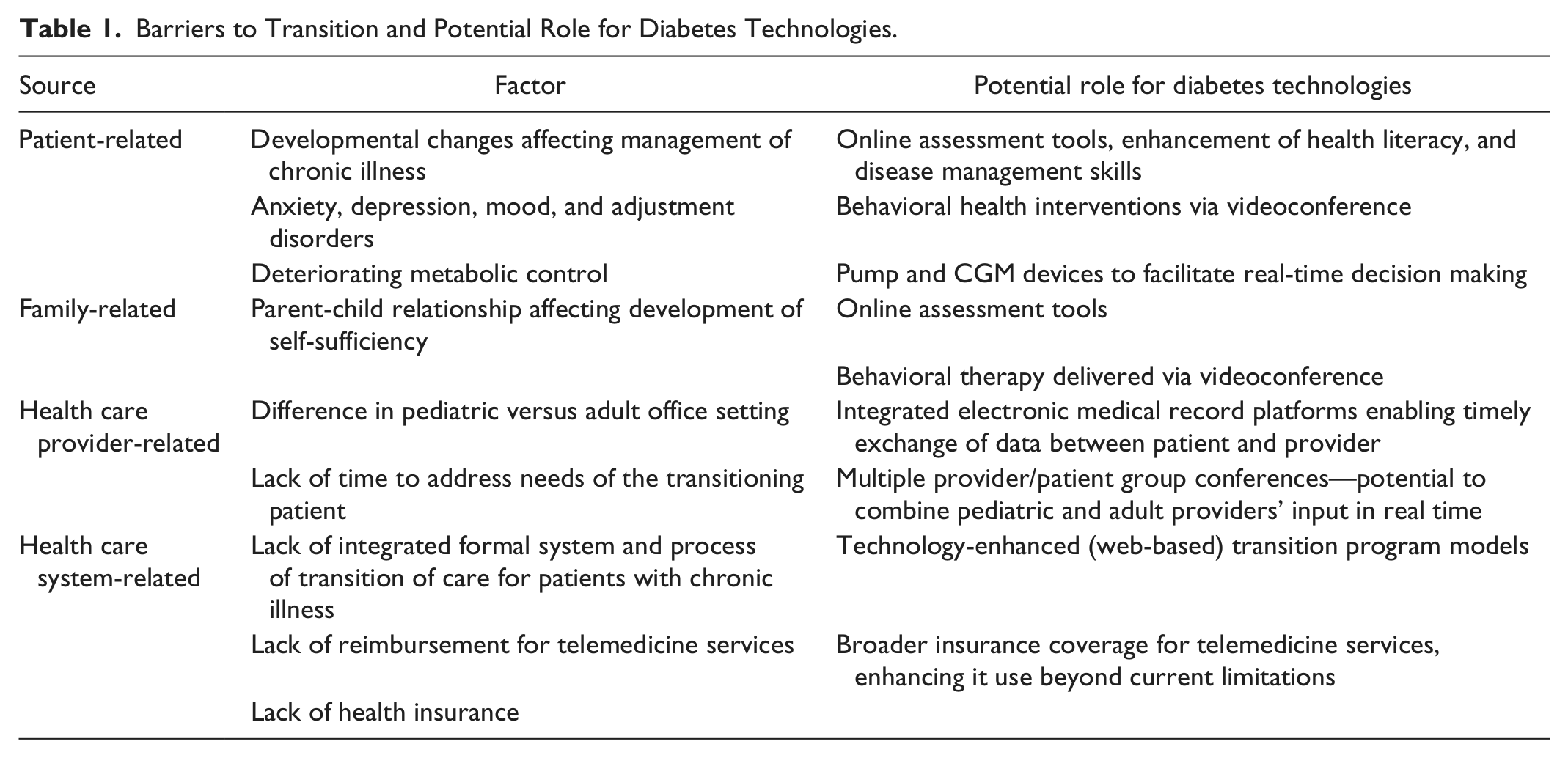
It is clear that transition-age youth with T1D are a group facing the biggest challenges in maintaining optimal glycemic control and minimizing long-term complications of their disease. This seems directly related to the complex interplay of physiological and psychosocial factors specific to their age and developmental stage. In the transition-age, adoption of new diabetes technologies not only depends on cost, usability and added value; but also privacy, growing independence, and changing self-identity. Transition-age patients have a different relationship with diabetes technologies than younger children or older adults. Even though they belong to a tech-savvy generation, the utilization of health care related technology in this group is lower than any other group. Barriers to successful technology integration into the transition process are likely falling into similar categories as the barriers to successful transition itself: 28 patient-, family-, health-care-provider-, and health-care-system-related barriers. It is our opinion that majority of those barriers could be addressed by targeted use of technology, as postulated in Table 1.
Barriers to Transition and Potential Role for Diabetes Technologies.
Conclusions
Despite the evidence that insulin pump therapy may be superior to multiple daily injection treatment, 35 patterns of prescribing technology devices for daily management (pumps and CGM) in the transition-age group are frequently restrictive (by providers and insurance), denying access to patients with poorer control. This approach may need to be modified if we are to understand the full extent of benefits technology may bring to this group. Evidence points to a more successful transfer of care during the transition-age in patients using technology for insulin delivery and glucose monitoring (insulin pumps and CGM).47-49 Larger randomized controlled trials are still needed to define patients that would most benefit from intervention, potential risks in relying on and promoting technology, and barriers to care needing to be addressed.
Patterns and barriers of telehealth utilization in transition-age youth with T1D should be studied more systematically to devise strategies for successful incorporation of telehealth in their care. Large-scale randomized controlled trials of interventions, preferably based on established theories of psychological development, need to be conducted to compare efficacy of approach to the transition process using different electronic and nonelectronic mediums.
Appropriate reimbursement for telehealth services, particularly in the area of behavioral and mental health in which successful interventions have been piloted, 51 are crucial to improve access to needed services, and to eventually improve outcomes in this particular group of patients.
Wherever possible, technology related to diabetes control and management should be integrated with other devices, particularly smartphones. The feedback from transition-age users should be actively solicited and incorporated into device upgrades.
Integrated platforms, giving access to multiple users (family, peers, and medical professionals—“the team”)—and encouraging interaction between them—should be developed in a user-friendly fashion, while ensuring privacy and security of the personal health information.
Footnotes
Abbreviations
CGM, continuous glucose monitor; T1D, type 1 diabetes.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.