
Abstract
Background:
The purpose was to assess the occurrence of white coat adherence, defined as an increase in adherence to treatment regimens prior to a clinic appointment, in children and adolescents with type 1 diabetes (T1D) who use insulin pumps.
Methods:
Blood glucose monitoring (BGM) data, carbohydrate inputs, and insulin boluses delivered were downloaded from the insulin pumps of children and adolescents, aged 7-19 years with T1D, at 2 consecutive routine diabetes clinic visits. Linear mixed models were used to analyze patterns of BGM, carbohydrate inputs, and insulin boluses delivered in patients who had ≥28 days of data stored in their insulin pumps.
Results:
In general, younger children engaged in more frequent BGM, carbohydrate inputs, and insulin boluses delivered than older children and adolescents. White coat adherence occurred with frequency of BGM, carbohydrate inputs, and insulin boluses delivered, but only in younger children.
Conclusions:
Diabetes care providers need to be aware that white coat adherence may occur, particularly in young children. Providers routinely download meter and insulin pump data for the 1- to 2-week period before the clinic visit. For patients exhibiting white coat adherence, their data will overestimate the patient’s actual adherence.
Diabetes technology is unique in that blood glucose monitors and insulin pumps have data storage capacity that allows for the objective assessment (vs self-report) of diabetes treatment adherence that reflects actual patient behaviors. The data derived from insulin pumps allow for the examination of general adherence to the T1D regimen (eg, blood glucose monitoring, [BGM] frequency ≥4 times/day, ≥3 carbohydrate inputs, and ≥3 insulin boluses delivered; 1 and whether these adherence behaviors increase prior to the diabetes clinic visit, a phenomenon known as white coat adherence.
Several studies of white coat adherence have been conducted with adult epilepsy, HIV, and dermatology patients demonstrating that many adult patients increase their medication use prior to the appointment with a physician.2-4 This pattern of increased medication use that precedes the medical appointment raises interesting questions about the reinforcing role that the appointment may have in medication adherence. 5 Studies in pediatric patients have been limited to young children <12 years of age,3,6,7 but have demonstrated a similar white coat adherence pattern.3,7 In the only study to examine white coat adherence in T1D, Driscoll and colleagues demonstrated that BGM increased in young children (ages 2-11 years) prior to appointments with the physician. 6 The overall objective of the current study was to extend Driscoll and colleagues, 6 study, which evaluated white coat adherence solely in the context of BGM (ie, they did not use carbohydrate or insulin bolusing data) in young children. The primary aim of the current study was to determine if white coat adherence occurs with carbohydrate inputs and insulin boluses (in addition to BGM) in both children and adolescents with T1D who use insulin pumps. Specifically, we hypothesized that the frequency of BGM, carbohydrate inputs, and insulin boluses delivered would increase prior to the appointment with the physician.
Methods
Participants were part of a larger observational study aimed at assessing BGM patterns across time; however, only data from children and adolescents (ages 7-19 years with diabetes duration ≥12 months) who used a Medtronic insulin pump were included in the analyses for the current study. Children were included in the current study if their insulin pump contained ≥28 days of data. This resulted in downloaded data from 48 children at clinic visit 1 and 50 children at clinic visit 2; data from 85% of the patients were available at both clinic visits. This study was approved by the Florida State University Institutional Review Board.
Insulin Pump Downloads
The Medtronic insulin pump stores 2-3 months of data including BGM readings (either wirelessly transmitted from compatible monitors or manually entered), carbohydrate inputs (as estimated by the patient and/or caregiver and manually entered), and insulin bolus doses delivered. Data were downloaded from each patient’s Medtronic insulin pump during 2 routine diabetes clinic visits that occurred approximately 3 months apart.
Glycemic Control
Hemoglobin A1C (A1C) representing the average glucose level during the past 2.5 to 3 months was obtained at each clinic visit using a Siemens Healthcare Diagnostics DCA Vantage (Siemens Medical Solutions USA, Inc.) (reference range 4.2-6.5%), which is National Glycohemoglobin Standardization Program certified as having documented traceability to the Diabetes Control and Complications Trial Reference Method.
Statistical Analyses
Once data were downloaded from the insulin pump, each participant’s data file was cleaned to identify and correct technological errors (eg, duplication of data, data included for dates from the previous clinic visit). 1 Descriptive statistics including means, standard deviations, and ranges were calculated for demographic, A1C, and insulin pump variables (BGM, carbohydrate inputs, and boluses delivered). Linear mixed models were used to evaluate white coat adherence for BGM, carbohydrate inputs, and insulin boluses delivered. Advantages of linear mixed models over other approaches include (1) ability to model individual change across time, (2) different number of observations per subject is allowable, and (3) time can be continuous rather than a fixed set of points (eg, no need to segment the data into blocks of time such as 2 weeks, 1 month, 2 months). Importantly, linear mixed models adjust within subject dependence in designs with repeated measures in which data from the same subject is intraindividually related. SAS Version 9.2 (Cary, NC, USA) was used for all analyses.
Results
Patient Characteristics. Participants ranged in age from 7 to 19 years (mean = 13.15 ± 3.13 years; 64% female) with a T1D duration of 1.22-15.40 years (mean = 7.06 ± 3.30 years) and insulin pump use duration of 0.42-11.09 years (mean = 4.53 ± 2.73 years).
Average A1C at clinic visit 1 was 8.32% (10.7 mmol/mol) ± 1.07 (range = 6.20-11.87%; 7.3-16.3 mmol/mol) and 8.48% (10.9 mmol/mol) ± 1.17 (range = 6.40-11.80%; 7.6-16.2 mmol/mol) at clinic visit 2.
Table 1 provides descriptive statistics for insulin pump data downloaded at 2 consecutive diabetes clinic visits. The following were calculated for each child: mean blood glucose level (mg/dL), mean number of BGM readings per day, mean carbohydrates consumed (grams) on each occasion, mean number of carbohydrate inputs per day, mean insulin delivered (units) on each occasion, and number of insulin boluses delivered per day.
Insulin Pump Data Downloads at 2 Separate Clinic Visits.
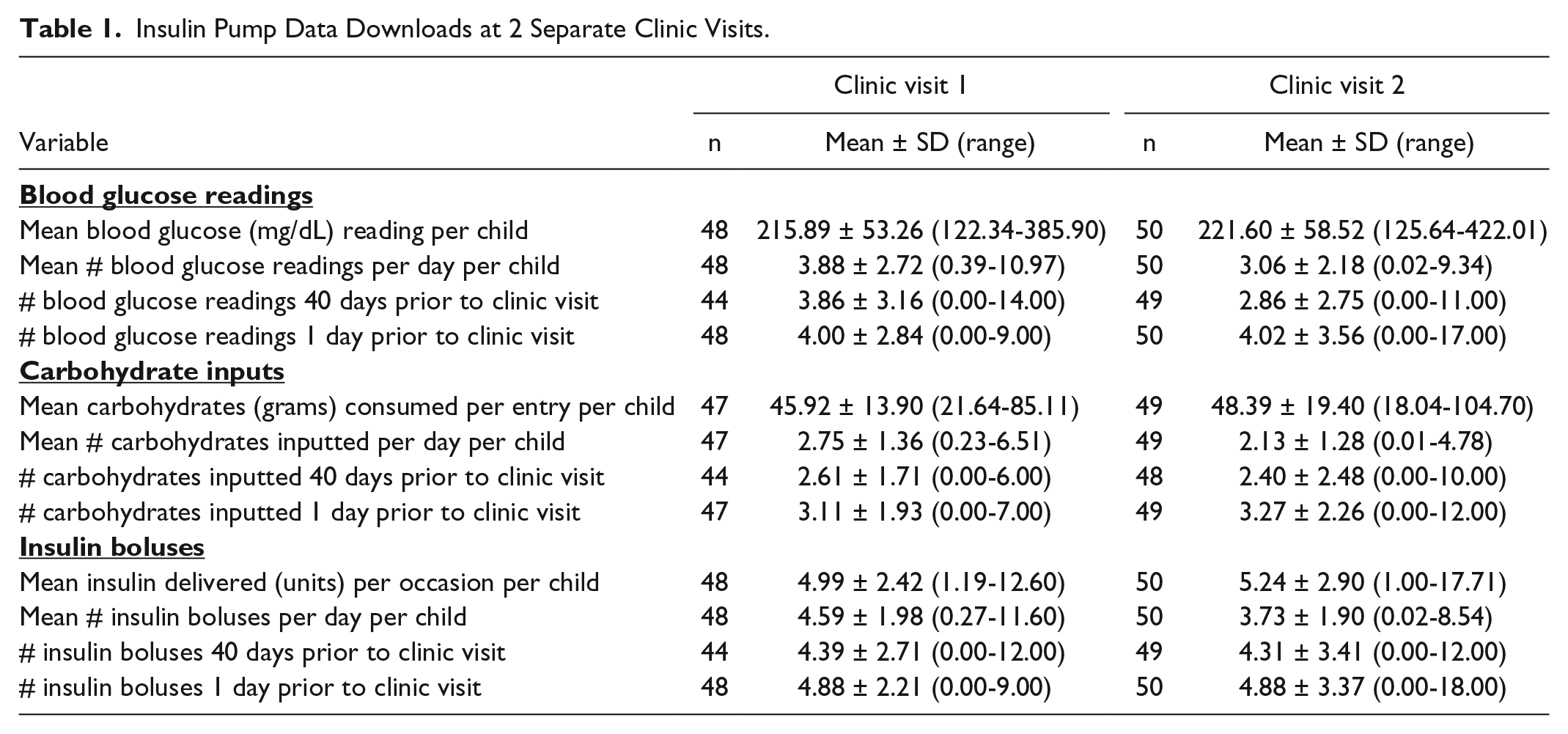
Also depicted in Table 1 is the white coat effect. The average number of BGM readings, carbohydrates inputted, and insulin boluses delivered at 40 days and 1 day prior to the diabetes clinic appointment are provided as well as standard deviations and ranges. Although great variability occurred regarding BGM, carbohydrate inputs, and insulin boluses delivered, the average number of BGM readings, carbohydrates inputted, and insulin boluses delivered increased from 40 days to 1 day prior to the diabetes clinic appointment.
Linear Mixed Models
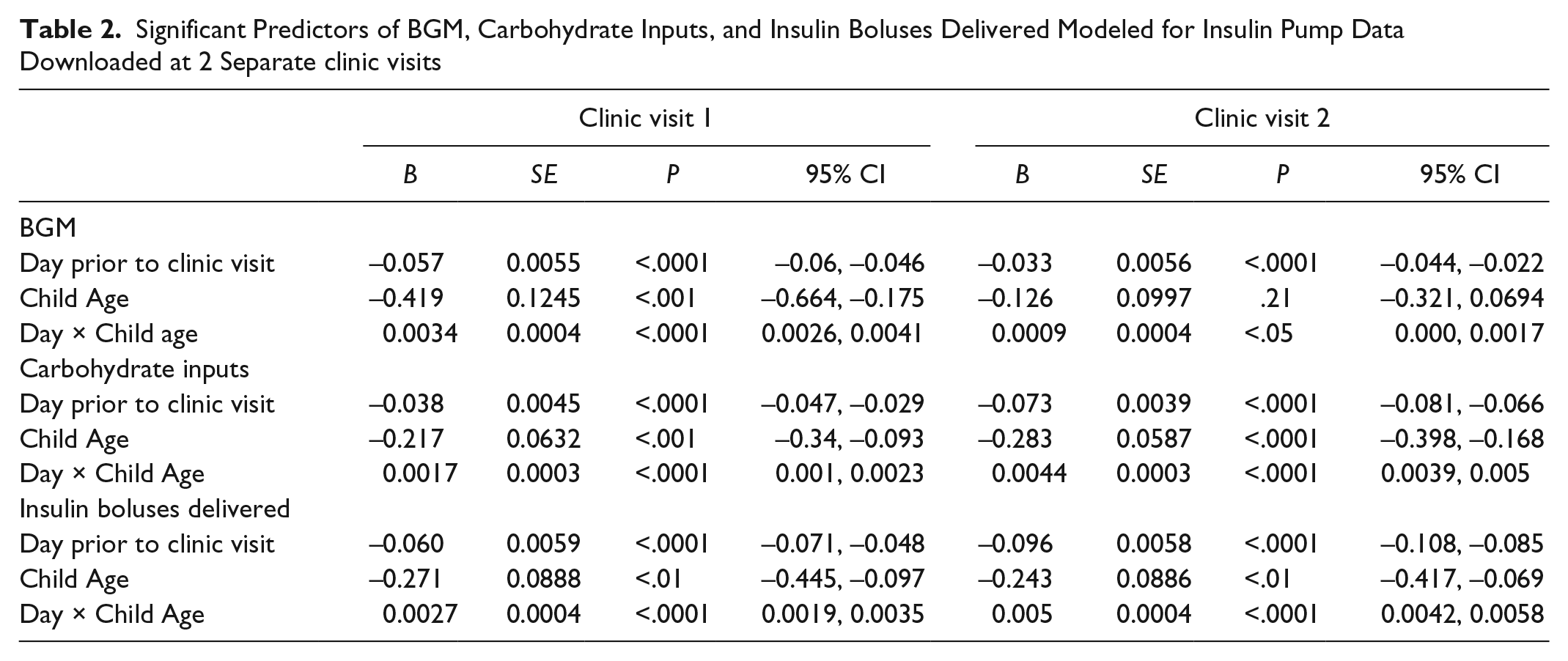
Linear mixed models were used to evaluate change in BGM frequency, carbohydrate inputs, and insulin boluses delivered across time as the diabetes clinic visit approached. Also tested was the effect of the child’s age at the day of the clinic visit and the interaction between the day (the number of days prior to the clinic visit) and child age. Table 2 provides the results of these analyses, highlighting the significant Day × Child Age interaction in all models.
Significant Predictors of BGM, Carbohydrate Inputs, and Insulin Boluses Delivered Modeled for Insulin Pump Data Downloaded at 2 Separate clinic visits
To interpret the significant interaction of Day × Child Age (see Table 2), we used the recommendations of Cohen and colleagues 8 to illustrate the interactions. Specifically, they recommend plotting the regression of Y (ie, BGM, carbohydrate inputs, insulin boluses delivered) on X (ie, day) at 3 meaningful values of Z (ie, age). In Figure 1, we chose 3 ages, 7, 14, and 19 years, to represent young children, older children/young adolescents, and older adolescents, respectively to illustrate the interaction. It should be noted that each regression line represents the regression of Y on X at 1 value of the predictor Z (7, 14, or 19 years). It should also be noted that we arbitrarily selected 40 days (ie, 40 days before the appointment) to illustrate the interaction. At both clinic visits, younger children showed an increase in BGM, carbohydrate inputs, and insulin boluses delivered per day as the date of the clinic visit approached. In contrast, older children and adolescents showed a flat pattern of BGM frequency, carbohydrate inputs, and insulin bolus delivery.
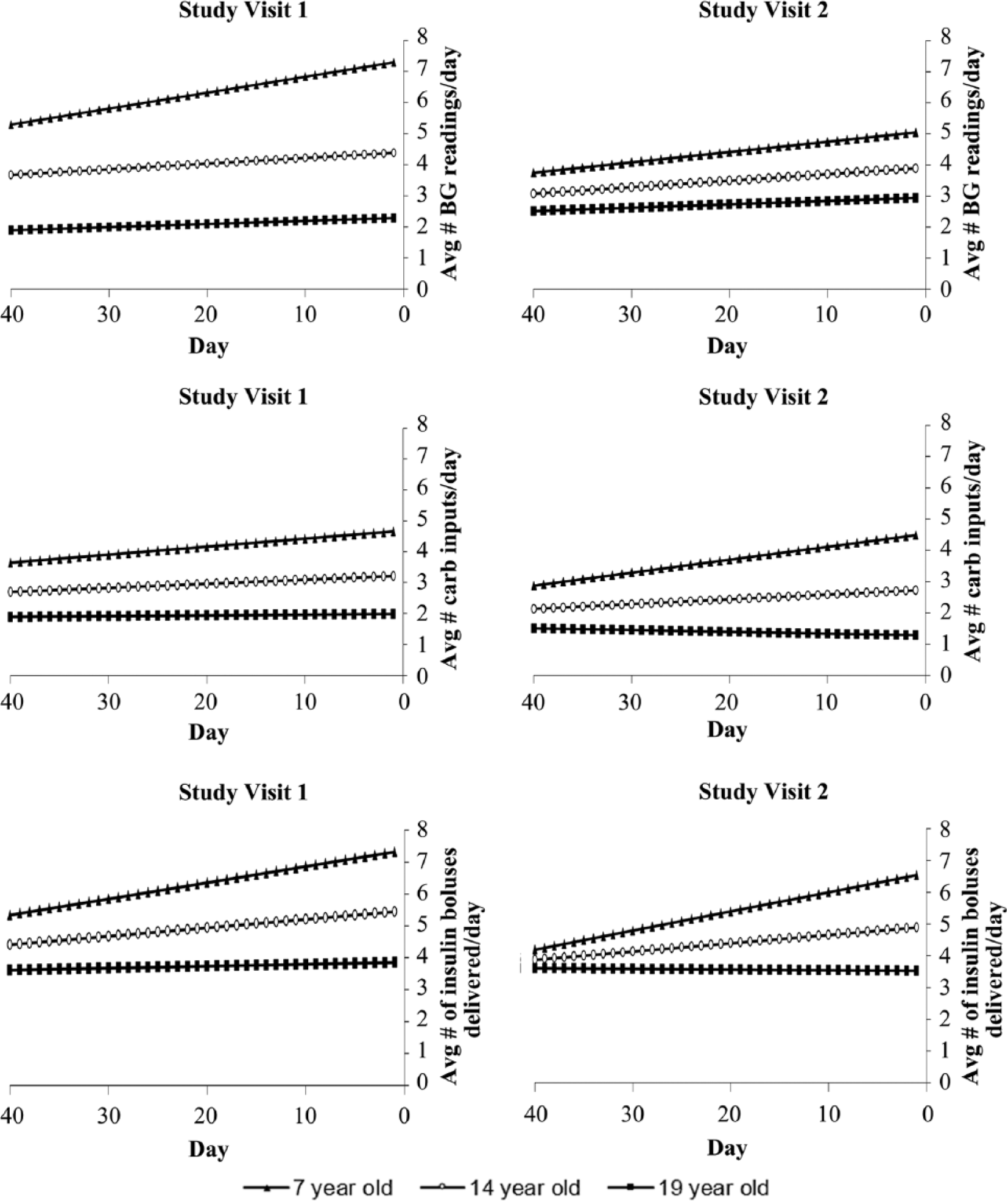
Illustration of white coat adherence in children, but not adolescents.
Discussion
Previous findings of BGM white coat adherence occurring in young patients (2-11 years old) with T1D 6 were replicated in the current study, but a white coat adherence effect in older children and adolescents was not demonstrated. This study extends prior findings of BGM white coat adherence, which was limited to data downloaded only from blood glucose monitors, by using data downloaded from insulin pumps. Importantly, the results of the current study demonstrated the white coat adherence effect for carbohydrate inputs and insulin boluses, which has not previously been documented. Moreover, this study adds to a growing literature that uses objective data to evaluate insulin bolus adherence and it is 1 of very few studies to use data downloaded from insulin pumps in children and adolescents with T1D to evaluate adherence behaviors.9,10
Several explanations may account for the increase in insulin pump adherence behaviors in parents of young children, who bear primary responsibility for diabetes care, as the date of the clinic visit approached. The clinic visit and contact with the diabetes care team may serve as a “trigger” or prompt, resulting in increased insulin pump adherence.6,7 This explanation is consistent with findings demonstrating that more frequent visits to the diabetes clinic result in better glycemic control across 3 years. 11 Another possibility is that parents increase insulin pump adherence to provide the diabetes care provider with more data, which may result in more comprehensive and helpful clinical recommendations. Finally, parents may be motivated to gain their diabetes care provider’s approval (or avoid the provider’s disapproval) by appearing more adherent. 7
White coat adherence may result in benefits to patients with T1D such as providing more data to the diabetes care provider so that more informed decisions can be made. In addition, better adherence may lead the diabetes care provider to praise parents and patients thereby reinforcing the practice of optimal diabetes care. However, the somewhat artificial increase in adherence behaviors may also be misleading to the diabetes care provider, which leaves the impression that adherence is higher than what is actually the case. In an effort to reduce the amount of data to interpret, diabetes care providers may routinely download BGM and insulin pump data for the 1 to 2 weeks prior to the diabetes clinic visit. This means that diabetes heath care providers are only using the data from the time period when white coat adherence is most likely to occur.
The pattern of white coat adherence in younger children was replicated in both clinic visits. In contrast, older children’s and adolescents’ pump adherence behaviors did not markedly change in the days preceding the diabetes clinic visit. These results highlight the need for open communication about adherence behaviors and the need for different intervention strategies depending on the age of the child. Intervention strategies will likely be different in content because younger children (and their parents) who demonstrate the propensity to increase adherence as the diabetes clinic visit approaches (eg, increase frequency of visits may be 1 solution), 11 whereas intervention strategies for older children and adolescents might focus on reinitiating or increasing parent involvement, or other novel models of care such as “Team Clinic.” 12
The present study has a number of strengths that expand on past research on T1D treatment regimen adherence and specifically, the occurrence of white coat adherence. Previous studies have only examined white coat adherence in children <12 years of age, yet this study extended that age range to include patients as old as 19 years of age, allowing for greater examination of the developmental variability of white coat adherence. The present study also used objective data to examine white coat adherence, rather than relying on patient self-reported adherence, which can be prone to error. However, notably, carbohydrate inputs are estimated and manually entered, as are BGM results for those patients who do not use a wireless meter. Nonetheless, data downloaded from insulin pumps offer the closest approximation of actual adherence behavior that is currently available. This study expands on the time frame for which white coat adherence behaviors have been examined. Most previous studies have used a limited amount of data (eg, 5 days, 2 weeks prior to the appointment); however, all the available data from insulin pumps were examined in the current study, with all children having at least 28 days of data. In addition, we replicated our findings at 2 diabetes clinic visits. Finally, we examined white coat adherence with respect to carbohydrate inputs and insulin bolusing.
Limitations of this study include relatively small sample size, missing data because of technological problems involving the download (hence only 85% overlap in patients), and lack of data for potential explanations of the white coat effect (eg, who is responsible for the diabetes treatment regimen). In addition, some patients may have changed their behavior simply because they were aware of being in the study; however, it is notable that the results were replicated at 2 separate diabetes clinic visits. Nevertheless, the results of the current study are highly clinically relevant as members of the diabetes health care team need to be aware that white coat adherence occurs, especially in families caring for young children with T1D.
Footnotes
Abbreviations
BGM, blood glucose monitoring; T1D, type 1 diabetes.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was partially supported by LifeScan, Inc, who provided meters and strips to participants. The sponsor had no role in the study design, data collection, analysis, interpretation, or writing of the manuscript.