
Abstract
Background:
Collaborative use of structured self-monitoring of blood glucose (SMBG) data and data management software, utilized within a 6-step cycle enables integrated Personalized Diabetes Management (PDM). The 2 PDM-ProValue studies shall assess the effectiveness of this approach in improving patient outcomes and practice efficiencies in outpatient settings.
Methods:
The PDM-ProValue studies are 12-month, prospective, cluster-randomized, multicenter, trials to determine if use of integrated PDM in daily life improves glycemic control in insulin-treated type 2 diabetes patients. Fifty-four general medical practices (GPs) and 36 diabetes-specialized practices (DSPs) across Germany will be recruited. The practices will be randomly assigned to the control groups (CNL) or the intervention groups (INT) via cluster-randomization. CNL practices will continue with their usual care; INT practices will utilize integrated PDM. The sample size is 1,014 patients (n = 540 DSP patients, n = 474 GP patients). Each study is designed to detect a between-group difference in HbA1c change of at least 0.4% at 12 months with a power of 90% and 2-sided significance level of .05. Differences in timing and degree of treatment adaptions, treatment decisions, blood glucose target ranges, hypoglycemia, self-management behaviors, quality of life, patients attitudes, clinician satisfaction, practice processes, and resource consumption will be assessed. Study endpoints will be analyzed for the modified intent-to-treat and per protocol populations. Trial results are expected to be available in late 2016.
Discussion:
Effective and efficient strategies to optimize diabetes management are needed. These randomized studies will help determine if PDM is beneficial.
Keywords
Despite numerous advances in diabetes treatment and monitoring technologies, many patients with type 2 diabetes (T2DM) do not achieve their treatment goals.1-3 Because T2DM is a progressive chronic disease, reassessment of metabolic targets in regular intervals plus appropriate adjustments of treatment strategies are required to achieve and maintain optimal glycemic control. Although the growing number of therapeutic options supports the ability to individualize treatment regimens to meet the specific metabolic needs of each patient, there is often a failure to treat to target or the treatment is not concordant with guidelines.
Several recent studies have shown that appropriate use of self-monitoring of blood glucose (SMBG) regimens, in combination with collaborative, patient-clinician relationships, facilitates therapy optimization and promotes desired behavioral changes, leading to improved clinical outcomes in patients with T2DM.4-9 Use of diabetes data management software has also been shown to convey significant benefits through time and cost savings, combined with significant improvements in glycemic control.10-12
In a recent position paper, Ceriello and colleagues proposed a model of care called the Diabetes Management Circle, 13 which incorporates collaborative use of structured SMBG data and data management software into a recurring, 6-step cycle to tailor therapy for personalized diabetes management: (1) patient education, (2) initiation of structured SMBG, (3) electronic documentation of measurement results, (4) analysis of measurement results, (5) selection/initiation of personalized therapy regimen, and (6) assessment of therapy efficacy. Although key elements of this cycle, such as patient education,14,15 structured SMBG,4-9 and use of specialized SMBG data management software,12,16 have been shown to be beneficial, integration of these elements into a structured, comprehensive approach to personalized diabetes management has not been studied with sufficient study design, duration, and sample size.
We hypothesized that use of the integrated PDM process with insulin-treated T2DM patients will facilitate improvements in glycemic control, therapy adoptions, patient-related outcomes (PROs), clinician satisfaction and efficiency of the outpatient management process within real world clinical settings. To test this hypothesis, we designed 2 studies to assess the impact of integrated PDM on patient outcomes and identify other effects when utilized in (1) general medical practices (PDM-ProValueGP study) and (2) diabetes-specialized practices (PDM-ProValueDSP study).
Methods
The studies are 12-month, cluster-randomized, multicenter clinical trials to evaluate the impact and potential benefits of integrated PDM on patients with T2DM within the scope of outpatient care. Two different levels of ambulatory care will be examined: general practitioners (PDM-ProValueGP study) and diabetes specialists (PDM-ProValueDSP study), respectively. The study protocols were approved by the Ethics Committee of the Medical Association Baden-Württemberg and Saxony (Ethik-Kommission der Landesärztekammer Baden-Württemberg bzw, Sachsen) and the Federal Institute for Drugs and Medical Devices (Bundesinstitut für Arzneimittel und Medizinprodukte, BfArM) and are in compliance with the Declaration of Helsinki. 17
The primary objective of both studies is to assess the effects of using integrated PDM on change from baseline in HbA1c compared with usual care over the study period in insulin-treated T2DM patients treated in general medical and diabetes-specialized practices. Secondary objectives include assessing: (1) the additional effects of integrated PDM on patients empowerment and expected self-efficacy, psychosocial outcomes, hypoglycemia, dyslipidemia and hypertension; (2) the effects of integrated PDM on the outpatient care processes and efficiencies; and (3) medical teams’ perceptions and acceptance the PDM intervention and tools.
Participants
Fifty-four general medical practices (GPs) and 36 diabetes specialized practices (DSPs) and outpatient facilities with a comparable diabetes orientation (eg, medical care centers, hospital outpatient departments) across Germany will be identified and recruited, using a systematic selection process based on a feasibility questionnaire for self-disclosure. Appropriate trial sites shall fulfill the following criteria for inclusion in the study: providing primary medical care (GPs) or specialized in providing diabetes care (DSPs) to at least 300 patients with diabetes mellitus (T1DM and T2DM); utilize diabetes management software with <50% of patients; possess a medical practice computer with internet access and printer; and the on-site investigator(s) and/or medical staff fulfill the necessary formal qualification requirements of investigators to initiate and utilize the PDM process within a medical product study.
GP and DSP sites will be randomly assigned (permuted-block randomization) to the control group (CNL) or intervention group (INT). CNL sites will continue to provide usual care; INT site will utilize integrated PDM (Figure 1).
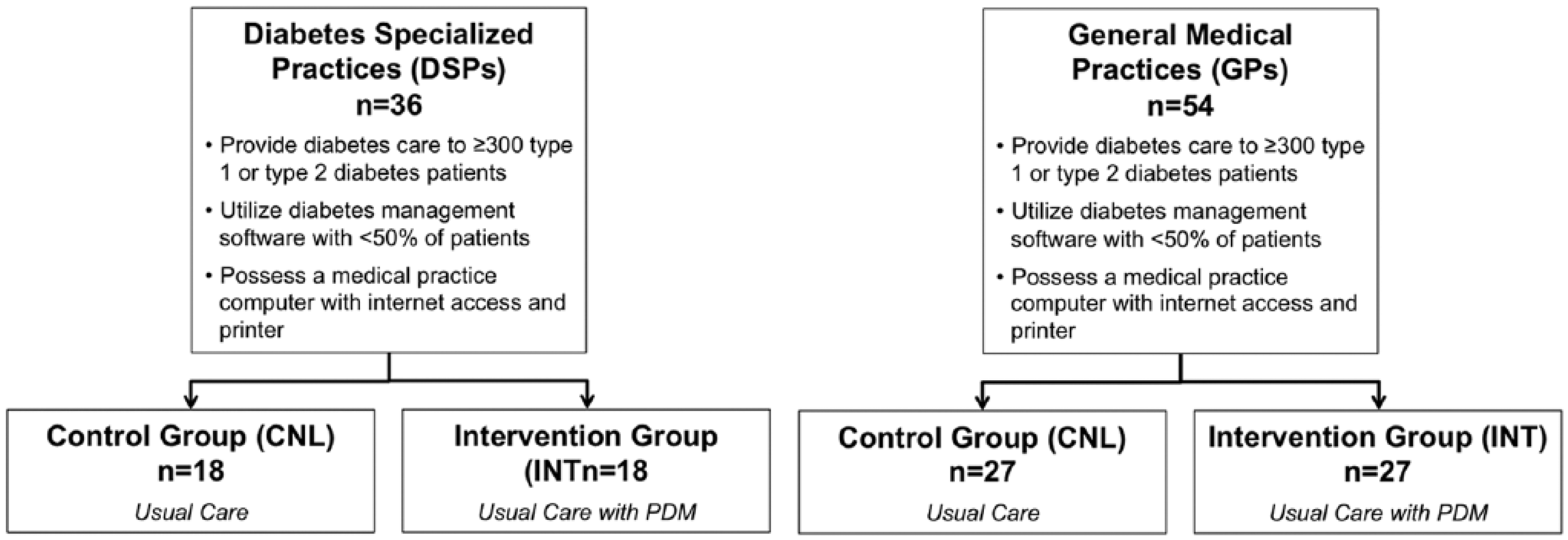
Study design.
A total of 540 DSP patients and 474 GP patients will be enrolled in the studies. Each study site will generate a list of all potential study patients who meet age, diagnosis, and HbA1c inclusion criteria from their individual databases or chart review.
Key inclusion criteria are diagnosis of T2DM; age ≥18 years; HbA1c ≥7.5% / 58.47 mmol/mol (measured during the last 6 weeks prior to study inclusion); insulin therapy for ≥6 months; insured by a statutory health insurance company (GKV) as a statutory or voluntarily insured member or as a family coinsured member; willing and able to follow the study procedures; and signed informed consent. Key exclusion criteria are T1DM; treatment with insulin pump; experience with use of SMBG data management systems/software; diseases, disorders or therapies that could impair ability to adhere to the study protocol and/or lead to erroneous laboratory measurement(s); pregnancy, breast-feeding or plan to become pregnant during study participation; dependency relationship (eg, colleague or family member) with study sponsor or investigator.
PDM Tools
Structured SMBG
Structured SMBG will be utilized by INT physicians in conjunction with individualized “therapy-adapted” testing regimens. Structured testing will include regimens for daily use and utilization of 3-day, 7-point glucose profiles using a validated paper form (Accu-Chek® 360º diabetes management system, Roche Diabetes Care, Indianapolis, IN, USA). 18 A specific structured SMBG regimen (daily and 7-point profiles) will be selected by INT group physicians based on each patient’s current HbA1c value (≥7.5% or <7.5%) and treatment regimen to monitor therapeutic efficacy (Table 1). 19 If the current treatment is found to be inadequate (indicated by HbA1c ≥7.5%), diabetes therapy will be adjusted and a new structured SMBG regimen will be recommended by the physician to accommodate the revised therapy.
Structured SMBG Management According to Treatment.
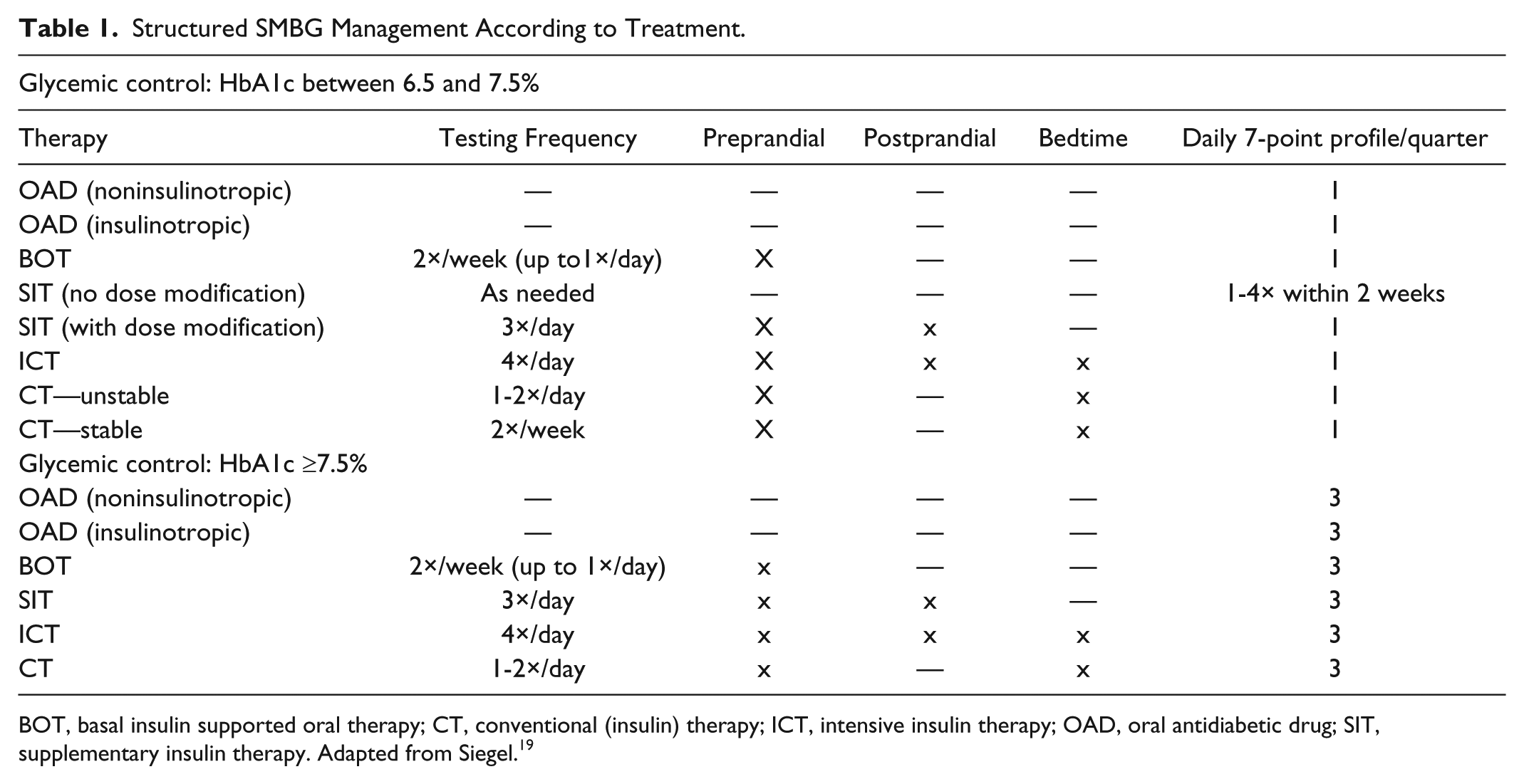
BOT, basal insulin supported oral therapy; CT, conventional (insulin) therapy; ICT, intensive insulin therapy; OAD, oral antidiabetic drug; SIT, supplementary insulin therapy. Adapted from Siegel. 19
Accu-Chek Smart Pix diabetes management system
The system provides systematic electronic evaluation and visualization of blood glucose measurement results and therapy data from compatible glucose monitoring systems. The evaluation is presented as an electronic report with selectable report elements, including graphics, tables and statistics on a computer. The system consists of the following components:
Accu-Chek Smart Pix device reader: With this base device, measured blood glucose data and therapy data (eg, insulin deliveries/dosages) can be read out from the device memory on a (medical practice) computer and systematically evaluated; select report elements can be created, displayed and printed out. All trial sites will be equipped with the device reader. However, only the SMBG measured data will be accessible for read-out and uploaded on a central study server at CNL sites; all other functions will be deactivated.
Accu-Chek Smart Pix (software version 1.2.0): Available only to INT sites, the software program extends the functional scope of the system by providing further analysis methods and reports, particularly the “Status Report” (Figure 2). The Status Report presents an evaluation of each patient’s quality of current glycemic control, focusing on hypoglycemic risk, average measured blood glucose and glycemic variability. INT sites will also be provided with newly developed software that will be used for verifying patient adherence to their structured SMBG regimens.
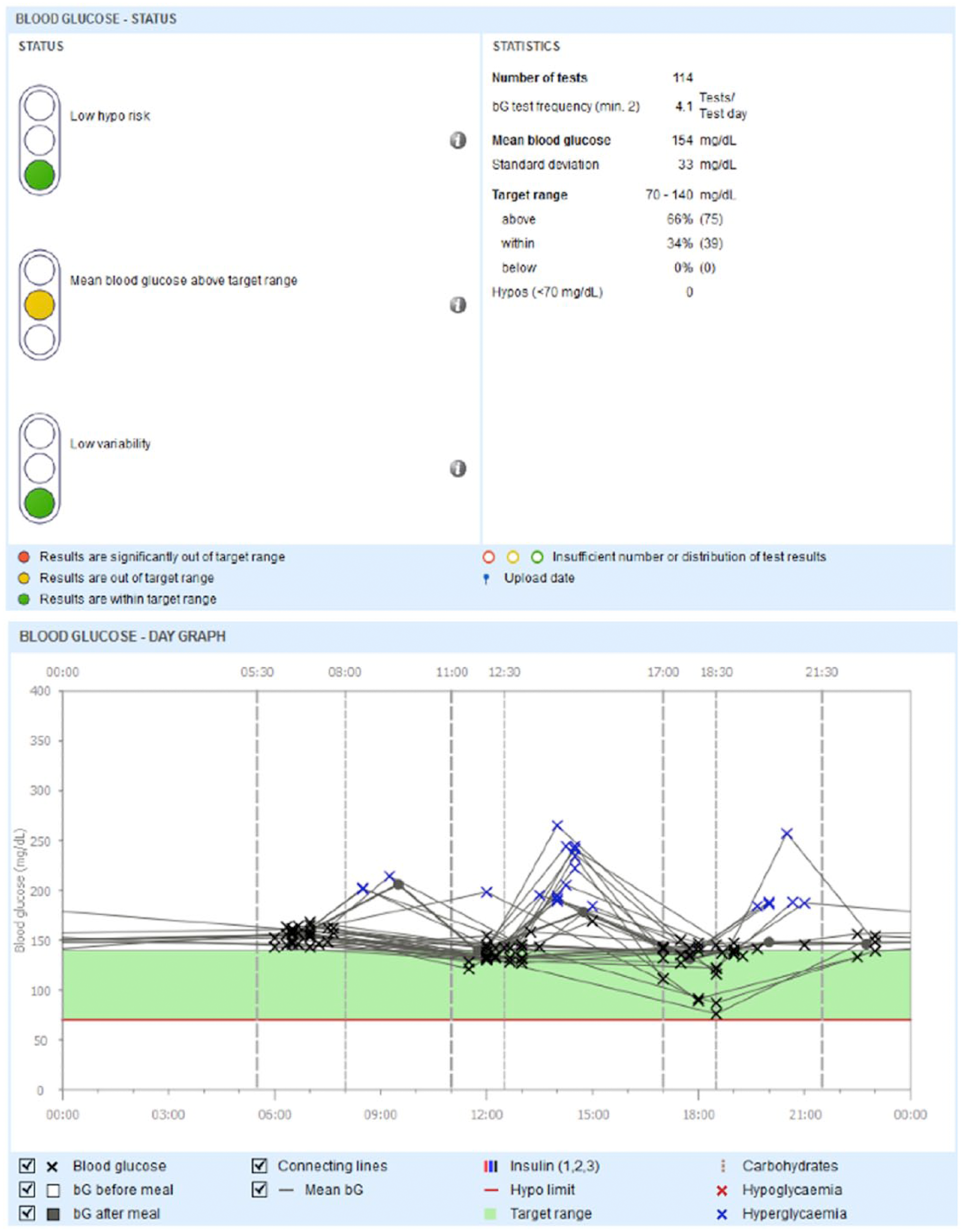
Example view of an Accu-Chek Smart Pix report: SMBG over course of the day (right) and section view of the SMBG risk traffic light (left).
Blood Glucose Measurement Systems
Patients who are currently using a blood glucose meter that is compatible with the data management system will have the option to use their current meter throughout the study. All other study patients will be provided a suitable blood glucose measurement system (Accu-Chek Aviva blood glucose monitoring system, Accu-Chek Aviva Nano blood glucose monitoring system or Accu-Chek Mobile blood glucose meter with an infrared interface; Roche Diabetes Care GmbH). Costs for blood glucose testing materials will be reimbursed by patients’ current insurance/health plan.
Interventions
Patients in both study groups will be treated with usual care under the boundary conditions provided by the GKV with 6 scheduled visits throughout the 12-month study period. Physicians are free to use their judgment in their treatment choices. Patients in the INT group will be treated also by integrated PDM to support therapy assessment and decision-making. Patients in both study arms will be evaluated with the same scales and measures at the same time intervals over 12 months.
The INT group (patients and study sites) will follow the integrated PDM process (based on the Diabetes Management Circle), 13 which comprises 6 recurring process steps (Figure 3). CNL patients and physicians will continue usual treatment according to their customary medical routine (treatment as usual).
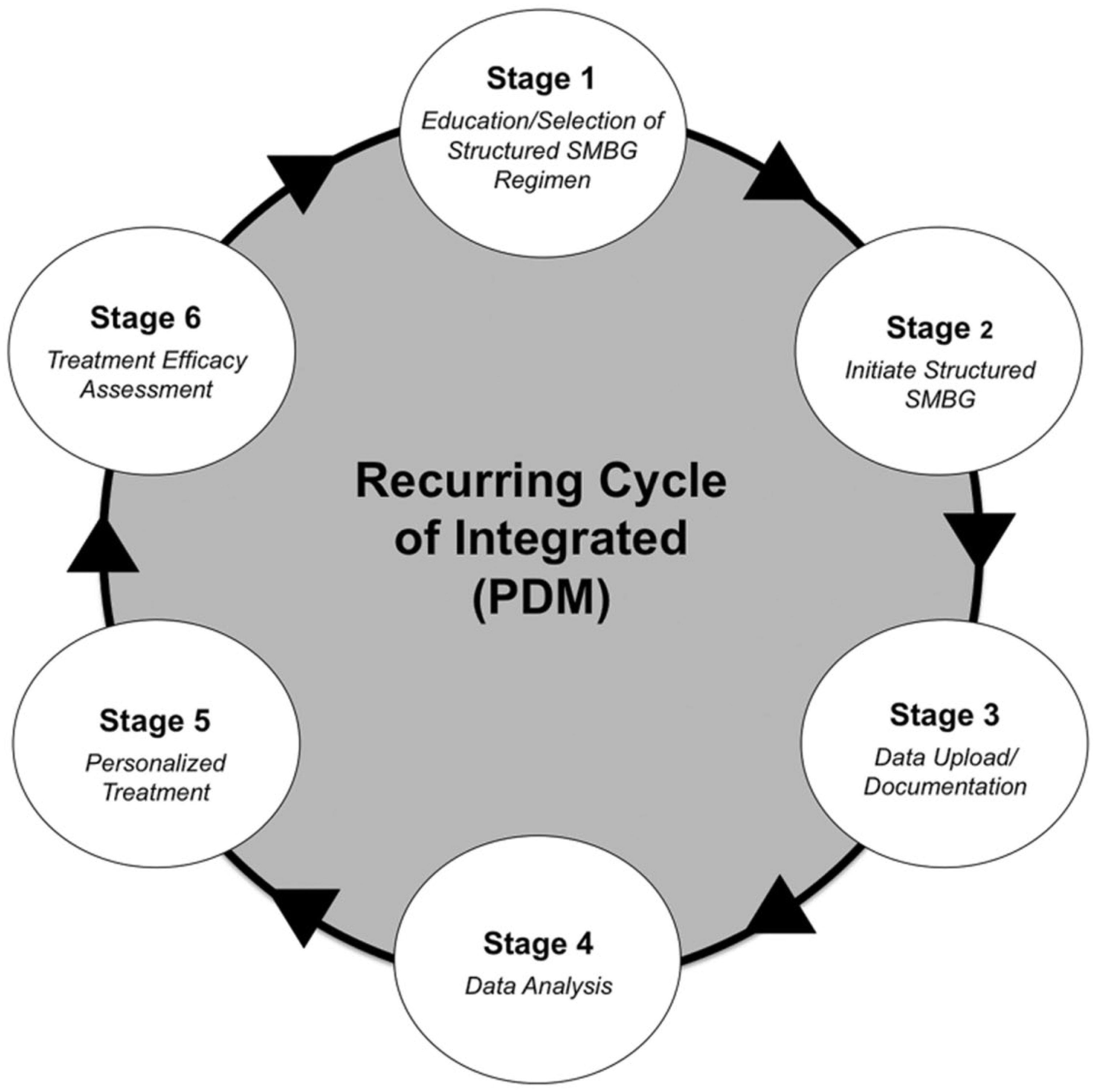
Integrated Personalized Diabetes Management (PDM) Cycle. Adapted from Ceriello and colleagues. 13
Procedures
Study visits will be scheduled as follows: visit 1 (month 0), visit 2 (2-3 weeks following visit 1), visit 3 (month 3), visit 4 (month 6), visit 5 (month 9), and visit 6 (month 12). Figure 4 presents the visit schedule for patients in both study groups.
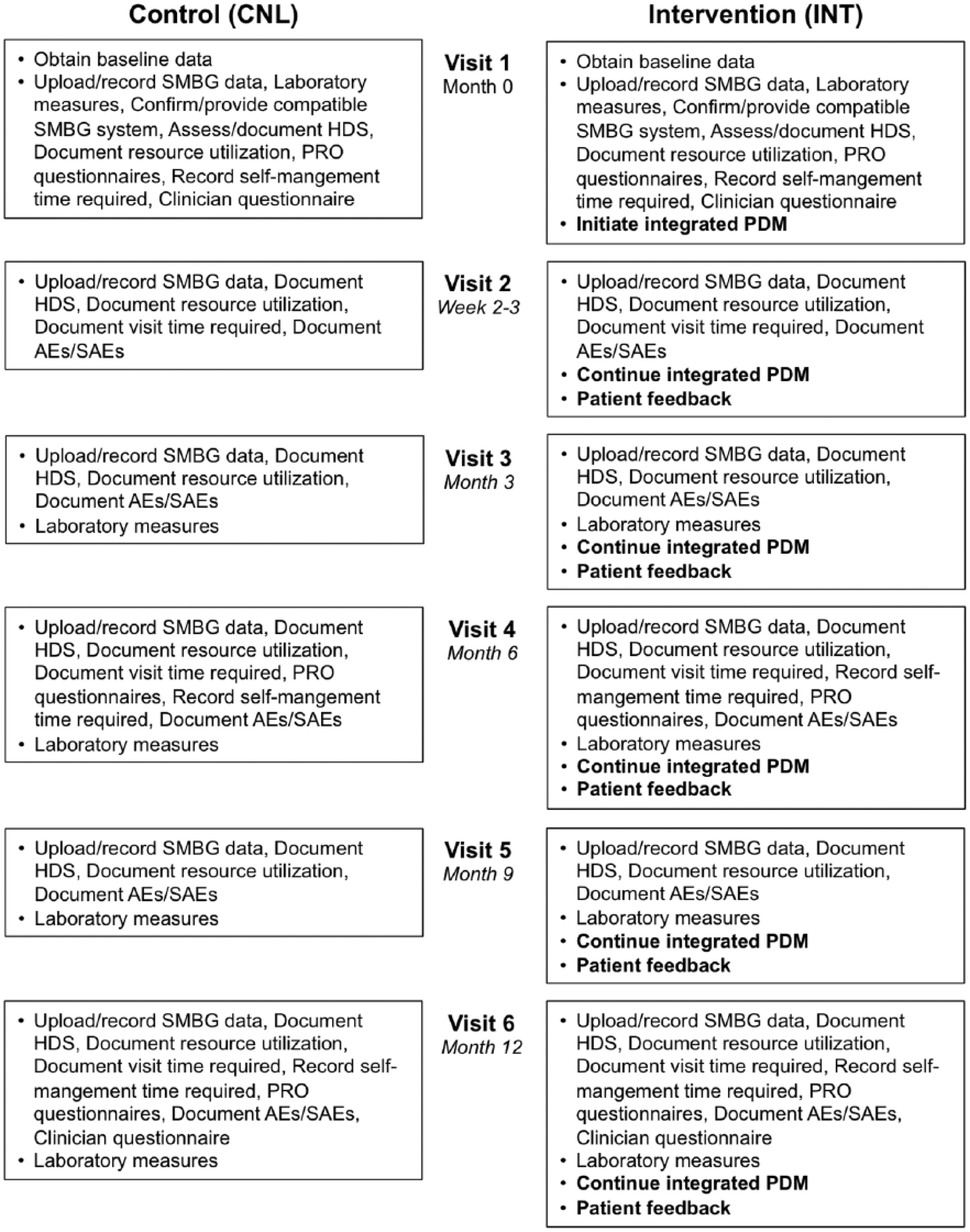
Visit schedule.
All Study Sites
Baseline Measures/Procedures
At visit 1 (baseline), investigators will confirm patient eligibility, describe the study in detail (relevant to each study group) and obtain written informed consent. Patients who do not have a blood glucose measurement system that is compatible with the system will be provided 1 of the systems specified above. Investigators will document patient history (eg, existing complications/comorbidities), changes in type of Insulin therapy and the occurrence of other therapy adaptations (eg, adaption of insulin dosage), record/upload previous SMBG data and instruct patients in proper procedures for blood glucose measurement. Blood pressure and lipids will be evaluated to obtain a more complete picture of each patient’s personal risk profile. Future therapeutic objectives (HbA1c value, blood glucose target range, and other diabetes-related objectives (eg, related to blood pressure and dyslipidemia) will be defined and documented.
Health and demographic status
At visit 1 and all subsequent visits, investigators will upload SMBG data, rate glycemic control, assess/review and document the health and demographic status in all patients. These data will include: weight and blood pressure; smoking status; hypoglycemia events (number/severity according to patient information and/or /documentation); therapy for management of diabetes and diabetic complications; adjunctive therapy (cardiac medication, lipid-lowering medication); socio-demographic data; and GKV insurance data regarding the name of insurance provider, insurance status and participation in a disease management program for diabetes and/or coronary heart disease, or in a family physician model.
Complications and adverse events
At visit 2 and all subsequent visits, investigators will document incidental complications and adverse events (AEs), including the seriousness, intensity, causality, and outcome of AEs.
Laboratory measurements
Measurement of HbA1c, lipid profiles and pregnancy tests (premenopausal patients) will be performed at visits 1, 3, 4, 5, and 6. Measurement of microalbuminuria, high-sensitivity C-reactive protein (hs-CRP) and creatinine will be performed at visits 1, 4, and 6. All measurement will be performed by a central laboratory (Bioscientia, Ingelheim, Germany).
Resource utilization
At all visits, investigators will document diabetes-related referral third parties (eg, cardiologist, podiatrist or hospital) and induced resource consumption (eg, new medications). Assessment and documentation of estimated time required for study visits will occur at visits 2, 4, and 6.
Patient/physician perceptions
Patient-reported outcome (PRO) questionnaires regarding diabetes-specific emotional distress, depression, empowerment and self-efficacy, diabetes treatment satisfaction and health-related quality of life will be administered at visits 1, 4, and 6 (see Secondary Endpoints). Physician questionnaires will be administered at visits 1 and 6 to assess physician perceptions of the integrated PDM process.
INT Study Sites
Investigators will analyze patient SMBG data at all study visits, focusing on glycemic patterns, the Risk Traffic Light findings and treatment adherence reports. Based on these analyses, physicians will recommend changes in therapy and SMBG regimens, as needed, and collaborate with INT patients in confirming/adjusting future therapy objectives. At visits 2-6, INT patients will be queried (via physician-patient dialog) regarding their perceptions of the benefits and use of the PDM tools. At visit 6, patients will be asked to provide feedback on their perceptions of the future benefits of the PDM tools.
Site Training
Subsequent to cluster randomization, representatives of the study sponsor will conduct training sessions at the study sites prior to patient enrolment. If needed, these sessions will be supplemented by regional training events and physician meetings. All sites will receive structured training (via CD videos) in the study protocol, objectives, visit procedures, patient SMBG training and utilization of the Accu-Chek Smart Pix readout device. INT sites will receive additional instruction in the concept and cycle process of integrated PDM, use of the Accu-Chek Smart Pix software, use of the therapy-adapted algorithm for selecting and modifying SMBG regimens and additional recommendations for structured discussion with patients.
Measures
Primary Endpoint
The primary endpoint is change in glycemic control, as assessed by the between-group difference in change in HbA1c from baseline to 12 months. Blood samples will be collected for measurement at visit 1 (month 0), visit 3 (month 3), visit 4 (month 6), visit 5 (month 9), and visit 6 (month 12). HbA1c measurements will be performed by a central laboratory (Bioscientia, Ingelheim, Germany).
Secondary Endpoints
Achievement of >0.5% HbA1c reduction
The proportion of patients who achieve >0.5% HbA1c reduction within each group will be calculated to further assess the clinical significance of glycemic improvement.
Current SMBG and/or SMBG change
SMBG data will be uploaded to a central server for statistical analysis of SMBG utilization. Analyses will focus on SMBG frequency, mean blood glucose values, glycemic variability, number/percentage of blood glucose values within individual target ranges and consumption of blood glucose test strips.
Diabetes-related health status
Measures of diabetes-related health status will include: frequency and severity of hypoglycemia episodes (<70 mg/dl) from measured blood glucose values; frequency and severity of symptomatic hypoglycemic episodes (according to self-reported patient information and/or patient documentation); change in HbA1c, including mean value, time curve, number, and/or percentage of patients below both the agreed-on long-term HbA1c value and the study target value (<7.5%); and subjective investigator assessment of patients’ diabetes-related state of health.
Dyslipidemia and hypertension
Investigators will assess and document prevalence of hypertension and dyslipidemia at baseline and monitor/document changes in blood pressure and blood lipids.
Therapy utilization (diabetes, dyslipidemia and hypertension)
Investigators will monitor and document current medications and changes in medications relevant to treatment of diabetes, diabetes complications, dyslipidemia, and hypertension.
Patient-reported outcomes (PROs)
PRO questionnaires will be administered at visits 1, 4, and 6. Assessment tools will include the following questionnaires: Problem Areas in Diabetes treatment (PAID), 20 Diabetes Empowerment and Expected Self-Efficacy (DEF/SWE), 21 Diabetes Treatment Satisfaction Questionnaire (DTSQ–status and change versions), 22 Hospital Anxiety and Depression Scale (HADS), 23 and Health-Related Quality of Life (SF-12). 24 The PDM-ProValueGP will also utilize the EuroQol-5 Dimensions-5 Levels measure (EQ-5D-5L). 25
Medical practice-related variables
Within each study group, the quality of the treatment process will be assessed from the physician/medical practice staff perspective, using a questionnaire (administered at visits 1 and 6). The questionnaire will obtain physician/staff assessments/perceptions of: information sources used for the review of the current diabetes therapy (eg, laboratory reports, diabetes diary and PDM tools [INT study arm only]); degree of the implementation, personalization, and integration of the cycle process, diabetes treatment decisions, time requirement per study visit and clinician benefit/satisfaction regarding diabetes therapy and SMBG (via validated questionnaire).
Diabetes-related resource consumption
Electronic case report forms (eCRFs) will be analyzed to assess all time and utilization of commercial and private resources associated with treating diabetes and related complications, including: type of antidiabetic medications; consumption of blood glucose test strips; third-party care (nursing, exercise training, nonmedical services); referrals to specialists and hospitals; inpatient treatment (indication and duration [when information is available]); and private costs (patients’ estimated average time spent on self-management activities per day/week, support by partner, friends and/or relatives).
Perceptions regarding use of PDM (INT clinicians)
Investigators will document patient adherence to structured SMBG recommendations. They will also document their frequency of utilizing the PDM tools and provide their perceptions regarding quality of physician-patient communication, benefits of using the PDM tools, and intentions for future use of the tools.
Statistical Analysis
Sample Size Calculation
Estimation of sample size for cluster-randomization-based studies requires estimates of the intraclass correlation coefficient (ICC), because the measurements of the patients within a cluster cannot be assumed as independent variables. Based on the information from various studies an ICC of 0.045 was assumed. 26 A sample size of 216 evaluable DSP patients per arm (12 patients per DSP site) and 189 evaluable GP patients per arm (7 patients per GP site) will have a 90% power to detect a difference of at least 0.4% in change from baseline in HbA1c values over 12 months, assuming a common standard deviation of 1.25%, a ICC of .045, and a R-squared value of .3 for the strength of the relationship between the primary variable and covariates considered in the analysis (HbA1c baseline, gender and age). The different number of patients per study site (12 vs 7 patients) leads to a higher VIF in the DSP study compared to the GP study (1.495 vs 0.27), which explains the higher sample size in the DSP study. Taking into account that up to 20% of the patients will not be evaluable for the per-protocol population, 540 and 474 patients are to be randomized in the DSP and GP study, respectively.
Analysis Populations
The analysis of change in HbA1c and other dependent variables (eg, self-management behaviors) over time will be performed for both the modified intent-to-treat (mITT) and per protocol (PP) populations. The mITT population is defined as all patients in the INT or CNL group with whom the examinations in visit 1 and at least one other visit of visits 3-6 were carried out and data were collected; the HbA1c value must be present during the additional subsequent Visits, so that the data of the patient can be included in the mITT analysis. The PP population is defined as all patients for whom the essential specifications of the study protocol were kept during the study.
Analysis of the Primary Endpoint
The difference in change from baseline in HbA1c at 12 months (Δ HbA1c visit 1 to visit 6) between the patients in the INT and CNL group will be analyzed by means of generalized estimating equations (GEE; population-averaged model) to consider the dependency of the patients within a cluster. HbA1c baseline, gender and age will be considered as covariates in the GEE model. 27 Robust estimators (so-called sandwich estimators) will be provided for the standard errors. In addition, an exchangeable correlation structure will be assumed, wherein this assumption will be verified before the analysis and if necessary, alternative correlation structures will be used. The SAS procedure PROC GENMOD will be used for the analyses. The 95% confidence intervals will be determined for the difference in Δ HbA1c between both treatment groups with the help of the GEE methods. Within the scope of the statistical evaluation, the primary endpoint might be influenced by other collected variables. Provided that additional covariates are identified, these will also be considered in the evaluation. Besides the primary analysis model, where the HbA1c values missing in visit 6 will not be replaced, additional sensitivity analyses will be carried out using last value carried forward methods.
Analysis of Secondary Endpoints
GEE Analyses will also be applied for secondary endpoints (eg, hypoglycemia episodes during the 12 months, mean value of all SMBG measured values within a defined period, percentage of patients with a HbA1c <7.5% at various time points, variables of the 5 PRO questionnaires). With binary end points (eg, HbA1c < 7.5%), a binomial error distribution will be assumed and the effect of the intervention versus usual care will be estimated and tested with a logistic regression model, using a Logit Link Function. With count data (eg, hypoglycemia episodes during 12 months), a Poisson error distribution will be assumed and the treatment effect will be estimated and tested with a Poisson regression using a log link function.
Discussion
In the 2 trials, we will evaluate the extent to which integrated PDM improves metabolic control, diabetes-related health status, dyslipidemia and hypertension, therapy utilization, and patient-reported outcomes in 1014 adult patients with insulin-treated T2DM. The impact of integrated PDM on medical practice-related variables will also be assessed. It is our hypothesis that use of integrated PDM will lead to a medically relevant and statistically significant improvement in glycemic control compared to usual care, and that this approach will improve patient perceptions of and adherence to their diabetes management regimen as well as the quality of the health care delivery process.
Although randomization of patients within a clinic or practice site is the most commonly used study design, this “within-site” approach has the potential to impact investigator behaviors as they become knowledgeable and experienced in both the experimental and the control treatment protocols. This creates a strong potential for “cross-contamination” of study participants (patients and clinicians), which may reduce any potential differences seen between the study groups.15,28 For example, clinicians may unintentionally utilize the knowledge they acquire working with the intervention group patients to adjust their treatment of control group patients. A cluster-randomization study design was chosen to avoid such a bias. This randomization scheme has been successfully utilized recently in other “behavioral-based” trials.5,29
A major advantage of the PDM-ProValue studies is that they will provide information about each step of the diabetes management circle. This will allow us to assess the potential effects of the intervention on all stakeholders (eg, patients, clinicians, payers) and better understand the mechanisms relating to any changes in glycemic improvement, patient perceptions of care and practice efficiencies.
Another strength of the study is utilization of PP analyses in conjunction with mITT analyses. Although most published study reports limit their analyses to the ITT population, this approach does not account for any changes in outcome measures among those patients and clinicians who adhered to the study intervention protocol. Therefore, differences between the mITT and PP analyses should be considered. Our approach, which has been applied in other recent studies,5,30 will enable us to identify any obstacles to implementation of integrated PDM and more fully assess the efficacy of the intervention. With this knowledge, it will be possible to evaluate the effects of the completed intervention and, potentially, identify specific patient and /or clinical site characteristics that are associated with poor patient adherence and/or clinician adherence to the integrated PDM protocol. This information can later be used to develop strategies that would assist patients and practices in overcoming barriers to integrated PDM implementation and utilization.
Patient recruitment for the PDM-ProValue studies began in the middle of 2014. Assuming a 12-month recruitment period, followed by the 12-month study. It is anticipated that study results will become available in late 2016.
Footnotes
Abbreviations
AE, adverse event; BOT, basal insulin supported oral therapy; CNL, control group; CT, conventional (insulin) therapy; DEF/SWE, Diabetes Empowerment and Expected Self-Efficacy; DSP, diabetes specialized practice; DTSQ, Diabetes Treatment Satisfaction Questionnaire; GEE, Generalized Estimating Equations; GKV, Gesetzliche Krankenversicherung; GP, general practitioner; HADS, Hospital Anxiety and Depression Scale; HbA1c, glycated hemoglobin; hs-CRP, high-sensitivity C-reactive protein; ICC, intraclass correlation coefficient; ICT, intensive conventional insulin therapy; INT, intervention group; mITT, modified intent to treat; OAD, oral antidiabetic drug; PAID, Problem Areas in Diabetes; PDM, integrated personalized diabetes management; PP, per protocol; PRO, Patient-reported outcome; RCT, randomized controlled trial; SAE, significant adverse event; SF-12, Health-Related Quality of Life; SMBG, self-monitoring of blood glucose; SIT, supplementary insulin therapy; T1DM, type 1 diabetes mellitus; T2DM, type 2 diabetes mellitus.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: BK, WD, ID, EGS, WS, CGP, and LH serve as paid consultants to Roche Diabetes Care GmbH for their involvement in the study design, study implementation, and preparation of the manuscript. JW, ZD, AM, and IV are employees of Roche Diabetes Care GmbH.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was funded by Roche Diabetes Care GmbH (RDG) and Roche Diabetes Care Deutschland GmbH (RDD), Mannheim, Germany.