
Abstract
HbA1c, a routinely used integrated measure of glycemic control, is traditionally thought to be equivalent to mean blood glucose in hematologically normal individuals. Therefore, particularly as the methodology of measuring HbA1c has been standardized, clinical decisions dependent on mean blood glucose are often predominantly decided based on the interpretation of measured HbA1c. In this commentary, however, now that a more routine method of measuring red cell life span has been developed, we present evidence that the relationship between HbA1c and mean blood glucose is influenced by variation in red blood cell survival even in the hematologically normal. This variation has consequences for the appropriate interpretation of HbA1c in diverse clinical conditions such as the diagnosis of diabetes and management of diabetes in chronic kidney disease.
The review by Heinemann and Freckmann focuses on the current status of HbA1c measurement. To complement their review, this commentary will highlight recent advances in determining the physiologic relationship between HbA1c and blood glucose that are independent of the accuracy of measurement. We then address how this may affect the capacity of HbA1c to serve as a biological marker of glucose for diabetes diagnosis and management of glycemic control in chronic kidney disease.
Summary of Current Application of HbA1c
Percentage HbA1c, a measure of hemoglobin glycation, has been a routine integrated measure of glycemic control for over 30 years.1-5. The prevailing view is that HbA1c is equivalent to mean blood glucose (MBG) and, thus, correlates closely with diabetes complications.2,5-10 HbA1c increments of 1% have been defined as significant with respect to glycemic control11,12 leading to guidelines in which a change of HbA1c from 7% to 8% triggers intensification of diabetes treatment. 13 This is primarily based on the International Expert Committee report on the role of the A1C assay in the diagnosis of diabetes12,14 and the A1c-Derived Average Glucose (ADAG) study, 12 which showed that subjects with normal hematocrits exhibit a strong average linear relationship between HbA1c and MBG (Figure 1). The diagnosis of diabetes is made at a specific HbA1c cut point, 6.5%. However, further inspection of the data in Figure 1 indicates that there are wide confidence limits to that relationship, even in this carefully selected population. For example, at HbA1c = 7%, MBG can vary from 130 to 200 mg/dl and, at MBG = 150 mg/dl, HbA1c can vary from 5.9 to 7.5%. In our view, this variability—observed in a setting where differences among assays do not apply—can overpower the differences used to make clinical decisions including diagnosis of diabetes.
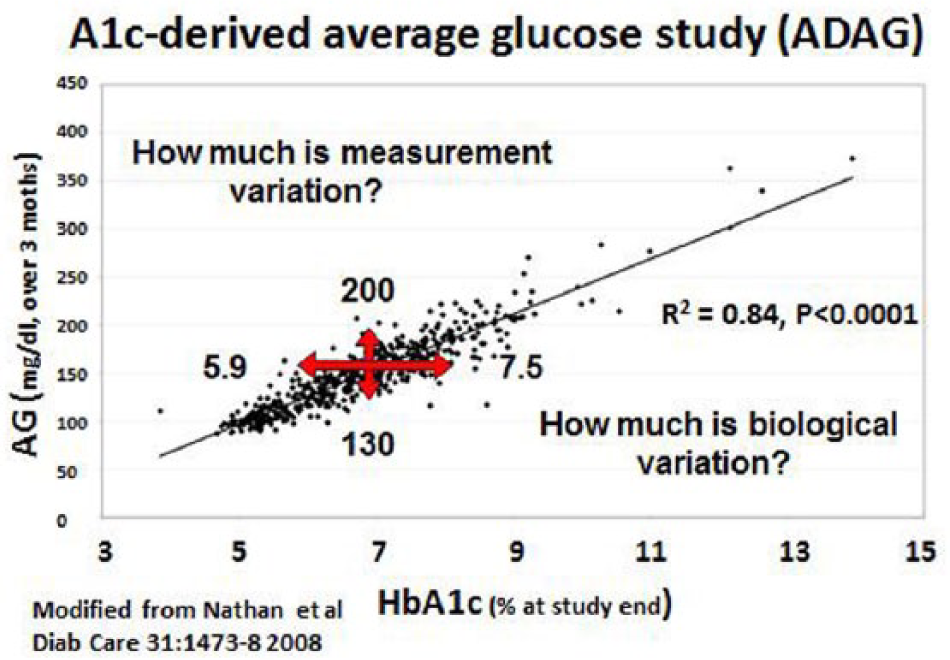
Correlation of average glucose (AG) over 3 months with A1c at the end of the 3-month period. Regression line shows correlation between AG and A1c.
What Determines HbA1c?
The routine peripheral blood HbA1c used clinically to evaluate glycemic control depends on 3 factors: (1) the HbA1c in reticulocytes when they are released from the bone marrow, (2) the synthetic rate of HbA1c (or Hemoglobin glycation rate) as RBCs become older, a function of the glucose concentration to which hemoglobin is exposed which in turn depends on plasma glucose and the transfer of glucose into red blood cells, 15 and (3) the mean age of RBCs in the circulation. 16 There is a widely held belief that RBC life span is stable at “120 days” in hematologically normal individuals. 17 Consequently, the assumption has been made that only hemolytic disease alters RBC life span enough to cause clinically important differences in HbA1c. However, RBC life span is not uniform and clearly has substantial interindividual variation even in people without diabetes.18-25 “Mean RBC age” (MRBC), which can take account of differing survival of subpopulations within an individual person’s RBCs is the more direct determinant of HbA1c than the more familiar RBC “survival” or RBC “life span,” and we will use that term predominantly. 16 Our research suggests that RBC survival, contrary to conventional wisdom, may be a more common source of clinically important variation in HbA1c than is generally recognized.
Four different methods for measuring RBC survival all show considerable variation in hematologically normal people.26-28 The apparent differences in RBC survival have been observed consistently over the past 60 years but there has been 1 critical limitation to interpreting that data: Because either the effort per subject or the risk to making RBC life span determinations has been so great, virtually all such observations were based on a single observation per subject. There has been no way to distinguish the variability within individuals versus the variability between individuals. Only with repeated measures within subject can this long ignored distinction be made and only since patient care decisions in diabetes have depended on small differences in HbA1c has this issue been clinically important enough to merit attention. Specifically, we have shown using a biotin labeling method 27 and a cohort stable isotope approach 28 that MRBC is variable between but consistent within individuals, and, therefore, could require significant adjustment in HbA1c for appropriate interpretation (Figure 2). 28 See Khera et al 28 for methodological detail pertaining to calculation of MRBC and HbA1c adjustment. The implications of this substantial MRBC variability on HbA1c interpretation are potentially far-reaching, but for this review we focus on 2 areas of particular recent interest, diabetes diagnosis and complications risk in chronic kidney disease.
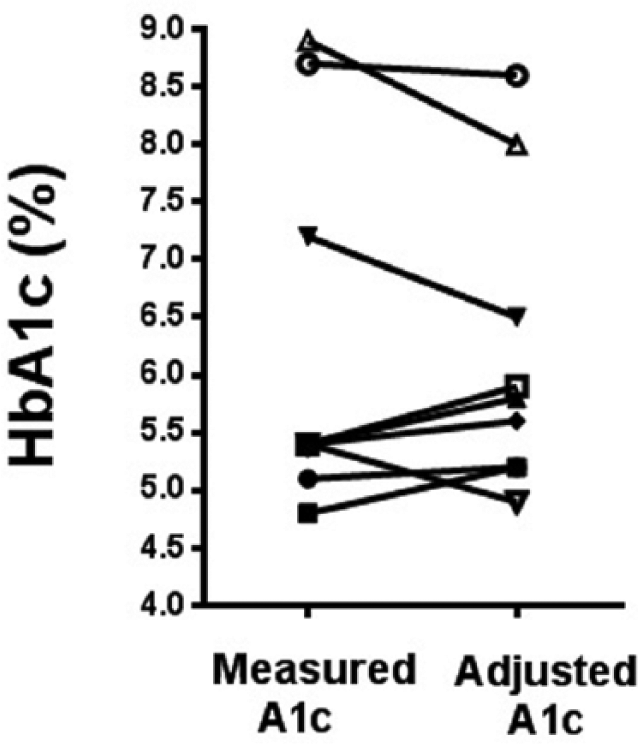
Measured A1c versus A1c adjusted for MRBC. MRBC was measured in a cohort of subjects. These values was used to calculate an adjusted
Current Diabetes Diagnosis
A critical implication of RBC life span variability lies in the use of HbA1c for the diagnosis of diabetes. Because oral glucose tolerance tests (OGTTs) are expensive and inconvenient, the concept of using a single integrated point-in-time measurement like HbA1c for diagnosis is appealing; indeed current ADA guidelines recommend its use. 29 The premise of diabetes diagnosis is to select a cut point in a measure of glycemic control which corresponds to the level at which an increased prevalence of a diabetes-specific disease consequence, namely retinopathy, is detectable. That was originally referenced to fasting and/or postglucose challenge blood glucose concentration. The extrapolation of that to a corresponding HbA1c cut point depends on the extent to which the HbA1c-MBG relationship is the same or differs among all those for whom the test is to be applied. The combination of the publication of the ADAG study and the adoption of the HbA1c standard for diabetes diagnosis has led to many subsequent publications with a very consistent message: 30 while the specificity of diagnosis by HbA1c relative to OGTT is quite high, exceeding 95% in most instances, 31 the sensitivity is fairly low varying predominantly between 40% and 60% among numerous populations. In simpler terms, HbA1c misses 40 to 60 of 100 people with diabetes.
Can we and do we need to overcome this limitation and, if so, what strategies and considerations can guide this process? What are the consequences to those individuals for a false negative diagnosis? While the regression line derived from the ADAG study is likely an excellent estimate of the average of the population (Figure 1), we would propose that the width of the distribution (or “scatter”) of people around that line is due substantially to biologic variation in the population and may be due less to the methodologic/technical limitations of the study (see review by Heinemann and Freckmann). The mechanism underlying where an individual falls in that distribution determines whether or not they will receive the correct diagnosis. If either an MRBC-adjusted HbA1c were measurable by some simple means or a suitable calculated surrogate could be validated, then the hypothesis that MRBC is an important contributor can be tested, potentially leading to a means to narrow the scatter and reduce error in diagnosis. If the evidence supports this hypothesis, it is not far to extrapolate that to improving diabetes management decisions after diagnosis as well. In pathophysiologic settings where there is even stronger evidence for interindividual variation in MRBC, as we will discuss shortly for chronic kidney disease, the benefit of this general approach may be even greater.
The Capacity of HbA1c to Predict Complications in the Setting of Chronic Kidney Disease
Large clinical diabetes trials that excluded chronic kidney disease (CKD) beyond stage 2, have clearly shown that microvascular32-35 and macrovascular6,11 complications are reduced by a tight glycemic control intervention. However a recent post hoc ACCORD study 36 reveals the alarming anomaly that subjects with early renal disease account for essentially all of the excess deaths that occurred in those with type 2 diabetes assigned to the tight control intervention which had previously not been explained. However, despite concerns that aggressive lowering of HbA1c was risky and the increasing awareness that renal disease is associated with artifactual reductions in HbA1c, the excess deaths in ACCORD occurred in those intensively treated whose HbA1c was not low. 37 The operational summary is that CKD and attempts at tight control but not HbA1c lowering were associated with the ACCORD excess deaths. Despite that, Skupien et al 38 found in a prospective observational study that protective effects of glycemic control on nephropathy extend further along the course of its natural history than had previously been recognized. These seeming contradictions make the interplay between diabetes control and renal disease and the resulting clinical decision-making quite complex.
Our studies and those of others suggest that much of the uncertainty regarding glycemic control in CKD may be accounted for by erroneous HbA1c interpretation in this setting. Managing glycemia is a challenge in the setting of CKD, particularly in stages 3 and greater. This is multifactorial and involves issues such as the overall complexity of treatment,39-41 underlying insulin resistance (thought to be caused by among other factors, metabolic acidosis, chronic inflammation and uremic toxins) and a degree of therapeutic pessimism. Although there are some technical challenges that can influence HbA1c measurement such as carbamylation (see the Heinmann review),42,43 it has long been recognized that with advanced CKD, RBC life span is profoundly affected. Ly et al used 51 Cr to show that average red cell half-life is 14.5 days in CKD versus 23.5 days in control. 44 Shima et al, 45 using exhaled carbon monoxide, a breakdown product of heme, as an approximate measure of RBC life span investigated a cross-sectional study in 4 groups: stages 1-2, 3, 4, and 5. Their results showed clearly that life span decreases with progression of CKD 46 and the measured HbA1c decreases almost in parallel. A consensus has evolved that HbA1c is not a reliable marker of glycemic control in CKD.47,48
There have been proposals to replace HbA1c with the use of glycated albumin, fructosamine, or serum albumin-adjusted fructosamine.49,50 At this point however there has not been sufficient validation with comparison of these markers to detailed glucose sampling as with continuous glucose monitoring over sufficient intervals.50-52 An MRBC-adjusted HbA1c validated in the same fashion holds the potential to allow the implications of decades of data on HbA1c and complications to be more broadly generalized, extended to satisfy the unmet clinical needs of multiple large patient populations, such as those whose diabetes diagnosis or whose glycemic management in advanced CKD are currently confounded.
A Number of “Ifs”
This document has been written with more “ifs” than we would use simply in a review of the literature. That reflects our intent to suggest future directions for research directed at improving clinical care of people with diabetes. Key among these is the statement that if either an MRBC-adjusted HbA1c were measurable by some simple means or a suitable calculated surrogate can be validated, then the hypothesis that MRBC is an important contributor to error in diabetes diagnosis and in management of glycemic control in CKD can be tested. Recent stable isotope methods development now makes feasible the assessment of MRBC in populations large enough to answer the basic physiologic and epidemiologic questions made clinically important by the interpretation of progressively smaller differences in HbA1c. Those findings are central to deciding which of the “ifs” will bear fruit for care of people with diabetes and set the level of priority for resources to develop either a “simple means” MRBC or a calculated MRBC-adjusted HbA1c surrogate (with RBC indices as strong candidates for that role).53-56 This approach provides the intellectual basis on which to adjust direction in future years as the needs for diabetes care change. We can already anticipate facing trade-offs between the goal of personalized medicine versus the realities of cost containment as the burden of diabetes in the world expands. It is also possible, however, that studies testing whether tight glycemic control protects residual β-cell function could provide the basis for a new endpoint for the very definition of diabetes. 57 It wouldn’t hurt to be ready for that as well.
Footnotes
Acknowledgements
We would like to thank Robert S. Franco and Christopher J. Lindsell for helpful comments on the topic of RBC life span and HbA1c.
Abbreviations
ACCORD, Action to Control Cardiovascular Risk in Diabetes; ADA, American Diabetes Association; ADAG, A1c-derived average glucose; AG, average glucose; CKD, chronic kidney disease; HbA1c, hemoglobin A1c; MBG, mean blood glucose; MRBC, mean red blood cell age; OGTT, oral glucose tolerance test; RBC, red blood cell.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by grants from VA Merit Award 1 I01 CX000121, NIH R01 DK63088, the Ursich Award Fund (UC Dept. of Medicine), and NCRR Grant 8 UL1 TR000077.