
Abstract
Purpose:
The purpose was to characterize participants’ experiences of a diabetes self-management (DSM) education program delivered via a virtual world (VW) versus a face-to-face (F2F) format.
Methods:
Participants included a randomly selected sample of participants who completed the Women in Control study. Four focus groups were conducted with 32 participants. Four researchers coded the data and conducted a qualitative thematic analysis.
Results:
Four overarching themes were identified. Three domains apply to both VW and F2F formats, including (1) the value of DSM knowledge gained, (2) cultivating DSM attitudes and skills, and (3) the value of peer-derived social support. The fourth domain is labeled positive technological development for DSM (VW condition only). VW and F2F groups both reported mastery of DSM knowledge, attitudes, and skills, and there were no differences in peer-derived social support between groups. The technological aspects of VW participation afforded VW participants a unique sense of personal agency and diabetes self-efficacy not reported by F2F participants.
Conclusions:
DSM education in a VW is feasible and educational outcomes are similar to a F2F classroom experience. Furthermore, learning DSM skills in a VW offers unique advantages in supporting personal agency for health behavior change. Further research is warranted.
Keywords
The prevalence of type 2 diabetes mellitus (T2DM) in the United States is disproportionately high among minority women. From 1988 to 2006, the prevalence of diagnosed T2DM nearly doubled among non-Hispanic blacks and Hispanics, for whom rates of T2DM are now approximately twice that of non-Hispanic whites. 1 Minority women also report low rates of physical activity, low consumption of healthy foods, and low levels of clinical self-efficacy for diabetes self-management (DSM), all significant risk factors for poor glycemic control. 2
Expert guidelines recommend DSM education to support health behavior change, including promotion of physical activity and reduction in both caloric intake and weight as foundations of treatment for T2DM. 3 Medically underserved persons with T2DM are particularly at risk for complications as they commonly face limited access to recommended DSM support and comprehensive clinical care.4-7
Prevalent disparities in diabetes outcomes also represent a challenge to health care providers to develop healthy living and self-management programs tailored to meet the cultural and social preferences and needs of ethnically diverse communities.8,9 Technology offers new means of delivering chronic disease self-management education, with computer-based self-management support having demonstrated benefits in improving health behaviors and glycemic control.10,11 A recent review of eHealth interventions indicates these programs have a positive impact on physical activity and dietary behavior; a Cochrane review reached similar conclusions. 12 To our knowledge, however, only a handful of researchers have begun to rigorously test the possibilities of avatar-based virtual world DSM education.13-15
A virtual world (VW) is a 3D, computer-based simulated environment which presents perceptual stimuli to the user, who in turn can manipulate elements of the modeled world. 16 Second Life is an example of a free, open-access, avatar-based VW that supports a high level of social networking and immersive interaction with information. Avatars have been defined as online manifestations of self in a VW and are designed to enhance interaction in a virtual space. 17 With more than 15 million global users, Second Life is the most popular VW platform used by adults, where 40% of users are women with average age > 35 years old.18,19 More than 200 institutes of higher education also utilize Second Life. 20
Preliminary evidence shows that VWs influence “real-world” behavior 21 as they are intrinsically designed to test behavior modifications anonymously among peers and restructure old habits.22-24 Still, the potential capability of VW self-management training and support compared to standard patient education approaches are largely unknown. To fill this gap, our team conducted Women in Control, a pilot randomized controlled trial (RCT) that compared the feasibility and potential efficacy of a DSM intervention for Black and African American women with uncontrolled diabetes via a VW versus a face-to-face (F2F) format. 25 Details of the methods used for the original comparative effectiveness pilot study and results of the clinical trial are reported elsewhere. 25 This article describes findings from a qualitative assessment of participants’ experiences.
Methods
Sample
We enrolled 32 focus group participants from the pool of 89 African American women who participated in the original Women in Control RCT. Following completion of the pilot study, we contacted a randomly selected list of participants using convenience sampling for focus group interviews. Focus group assignment was determined on a first-come first-served basis and stratified by study arm assignment (VW or F2F). We attempted to contact 74 participants (83% of 89 original study participants); we could not reach 26 potential participants, we spoke directly with 48 women (54%), 38 were interested. We enrolled and randomized 32 women to form 4 focus groups (2 with VW participants and 2 with F2F participants) with 8 participants in each group. Sample size was based on feasibility and average qualitative sample size methods. 26 Participants received a $25 incentive and taxi vouchers for transportation to and from Boston Medical Center to compensate for participation. The Boston University School of Medicine/Boston Medical Center Institutional Review Board approved these procedures.
Data Collection and Instrument
Focus groups were chosen as the primary data collection method. Focus groups were stratified by study arm: VW and F2F. We developed an interview guide to assess specific aspects of the participants’ experiences in the study. We used open-ended, semistructured questions to facilitate the emergence of themes of importance to participants (see Table 1). These questions were followed by more specific prompts or cues to solicit data about items of interest to the research team that had not yet been mentioned. A member of the research team (SEM or LB) led the four 90-minute focus groups; another team member took notes (MCR). Discussions were audio-recorded and then transcribed verbatim.
Focus Group Interview Questions.
Qualitative Analysis
We used thematic analysis to analyze the results of the focus groups using the qualitative data management software NVivo 9. 27 Four researchers used open coding of 2 of the transcripts to form a codebook with which to code all 4 focus group transcripts. As a research team, we agreed that we achieved a high level of “saturation”—when the collection of new data does not shed any further light on the issue under investigation—after coding 1 VW and 1 F2F transcript. 26 NVivo reported average internal coding agreement greater than 90%. We then applied the concept of thematic networks within NVivo to develop a hierarchical structure of codes that linked organizing themes to global, overarching themes. 28 Table 2 lists the 6 phases of thematic analysis.
Phases of Thematic Analysis.
Results
A total of 32 Women in Control participants attended focus groups. Of these, 16 women were in the VW study arm and 16 women were in the F2F study arm. Sample characteristics for focus group participants are summarized in Table 3.
Baseline Focus Group Characteristics (%).
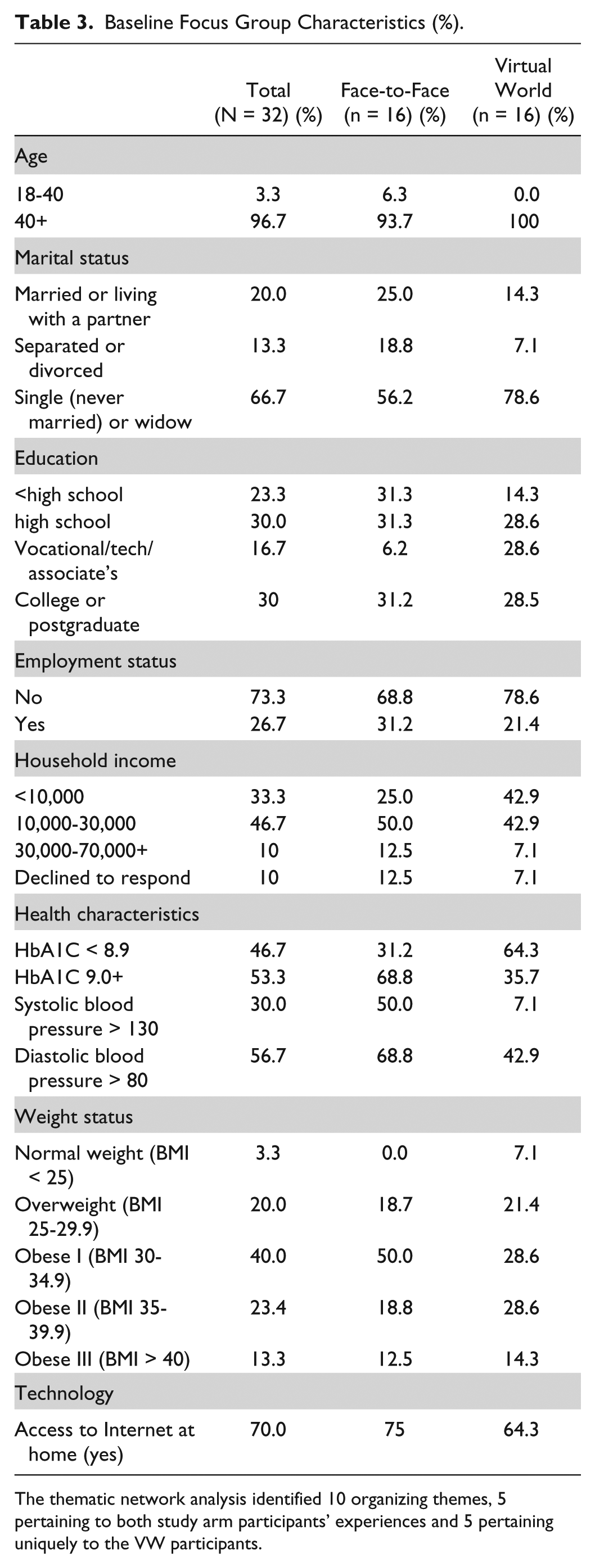
The thematic network analysis identified 10 organizing themes, 5 pertaining to both study arm participants’ experiences and 5 pertaining uniquely to the VW participants.
The 5 themes similar to all participants included (1) impact of DSM curriculum, (2) ability to share knowledge with friends and family, (3) mastery of self-care behaviors related to DSM, (4) valued social support, and (5) being with women of the same ethnicity or culture. The 5 themes pertaining to the VW participants only were (6) overcoming fear of technology and computers, (7) learning to use and work with computers, (8) trying new, fun activities with avatars, (9) experimenting with identity through avatars, and (10) increased sense of personal agency and clinical self-efficacy (see Figure 1).
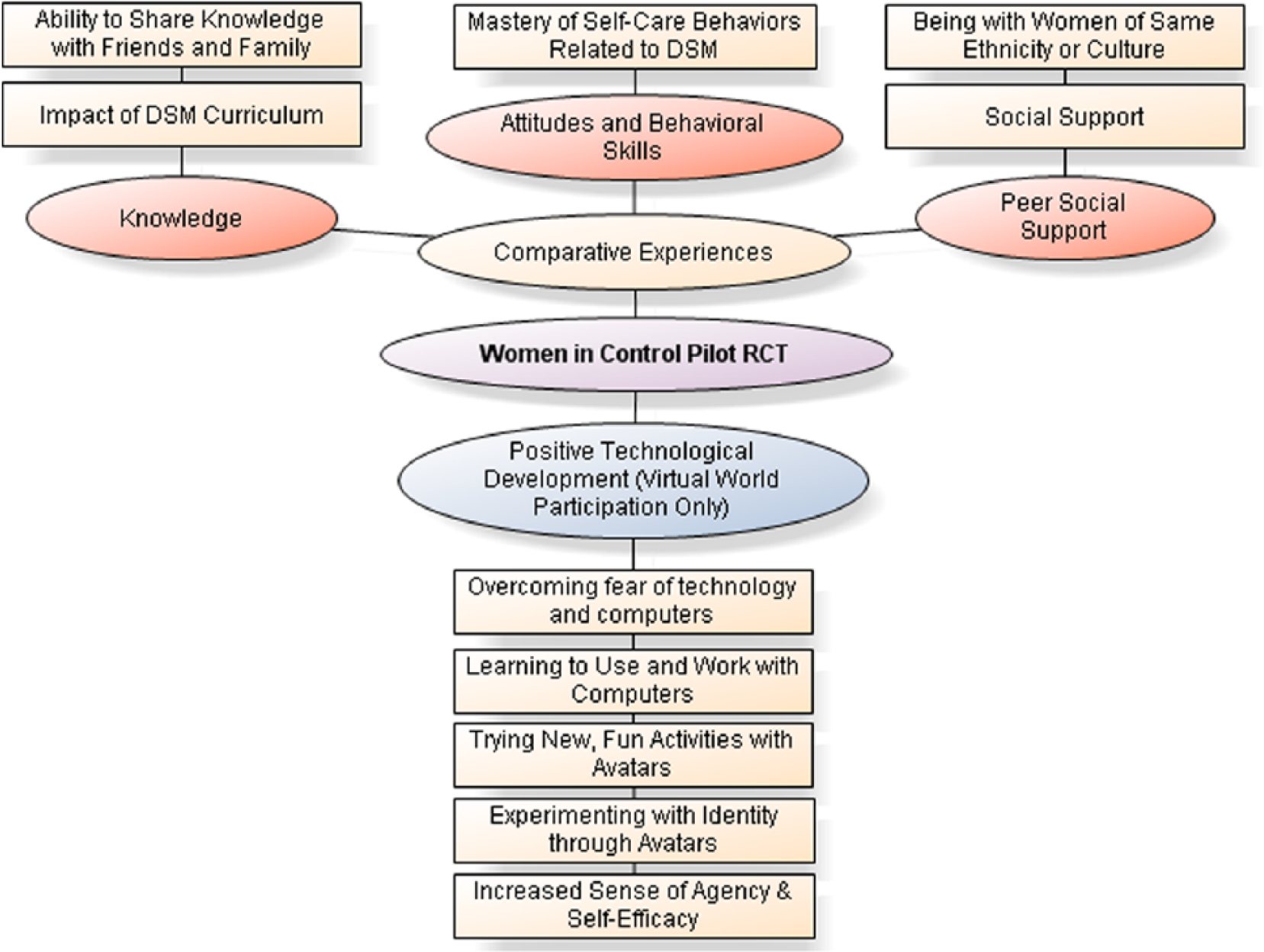
Thematic network.
We then identified 4 overarching domains: 3 comparative domains (VW and F2F participants) and 1 domain characterizing the unique technological experience of virtual DSM learning. The 3 domains characterizing participants’ similarities in the DSM training experience were related to acquiring the knowledge, attitudes and skills to self-manage diabetes, including (1) diabetes knowledge (impact of the curriculum), (2) DSM attitudes and skills, and (3) peer social support. We named the fourth domain uniquely pertaining to VW participants’ positive technological development (PTD) for DSM, based on an educational technology pedagogical framework developed by Bers et al (see section IV of the results), explaining how educational interactions with technology can enhance an individual’s self-efficacy. 29
I. DSM Knowledge
Participants in both groups reported having learned valuable information about how to manage diabetes. The VW participants described the VW setting of Second Life as just as feasible a platform to learn about DSM as traditional F2F interventions. Both groups of participants reported new perspectives regarding the ability to learn and retain information related to DSM.
1. Impact of DSM Curriculum
This program . . . really helped me figure out for the first time really and truly what diabetes really does to your body. (VW participant)
Furthermore, both groups also endorsed their desire to share their new knowledge with family and friends with diabetes, confirming the investigators’ rationale to target women for the intervention because of the tendency for women to influence the health care of other family members.
2. Ability to Share Knowledge with Friends and Family With Diabetes
I feel more equipped that if [my family does] become diabetic, I can deal with it. I can help them with their . . . regimen. It won’t be something that I don’t know anything about. (VW participant) What I’ve learned I hope to be able to pass it on to the rest of my family. I’ve already shared with a friend of mine who has diabetes. . . . I share back and forth with him over the phone telling him about how important it is to watch what you eat, take your medications, and stay active, keep the body moving and you can live a much better life. (F2F participant) You believe in it so much that you start spreading the word to family and friends. It’s like spreading the gospel. (F2F participant)
II. DSM Attitudes and Behavioral Skills
Both groups of participants supported the feasibility of the intervention formats to promote DSM attitudes and behavioral skills through the mastery of self-care behaviors such as at-home glucose monitoring, adherence to medications, increased physical activity, ability to comprehend a food label, and reduction in caloric intake. Both groups also reported DSM behavioral changes.
3. Mastery of Self-Care Behaviors Related to DSM
I want to live and I’m willing to do whatever I have to do every single day to live. I take my sugar regularly. That’s something I learned – it was hard ‘cause it’s not easy sticking your fingers or taking it from your arm. I had an issue about taking insulin because I don’t think anybody wants to stick themselves. (F2F participant) The study helped us step by step get our diabetes under control, each week it was something different like checking your sugars, making it a goal, or looking at how many calories or how much fiber and carbohydrates. . . . I feel that’s very helpful because you try to take your medicine, take your blood sugar, and take your insulin at one time and it’s actually a process . . . to work it into your daily routine. (F2F participant) At first I thought this is going to be ridiculous, but then I found out how important it was, because I never paid attention to when I went to the grocery store on the labels and reading them, what’s in there and how many calories and how much sugar, because I’ve looked up stuff and been like oh, that’s a lot of sugar. I don’t want that. (VW participant)
III. Peer Support
Both cohorts reported similar values and experiences with peer-derived social support and expressed the importance of being together with women of the same ethnicity and diagnosis. Importantly, VW participants expressed attitudes suggesting that the VW intervention delivery format provided peer support that was just as intimate as F2F interactions, and appreciated the convenience, comfort, and anonymity of engaging in the program from home. Participants in both groups shared that the peer support allowed them to adopt compassionate attitudes—having learned that they were not alone in their struggle—which led them to want to participate more fully.
4. Valued Social Support
I was devastated when I found out I had diabetes and I was listening to everyone else and I was like I’m not alone and that made me want to participate even more. (VW participant) You don’t feel like you’re alone anymore . . . even though you were at home . . . you still weren’t alone because the avatars were walking around. (VW participant) I could sit up and do what I had to do and be comfortable and it was raining and it was cold and I was in my bed talking to you guys and it was great. I loved that, in my own comfort. (VW participant)
5. Being With Women of Same Ethnicity/Culture and Diagnosis
You were talking to other women about the same issues you have . . . and they were there to encourage you. . . . To say good things to help you to go forward, so it was absolutely . . . wonderful . . . nobody judged you. (VW participant)
IV. Positive Technological Development: The Unique Capabilities of VW DSM Learning
We asked the VW participants to characterize their experiences using Second Life for the DSM education. We analyzed responses and categorized them in a separate domain labeled “positive technological development for DSM” because of the consistency of these themes with Bers et al’s pedagogical framework. 29 Within this domain are 5 themes that describe the unique advantages of learning with VW technology.
We hypothesize that the themes may be explained by the theoretical framework of PTD. 29 PTD posits the cultivation of 6 personal assets acquired through developing technological fluency to express oneself creatively, use technology to make shared decisions with peers, and visualize and enact transformation for oneself and others through applied practice. These assets include competence and confidence using technology to compassionately connect with peers and contribute to society through solving social problems. This type of applied learning in a personalized context is associated with successful behavior change and improved self-efficacy. 30
We theorize that the use of VW technology translated to an enhanced sense of personal agency or self-efficacy for the VW participants compared with the F2F group. We defined self-efficacy as the sense of one’s ability to control diabetes. 31 For example, VW participants reported lack of experience using technology and fear of using computers. Some women adopted new behaviors (increased physical activity) that they tried via their avatar. For example, 1 woman described that visits to Club One (VW athletic center) led her to join a gym. Participants also described experimenting with their identity as avatars, such as making their avatars appear thinner. We theorize that this empiric evidence supports the premise that VW self-management education leads to a higher likelihood of real-world behavior change. The PTD domain subthemes included the following:
6. Overcoming Fear of Technology
I never used [a computer] before now. I was scared at first, but you all talked me through it and I was amazed . . . it was so comfortable being at home . . . your group is there and you’re conversing and it’s comfortable. (VW participant)
7. Learning to Use and Work With Computers
Finding out about diabetes and going through it on the computer as an avatar was a new beginning for me. I wasn’t ever computer literate, I mean I was computer illiterate, well this is something new. This is part of the new me, to me getting into me. (VW participant) If it wasn’t for the diabetes, I wouldn’t be into the computer. (VW participant)
8. Trying New, Fun Activities in a VW With Avatars
[Club One] was so cool, and I don’t go to gyms. You know it was nice to do a little working out. (VW participant) Maybe the intention was it would help to encourage you to exercise. . . . I mean if we can see it . . . you know maybe we’re going to get out and we’re going to exercise . . . we’re going to try it. Well, I did. I exercised. I joined the Y and went and worked out. (VW participant)
9. Experimenting With Identifying Using Avatars
[The avatar] represented the change that you [were] going to make in your life towards the diabetes. (VW participant) [Having an avatar] was absolutely cool because you got to be . . . whoever you wanted. You could change your outfit, your hair . . . you could weigh anything you wanted. You could put on clothes that you wouldn’t normally wear. . . . If I could only be built like this for real. (VW participant) I tried to make myself thinner three times. (VW participant)
10. Increased Senses of Personal Agency and Clinical Diabetes Self-Efficacy
When you’re in Second Life you know what Second Life is. Second Life is women in control of their diabetes. (VW participant) If your avatar does it, you can do it. (VW participant)
Technological Difficulties With Learning in a Virtual World and Suggestions for Improvement
While participant response was essentially positive regarding curriculum content and participation condition (F2F vs VW), VW participants did report technical difficulties largely related to audio (headset) and chat capabilities of the VW platform. However, technical staff—who were immediately available during sessions—quickly solved issues for participants, suggesting that success and satisfaction interacting with VW technology are contingent on having a communicative and user-friendly technical staff to address audiovisual barriers to participation.
I never had [issues with the technology] . . . they troubleshooted it right away. (VW participant) Some of it was troubling to me because I could hear other people [but] I couldn’t participate after writing out all my notes . . . and everything that I wanted to participate in, but they used certain technology to get to me in order for me to respond. (VW participant) I had problems with my earphones. And so what they did, they printed it [instant messaging], what everybody was saying on the computer so you can see what’s being said so you wouldn’t miss out on anything. So you had to type . . . what you wanted to say. (VW participant)
Suggestions for improvement mainly did not pertain to curriculum or technological aspects of participation but instead primarily dealt with interpersonal, relationship-centered aspects of managing diabetes. For example, 1 woman in the VW group shared that she thought it would be great if those who had completed the program could assist future participants, acting as peer-guides. Another participant (F2F condition), felt it would be helpful to include women with controlled diabetes into the group to learn how they successfully self-manage diabetes. Last, both groups discussed the possibility of involving their families in this research study. As mentioned earlier, many participants shared information with friends and family, but ultimately expressed mixed perspectives whether to invite family members (both with and without) diabetes to participate or expressed concerns with ongoing difficulty managing their own diabetes in nondiabetic households, perhaps recognizing the greater interpersonal factors involved with chronic disease management that extend beyond oneself.
I think it would be great if we—as those that went through the program already—were able to come in and speak with a class that’s already in session or getting started. (VW participant) The only thing I wish they would have [is] people that were managing their diabetes in with us that weren’t managing so that we could learn what they were doing right. I met several women that were denied the program because they had their levels all set. (F2F participant) Some family members [want to participate] and some . . . you just [need] to leave everybody home. Because you want to have a different view, a different opinion . . . [from] somebody that’s just in the same place as you. (VW participant)
Conclusions
This qualitative study assessed the experiences of 32 Black and African American women who participated in the Women in Control pilot RCT, which compared the feasibility of a DSM intervention in a VW platform (Second Life) versus a traditional F2F setting. Both groups reported high satisfaction with the knowledge gained from the DSM education and both reported changes in DSM behaviors and similar positive experiences of peer support. Virtual participation afforded peer support reported to be more accessible, anonymous, and convenient. While both cohorts received a laptop and basic computer training, F2F participants did not report using the computer to access DSM information or interact with peers online.
Our study has limitations which should be acknowledged. First, we used convenience sampling for recruiting our participants for these focus groups. This approach could introduce responder bias and limit generalizability. However, given the limited experience in the field of DSM education using VW technology, this empiric evidence provides important insights and preliminary data for designing future studies of VW learning environments for DSM education. Similarly, while our qualitative results are promising, we cannot state with certainty that the use of VW technology resulted in greater DSM behavior change compared to F2F learning using a qualitative study approach. Nonetheless, our results support a conceptual framework (PTD) that further explains how a VW learning environment might lead to greater increases in diabetes self-efficacy and adoption of DSM behaviors compared with F2F learning beyond the convenience of remote access to DSM education.
In summary, this work suggests that novel health care applications of VW technology afford unique opportunities to deliver information to improve diabetes knowledge, cultivate favorable attitudes and behavioral skills and receive peer support, all required by patients for successful management of chronic illness. One participant poignantly reported the VW allowed her a new beginning. Thus, this study lends support for the acceptability of technology-based interventions to enhance DSM behaviors among low-income Black and African American women with limited experience working with VW technology.
Second Life means a lot more than just Second Life. You know for some of us, it’s a new beginning of a second life for us. Second Life is a second life. (VW participant)
Footnotes
Abbreviations
DSM, diabetes self-management; F2F, face-to-face; PTD, positive technological development; RCT, randomized controlled trial; T2DM, type 2 diabetes mellitus; VW, virtual world.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by NIH grant 1RC1LM010412-01 to JW and MCR. SEM is supported by a mentored career development award funded by the Agency for Healthcare Research and Quality (1K08HS019771-01).