
Abstract
Diabetes is an increasing public health problem, and insulin is the mainstay for treatment of type 1 diabetes. In type 2 diabetes treatment, insulin therapy is used after oral or other injectable agents become inadequate to achieve glycemic control. Despite the advances in insulin therapy, management of diabetes remains challenging. Numerous studies have reported low adherence and persistence to insulin therapy, which acts as a barrier to successful glycemic control and diabetes management. The aim of this targeted review article is to provide an overview of adherence and persistence to insulin therapy in people with diabetes and to discuss the impact of the emergence of a new connected ecosystem of increasingly sophisticated insulin pens, glucose monitoring systems, telemedicine, and mHealth on diabetes management. With the emergence of a connected diabetes ecosystem, we have entered an era of advanced personalized insulin delivery, which will have the potential to enhance diabetes self-management and clinical management. Early systems promise to unlock the potential to address missed or late bolus insulin delivery, which should help to address non-adherence and non-persistence. Over time, improvements in this ecosystem have the potential to combine insulin data with previously missing contextualized patient data, including meal, glucose, and activity data to support personalized clinical decisions and ultimately revolutionize insulin therapy.
Introduction
Diabetes mellitus is a major public health problem that affects 415 million people worldwide 1 and approximately 34.2 million people (10.5% of the population) in the United States. 2 It is characterized by hyperglycemia and can lead to morbidity, mortality, and reduced quality of life. Type 1 diabetes (T1D) is an autoimmune disease in which pancreatic islet β-cells are destroyed through T-cell mediated mechanisms, leading to lifelong exogenous insulin dependence, whereas type 2 diabetes (T2D) is characterized by insulin resistance and progressive loss of β-cell function with subsequent insulin deficiency. For the treatment of T1D, the American Diabetes Association (ADA) recommends multiple-dose basal and bolus insulin injections or continuous subcutaneous insulin infusion. Although insulin is usually not the first-line treatment for T2D, as the disease progresses, oral or non-insulin injectable treatment may become inadequate and often need to be intensified by adding insulin to the treatment regimen.3-6 Insulin therapy thus remains the cornerstone of diabetes management, and over the past 100 years, significant progress has been made in its development. 7 Despite these advances, many people with diabetes fail to achieve adequate glycemic control. It has been reported that 50%-73% of people with T2D, treated with basal insulin, fail to meet glycemic targets. 8 A primary care database analysis of 4,062 people with T2D found that after one year of basal insulin therapy, only 7.2% reached the target of glycated hemoglobin (HbA1c) ≤6.5%. 9
Although insulin treatment is the oldest and one of the most effective glucose-lowering therapies, a large proportion of people interrupt or discontinue treatment shortly after initiation.10-12 Adherence and persistence are the two patient behaviors that play a vital role in achieving good glycemic control. Adherence is defined by the World Health Organization as “the extent to which a person’s behavior-taking medication, following a diet, and/or executing lifestyle changes, corresponds with agreed recommendations from a healthcare provider.”13,14 Insulin therapy has unique adherence challenges. A study published in 2015 reported that non-adherence to insulin therapy may occur in up to 44.3% of T2D patients and is associated with both poor glycemic control and increased microvascular complications. 15 Persistence refers to continuing the treatment for the prescribed duration. It may be defined as “the duration of time from initiation to discontinuation of therapy.” 16 Perez-Nieves et al. reported that only 20% of people initiating basal insulin continued treatment within the year after initiation. 11 Similar to non-adherence, non-persistence with insulin therapy may also cause poor glycemic control, which can further lead to increased risk of diabetic complications. 12
The aim of this targeted review article is to provide an overview of adherence and persistence to insulin therapy in people with diabetes, with emphasis on the clinical and economic impact of insulin pen advances and emerging mobile health (mHealth) technology use in this population. A connected insulin pen delivery ecosystem may be defined as the combination of insulin pens and pen attachments (hardware) and the software that integrates with this hardware, including mobile health applications and internet web application that support people living with diabetes and their health care providers by creating personalized insulin dose recommendations. The authors believe that this knowledge can benefit healthcare providers to help and support people with diabetes in achieving their glycemic targets. This review is based on a targeted literature search of previously conducted studies. We searched PUBMED with the keywords adherence, diabetes, insulin, digital health, mobile apps, and persistence.
Insulin Adherence and Persistence
Current Scenario: Non-Adherence and Non-Persistence Are Prevalent
The National Health and Wellness Survey of 1198 people with T2D reported that each 1-point drop in self-reported medication adherence (using the Morisky Medication Adherence Scale) was associated with 0.21% increase in HbA1c, as well as 4.6%, 20.4% and 20.9% increase in physician, emergency room, and hospital visits, respectively. 17
A study of adherence conducted as part of a systematic review of 27 studies, published in peer-reviewed journals, concluded that adherence to diabetes medication remains an ongoing problem. Of the 27 studies identified, only six (22%) reported an adherence rate of ≥80%. 18 Several other studies, across all age groups, have shown that the adherence rate and persistence to insulin therapy is low in both T1D and T2D. A facility-based cross-sectional study conducted at pediatric diabetes clinics in Uganda reported that the insulin adherence rate was 52.0% among children (0-9 years) and adolescents (10-19 years) with T1D. 19 A retrospective study evaluated adherence and persistence to insulin therapy among 24192 insulin-naive adult Chinese people with T2D. The study reported that adherence (30.9%; mean medication possession ratio [MPR], 0.499) and persistence (53.0%; mean time to non-persistence, 230.3 days) were poor among this patient population. 20 A recent study in adult people (n = 21363) with T2D (utilizing the US-based Truven Health MarketScan Research Database) reported that 33.8% people were adherent to basal insulin treatment, over the three-year period post-insulin initiation. 21 However, it is very challenging to measure insulin adherence and persistence due to individualized dosing requirements. Stolpe et al. reported that the methods used to measure insulin adherence qualitatively are not appropriate. 5
Key Barriers
Both adherence and persistence are influenced by several factors, including the mode of administration, frequency of administration, complexity of regimen, cost of medications, fear of hypoglycemia, and patient–provider interactions.13,22,23 A recent real-world study (131 participants) evaluated the reasons behind patients’ persistence behaviors among insulin-naive people with T2D who initiated a basal insulin analog. The main reasons for insulin continuation (n = 50), reported in the study were improved physical feeling (52.0%) and improved glycemic control (48.0%). The common reasons for insulin interruption (n = 50) or discontinuation (n = 31), respectively, were weight gain (50.0%, 48.4%) and hypoglycemia (38.0%, 25.8%). 12 It is important for clinicians to understand the patients’ feelings, concerns, and challenges when starting insulin therapy. Furthermore, it is important for clinicians to consider what motivates patients to continue and the reasons that drive patients to interrupt or discontinue insulin therapy.
Impact of Diabetes Pen Technology Advances on Adherence and Persistence
Over the years, insulin pen technology has evolved, and insulin delivery options have progressed. Insulin pen devices were first introduced in 1987 and have helped to partially address many barriers to insulin therapy that are more often associated with insulin vial and syringe delivery, including difficulty of transportation, anxiety and fear about self-injection, more complex training process, and social embarrassment. 4 As described below, in multiple studies, disposable insulin pens have been associated with improved treatment adherence and persistence compared with traditional insulin vial and syringe delivery. 22
Insulin Pens
A systematic review of factors affecting real-world treatment adherence in people with T1D and T2D identified several studies showing significantly better treatment adherence among pen users compared with vial and syringe users, both for people initiating insulin therapy and for those switching from vial and syringe delivery to a pen device.22-24 A retrospective study among 1308 insulin-naive people with T2D reported that persistence was significantly higher (P = 0.011) and longer (P = 0.001) in people who initiated insulin glargine via a disposable pen compared with those who initiated with vial and syringe. 25 A retrospective longitudinal study in 955 people with diabetes in Singapore compared the adherence with premixed insulin formulated in a prefilled pen versus a vial and syringe system. The study reported that prefilled pen users were more persistent with therapy compared with vial and syringe users (odds ratio [OR], 1.4; 95% confidence interval [CI], 1.01-1.86) after adjusting for sociodemographic and clinical covariates. Median time to discontinuation of therapy was comparable (vial and syringe vs. prefilled pen, 409 vs. 532 days; P = 0.076). 26
A pre–post analysis from the United States reported that medication adherence significantly improved after switching from insulin injection (vial and syringe) to the prefilled insulin analog pen device (from 62.0% to 69.0%; P < 0.01) in people with T2D. 27 A retrospective cohort study of a large national claims database in 3842 people reported that insulin glargine therapy initiation with a disposable pen was associated with better treatment persistence compared with insulin glargine therapy initiation with a vial and syringe (P < 0.001) in people with T2D. 28
In a study of the effect of insulin delivery systems in elderly people (≥65 years) with T2D, it was found that people initiating insulin glargine using a pen device were significantly more persistent (58.5% vs. 50.8% at 12 months, respectively; P < 0.0001) and adherent (adjusted MPR ≥0.8; 71.5% vs. 63.1%, respectively; P < 0.0001) than people who initiated treatment using vial and syringe delivery. 29 Other studies in elderly people with T2D have also suggested that pen devices improved insulin therapy adherence and persistence.30,31
Insulin Pens: Economic Impact
There are several real-world studies reporting the association between insulin adherence and healthcare costs in people with diabetes using insulin pens.32,33 These studies suggest that higher rates of medication adherence may present an opportunity to curb healthcare costs in insulin pen users.
A large retrospective claims-based analysis investigated whether higher insulin pen adherence in people (n = 32361) with T2D was associated with lower healthcare costs. The study reported that total healthcare expenditures of people who utilized insulin pens decreased significantly with improvement in adherence; least adherent group, MPR <0.20, total expenditure USD 26310 versus most adherent group, MPR >0.80, total expenditure USD 23839, respectively (P = 0.007). 32 Data from a real-world study in 13428 people with T2D initiating insulin treatment reported that adherent insulin pen use decreased the hospitalization rate in comparison with non-adherent vial users. 33 Another study reported a significant decrease in emergency department visits (OR, 0.4; 95% CI, 0.21-0.92; P < 0.05) after conversion from vial and syringe to pen administration of insulin therapy. This was associated with total mean all-cause treatment cost reduction of USD 1590 per patient per year. 27
Emerging Technologies
With the growth of mobile technologies like smart insulin pens, smartphone mobile applications (apps), handheld tablets, and other devices, new avenues and opportunity for diabetes management and insulin delivery have been created. 34 These technologies enable the potential for remote patient monitoring and delivering clinical advice through a wide range of functions (e.g., text messaging, e-mail, web browsing, and videos). 35 These systems incorporate data and information and facilitate communication to promote positive health outcomes. 36 When applied appropriately, these technologies can improve insulin therapy and the lives and health of people with diabetes.3,37
Telemedicine
Telemedicine involves the use of telecommunications to deliver interactive, consultative, and diagnostic health services. For diabetes, telemedicine interventions can vary from simple reminder systems via text messaging to complex Web interfaces through which patients can upload their glucose and insulin delivery data measured with a home meter, continuous glucose monitor or insulin pump and other pertinent data such as medications, dietary habits, activity level, and medical history. 38 Over the last five years, numerous telemedicine studies or projects based on connected objects and new information and communication technologies have emerged. 39 A meta-analysis conducted by Tchero et al. reported that telemedicine interventions are more effective in managing T2D than the usual care. 40 Telemonitoring is a specific type of telemedicine defined as the use of information technology to monitor patients at a distance.41,42 Various studies in people with T1D and T2D have reported that telemonitoring has resulted in
improvements in control of blood glucose and significant reductions in HbA1c (Telescot et TELESAGE studies),41,43
positive impact on co-morbidities like arterial hypertension, weight, dyslipidemia (Telescot and DIABETe studies), 41
improved patient quality of life (DIABETe study), 42 and
positive impact on appropriation of the disease by patients and/or greater adherence to therapeutic and healthy-dietary measures (The Utah Remote Monitoring Project). 44
Although several studies have reported that telemedicine has shown improvements in blood glucose levels, further investigations are needed on the impact of telemedicine on patient adherence and persistence to insulin therapy.
mHealth
The World Health Organization has recognized a new term “mobile health,” which refers to “the use of mobile applications and texting to help in the management of medical conditions.” 45 FDA quotes, “These technologies can empower consumers to make better-informed decisions about their own health and provide new options for facilitating prevention, early diagnosis of life-threatening diseases, and management of chronic conditions outside of traditional care settings.” 46
Mobile Apps
There has been a tremendous growth in the use of smartphones, even in underserved populations, which makes them a powerful platform to provide tailored healthcare, delivered conveniently to patients through health apps. 47 The key functions of apps include interaction functions such as messages and chatting with physicians; health-monitoring functions such as tracking blood glucose, blood pressure, medication, and weight; lifestyle-monitoring functions like physical activity and dietary habits; and educational functions supplying information. 48 Within diabetes, apps are now commonly able to pair with traditional diabetes technologies, such as continuous glucose monitors and subcutaneous insulin pumps, and mHealth interventional diabetes research is of increasing interest. 49 Several studies have demonstrated the potential adjuvant role of mobile apps in supporting better blood glucose control in individuals living with diabetes.50-53 Hou et al. reported, in a meta-analysis, an average improvement of 0.5% in HbA1c levels for people using mobile apps for T2D management versus controls. 50 A systematic review published in 2017 reported that the various app features including “storage and feedback of blood glucose data,” “assist in diet,” “help practice in physical exercise,” and “assist in control of dosage and adherence to drug therapy” as well as access to health care professionals contributed to improved glycemic control. Another review article similarly highlighted that use of apps in people with diabetes could help improve HbA1c. 54 Small-scale studies of apps and digital platforms targeting glucose control and medication adherence have shown promising results. 55 A few examples of mobile apps are outlined in Table 1.
Few Examples of Recent Mobile Apps.
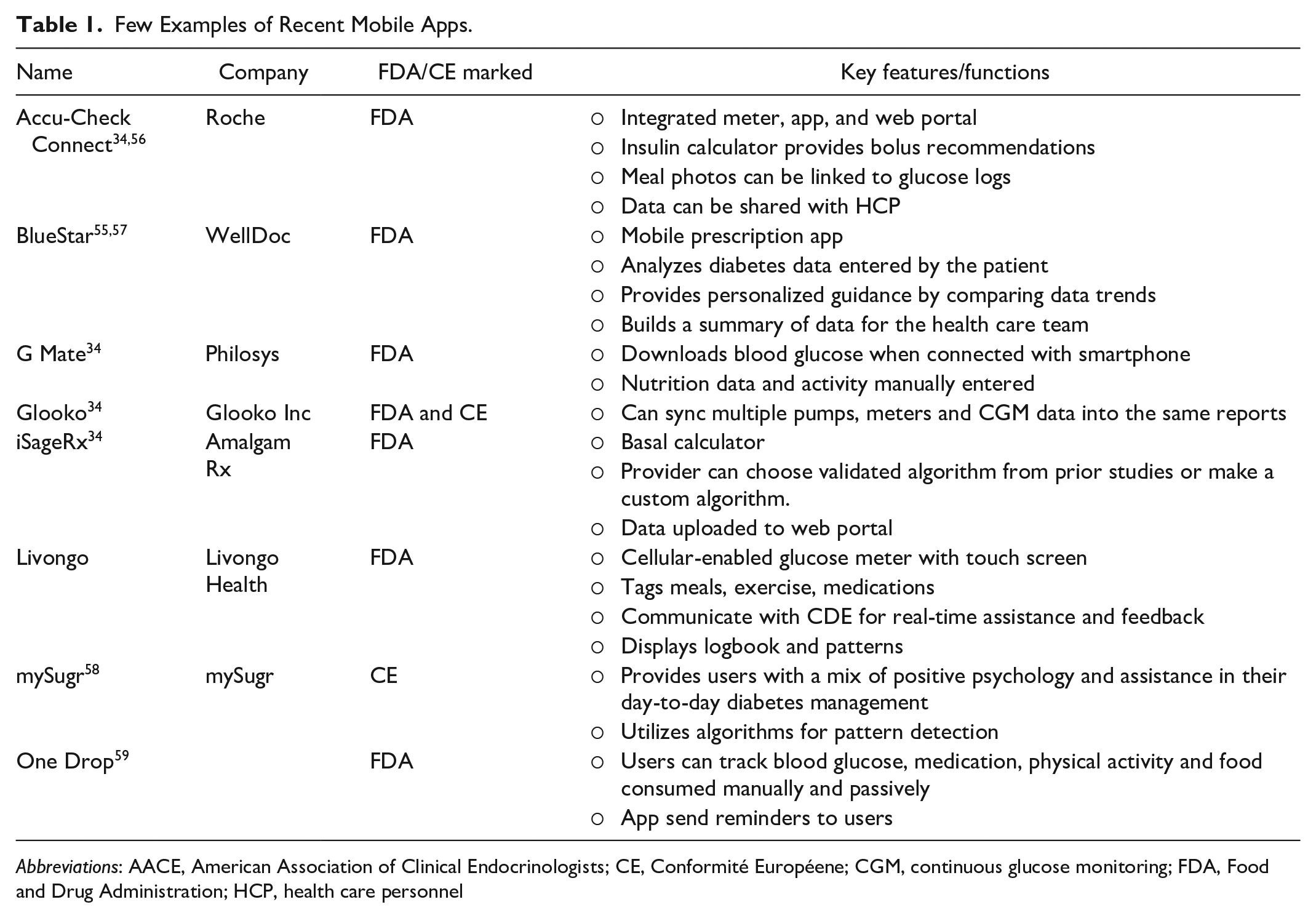
Abbreviations: AACE, American Association of Clinical Endocrinologists; CE, Conformité Européene; CGM, continuous glucose monitoring; FDA, Food and Drug Administration; HCP, health care personnel
Smart Pens
In 2007, Eli Lilly launched a digital pen, HumaPen Memoir, an insulin pen with a memory of the date, time, and amount of the most recent 16 insulin doses.60,61 In recent years, more sophisticated smart insulin pens have become available and others are under development. The first smart insulin pen (InPen; Companion Medical Inc., San Diego, CA) was made available in 2017 in the United States. 37 This device can record the amount and timing of each rapid-acting insulin dose and wirelessly transmit the information via Bluetooth (Bluetooth SIG.Inc, WA, USA) to a dedicated mobile app. This associated app also tracks insulin onboard, suggests dosing calculations like the traditional insulin pump bolus calculator, and prepares reports for health care professionals. 37 With the introduction of smart pens, insulin users and health care professionals now have detailed access to previously limited clinical data on mealtime and correctional insulin administration to assist with individualizing diabetes management. In particular, the exact timing of insulin boluses is all recorded and available for retrospective review, allowing clinicians to address late or missed boluses, which is an important contributing factor to inadequate glycemic control in individuals using multiple daily dose injections. Paired with glucose monitoring data and supported by contextual information obtained from the patient, the data derived from smart pens allow the potential for a step up to the “next level” of integrating glucose and insulin data to further support personalized bolus decisions. Although there are no studies reported on persistence of smart insulin pens, they have significant potential to support adherence to treatment plans, appropriate dosage decisions, and accurate dosing. A recent study by Adolfsson et al. 62 has reported a 43% reduction in missed bolus dose injections and a 1.9 h/d increase in glucose time in range (70-180 mg/dL) in people with T1D using a basal-bolus insulin regimen augmented by continuous glucose monitoring in a real-world setting. Furthermore, in a review article on the future of diabetes technology, Sangave et al. summarized that the “smart pen devices for insulin delivery have the potential for improved adherence, administration and quality of care.” 60
Smart Caps
Smart caps attach to certain currently available disposable rapid-acting insulin pens and have similar features to smart pens, such as monitoring of the timing of injections and the quantity of insulin administered that can help assess adherence. 60 Similar to smart pens, these devices could potentially improve adherence, administration, and quality of care through closer monitoring of pharmacotherapy via sensors and wireless communication. Recent studies utilizing smart caps (with and without continuous glucose monitoring [CGM]) reported that non-adherence including missed and late dosing are associated with poor glycemic control.63,64 Some examples of smart pens and caps apps are outlined in Table 2.
Few Examples of Recent Smart Pens and Smart Caps.
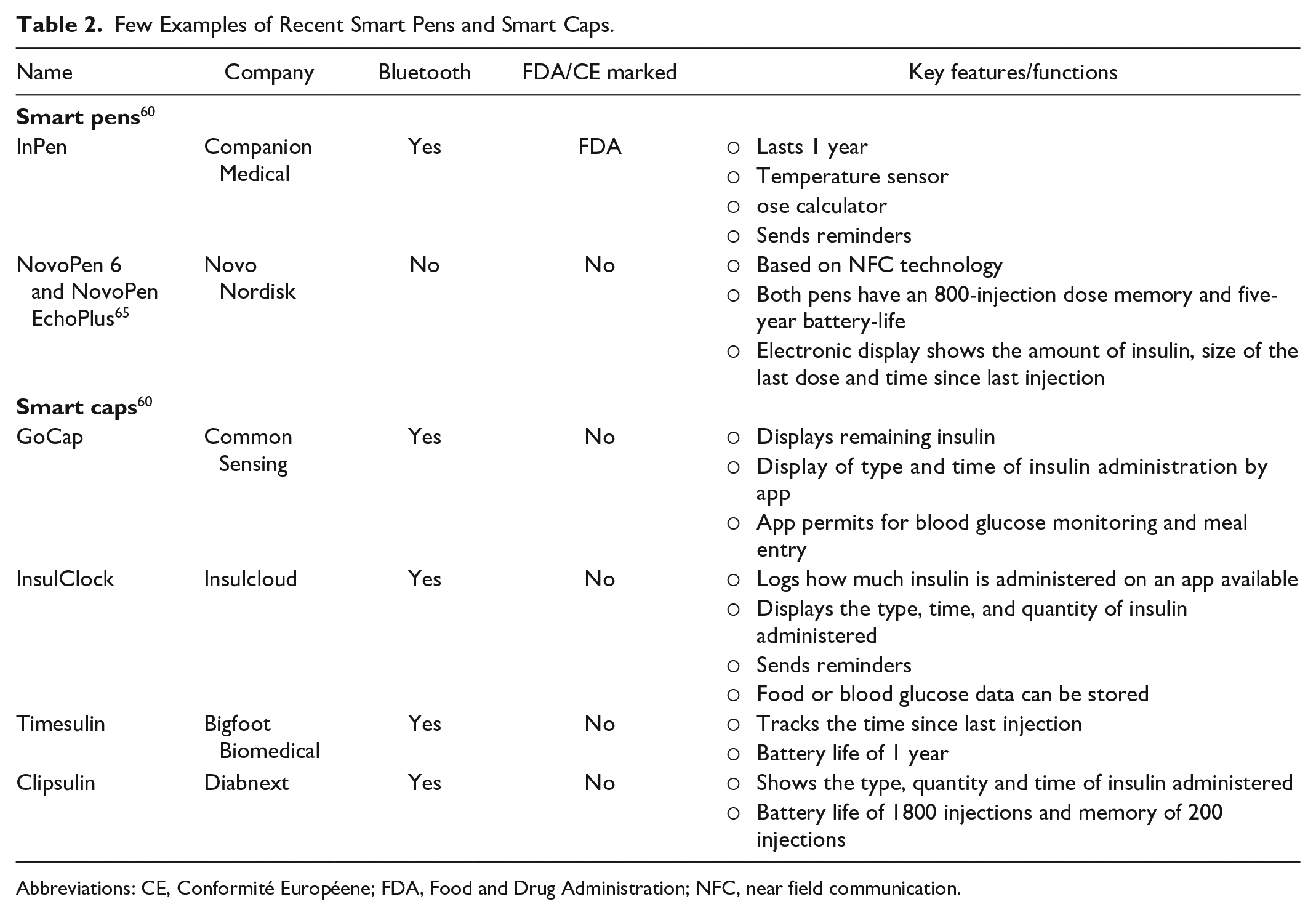
Abbreviations: CE, Conformité Européene; FDA, Food and Drug Administration; NFC, near field communication.
Summary and Future Perspectives
Insulin therapy has its unique adherence and persistence challenges in people with diabetes. Several studies have reported that adherence and persistence with insulin therapy is very low. As technology evolved, insulin pens were introduced, resulting in improved patient adherence and reduced healthcare costs. With the co-emergence of mHealth and the development of smart pens, caps, and increasingly accurate continuous glucose monitors, we are about to enter an era of advanced personalized insulin delivery. Increasing societal adoption of mHealth provides a platform to build a connected diabetes ecosystem. The first wave of this new ecosystem will allow individuals with T1D, who manage their diabetes with MDI, to improve their self-management efficacy and support clinicians who care for them by providing them with much needed integrated data (insulin, self-monitored blood glucose, diet, CGM, and exercise data) that have never been well aligned and available for real-time or retrospective review. Modern CGM data provides the background upon which connected bolus and correctional insulin data can be leveraged to a far greater potential. However, individuals on less intensive insulin regimens, including people with T2D on basal insulin, will likely also benefit from a connected ecosystem, potentially through data-driven feedback that may positively impact behavior change; a foundational aspect of the management of all forms of diabetes. The thoughtful, individualized, and consistent delivery of insulin to correct unanticipated hyperglycemia and to deliver a precise, meal-specific, insulin bolus before meals is the next frontier in prandial insulin delivery. Clinicians and individuals living with diabetes should both have access to the wealth of this data. Shared decision making between clinicians and patients will likely shift to an increasingly important recognition of the context underlying individual or recurrent glucose perturbations. This connected ecosystem has the potential to shine a bright light on the underlying reasons and unlock possible solutions for non-adherence and non-persistence. Addressing missed or late meal-time insulin doses is only the beginning. Future studies will help to inform us of the precise role of the connected ecosystem in diabetes care. As the connected ecosystem grows, inclusion of additional important physiological variables, such as quantification of food intake (through wearable devices including smart watches 66 or modern smartphone camera technologies) 67 and physical activity variables (heart rate, steps counted) will supplement more traditional insulin and glucose data and should allow for improved personalized decision making and increasing automation. 68
Footnotes
Abbreviations
HbA1c, glycated hemoglobin; T1D, Type 1 diabetes; T2D, Type 2 diabetes.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: EE and BL are employees of Eli Lilly and Company, Indiana, USA. NG is an employee of Eli Lilly Services India Private Limited. DS has provided consulting services to Eli Lilly and Company and served on an advisory board for Dexcom.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.