
Abstract

Since the Food and Drug Administration (FDA) approved the integrated pump and sensor system, our clinic and many others have provided patient training for effective use of this technology. This survey investigates all aspects of real-time continuous glucose monitoring (CGM), including frequency of wear, decision to use, calibration, reasons for not wearing, and the need for additional training.
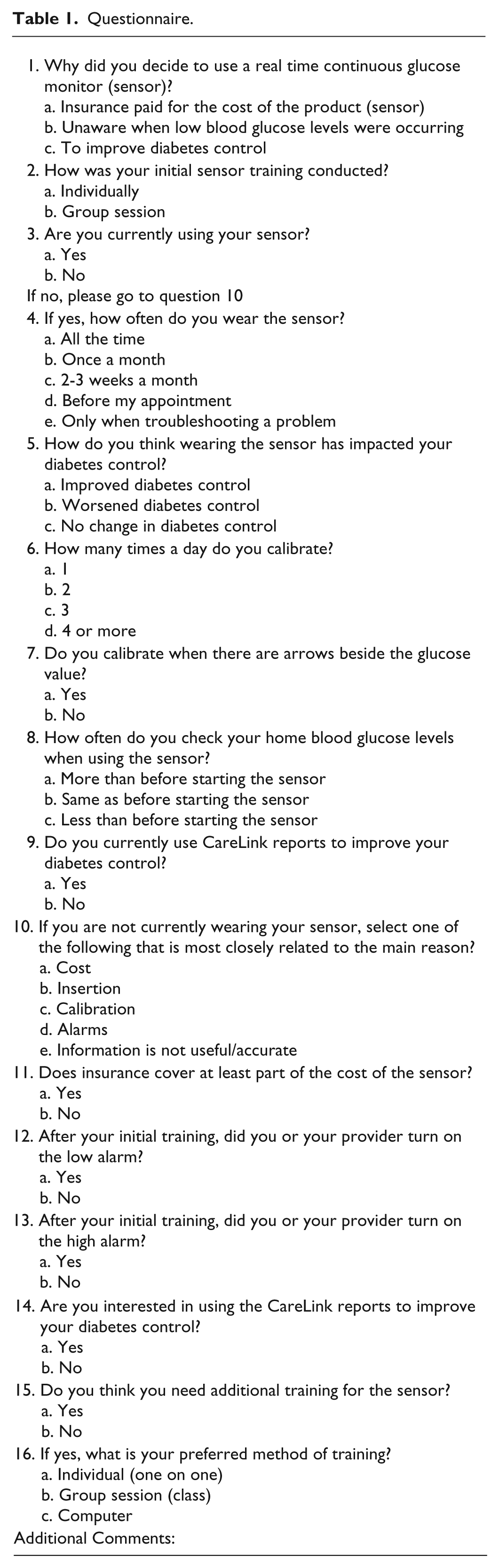
The sample was composed of 39 women and 18 men (ages 19 to 75) with a mean age of 45 years. The majority of patients (82%) had type 1 diabetes. All patients were included if they had used real-time CGM for more than 1 month. The structured questionnaire developed by the lead author, with input from 2 other diabetes educators and providers, comprised a total of 16 multiple choice questions (Table 1). 1
Questionnaire.
The survey revealed 24 patients (42%) were using their real-time CGM, and the majority of these patients wore the sensor all the time (63%). Of patients, 13% reported wearing the sensor once a month. The remainder of patients wore the sensor 2 to 3 weeks a month, before an upcoming appointment or only when troubleshooting a problem. Use of the sensor at least once month was not associated with a significant improvement in A1C (t = −1.09, df = 23, P = .29), but the majority of patients felt using the sensor had improved their diabetes control. A small group felt it had made no difference. Interestingly, the most dramatic improvement was a patient with type 1 diabetes who experienced a 4.5% drop in A1C using the sensor every day for the last year and a half. Within the group wearing the sensor, most patients reported calibrating 3 or more times a day. Most patients in this study did not calibrate when the glucose levels were changing. The majority (75%) of patients in the study reported improved diabetes control as the main reason they decided to use real-time CGM. Hypoglycemia unawareness was the second most common reason patients elected to use the device. The primary reason for not using the sensor was insertion (27%). Other reported barriers to using the sensor included alarms and not useful or inaccurate information. Last, calibration and cost of the sensor were reported equally as a barrier to using the sensor. The manufacturer provides a software package that is available to patients to review their continuous glucose data and identify trends. Our survey revealed that approximately 59% of patients used this advanced feature. Most patients at this office were initially trained individually by a certified diabetes educator or company representative. For those who did want additional training, the preferred method was one-on-one instruction.
The results from this survey were used to offer patients not currently using their real-time CGM additional training with options for group or individual instruction. Other areas identified for ongoing education included a continual emphasis on the difference in sensor readings compared to finger sticks, and not turning on alarms until after the initial training to minimize patient frustrations. 2 Our findings also suggest that improvements in CGM systems to ease insertion and cause less pain could result in more consistent use among patients.
Footnotes
Abbreviations
A1C, glycosylated hemoglobin; CGM, continuous glucose monitoring; FDA, Food and Drug Administration.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Product trainer for Medtronic and Animas.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.