
Abstract
Background:
Severe hypoglycemia remains a major barrier to optimal diabetes management and places a high burden on the US health care system due to the high costs of hypoglycemia-related emergency visits and hospitalizations. Patients with type 1 diabetes (T1DM) who have hypoglycemia unawareness are at a particularly high risk for severe hypoglycemia, the incidence of which may be reduced by the use of real-time continuous glucose monitoring (RT-CGM).
Methods:
We performed a cost calculation using values of key parameters derived from various published sources to examine the potential cost implications of standalone RT-CGM as a tool for reducing rates of severe hypoglycemia requiring hospitalization in adult patients with T1DM who have hypoglycemia unawareness.
Results:
In a hypothetical commercial health plan with 10 million members aged 18-64 years, 9.3% (930 000) are expected to have diagnosed diabetes, with approximately 5% (46 500) having T1DM, of whom approximately 20% (9300) have hypoglycemia unawareness. RT-CGM was estimated to reduce the cost of annual hypoglycemia-related hospitalizations in this select population by $54 369 000, yielding an estimated net cost savings of $8 799 000 to $12 519 000 and a savings of $946 to $1346 per patient.
Conclusion:
This article presents a cost calculation based on available data from multiple sources showing that RT-CGM has the potential to reduce short-term health care costs by averting severe hypoglycemic events requiring hospitalization in a select high-risk population. Prospective, randomized studies that are adequately powered and specifically enroll patients at high risk for severe hypoglycemia are needed to confirm that RT-CGM significantly reduces the incidence of these costly events.
Keywords
Incidence and Health Consequences of Severe Hypoglycemia
Intensive therapy has become the standard of care for treatment of type 1 diabetes (T1DM) based on its proven ability to help patients achieve near-normal glucose levels and significantly reduce the risk of microvascular diabetes complications and cardiovascular disease events. 1 Unfortunately, intensive therapy also increases the risk of severe hypoglycemia,2,3 an iatrogenic acute complication with significant health and socioeconomic consequences. Although it has been over 20 years since the Diabetes Control and Complications Trial (DCCT) showed that intensive therapy tripled the incidence of severe hypoglycemia, 4 and despite the advent of insulin analogues and easier-to-use glucose monitoring devices, most clinicians still believe that hypoglycemia represents the biggest barrier to intensive glucose management. 5 In adults, severe hypoglycemia is defined as hypoglycemia that requires assistance from another person to actively administer carbohydrates, glucagon, or take other corrective actions. 6 A review of the literature indicates that most studies of adults with T1DM have reported annual incidence rates of approximately 1 episode of severe hypoglycemia per patient.7-12
Severe hypoglycemia causes poor health outcomes in people with T1DM, is a major barrier to optimal diabetes management, and often results in acute complications requiring emergency medical care. Potential long-term serious sequelae of severe hypoglycemia include increased risk of dementia, fracture-related falls, and cardiovascular events.13-16 In addition, severe hypoglycemia has been associated with an increased risk of mortality in patients with T1DM,17,18 although it is not yet clear whether severe hypoglycemia is a direct cause of death or a marker for other risk factors associated with elevated mortality. Fear of severe hypoglycemia, which may be triggered by a single episode, can cause patients, parents, and providers to utilize less aggressive diabetes management and prevent patients from achieving target glycemic levels. 19 Approximately 19% of severe hypoglycemic episodes result in acute complications, including loss of consciousness, transport to emergency room, hospitalization, or fracture or trauma. 20
Hypoglycemia unawareness, the diminished ability to perceive the acute autonomic warning symptoms of hypoglycemia, 21 affects approximately 20% of adults with T1DM. 22 Because awareness of the onset of hypoglycemia is fundamental to effective self-management to prevent progression to severe hypoglycemia, 21 the presence of hypoglycemia unawareness greatly increases the risk of severe hyperglycemia in adults with insulin-treated diabetes.22-24
High Medical Costs of Severe Hypoglycemia
Severe hypoglycemia places a high burden on the US health care system due to the high costs of hypoglycemia-related emergency department (ED) visits and hospitalizations. Each year in the United States, hypoglycemia is responsible for 100 000 ED visits, approximately one-third of which result in hospitalization. 25 Over a 5-year period, ED visits for severe hypoglycemia cost the US health care system an estimated $600 million ($120 million per year), 25 with an average cost of $1387 per visit. 26
Approximately 30% of all severe hypoglycemic events in patients with T1DM necessitate ambulance/emergency team care, 10% emergency room/hospital attendance (<24 hours), and 5% hospital admission >24 hours. 27 Among 43 patients with T1DM admitted to the emergency room for hypoglycemia on 59 occasions, 47% were admitted to the hospital, of whom 64% had no coexistent reason other than hypoglycemia for hospitalization. 28 Among Medicare beneficiaries, the number of hospital admissions due to hypoglycemia admissions now exceeds that for hospital admissions due to hyperglycemia. 29 These admissions come at a high cost. An analysis of claims data for a large cohort of privately insured, working-age adults with type 2 diabetes (T2DM) estimated the average cost of a hospitalization for hypoglycemia at $17 654 in 2008 USD, which was significantly higher than the average cost of other diabetes-related inpatient admissions. 26 Based on this figure, Vigersky estimated the total annual cost of hospitalizations for hypoglycemia for the US T1DM population to be between $1.8 billion and $5.9 billion. 19
Impact of Real-Time Continuous Glucose Monitoring on Severe Hypoglycemia
Real-time continuous glucose monitoring (RT-CGM) offers opportunities to improve hyperglycemia and hypoglycemia by providing patients with real-time actionable information about their current blood glucose levels, the rate and direction of blood glucose changes, and alerts/alarms when blood glucose values exceed or fall below specified thresholds. 30 Meta-analyses have shown that RT-CGM significantly lowers HbA1c without increasing the risk of hypoglycemia in patients with T1DM, and is most effective in reducing HbA1c when patients use RT-CGM at least 70% of the time.31-33 Studies have not examined whether regular RT-CGM use is associated with a greater reduction in the frequency of hypoglycemic events, but it stands to reason that patients must be using the device to benefit from alerts/alarms indicating when blood glucose levels fall below a threshold. There is not yet conclusive evidence that RT-CGM reduces the number of hypoglycemic events, including severe episodes, but data support the role of RT-CGM in reducing moderate hypoglycemia as well as the time spent in hypoglycemic range.34,35 Although clinical trials of RT-CGM have largely failed to demonstrate a significant reduction in hypoglycemic events,31-33,36 these studies were not adequately designed or powered to detect a statistically significant decrease in this endpoint that occurs relatively infrequently in an unselected population. 37 Two studies that had a reduction in hypoglycemia as the primary outcome showed a significant reduction in the rate of mild hypoglycemia, but rates of severe hypoglycemia were very low.34,38 Although the Juvenile Diabetes Research Foundation (JDRF) randomized controlled trial 35 was not adequately powered to detect a statistically significant reduction in the frequency of severe hypoglycemia, in a 6-month usual care extension study, T1DM patients, including both adults and children, assigned to the control group in the original trial who were newly initiated on RT-CGM experienced a 46% reduction in the incidence of severe hypoglycemia. 39
Several recent studies conducted in patients with T1DM and hypoglycemia unawareness suggest that RT-CGM may significantly reduce the rate of severe hypoglycemia in this high-risk population. In a small retrospective study, the mean rate of severe hypoglycemia declined from 8.1 to 1.2 episodes/year (P = .005) after initiation of RT-CGM in patients who had problematic hypoglycemia that were primarily using insulin pumps. 40 A 6-month randomized controlled trial found that a sensor-augmented insulin pump with low-glucose suspension significantly reduced the rate of severe hypoglycemic events compared with standard insulin pump therapy. 41 Another 6-month prospective clinical trial reported that the average annualized rate of severe hypoglycemia fell from 11.3 to 0.8 events in patients with T1DM who received RT-CGM. 42 The HypoDE (Hypoglycemia in Deutschland) is the first study that will examine the impact of RT-CGM in reducing the frequency of severe hypoglycemia in T1DM patients who have high baseline rates of severe hypoglycemia and are being treated with multiple daily doses of insulin. 37 This study should provide some important information about the advantages of standalone RT-CGM in patients with T1DM at increased risk for experiencing severe hypoglycemia.
Cost-Effectiveness and Reimbursement of RT-CGM
Mounting evidence of the benefits of RT-CGM has resulted in improved reimbursement of this technology by US commercial health plans. 43 There are dedicated current procedure terminology billing codes for educating/training patients about CGM and interpreting CGM data, 44 although these codes do not distinguish between real-time and retrospective CGM. Commercial health plans almost universally provide coverage for RT-CGM in subsets of patients with T1DM, 43 and are expanding to cover similar types of patients with insulin-treated T2DM. 45 Despite these positive developments, barriers continue to hinder greater access to RT-CGM. Medicare does not currently cover RT-CGM, which it considers to be a “precautionary” rather than a “medically critical” device. 46 The different structures of health plans affect patient copays and deductibles, some of which may place a high burden on patients for out-of-pocket costs for RT-CGM. RT-CGM is usually considered durable medical equipment and is subject to the same deductibles and copays as other types of durable medical equipment. However, some health plans provide continuous glucose monitoring sensors through the patient’s pharmacy benefit, which is typically far less costly to the patient.
Additional evidence supporting the economic value of RT-CGM may improve payer coverage and reimbursement. To date, 6 studies have examined the cost-effectiveness of RT-CGM in patients with T1DM (see Table 1).47-52 The results of these studies have been wide ranging, which may be due both to advances in RT-CGM technology over time and differences in assumptions that form the basis of the models, and may not be compelling to US payers for several reasons. First, most studies estimated costs over a long time horizon even though the average retention of commercial health plan members is typically a few years, and US payers traditionally focus on 1- to 3-year time frames corresponding to their budget and contracting cycles. 53 Second, almost all economic models of RT-CGM are complex Markov models, which payers may not find credible because of the use of implausible or unsubstantiated assumptions or lack of transparency. 54 Third, all studies reported the economic value of RT-CGM in terms of cost per quality-adjusted life year gained, which may have limited relevance, meaningfulness, validity, and reliability to US payers. 55 Fourth, models using a societal perspective (ie, which include both direct and indirect costs) may not be relevant to payers who are mainly concerned with direct costs. Finally, many of the studies focused on devices that combined an insulin pump and RT-CGM (eg, sensor-augmented insulin pump), which makes it difficult to discern the relative value of RT-CGM alone.
Cost-Effectiveness Studies of RT-CGM in Patients With Type 1 Diabetes.
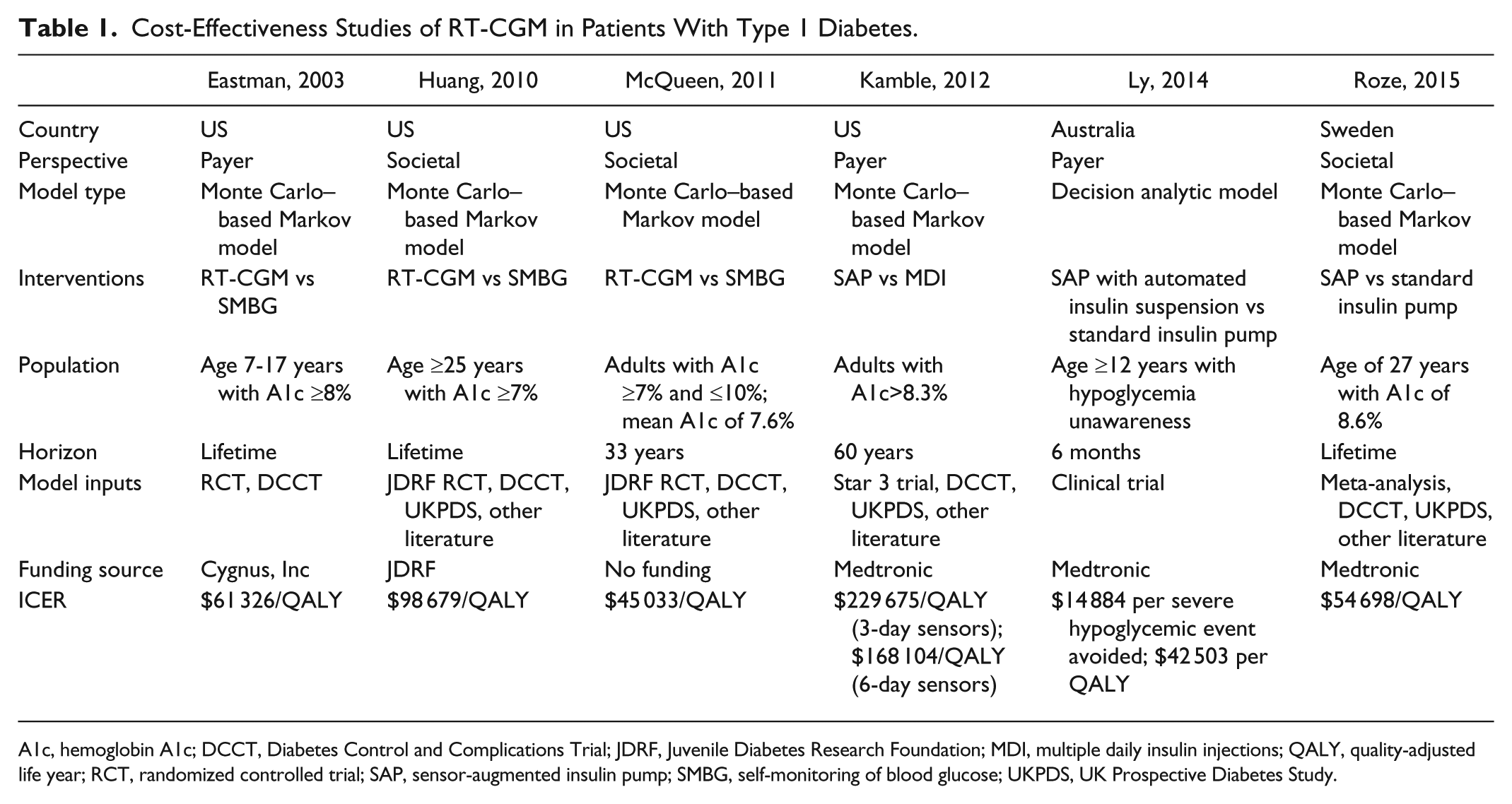
A1c, hemoglobin A1c; DCCT, Diabetes Control and Complications Trial; JDRF, Juvenile Diabetes Research Foundation; MDI, multiple daily insulin injections; QALY, quality-adjusted life year; RCT, randomized controlled trial; SAP, sensor-augmented insulin pump; SMBG, self-monitoring of blood glucose; UKPDS, UK Prospective Diabetes Study.
Potential Cost Implications of Reducing Severe Hypoglycemia in Hypoglycemia Unaware Adults With T1DM With RT-CGM
Assumptions and Estimates
Given the limitations of existing cost-effectiveness models for demonstrating the economic value of RT-CGM to US payers, it may be worthwhile to explore the potential cost implications of standalone RT-CGM as a tool for reducing rates of severe hypoglycemia requiring hospitalization in a subset of T1DM patients at high risk for these costly events. Although there are insufficient data to develop a robust economic model addressing this question, a simple cost calculation using values of key parameters derived from various published sources may provide a rough estimate for the direct cost benefits of providing RT-CGM to T1DM adults at high risk for severe hypoglycemia.
Table 2 summarizes the parameters that will serve as the basis of this cost calculation. We have defined individuals at high risk for severe hypoglycemia as those with hypoglycemia unawareness. In a large cohort study, approximately 20% of adults with T1DM had hypoglycemia unawareness, 22 which was identified by asking individuals to rate on a 7-point Likert-type scale (1 = always aware, 7 = never aware) the extent of their awareness of when hypoglycemia was commencing, with a value of 4 or higher indicating impaired awareness of hypoglycemia. Adults with T1DM and hypoglycemia unawareness have a 6-times greater risk of severe hypoglycemia than those without hypoglycemia unawareness.22,23
Estimates for Cost Calculation.
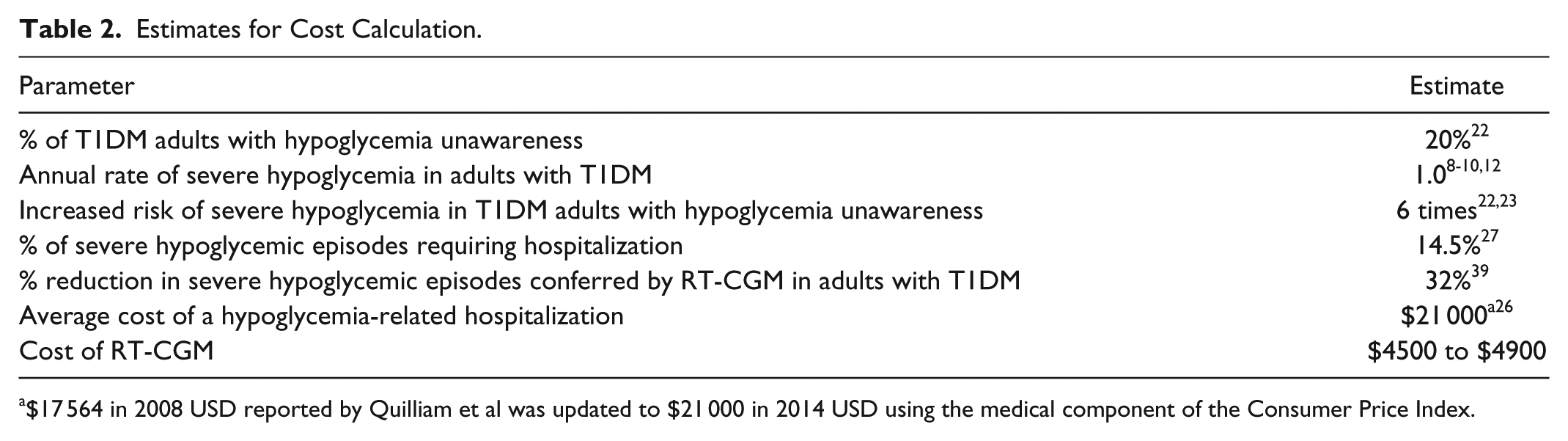
$17 564 in 2008 USD reported by Quilliam et al was updated to $21 000 in 2014 USD using the medical component of the Consumer Price Index.
To estimate the annual rate of severe hypoglycemic events in patients with T1DM and hypoglycemia awareness, we first examined studies that estimated the annual rate of severe hypoglycemia in the general population of adults with T1DM (which includes individuals with and without hypoglycemia unawareness) to determine the average incidence of severe hypoglycemia among all adults with T1DM. Although these studies reported varying rates of severe hypoglycemia, defined as episodes of hypoglycemia requiring assistance from a third party, in the general T1DM population, the majority reported rates close to 1 episode per patient-year (Table 3).7-12,56 A lower incidence rate (0.49 events per patient-year) was reported in a recent retrospective study of 206 T1DM patients in Italy. 56 The authors surmised that the comparatively lower incidence of severe hypoglycemia found in their study may have been due to the fact that study patients were receiving optimal diabetes care, including treatment by diabetes specialists and almost universal treatment with insulin analogues. In contrast, a global study conducted in 24 countries involving 8022 individuals with T1DM reported considerably higher annual rates of severe hypoglycemia (2.1 and 4.9 events per patient-year, respectively, when assessed retrospectively and prospectively). 57 Based on the totality of evidence, we assumed the annual rate of severe hypoglycemia in the general adult T1DM population to be 1 episode per patient-year, which we believe is a conservative estimate. Given that adults with T1DM and hypoglycemia unawareness have a 6-fold greater risk of severe hypoglycemia than those without hypoglycemia unawareness,22,23 we estimated the incidence of severe hypoglycemia in adults with T1DM and hypoglycemia unawareness at 6 episodes per patient-year (ie, the rate of severe hypoglycemia in the general T1DM adult population [1 episode per patient-year] multiplied by 6).
Annual Incidence of Severe Hypoglycemia in Adults With T1DM.
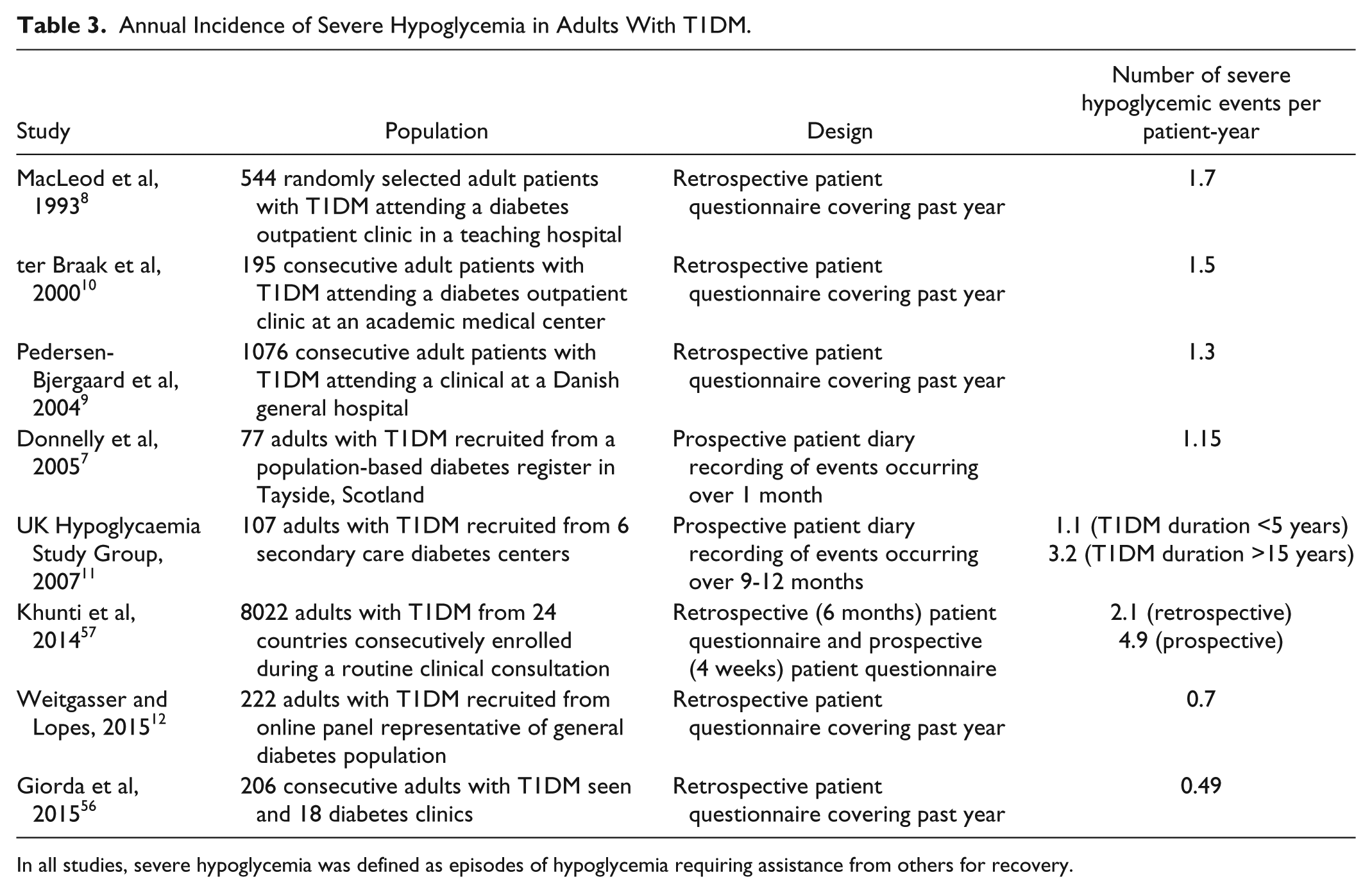
In all studies, severe hypoglycemia was defined as episodes of hypoglycemia requiring assistance from others for recovery.
Estimates for the percentage reduction in the frequency of severe hypoglycemic events conferred by RT-CGM in adults with T1DM were derived from the 6-month JDRF extension study, in which adults (aged ≥25 years) who were formerly assigned to the JDRF randomized trial control group experienced a 32% reduction in the incidence of severe hypoglycemia after initiating RT-CGM. 39 Given that several small studies have reported much larger reductions (>80%) in the incidence of severe hypoglycemia following initiation of RT-CGM in patients with hypoglycemia unawareness,40-42 estimates derived from the JDRF extension study (which did not select patients at high risk for severe hypoglycemia) may be considered conservative for a population with hypoglycemia unawareness.
In 15 open-label, randomized, treat-to-target clinical trials with durations of 26 or 52 months involving 8000 patients, all episodes of severe hypoglycemia requiring emergency medical assistance (ambulance services or hospital/ER visit) were captured. 27 Among patients with T1DM, 420 severe hypoglycemic events occurred, of which 14.5% required hospital/ER visits (< or ≥24 hours). The average cost of a hypoglycemia-related hospitalization ($17 564 in 2008 USD [updated to $21 000 in 2014 USD using the medical component of the Consumer Price Index]) was derived from an analysis of administrative claims data for a large cohort of privately insured, working-age US adults with T2DM. 26 The annual cost of RT-CGM (as a standalone device) was estimated to range from $4500 to $4900, depending on the frequency and duration of sensor use. This range is consistent with the estimated annual cost of 2 commercial types of RT-CGM devices used in the JDRF randomized clinical trial. 48
Cost Calculation
Table 4 applies the assumptions and estimates described above to a hypothetical US commercial health plan with 10 million members aged 18-64 years. The prevalence of diagnosed diabetes among US adults aged ≥18 years is 9.3%. 58 Thus, in this hypothetical health plan, 9.3% (930 000) of the 10 million adult members would be expected to have diagnosed diabetes, with approximately 5% (46 500) having T1DM. 59 All enrollees with T1DM are assumed to be receiving insulin therapy.
Cost Calculation Inputs and Results for a Commercial Health Plan.
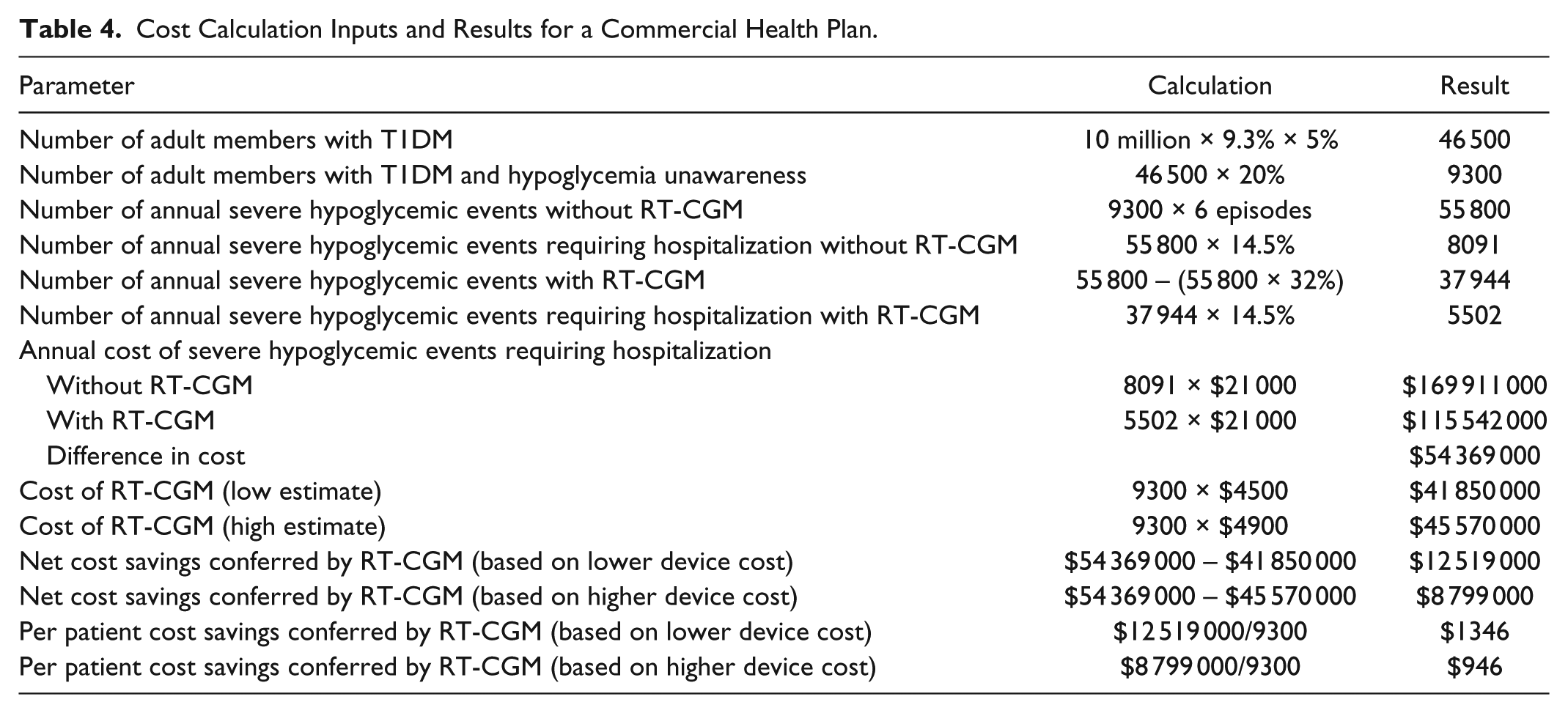
The target population for treatment with RT-CGM is the approximately 9300 adults with T1DM and hypoglycemia unawareness. Without the use of RT-CGM, these patients are estimated to experience 55 800 episodes of severe hypoglycemia each year, of which 8091 require hospitalization at a total cost of $169 911 000. With RT-CGM, these same patients are expected to experience 37 944 episodes of severe hypoglycemia each year, of which 5502 require hospitalization at a total cost of $115 542 000. Thus, RT-CGM is estimated to reduce the cost of hypoglycemia-related hospitalizations in this select population by $54 369 000. Subtracting the cost of providing RT-CGM to this population ($41 850 000 to $45 570 000) yields an estimated net cost savings of $8 799 000 to $12 519 000 and a savings of $946 to $1346 per patient.
Discussion
Coverage and reimbursement of RT-CGM has expanded following improvements in the accuracy and usability of these devices and the growing number of high-quality clinical trials that have demonstrated the superiority of RT-CGM versus self-monitoring of blood glucose in reducing hypoglycemia and HbA1c in children and adults with T1DM. To further broaden access to RT-CGM, the economic value of the technology must be more firmly established in terms that are relevant and compelling to US payers. An important gap in the clinical literature is the extent to which standalone RT-CGM improves the rate, severity, and duration of hypoglycemia. In particular, it will be important to demonstrate the impact of RT-CGM on severe hypoglycemia, which is associated with significant morbidity, mortality, and health care costs. To accomplish this, studies like HypoDE, 37 which are specifically designed and powered to address these questions, are needed.
The cost calculation presented in this article applied arguably conservative estimates for the incidence of severe hypoglycemia and potential impact of RT-CGM on the frequency of severe hypoglycemic episodes in patients with T1DM who are at particularly high risk for these events. Results indicated that providing RT-CGM to patients with T1DM and hypoglycemia unawareness could save a US commercial health plan with 10 million members aged 18-64 years between $8.8 and $12.5 million each year by averting hospitalizations for severe hypoglycemia.
Of course, patients with hypoglycemia unawareness constitute a minority of T1DM patients for whom RT-CGM is indicated and potentially beneficial. Many patients with T1DM who have difficulty achieving glycemic targets, but who are not at high risk of experiencing severe hypoglycemia, may benefit from the glucose lowering effects of RT-CGM. Quantifying the economic benefits of the glucose-lowering effects of RT-CGM, as measured by HbA1c, necessitates a long-term view as the most serious health consequences of prolonged hyperglycemia (eg, renal failure, lower limb amputation) typically do not manifest until later in the disease process. An economic model that takes into account both the short- and long-term health benefits of RT-CGM may prove to be particularly compelling as the potentially large short-term cost savings arising from the reduction of severe hypoglycemia in high-risk patients coupled with the decreased risk of long-term diabetes complications may offset the costs of providing RT-CGM to a broader population of patients with T1DM over their lifetimes. In addition, although RT-CGM effects on quality of life are more difficult to quantify in short-term budget impact analyses, quality-of-life metrics are an important component in many long-term cost-effectiveness analyses.
Use of RT-CGM is expanding to treat insulin-treated patients with T2DM who meet the same indications as patients with T1DM (eg, glucose levels above target, recurrent hypoglycemia). We did not include patients with insulin-treated T2DM in the cost calculation because there are not yet sufficient data to estimate key parameters for this population, such as the reduction in the frequency of severe hypoglycemia conferred by RT-CGM. As these data are reported, we will expand the model to include this population. A number of studies have reported a lower incidence of self-reported severe hypoglycemia in patients with insulin-treated T2DM than is typically seen in patients with T1DM,7,8,24,60 with duration of diabetes and insulin therapy and presence of hypoglycemia unawareness identified as major risk factors. However, a recent study found that patients with T2DM receiving multiple daily injections of insulin or basal-oral therapy had much higher rates of emergency room/hospital use due to hypoglycemia than patients with T1DM. 27 The 14.5% rate of hospital/ER visits for patients with T1DM cited in the recent study by Heller et al includes both hospital visits for <24 hours and those lasting ≥24 hours. Heller et al noted that the 18.6% of T1DM and T2DM patients with severe hypoglycemia who sought hospital treatment in their study was lower than the 28% of insulin-treated patients with severe hypoglycemia who required hospitalization in an earlier study by Leese et al. 61 The authors surmised that the higher rate of severe hypoglycemia-related hospitalizations reported in the earlier study may have been due to a more severely affected population, but also acknowledged that rates of severe hypoglycemia reported in clinical trials, which have excluded patients at high risk for severe hypoglycemia, including those with hypoglycemia unawareness, may underestimate the frequency of these events in real-world settings. In support of the contention that the true incidence of severe hypoglycemia has been underestimated in both clinical trials and observational studies, the Hypoglycaemia Assessment Tool study recently reported considerably higher rates of the incidence of severe hypoglycemia in a global T1DM patient population than have been previously reported. 57 Therefore, it seems reasonable to assume that the proportion of severe hypoglycemia events requiring hospitalization in adults with T1DM lies somewhere between 15% and 28%.
We acknowledge the limitations of the cost calculations presented herein. First, the assumptions and parameters used in the calculations were derived from multiple studies that had variable strengths and weaknesses. To maximize the external validity of our findings, we selected large, population-based studies as sources of estimates for key parameters, such as the incidence of hypoglycemia awareness and severe hypoglycemia among adults with T1DM and the cost of hospitalization for severe hypoglycemia. Despite these efforts, it is possible that certain assumptions and estimates that formed the basis of our cost calculations were not broadly representative of the target population. Second, this article focuses on the potential cost benefits of providing RT-CGM to a highly select subgroup of patients with T1DM. A longer term perspective may be needed to demonstrate the cost-effectiveness of RT-CGM for the broader population of patients with T1DM who are at normal risk for severe hypoglycemia but have a high risk for developing long-term complications of diabetes due to chronic hyperglycemia.
Conclusion
In conclusion, although the long-term health benefits of good glycemic control are clearly important and should justify the value of RT-CGM, it has been challenging to demonstrate that reducing the risk of microvascular and macrovascular diabetes complications over patients’ lifetime is a cost-effective strategy for commercial payers. In this article, we present a cost calculation based on available data from multiple sources showing that RT-CGM has the potential to reduce short-term health care costs by averting severe hypoglycemic events requiring hospitalization. Prospective, randomized studies that are adequately powered and specifically enroll patients at high risk for severe hypoglycemia are needed to confirm that RT-CGM significantly reduces the incidence of these costly events.
Footnotes
Abbreviations
DCCT, Diabetes Control and Complications Trial; ED, emergency department; JDRF, Juvenile Diabetes Research Foundation; RT-CGM, teal-time continuous glucose monitoring; T1DM, type 1 diabetes mellitus; T2DM, type 2 diabetes mellitus.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: AB is a paid consultant to Dexcom, Inc. CG is an employee of Dexcom, Inc.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by Dexcom, Inc.