
Abstract
Introduction
The carotid artery's name is derived from the Greek word “karos,” which means “to stupefy” or “to fall into deep sleep” (1). Avicenna knew that pressure on the neck could cause someone to faint (2). Heinrich Ewald Hering is credited with first describing the carotid sinus reflex in 1924 (3, 4). Thus, it has long been known that pressure to some regions of the neck may elicit a neural reflex that can cause profound hypotension, cardiac standstill, and collapse—but can it cause death? Only ventricular arrhythmias and cardioinhibition (CI) can suddenly stop the heart from pumping. On the other hand, instantaneous neurogenic cardiac arrest (INCA) is a controversial entity discussed in forensic literature. The knee of Officer Chauvin on the neck of George Floyd for 9 ½ minutes brings this consideration to the fore (5).
Methodology
We performed an exhaustive, deep, iterative literature search of the topic and collateral topics using multiple terms and multiple search engines. We reviewed the citations of the articles and articles that cited them and then repeated the process. We had to translate some articles and enlist the help of librarians to pull articles from physical archives. We are unable to present our full findings here.
Pressure on the Neck
The internal carotid artery undergoes substantial growth and reorientation during the developmental years, and the carotid sinus (carotid bulb) appears to develop in late adolescence (6). It generally develops into a bulbous concentric dilatation of the root of each internal carotid artery (Figure 1), beginning just below the bifurcation of the common carotid (7). However, there can be variations from that location, with 17% in the common carotid only, 7% in the common carotid, internal carotid, and external carotid, and 1% in the common carotid and external carotid (8). With catheters inserted and clipped in place in the distal carotid stumps for embalming purposes, the carotid sinuses may be removed with the neck organ block during autopsy dissection (9–12).
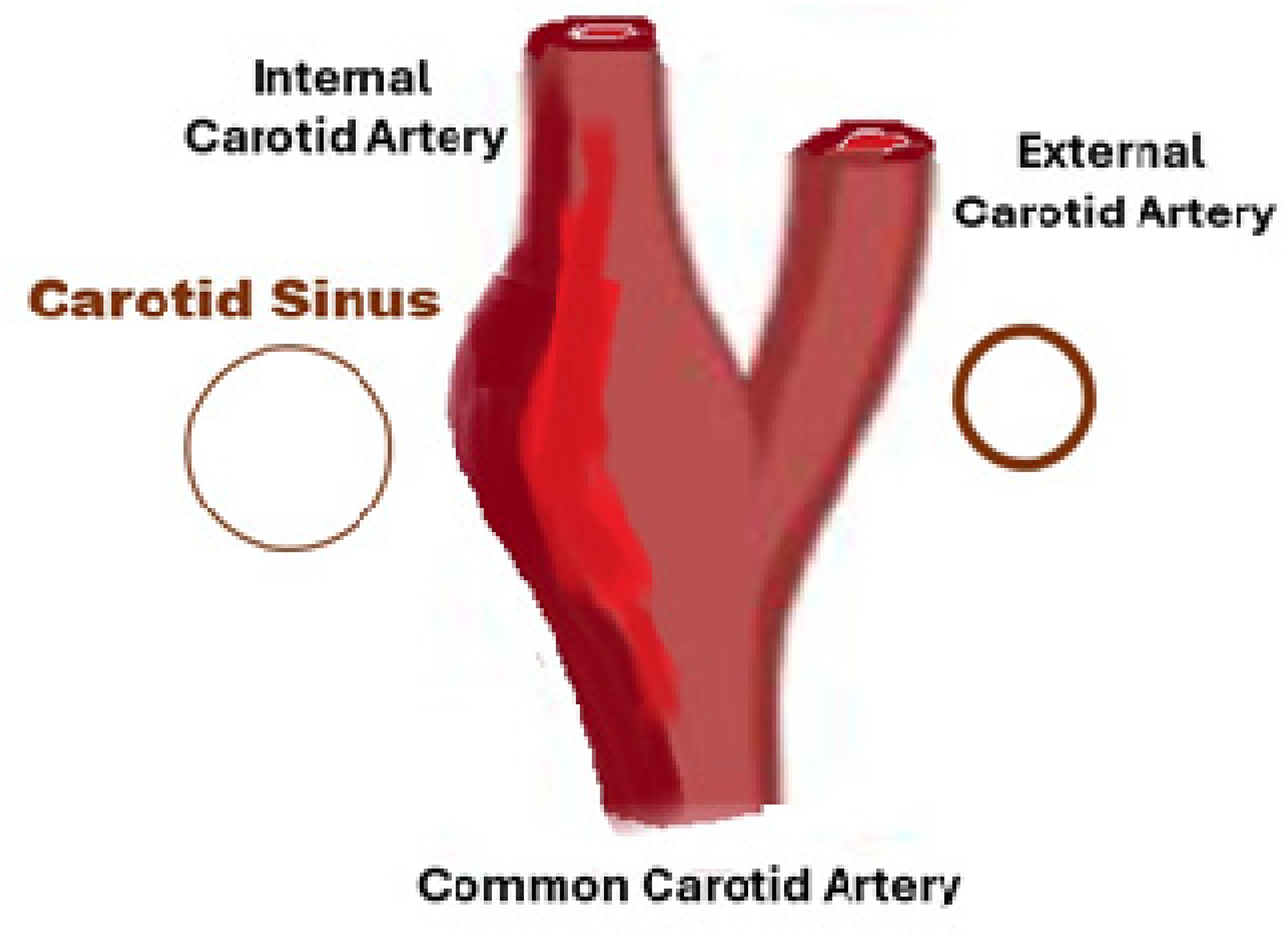
Cartoon of the carotid sinus.
The right and left carotid bifurcations are in the upper mid-lateral neck, below the angle of the jaw, at the superior edge of the thyroid cartilage, deep in the carotid triangle, bounded by the sternocleidomastoid, omohyoid, and digastric muscles (13) (see Figures 2–4). The sternocleidomastoid and deep neck muscles protect the carotid sinus, especially the suprahyoid muscles. When the head is turned to the opposite side, the sternocleidomastoid and jugular vein will slide anteriorly and over the carotid artery (14).

Dissection of the neck, exposing the carotid bifurcation and carotid sinus, superimposed upon the neck of the same individual [courtesy of Matthew B. Brown, DC OCME].

Magnetic resonance imaging reconstruction shows the carotid arteries’ relation to the jaw and cervical vertebral column.
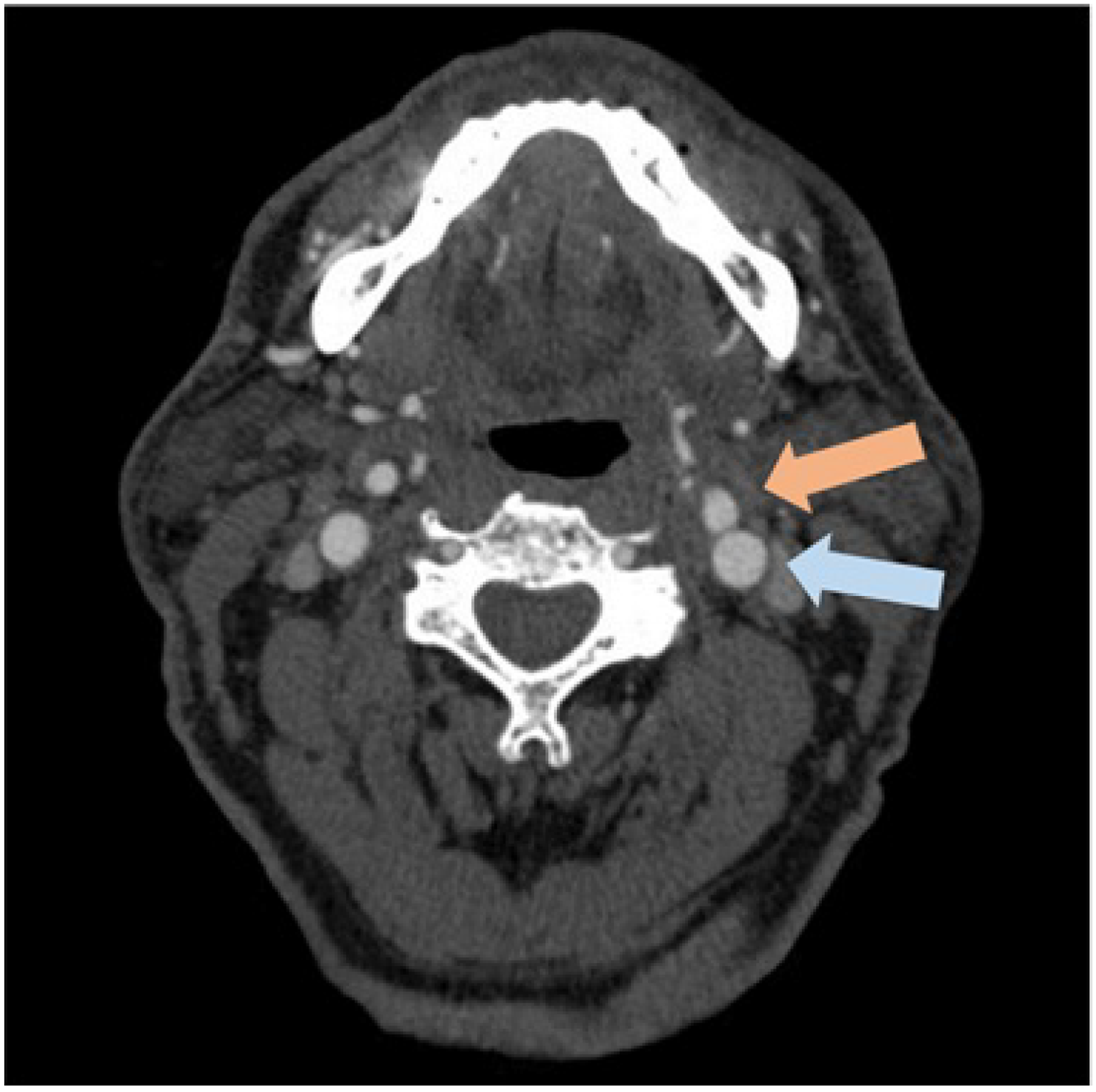
Magnetic resonance imaging transverse section through the neck with contrast dye showing the internal (pale red arrow) and external (pale blue arrow) carotid arteries and their relation to other structures.
Significant vertical variations of the carotid sinus exist in this anatomical location. In one study, the carotid sinus averaged 3.2 cm below the mandibular angle (gonion) on the left and 3.6 cm below on the right, but with a range of 0 to 7 cm, corresponding to a C2-C3 vertebral level (ranging down to the C7 vertebra) (15). In another study, the carotid bifurcation varied widely concerning its location relative to the mandibular angle, relative to the hyoid bone, differing between the left and right sides, and differing between males and females (16). The authors stated that the carotid bifurcation is usually situated at the level of the C4 vertebra or the upper border of the thyroid cartilage but may be as high as the level of the hyoid bone and as low as the T3 vertebra.
The carotid bifurcation may be pressed against the spine by lateral forces, and the larynx will spread and press against the carotid bifurcation from frontal forces (9). It should also be noted that pressure over the carotid bifurcation will deform or stretch and stimulate the carotid sinus baroreceptors (mimicking hypertension), increasing parasympathetic activity. In contrast, pressure below the carotid bifurcation will decrease pressure transmitted to the carotid sinus baroreceptors mimicking hypotension, resulting in increased sympathetic activity.
Studies of pressure on the neck causing cardioinhibition are mixed. Rossen et al did not observe cardiac arrest in more than 100 healthy volunteers subjected to nonlethal strangulation, although when the neck compression lasted for more than 30 s, bradycardia was observed (17). Joshi et al, studying the use of jugular compression (“Q”) collars to reduce brain injury caused by head impacts in sports, found in 16 subjects that both the veins and the arteries were compressed and influenced sympathetic nervous activity, although the effect was limited in the upright position (18). Mitchell et al studied vascular neck restraint by police, specifically the physiological effects of external pressure on carotid arteries on 24 subjects. They concluded that the loss of consciousness was from cerebral hypoxia due to diminished blood flow without the significant contribution of the carotid sinus baroreceptor reflex because they found no significant decrement in cardiac output (19).
In the case of George Floyd, Chauvin's knee was on the mid-lateral left neck in the region of the carotid triangle. No hemorrhage of the soft tissues of the neck were found at autopsy to reveal the point of pressure. If the pressure was solely on the posterior neck, then the carotid sinus pressure may have been spared. We believe this is unlikely and that the carotid sinus would likely have been stimulated.
The Carotid Sinus Reflex
The carotid sinus baroreceptor reflex is a neural-controlled homeostatic negative-feedback reflex regulatory mechanism to maintain constant blood pressure (20–23). The autonomic nervous system unconsciously regulates blood pressure acutely through control of blood flow and, in the longer term, through control of blood volume (24, 25). It is essential in preventing orthostatic hypotension. The sympathetic nervous system appears to have evolved after the parasympathetic system and is probably more critical to postural orthostasis (26). Denervation of baroreceptors causes instability of the systemic blood pressure, causing the variability to increase approximately two-and-a-half-fold (21). However, the notion of a closed loop is oversimplified, as it does not account for central system influence with some input from higher nervous centers, and it has been seen by some more as an open loop system to stabilize and control variation (26, 27). The full physiology of the baroreceptor reflex is complex and includes respiratory and endocrine components (21).
Mechanosensors (spray-type nerve endings) are particularly abundant in the carotid sinus and act as high-pressure baroreceptors that respond to the vascular wall being stretched and strained by arterial pressure (21, 28–30). The baroreceptors appear to have evolved from primitive fish to protect gills from excessive blood pressure in the gills by slowing the heart rate (26). A continuous stream of electrical pulses is sent through long bipolar (sensory) neurons projecting into the vasomotor center in the brainstem. The afferent nerves (Hering's nerves) transmitting these action potentials are branches of the glossopharyngeal nerve (CN IX) that run along the internal carotid artery, often as double nerves, through the jugular foramen of the temporal bone (along with CN X and XI), to the solitary nucleus in the brainstem and then to the vasomotor center (3, 31, 32).
The carotid sinus baroreceptors will increase their impulse firing rate within a fraction of a second during systole and decrease it during diastole (21). Even slight pressure changes in the normal operating range cause an immediate and strong feedback signal to correct the pressure. The baroreceptors have an operating range of 50 to 175 mm Hg but are most sensitive at the normal mean arterial pressure of 93 mm Hg (21). The baroreceptors are excited more by rapidly changing pressure than by stationary pressure (21, 33). While the carotid sinus responds to a sudden increase in blood pressure, the rate of impulse firing will diminish within a minute—perhaps due to sensor attenuation, acute central reset, or sympathetic rebound (21, 34–37).
The efferent arc of the reflex includes vasodilatation (VD) and cardioinhibition (CI) in response to carotid sinus stimulation (20, 21, 38) (see Figure 5). Cardioinhibition involves depression of both heart rate and contractility, reducing the cardiac output by 50% or more (20). Parasympathetic action through the vagus nerves directly inhibits the sinoatrial (SA) and atrioventricular (AV) nodes (1, 38). CI of the SA node results in a marked decrease in heart rate, but the CI of both the SA node and the atrioventricular node results in asystole; however, usually for only a few seconds before a 20 to 40 bpm escape rhythm takes over and continues until the vagal stimulation stops (20). Lown and Levine report the effects of direct stimulation of the carotid sinus by carotid sinus massage (CSM): “The cardiovascular effects are upon the sinoatrial pacemaker, the atrioventricular (A-V) conduction system, and the blood pressure…The changes, in order of their frequency, are the following: sinoatrial slowing, atrial conduction defects with changes in amplitude, duration, and morphology of the P wave, sinoatrial bradycardia with rates ranging from 30 to 50 per minute, A-V block, sinoatrial arrest, nodal escape, and ventricular ectopic beats. … When constant pressure is exerted on the carotid sinuses, maximum prolongation of the P-P interval is often observed promptly with the first cardiac cycle after the onset of stimulation. When such pressure is applied for 30 s or more, the sinoatrial rate often returns to its control level within 10 to 15 seconds. With release of pressure the heart rate may accelerate slightly. This is probably due to sympathetic rebound, since there is a reduction in impulse conduction in the sympathetic chain during carotid sinus stimulation.” (1)
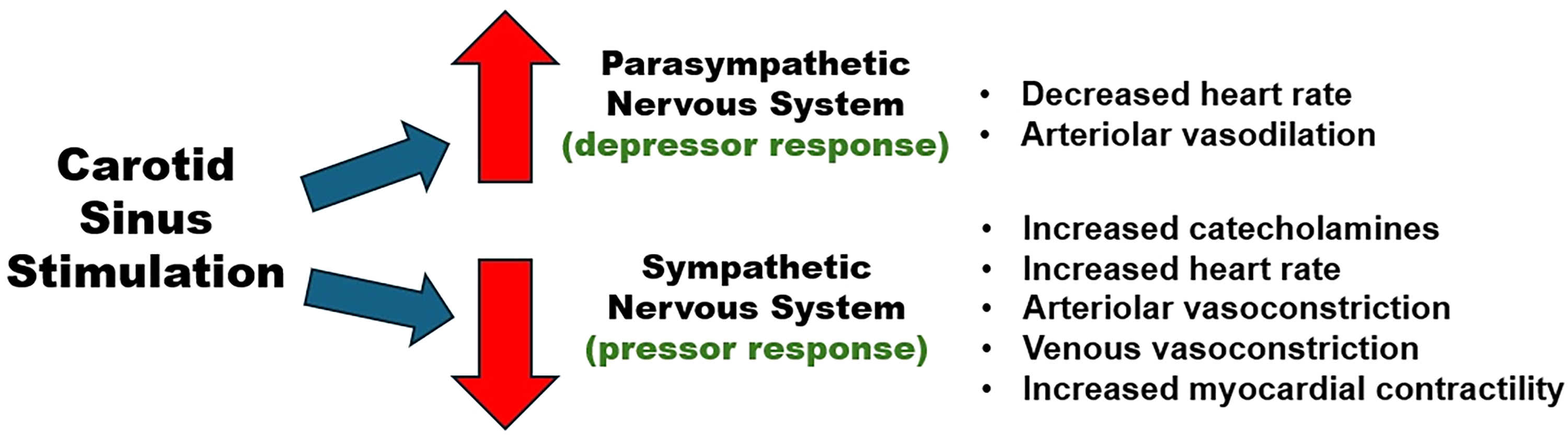
Physiological response to carotid sinus stimulation.
Carotid sinus stimulation immediately triggers a reflex reaction. Prolonged stimulation of the carotid sinus does not result in continuation of the carotid sinus reflex. In the case of George Floyd, he did not die instantaneously or near instantaneously, and therefore, it cannot be attributed to carotid sinus stimulation; the pressure applied to his neck was prolonged—9 ½ minutes.
Reflex Syncope
An exaggerated or abnormal carotid sinus reflex may result in syncope. Syncope is a form of sudden and transient loss of consciousness (TLOC) caused by cerebral hypoperfusion due to a drop in systemic blood pressure rather than from trauma, epilepsy, or psychological dysfunction (ie, psychogenic nonepileptic seizures, psychogenic pseudosyncope) (42–45). Syncope occurs when the systolic blood pressure falls below 60 mm Hg, decreasing cerebral blood flow by approximately 30% (46, 47) and overwhelming cerebral autoregulation (48–50). The response varies, as some individuals lose consciousness after a few seconds of bradycardia, whereas others do not (44). Syncope is a uniquely human phenomenon that may have been an evolutionary adaptation (51), possibly to blood loss or to protect the heart against sympathetic overactivity (52). The mechanism of syncope is not fully understood (45, 53). For instance, reflex syncope occurs in heart transplant patients where all nerves have been cut (54–56), suggesting the release of acetylcholine directly into the bloodstream.
Guidelines on the diagnosis and workup of syncope were published in 2017 by the American College of Cardiology, American Heart Association, and Heart Rhythm Society (ACC/AHA/HRS) and in 2018 by the European Society of Cardiology (ESC) (42–44), with additional guidance published recently (57–59). The American guidelines categorize cardiac and noncardiac syncope, recognizing the potential lethality of the former and the benignity of the latter. The ESC defines 3 etiologies of syncope: (1) cardiac, (2) orthostatic hypotension, and (3) reflex (see Figure 6).
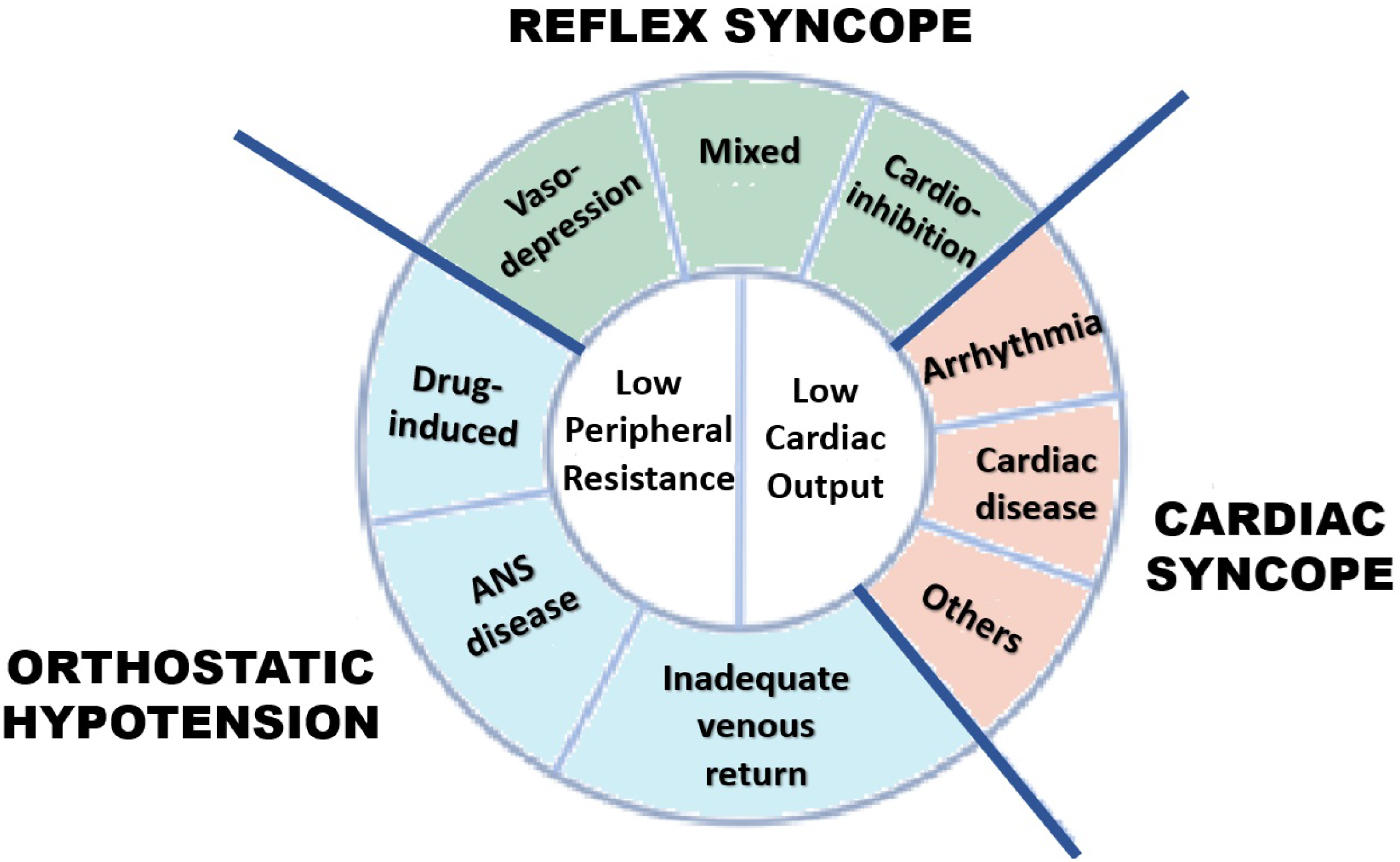
Classification of syncope [adapted from Brignole et al Figure 3 (43)].
Reflex syncope is defined as syncope caused by a reflex that results in VD, CI, or both and is generally considered benign (44, 60). It is a syncopal TLOC arising from an inappropriate, even paradoxical, baroreceptor neurogenic reflex, resulting in profound hypotension and global cerebral hypoperfusion (45–47, 60). Patients with reflex syncope tend to have a somewhat different hemodynamic profile than the general population (61–64). Individuals with marked CI tend to be younger and female (61).
Reflex syncope is not a single entity but a heterogeneous grouping of neurogenic syncopes (60, 65). Reflex syncope is usually subclassified into: (1) vasovagal syncope (VVS), (2) situational syncope, (3) carotid sinus syndrome, and (4) nonclassical forms of syncope (44, 60, 66).
Vasovagal syncope (VVS) is a common and benign neurogenic reflex from autonomic activation causing bradycardia, hypotension, and TLOC (42–45, 60, 67–, 76). VVS is what is meant by a “faint.”’ Episodes usually last for no more than 20 s (72) and resolve without sequelae, except for trauma from falls. Episodes are typically preceded 30 to 60 s before LOC by a characteristic progressive prodrome of headache, pallor, warmth, sweating, and/or nausea. Fatigue may follow the event (43, 44). However, these typical features may be absent in older patients (42).
VVS is by far the most common form of syncope (73–75), occurring in 20% to 40% of the general population (70, 74, 75). Females have a 1.5 times higher prevalence than men (74). VVS occurs in all ages but has a bimodal distribution with peaks at ages 15 and 70 (74–76). VVS is generally more common in younger individuals, while other causes of syncope become increasingly prevalent with age (73, 75, 76). The first episode occurs typically around 13 to 14 years old, with a recurrence rate of approximately 30% (74).
Classic VVS has an emotional or physical trigger, and nonclassic VVS is without a recognized trigger (74). Common triggers for VVS include fear, pain, stress, or strong emotions (42–44, 67, 72). Among the physical triggers are prolonged standing and medical procedures, regional anesthesia, bleeding, and compression of the inferior vena cava (74). Exercise has also been associated with VVS (77). A given stimulus will not trigger syncope in different individuals nor consistently trigger syncope in the same individual (44, 73). VVS does not seem to happen when an individual moves but rather when they are stationary (60). A hot environment appears to increase the risk of VVS (74). VVS occurs most often in the morning after a night's sleep without drinking fluids (60).
Situational syncope is a rare neurogenic reflex syncope with a well-defined trigger, usually specific bodily “situations” (44, 60, 66, 71). Situational syncope is more common in older individuals. The most common trigger is coughing, but it may also be triggered by laughing or sneezing, as well as by gastrointestinal (ie, swallowing, defecation, and endoscopy), or genitourinary (ie, micturition and coitus) triggers. Raising intrathoracic pressure appears to be a common feature. Despite different triggers, the reflex mechanism seems similar, if not identical, to VVS (71).
Carotid sinus syndrome (CSS) culminates in a reproducible neurogenic reflex syncope caused by an exaggerated response to mechanical stimulation of the carotid baroreceptors (1, 42, 43, 60, 78–80). It is defined as carotid sinus hypersensitivity (CSH) (see below) causing syncope (42, 43, 78). CSM in patients with CSS will elicit an asystolic period that is usually >6 s (41). CSS typically occurs in older males and is associated with bilateral obstructive carotid disease (72) and, more generally, with hypertension and atherosclerosis (including coronary and cerebral atherosclerosis) (1). CSS below the age of 40 is exceptional (57). CSS, or just lightheadedness, may be triggered by prolonged standing, sitting, shaving, or turning the head (often while changing clothes) (60). Neck surgery may result in CSS. Mechanical, pharmacological, and orthostatic factors may stimulate CSS (81). The right carotid sinus is more than twice as likely as the left to produce a cardioinhibition response to carotid stimulation (82).
Carotid sinus hypersensitivity (CSH) is a condition in which individuals exhibit an exquisite sensitivity and an exaggerated response to mechanical stimulation of the carotid baroreceptors without syncope (1, 42, 43, 78–80, 83–86).
CSH was first described by Roskam (82, 86). Despite its name, CSH is defined not by baroreceptor sensitivity but rather by reflex response. Both the ESC and AHA guidelines define CSH as (1) a fall in systolic blood pressure of ≥50 mm Hg and/or (2) a ventricular pause of ≥3 s in response to cardiac sinus massage (CSM) (see below) (42, 43). It has been suggested that the 3 s criterion for CSH is too sensitive and should be changed (78, 87). CSS is often assumed to be a severe form of CSH, but that is not necessarily so (85). CSH typically occurs in older males; it is associated with age, hypertension, and atherosclerosis (78). Kerr found that 39% of those over 65 years of age have CSH, and he noted a prevalence of vasodepressor response in this elderly cohort (87, 88). Advanced age is a prominent risk factor for baroreceptor dysfunction, and blood pressure variability is a marker of age (27, 59). Doberentz et al state that atherosclerotic CSH occurs after the age of 40 and “asystolia” (CSS) after the age of 60 (9–11) (but see Figure 1 of reference 62). An exaggerated baroreceptor response is associated with decreased distensibility of the carotid wall (89). Doberentz et al also note that diseases that promote atherosclerosis (hypertension and diabetes), medication (insulin, digitalis), icteric disease, and space-occupying lesions in the neck can increase the reflex activity of the carotid sinus; in contrast, alcohol may lower it (9–12). Nouraei has recently noted that patients with laryngeal dysfunction have reduced baroreflex sensitivity (“overwhelmed vagus hypothesis”) (90).
The carotid sinus reflex causing syncope is primarily vasovagal syncope in young females and carotid sinus syndrome in elderly males. George Floyd, a 46-year-old Black male, did not fit either of these epidemiological profiles.
Reports of Deaths Due to Carotid Sinus Stimulation
Provocative testing of the carotid sinus through tilt-table testing (TTT) or carotid sinus massage (CSM) is commonplace in the clinical setting where safeguards are in place (91–96). CSM and TTT are complementary diagnostic tests for noncardiac syncope, with CSM being better at diagnosing bradycardic phenotypes and TTT being better at diagnosing hypotensive phenotypes (59).
TTT is frequently performed to diagnose and assess syncope (93). It is an orthostatic/hypotensive challenge and is almost exclusively the basis for most research on syncope (45, 47, 51, 96–98). Velazquez-Rodriguez et al reviewed the long-term follow up of patients with tilt-induced asystole and concluded: “[TTT] “is safe and low-risk, …even four decades ago, it was suggested that asystole may present as a life-threatening manifestation of neurally mediated syncope… asystole does not necessarily predict adverse outcomes, with most patients having a benign clinical course…” (99). Van Dijk found asystole (ventricular pause of >3 s) in 42% of 163 patients with tilt-induced reflex syncope (98), and Russo found asystole in 28.6% of 1285 such patients (99), while other studies found lower rates using different definitions, methods, and populations. The asystole evoked during tilt table testing may last up to a minute but is typically only a few seconds (46). However, after syncope or EEG slowing, the subjects are immediately placed back in the horizontal position, where they recover, which may have prevented deaths.
The CSM technique, first explicitly described by Parry in 1799 (1, 78), has evolved (78) and currently includes firm pressure for 10 s (1, 94–96). CSM is used diagnostically for syncope and therapeutically for supraventricular tachycardias (1, 100, 101). A positive CSM test without symptoms defines CSH; with symptoms, it defines CSS (78, 96); nonetheless, the diagnostic value for syncope has been described as dubious (102).
CSM is considered a safe procedure and has become safer, with stroke as the primary concern (96). Cases of strokes and deaths have been reported (103–106), but not myocardial infarctions. De Lange et al declared the first step in performing CSM is to exclude patients with contraindications, specifically patients with high-grade carotid stenosis or a history of transient ischemic attacks or strokes within the last 3 months (96). The patient should be monitored by electrocardiography and performed in a medical facility with an ACLS crash cart.
We have found 7 case reports of deaths after CSM from CI (107–112), although the case of Porus and Marcus involved a delay of death and thus not as clearly attributable to the CI; these reports are summarized in Table 1.
Reports of Fatalities After Clinical Carotid Sinus Stimulation.
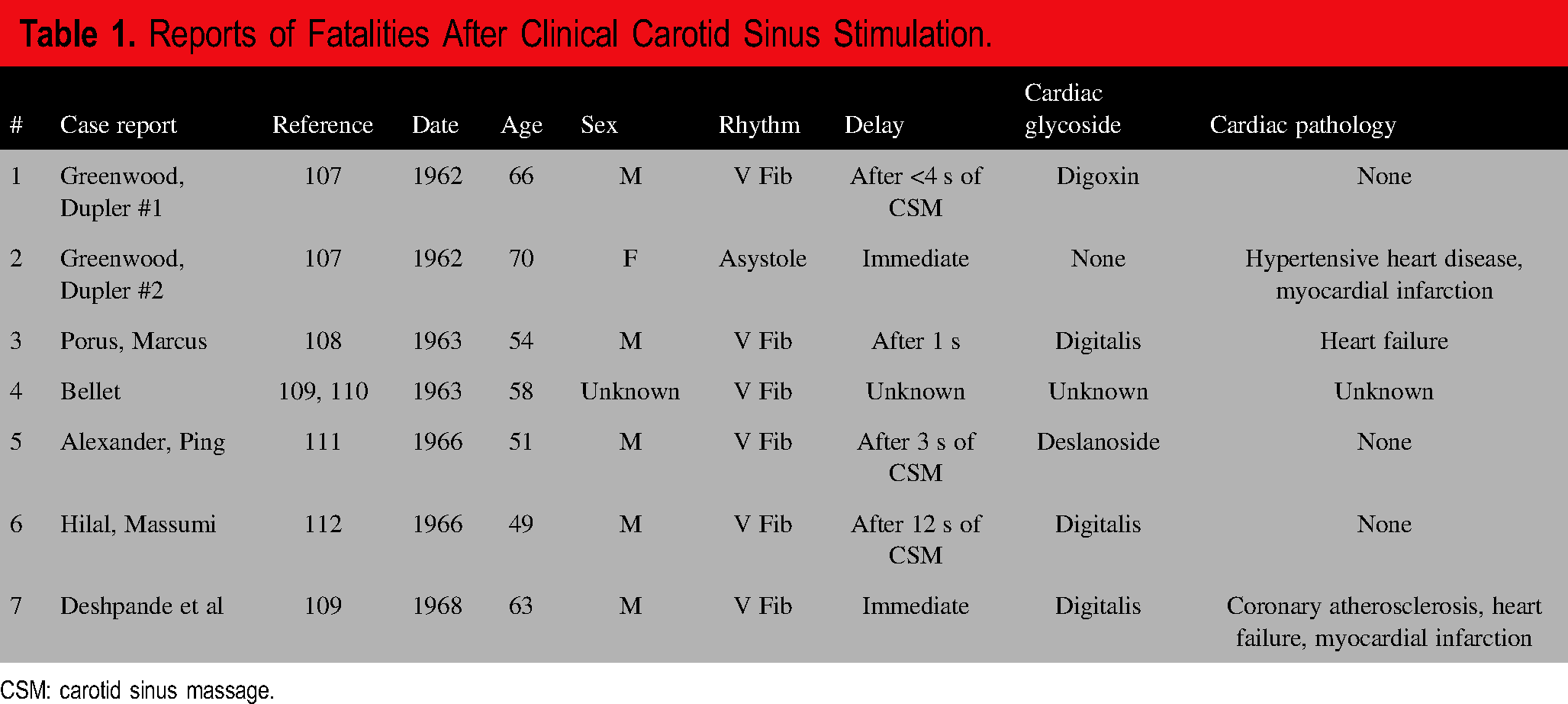
CSM: carotid sinus massage.
Given the many thousands of times CSM and TTT have been performed, this represents a vanishingly small number of deaths, even recognizing that not all cases are reported. Deshpande et al considered ventricular fibrillation to be transient and did not attribute the death to it (109). There are also reports of nonfatal ventricular arrhythmias after CSM (109, 113–115).
In these 7 cases of death from CSM, the CSM was used therapeutically for supraventricular tachycardia in mostly ill patients on a cardiac glycoside. There have been no more reports after 1968, perhaps due to the decline in the use of cardiac glycosides and preventive safety measures, or that such case reports are no longer publishable.
The mechanism of death appears to be ventricular fibrillation. The time frame for developing ventricular fibrillation after CSM was from “immediate” to more than 12 s of massage, but usually after 1 to 3 s.
In the case reported by Alexander and Ping, no cardiac pathology was confirmed at autopsy (111). Deepak et al reported a nonlethal case of ventricular fibrillation with a full cardiovascular workup that was negative (114), and Tontsch et al reported a nonlethal case of 55s asystole following CSM that afterward had a negative Holter monitor (115). It cannot be said that an underlying cardiac pathology is a necessary requisite for death from carotid sinus stimulation.
Death does not appear to result from continued cardiac standstill or severe hypotension produced directly from vagal CI (116) but instead from the rare development of ventricular arrhythmia (see Table 1). In an early case, Greenwood and Dupler reported a 70-year-old woman suffering an acute posterior myocardial infarction (case #2); they reported that her heart just stopped; it was not a well-documented case, and there was no ECG recording or autopsy (107). Velazquez-Rodriguez et al declared that concern for asystole is antiquated (99). Tontsch described asystole after CSM as a “cardiac arrest,” but this now seems to be an overreaction (115). Thus, asystole in this setting is better termed a “ventricular pause.” This is consistent with clinical researchers using TTT. Resumption of the rhythm after asystole may be from sympathetic override, baroreceptor attenuation, acute vasomotor center reset, a sympathoexcitatory cerebral reflex, or intrinsic ventricular automaticity.
Ventricular fibrillation is generally associated with sympathetic stimulation, but it appears to be after a vagal reflex in these cases. Perhaps ventricular fibrillation is a manifestation of a sympathetic response to parasympathetic activity. Several authors in the reports mentioned here rationalized the development of ventricular fibrillation as likely from acetylcholine or the few vagal fibers reaching the cardiac ventricles (110, 111, 115). Interestingly, the first case of ventricular fibrillation (case #1 of Greenwood and Dupler) involved a patient after vagotomy and is reminiscent of the cases of vasovagal syncope after heart transplant noted above (107). ECG studies of CSM have been reported; they note greater automaticity but do not mention ventricular fibrillation (40, 117–120). Vagal stimulation is known to give rise to ventricular ectopy (1, 116). Furthermore, vagal stimulation may cause arterial spasms and local ischemia (121–123). Any of these mechanisms may result in ventricular fibrillation (124–128). In general, vagal stimulation may be cardioprotective to hypoxia (129–132).
This clinical literature evidence that deaths from the carotid sinus reflex do not die of asystole but of ventricular tachycardia or fibrillation. George Floyd died with an initial cardiac rhythm of pulseless electrical activity, not asystole or ventricular fibrillation.
Reports of Instantaneous Neurogenic Cardiac Arrest Deaths
The potential of a lethal carotid sinus reflex came to the attention of the forensic community in a 1926 German trial. von Dielingen was sentenced to death for the killing of his pregnant lover (12, 133–136). In his initial confession, he stated that he grew angry in a heated discussion; he grabbed at her neck scarf and pulled her close; she kicked her legs a few times and then went quiet. In a second confession, he stated that he only pulled at the cloth, and then she suddenly collapsed. The usual injuries associated with strangulation were not present, only very slight external marks. It was postulated that she died of a Hering's reflex rather than an intentional ligature strangulation. A member of the court opined, “It seems to me beyond doubt that the carotid sinus reflex can cause sudden death if the fact stated by Herring is correct, that an isolated stimulus to this area can cause cardiac arrest.” The perpetrator's confession was found to be credible, and he received a reduced sentence of 2 years for bodily harm that resulted in death. Professor Lochte, the head of forensic medicine at the University of Gottingen, wrote about the case and noted that in Hering's 1927 monograph, he had a paragraph entitled, About the influence on the Sinus caroticus in cases of hanging, throttling, and boxing, in which he wrote, “Since by the compression of the carotid arteries it may come to extra-systoles and in proper disposition also ventricular fibrillation. These consequences have to be considered in Legal Medicine, especially in cases where throttling was not long or heavy but nevertheless deadly” (135).
This trial scenario was later repeated in the U.S. 1986 “Preppy Murder” (137–139). The defendant alleged that the death was a freak accident during rough sex rather than manual strangulation. The jury deadlocked, and the defendant entered a plea that reduced the charge of second-degree murder to first-degree manslaughter, and he served 15 years in prison. Given the medical examiner's description of bruising and scratches on her neck and conjunctival petechiae, we view this as merely a successful defense ploy in a typical manual strangulation.
We define instantaneous neurogenic cardiac arrest (INCA) as an immediate collapse or death mediated through a vagal neural reflex. The first case reports of INCA deaths by a forensic pathologist were by Keith Simpson in 1949. He wrote in the Lancet, “the catastrophic suddenness of vagal inhibition can only be explained as a neural reflex conditioned by some sharp stimulus” (140). He reviewed 87 cases of fatal reflex inhibition and declared that the sources for the reflex action were obstetrical in 19, serous membrane in 18, throat and glottis in 17, bladder and urethra in 13, carotid sheath in 9, skin in 4, cardiovascular in 3, alimentary (viscus) in 3, and peripheral nerve in 1. He described in more detail 6 cases.
We have identified 27 deaths reported in the literature in which the authors have posited an INCA mechanism.
In 4 cases, INCA was determined by history alone (see Table 2). In each case, the death was instantaneous or near-instantaneous after a physical trigger, with no other obvious explanation for the death. At least 3 of the cases involved young adults. Half of these cases were male and half female. One was pregnant, one was undergoing thoracentesis, another undergoing thyroidectomy, and one was presumably healthy. An unrevealing autopsy was performed in one case.
Reports of Deaths From INCA Based on History.
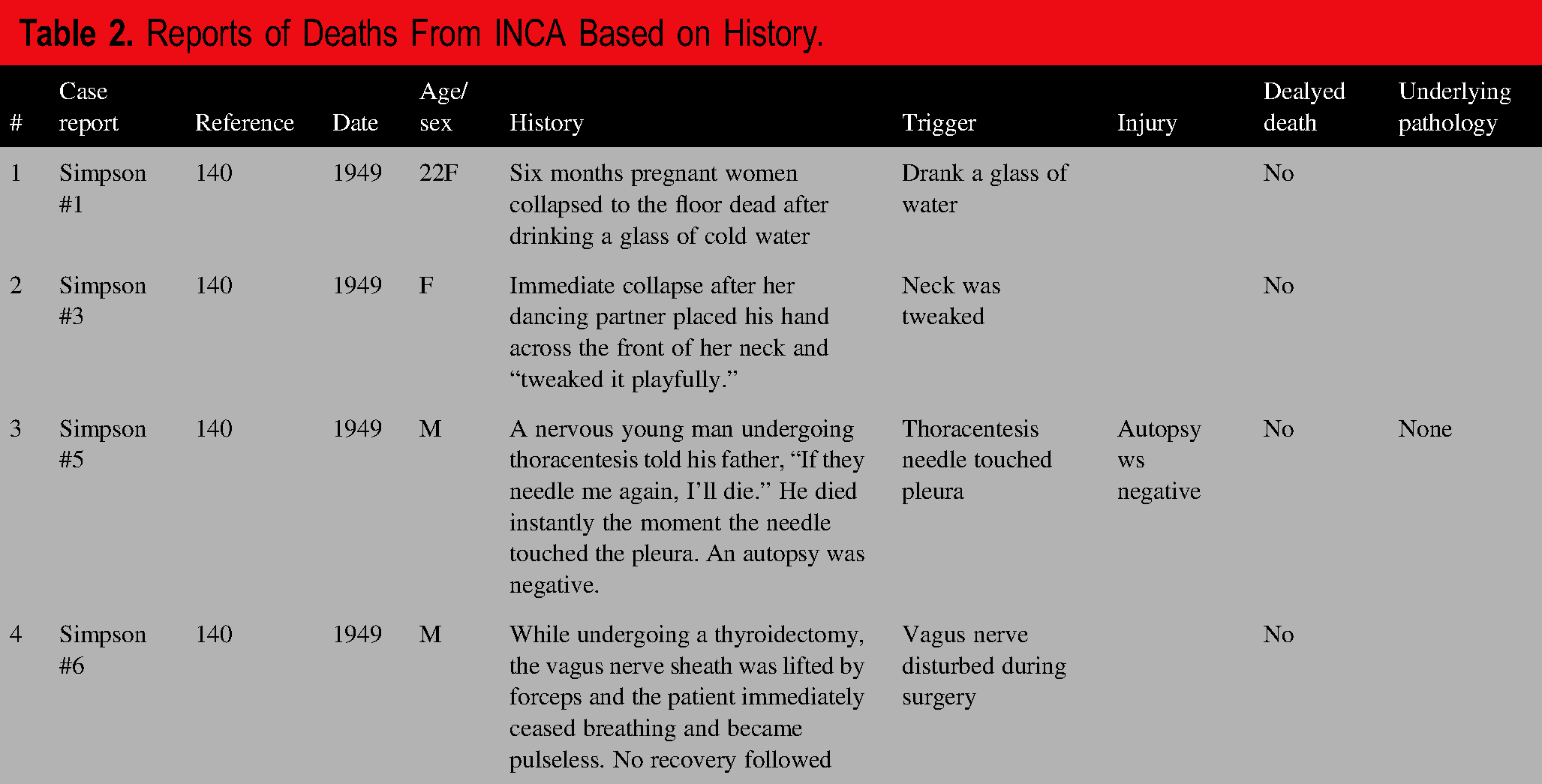
Only one of these cases involved pressure on the neck, described as a “tweak,” and the other 3 involved stimulation of the oropharynx (drinking a glass of water), a serous membrane (pleura touched by thoracentesis needle), and vagus nerve (during surgery). Case #2, involving the mere tweak of the neck, is reminiscent of the von Dielingen and Preppy deaths.
All of these cases were reported by Simpson (140). Simpson's case #4, not listed here, involves an unpopular janitor who was subjected to a mock guillotine execution by students. “He was in terror as last rites were read, and collapsed and died the instant a wet towel was flicked …across the back of this neck.” We view that case as an instance of “frightened to death,” caused by emotional stress and activation of the sympathetic autonomic nervous system (141–147), and not from a parasympathetic vagal reflex characterizing INCA. Simpson's case #5 may also be a case of fright.
In 8 cases, INCA was determined by the absence of evidence of vital reaction at death (148), indicating an instantaneous or near-instantaneous cardiac arrest, although one death occurred after 4 to 5 min and another after 8 days (see Table 3). This group was populated by middle-aged and older adults, predominantly males, with underlying disease noted in only 2.
Reports of Deaths From INCA Based on an Absence of Evidence of a Vital Reaction at Death.
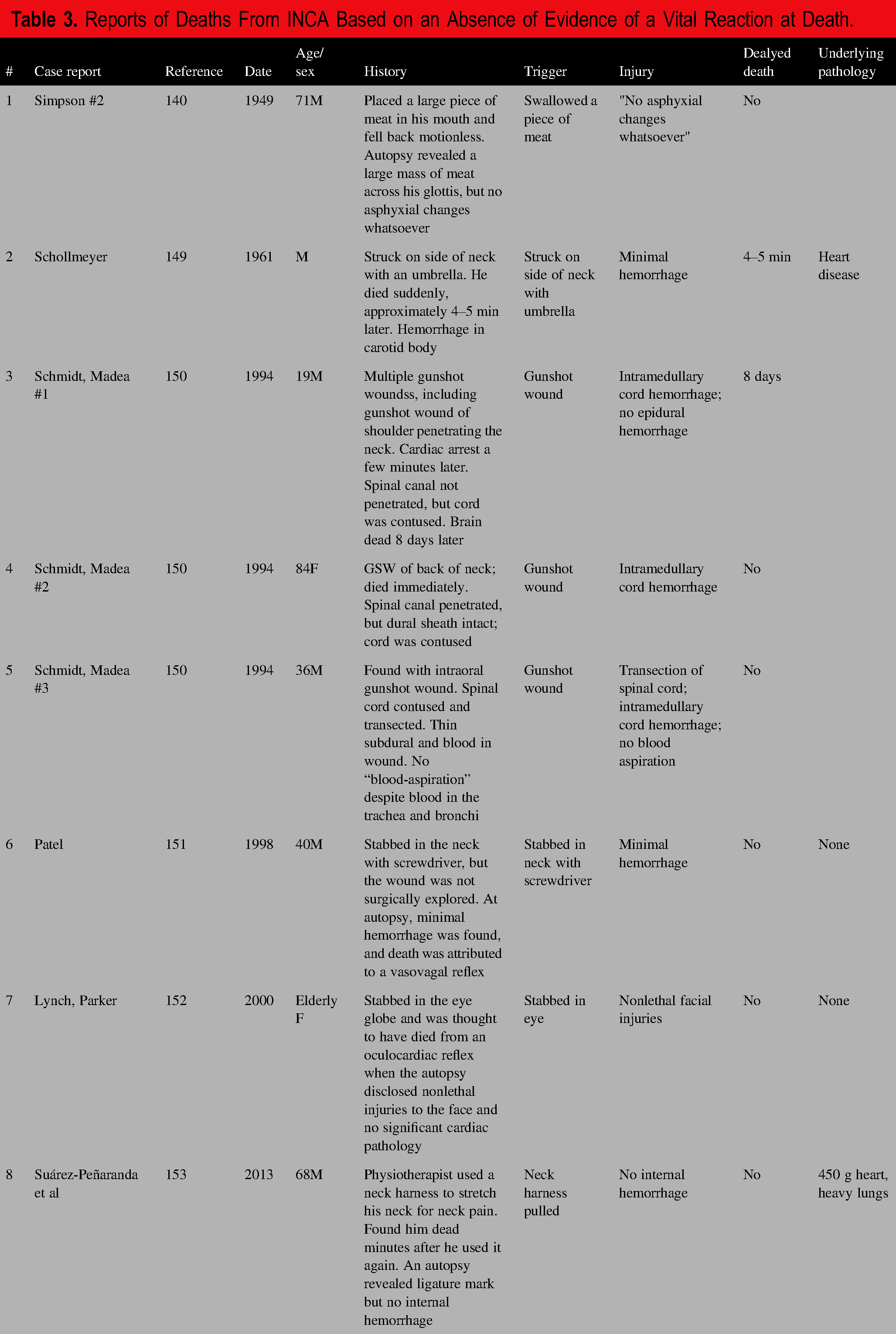
The absence of evidence of vital reaction at death was usually an absence of the expected hemorrhage, but an absence of “asphyxial changes” in Simpson's case #2 and an absence of blood aspiration in Schmidt and Madea's case #3. In that case, the authors described wound hemorrhage and blood filling the trachea and bronchial tree. The authors pointed to intramedullary spinal cord hemorrhage, postulated that it triggered a “reflex cardiac heart arrest,” and referred to experimental contusions of spinal cords that result in an initial hypertensive phase followed by bradycardia and hypotension. Simpson's case of a meat bolus in the airway and the 3 gunshot cases of Schmidt and Madea are less convincing due to an obvious explanation for their deaths; the other 4 cases are more compelling. All appeared to have had an autopsy, and the case of Suárez-Peñaranda et al was particularly well worked up.
Two cases involved no injury at all and one minor nonlethal injury, but 5 sustained significant injuries. The absence of hemorrhage in the case of the stabbing in the neck by a screwdriver, that missed vital structures, was particularly remarkable. A neck trigger was involved in all, but one case of a person stabbed in the eye triggering an “oculocardiac reflex” and one case involving swallowing. The case of Suárez-Peñaranda involved a neck harness and is reminiscent of the von Dielingen and Preppy deaths.
In 13 cases, INCA was determined by hemorrhage in the “reflex zone,” an area surrounding the carotid sinus (9–12), and, in a fourteenth case, INCA was determined by hemorrhage around the celiac plexus (see Table 4). Ten cases were sudden and 3 were delayed deaths. This group was populated by young and old, with and without other underlying pathology.
Reports of Deaths From INCA Based on Hemorrhage in the Reflex Zone.
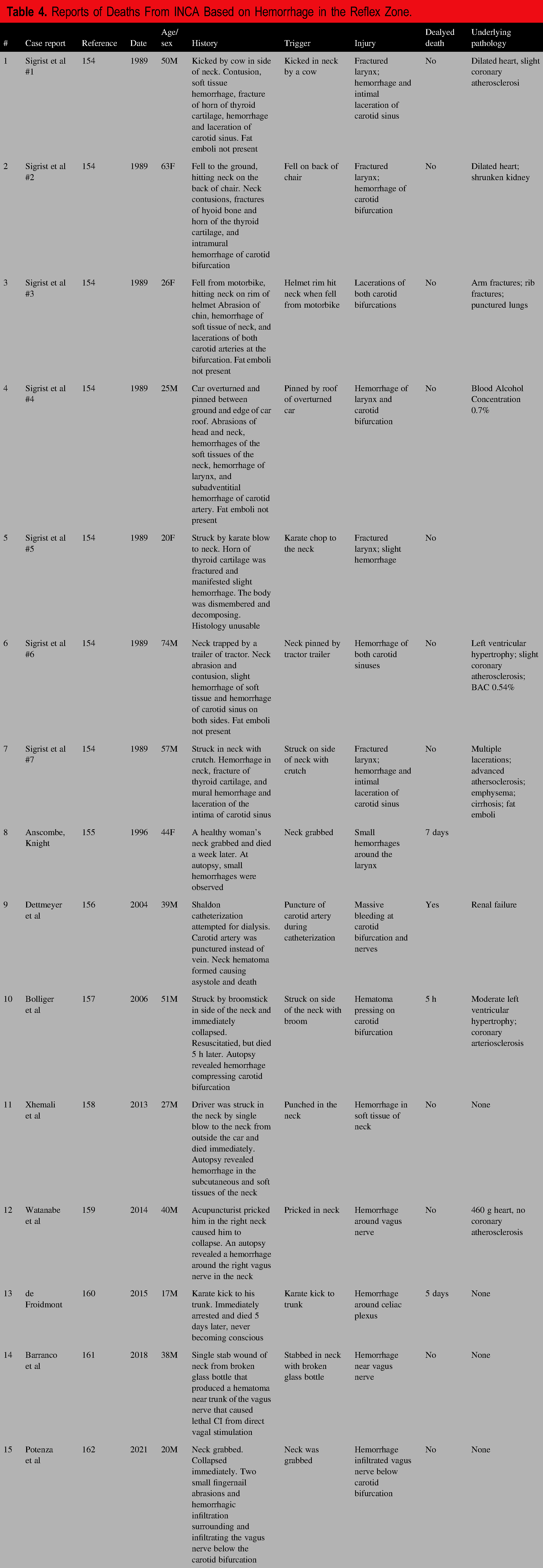
Nine cases involved serious neck injuries (cases #1-7, 9, and 14), but ostensibly nonlethal were it not for the presumed INCA reflex. Injuries to the neck with continued bleeding are considered dangerous and require surgery (163). In 40% of penetrating neck trauma cases, there is no significant damage to structures; damage to a major artery is seen in only 10% to 15% (164). Magnetic resonance imaging (MRI) studies of survivors of strangulation have shown that hemorrhage of the soft tissues of the neck is not uncommon and is not always externally visible, but such studies have not explicitly reported the prevalence of hemorrhage in “reflex zones” (165–167).
The remaining 5 cases (case #8, 10-13, 15) involved minimal injury but had hemorrhage allegedly triggering a neurogenic reflex death. These cases involved grabbing, pricking, striking, and stabbing of the neck as well as one karate kick to the stomach. The cases of Anscombe and Knight and of Potenza et al are reminiscent of the von Dielingen and Preppy deaths. In 2012 and later in 2019, 2020, and 2022, Doberentz et al published their studies on injury to the carotid sinus in neck trauma cases (9–12). They did not study cases of “massive” neck trauma as described by Sigrist et al, nor was there any case of sudden collapse; this was not a study of INCA cases. Instead, they studied cases of carotid sinus trauma. The original study included 20 cases, but the set was extended to 22 cases in 2022 (ages ranging from 10 to 91 years), including 16 hangings and 6 ligature strangulations. A control group was also studied, consisting of 82 cases without neck compression or head trauma. Gross and microscopic examinations, including immunohistochemistry and iron stains, were conducted. None had severe plaque arteriosclerosis, but 2 exhibited “relevant carotid bifurcation stenosis,” although varying arteriosclerosis was found in the control group. None showed findings evidencing direct trauma of the carotid bifurcation. They found only one case with hemorrhage in the soft tissue around the carotid bifurcation, which was in a ligature strangulation case with hemorrhage in the subcutaneous tissues and anterior musculature of the neck, laryngeal hemorrhage, and fractures of the hyoid bone and thyroid cartilage. However, the hemorrhage was outside the “reflex zones”—it did not extend into the wall of the carotid artery or within the carotid body, and the death was not considered an immediate sudden death because, at autopsy, there was swelling and lividity of the face and petechiae of the neck musculature, interpreted as signs of preserved circulation. In no case did they find evidence of lethal cardiac reflex. They noted that continued bleeding may lead to a delayed reflex due to an expanding hematoma that might press against the carotid sinus or infiltration that might eventually reach the carotid sinus, in which case vital signs will be present at autopsy.
Discussion of the Forensic Literature
INCA as an explanation for death is found in the current edition of Knight's Forensic Pathology textbook (168), under the chapter heading Fatal Pressure on the Neck, “The vagal reflex has profound implications in relation to pressure or blows on the neck. Sometimes called ‘vagal inhibition,’ ‘vasovagal shock,’ or ‘reflex cardiac arrest’ …Overstimulation of nerve endings in the carotid sinus or adjacent arterial sheath may be brought about by direct pressure from fingers or from a ligature during strangulation or hanging—or from a blow directed at the side of the neck. Severe pain, such as a blow on the larynx or genitals, may also trigger a ‘vagal response … However, it is not known whether cardiac arrest caused by the vasovagal reflex can spontaneously revert to normal rhythm some minutes later … It is a matter of some dispute as to whether this reflex can cause immediate cardiac arrest or whether there has to be a period of marked slowing of the heart with negligible cardiac output – or whether an arrhythmia such as ventricular fibrillation precedes such an arrest.”
Yet, most other forensic pathology textbooks do not include such a passage (169). Reported cases have been sparse and consist of brief descriptions. In these cases, is INCA a logical inference or a speculative leap? A ventricular pause is not a cardiac arrest, but could the vagal response lead to ventricular fibrillation as Herring suggested? Skepticism is warranted, but can such reported cases be outright dismissed? What evidence could support functional disturbance that lasts seconds? Forensic pathologists can search for anatomic causes of death and have difficulty proving functional causes of death.
Doberentz et al reviewed the clinical literature, particularly the German literature, and concluded: “In healthy people, triggering a significant (lethal) cardiac reflex seems to be impossible, even with strong bilateral pressure on the carotid bifurcations” (9–12). They refer to a study by Kleemann, who applied pressure to the necks of 8000 subjects (aged 15–95) without any deaths (170), to animal experiments by Mueller in which researchers were unable to inflict lethal irritation of the carotid sinus (171), and an article by Denk reporting that in martial arts where lateral blows to the neck are used to temporarily knock out opponents by inducing syncopal events yet no deaths having been reported (172) [but see Sigrist (154,160,) and de Froidmont et168); the “commando punch” is banned because of its lethal potential ()].
In 2011, Schrag et al, from the University Centre of Legal Medicine (Lausanne-Geneva), reviewed the literature on what they termed “cardioinhibitory reflex cardiac arrest (CiRCA)” (173). Of the initial 1475 articles based upon searching variations of 4 terms (death, reflex, trauma, and neck or throat), they identified 12 relevant articles and then added 17 other publications by other means, resulting in 48 publications for their review. They included cases from as early as 1880 but found that most articles before Simpson's 1949 article involved cerebral hypoxia from prolonged neck compression. The authors felt other mechanisms of death were more likely than CiRCA in more than half of the cases. Of the 48 articles reviewed, they could not exclude CiRCA from 20 reported deaths. However, they noted that these included many cases involving police in the 1970s and 1980s. Thirteen of 19 cases following carotid stimulation were positive for drugs or alcohol. They identified only one case, reported by Bolliger et al in 2006, in which they found no alternative possible explanation, although the victim in that case did have cardiovascular disease.
Schrag et al declared: “CiRCA is a diagnosis by exclusion that requires a thorough investigation including histopathological, metabolic, genetic, and toxicological analysis to rule out other mechanism[s] of sudden unexplained death or identify carotid bifurcation stimulation as a contributory factor” (173). Schrag et al's literature search was limited by the inclusion of “trauma” as a requisite search term. We also think the authors were too quick to dismiss cases. Schrag et al declared that “studies that support a link between CiRCA and death are observational and remain insufficient to infer a causal link.” They concluded, without conclusive evidence, that “reflex cardiac arrhythmia due to carotid bifurcation stimulation cannot provoke death without the presence of contributory factors,” such as drug abuse, cardiac pathology, and physical or mental excitation.
In a subsequent article, Schrag et al sent out 1429 electronic questionnaires on the issue of “cardioinhibitory reflex” death to forensic experts worldwide in 2007, but only 182 experts responded (174). They found that 80% of the responding experts believed that the cardioinhibitory reflex could theoretically cause death, whereas 10% rejected it as a cause of death, and 10% had no opinion. Only 42.3% used it as a cause of death. There was no consensus on diagnostic criteria among the responses of experts surveyed. Of the 42.3% that used the diagnosis, they reported using 18 different combinations of suggested diagnostic criteria, and 30.8% said the diagnosis was one of exclusion. In that second Schrag article, the authors declare that 5 articles on sudden death after neck compression were well-known and often cited; these included Simpson's article (140) and 4 others in the German literature that discuss the von Dielingen case (133–136).
In 2013, Suárez-Peñaranda et al described 3 criteria for INCA: (1) circumstances were consistent with a sudden cardiac arrest, (2) a triggering stimulus was present, and (3) an autopsy ruled out other causes of death (153).
It appears that several investigators have concluded that due to the rareness of INCA, some preexisting conditions, presumably underlying cardiac conditions, must be present. Kleemann et al conclude, “According to the available literature and the pathophysiological basis of the carotid sinus reflex, a sudden death caused by a short grip on the neck appears to be conceivable only under special conditions for the injured person and is practically impossible in the ‘normal case’” (170). Schrag et al conclude, “Our findings support the presumption that reflex cardiac arrhythmia due to carotid bifurcation stimulation cannot provoke death alone. Actual state of knowledge suggests CiRCA might be contributory to death in the presence of drug abuse and/or cardiac pathology, often associated with physical and/or mental excitation.” (173). Doberentz et al conclude, “According to the literature, sudden death after a short grip to the neck seems to be extremely improbable in a ‘normal case’ and should be considered only when special preconditions are present in the deceased” (10). However, the reported clinical and forensic cases include cases in healthy adults without underlying cardiac conditions.
Doberentz et al also conclude, “There is general agreement that a sinus reflex can occur and can rarely cause death, but it seems to play no role in healthy children, adolescents, and young adults.” However, the reported forensic cases include young adults. Children and adolescents appear to be spared, and we note that the carotid sinus does not develop until adolescence (10).
INCA is an immediate collapse or death mediated through a vagal neural reflex. The forensic literature reveals several reports of INCA deaths, but they are often poorly documented and unconvincing. The forensic pathology literature is wanting (169). As Schrag stated, “In practice, the association between cardioinhibitory reflex and death remains difficult or even impossible to prove” (174), but so too are they difficult to disprove. A history of instantaneous death, absence of evidence of vital reaction at death, and bleeding in the reflex zones have been used to rationalize an INCA theory of death without other explanations for the death.
The forensic literature suggests that George Floyd did not die of INCA. Other explanations for Floyd's death have been imputed. No hemorrhage of the soft tissues of the neck was found, but numerous contusions were described, indicating continued heart pumping, although some of such hemorrhages may be accounted for by cardiopulmonary resuscitation. Thus, neither the absence of vital reaction to his injuries nor hemorrhage in a reflex zone were described in his autopsy report.
Conclusion
We believe the literature supports the existence of INCA deaths. However, they seem to be extremely rare and difficult to prove or disprove. Most forensic pathologists would need to justify such a determination rigorously, supported by solid evidence or exclusion of other causes. George Floyd's death did not align with an INCA pattern, and other causes/mechanisms of death are being imputed, the demise of George Floyd cannot be justified as an INCA death.
Supplemental Material
sj-doc-1-afp-10.1177_19253621251327721 - Supplemental material for Did George Floyd Die of Cardioinhibition From Pressure on His Neck?
Supplemental material, sj-doc-1-afp-10.1177_19253621251327721 for Did George Floyd Die of Cardioinhibition From Pressure on His Neck? by Victor W. Weedn, MD, JD, Alon Steinberg, MD, and Peter Speth, MD in Academic Forensic Pathology
Footnotes
ACKNOWLEDGEMENTS
None.
DECLARATION OF CONFLICTING INTERESTS
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
FUNDING
The authors received no financial support for the research, authorship, and/or publication of this article.
SUPPLEMENTAL MATERIAL
Supplemental materials for this article are available online.
Authors
Roles: A–E, 1, 4, 5, 6
Roles: B–E, 5 ,6.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.