
Abstract
Importance
With advancements in robotic surgery, robotic-assisted thyroidectomy is gaining popularity. The introduction of the 3-port transoral robotic thyroidectomy (T-TORT) offers an alternative approach with potential benefits in postoperative recovery compared to traditional methods.
Objective
To assess the safety and feasibility of T-TORT in comparison to the transoral endoscopic thyroidectomy vestibular approach (TOETVA).
Design
A retrospective cohort study with 1:1 propensity score matching was conducted to compare perioperative outcomes between T-TORT and TOETVA. The learning curve was analyzed using cumulative summation (CUSUM).
Setting
Tertiary A hospital.
Participants
One hundred sixty-two patients who underwent either T-TORT or TOETVA were included.
Intervention or Exposures
The T-TORT group underwent three-port robotic thyroidectomy, while the TOETVA group received standard transoral vestibular endoscopic thyroidectomy.
Main Outcomes and Measures
Demographics and perioperative data were compared. The learning curve was evaluated using CUSUM.
Results
Compared with the TOETVA group the operation time in minutes of the T-TORT group was relatively longer (136.14 ± 36.52 vs 122.49 ± 34.85, P = .012), the postoperative stay, in days, was shorter (2.77 ± 0.78 vs 3.51 ± 0.95, P < .001), the drainage volume on a postoperative day 1 (POD1) and POD2, in milliliter, was less (POD1 56.57 ± 23.29 vs 65.12 ± 26.04, P = .029 and POD2 27.43 ± 25.29 vs 38.21 ± 25.09, P = .008). The other statistics, including bleeding amount, retrieved and metastatic central lymph nodes, visual analog scale score, and drainage volume on an operative day were comparable between the 2 groups. Meanwhile, there were no significant differences between the 2 groups in postoperative complication rates. The turning point of the learning curve was in the 16th case with a hemithyroidectomy with central neck dissection (CND) and the 21st case with a bilateral thyroidectomy with CND.
Conclusions and Relevance
T-TORT is a safe and feasible option with enhanced postoperative recovery compared to TOETVA. It may be a preferable choice in specific clinical situations.
Trial Registration
This study was registered at the Chinese Clinical Trial Registry (UIN: ChiCTR2300069021, https://www.chictr.org.cn) in accordance with the World Medical Association’s Declaration of Helsinki, 2013.

Keywords
Introduction
Transoral robotic thyroidectomy (TORT), as a further refinement of the conventional endoscopic transoral approach, has attracted more and more attention from surgeons and patients.1-4 The TORT has the advantages of precise operation and shake-filter technology, and it can also provide 3d high-definition vision.5-7 All these features provide advantages for nerve exposure and parathyroid gland protection.8-10 Current studies have reported that TORT has advantages in the narrow neck space, leading to a satisfactory outcome and a faster recovery compared with the transoral endoscopic thyroidectomy vestibular approach (TOETVA).11-13
Initially, TORT was conducted utilizing 3 vestibular incisions. 14 Nevertheless, with the introduction of the axillary incision by Dr. Hoon Yub Kim, 3 the prevailing approach to TORT now involves a 4-port technique incorporating an additional axillary incision.12,15,16 This modification facilitates surgical manipulation and specimen extraction. However, the construction of the axillary tunnel increases the operation time and affects the patient’s postoperative recovery. 17 Patients may experience pain and discomfort in the anterior chest wall in the short term after surgery, and there is even a risk of injury to the brachial plexus nerve, internal jugular vein, and carotid sheath.18,19
In response to these challenges, some surgeons have reverted to the three-port TORT (T-TORT) approach without the axillary incision.15,17,20 Additionally, Park et al proposed a single-incision approach for TORT, 20 which aligns with our previously reported single-incision technique for exposing the mental nerve. 21 In this study, we further evaluate the safety and efficacy of T-TORT by comparing it with TOETVA.
Methods
Study Cohort
This was a retrospective cohort study performed at a single tertiary-level academic health care institution. We recruited into this study a total of 281 patients consecutively admitted to our hospital who underwent endoscopic thyroidectomy from July 2021 to September 2022. According to the operation method, they were divided into an experimental group (T-TORT group) and a control group (TOETVA group). All patients were well informed about the characteristics of each procedure and chose T-TORT or TOETVA on their own. All the surgeries were performed by the same surgeon at the Hunan Cancer Hospital, Changsha, China. This study was registered at the Chinese Clinical Trial Registry (UIN: ChiCTR2300069021, https://www.chictr.org.cn) in accordance with the World Medical Association’s Declaration of Helsinki, 2013. This study was compliant with the STROBE guidelines. 22
The inclusion and exclusion criteria were as follows 21 :
Inclusion criteria included: (1) Over 18 years old; (2) Benign tumor with a diameter not exceeding 6 cm; (3) Differentiated thyroid carcinoma with a diameter not exceeding 4 cm; (4) Patients without parathyroid-related diseases; (5) Preoperative laryngoscopy showed no abnormalities; (6) Patients understood the content of this study and signed an informed consent.
Exclusion criteria included: (1) Patients who were unfit for surgery; (2) History of neck surgery or radiotherapy; (3) Hyperthyroidism or hypothyroidism; (4) Clinically evident lateral neck lymph node metastasis; (5) The tumor invaded the capsule or adjacent structures such as the trachea or esophagus or severe tissue adhesions; (6) Distance metastasis; (7) Endoscopic surgery was converted to an open technique; (8) Patients lost to follow-up.
Preoperative Preparation
A 2.0 g Cefazolin infusion was given 30 minutes before the surgery. After general anesthesia, the patient was placed in a supine position with arms adducted and fixed in position. The neck was maintained in a slightly overstretched position.
Surgical Procedure
T-TORT group
A silk thread was used to locate the vestibular midpoint. Two retractors were used to retract the lower lip to fully expose the oral vestibule. At the midpoint of the vestibule, a small transverse incision of 1 to 2 cm in length was made with an electrotome to avoid cutting the lower lip frenulum (Figure 1A). The incision was extended to both ends of the first premolar to expose the mental nerves bilaterally (Figure 1B). Part of the mental muscle was severed, and an electrotome was used to expose the bony surface of the mandible with a width of about 5 to 10 mm (Figure 1C).21,23 The first space was established by blunt separation after injection of 5 ml of expansion solution (1:500,000 epinephrine in normal saline). Attention should be paid to avoid CO2 leakage after central Trocar insertion due to excessively wide incision. The tip of the 10 mm Trocar was placed with the bevel facing up, and when the tip reached the hyoid plane, the Trocar was rotated 180° to make the bevel facing down (Figure 1D). At a distance of 2.5 cm from the midline, the puncture point was separated using a Mosquito-Type Hemostatic forceps, taking care to avoid injury to the mental nerve, two 5 mm Trocar were then inserted. A pneumoperitoneum tube was connected and high-flow CO2 gas was injected, and the pressure was maintained at 6 to 8 mmHg. The Da Vinci robot system was connected, the flap was dissected, and the surgical space was established (Supplemental Video 1). The linea alba cervicalis was severed and the strap muscles were suspended with sutures. A lymphatic tracer (0.3 ml Mitoxantrone Hydrochloride Injection for Tracing, or 0.1 ml Carbon Nanoparticles Suspension Injection) was injected (Supplemental Video 2).

Schematic diagram of the surgical incision. (A) A small transverse incision of 1 to 2 cm in length was made with an electrotome at the midpoint of vestibule. (B) The incision was extended to both ends of the first premolar to expose the mental nerves bilaterally. (C) The mandibular surface was exposed with an electrotome, approximately 5 to 10 mm in width. (D) The trocar was inserted.
The prelaryngeal lymph nodes were dissected (Supplemental Video 3). After severing the thyrothymic ligament and continuing upward until the upper pole was revealed, the upper pole vessels were then severed with an ultrasonic scalpel (Supplemental Video 4). After severing the middle thyroid vein the nerve entry point of the recurrent laryngeal nerve (RLN) was revealed, and the RLN was completely dissected after exposure (Supplemental Video 5). The inferior thyroid artery was severed (Supplemental Video 6) and central lymph node dissection was performed (Supplemental Video 7). Isthmectomy or contralateral thyroidectomy was performed according to the extent of surgery. The surgical specimen was extracted through the observation port, which could be suitably enlarged if the specimen proved too large. The operation area was rinsed with normal saline and drainage tubes were placed in the thyroid surgical bed. 23
TOETVA group
The specific operation steps are the same as the T-TORT group. The operating instruments are ultrasonic scalpel, electrotome, and grasping forceps.
Postoperative Management
Twenty-four hours after surgery ice and headband pressure were applied to the neck and chin skin to relieve swelling and bleeding. An oral liquid diet was started 6 hours after surgery and the drainage tube was removed when the drainage volume was less than 15 ml/day. Postoperative antibiotics were administered intravenously for 1 day to avoid infection. Vocal fold function was examined by laryngoscopy before discharge. Outpatient follow-up was performed at 1-month, 3-months, 6-months, and 1-year postoperatively. The follow-up was up to April 2023.
Observation Indexes and Evaluation Criteria
The observation indexes were as follows: (1) Demographics and clinical characteristics of patients, including sex, age, body mass index (BMI), diameter of the largest tumor (mm), presence of combined Hashimoto’s thyroiditis, extent of surgery, and whether to perform central neck dissection (CND). (2) Surgical data, including operation time, bleeding amount, retrieved and metastatic central lymph nodes. (3) Postoperative data, including postoperative hospital stay, drainage volume on operation day, postoperative day 1 (POD1) and postoperative day 2 (POD2), and the visual analog scale (VAS) score on POD2. The postoperative re-examination results included thyroglobulin (Tg), anti-thyroglobulin antibodies, thyroid stimulating hormone, ultrasonography of the neck operation field, and Neck Computed tomography (CT). A significant rise in Tg and a significant mass or enlarged lymph nodes on ultrasonography/CT were used as indicators of recurrence.24,25 (4) Complications, including transient and permanent RLN palsy, transient and permanent hypoparathyroidism, infection, subcutaneous emphysema, seroma, mental nerve injury, chylous fistula, and bleeding. Transient hypoparathyroidism and RLN palsy were defined as occurring for less than 6 months after surgery. Permanent hypoparathyroidism was defined as subnormal intact parathyroid hormone serum concentrations more than 6 months after the operation, requiring calcium and calcitriol supplementation. Permanent RLN palsy was defined as failure to recover vocal cord function within 6 months. 26
Statistical Analysis
Statistics were analyzed by the SPSS 26.0 package. A propensity score-matched analysis was done using a multivariable logistic regression model. According to clinical experience, there were 7 factors that may affect surgical outcome and postoperative recovery, including sex, age, BMI, presence of Hashimoto’s thyroiditis, tumor size, extent of surgery, and whether to perform CND were selected as covariables. Pairs of patients receiving T-TORT or TOETVA were derived using 1:1 greedy nearest neighbor matching within a propensity score of 0.02. 27 Quantitative data are expressed as mean ± SD, classification data are expressed as n (%). Before propensity score matching (PSM), an independent sample t test was used for quantitative data and a Chi-square test for classification data. After PSM, a paired t test was used for quantitative data and the McNemar test for classification data. Statistical significance was accepted at a P value <.05. With the operation time as the main parameter, we obtained the learning curve by cumulative sum analysis according to the sequence of operation dates. The fitting curve whose R2 is closest to 1 was selected as the best model.
Results
During the study period, 244 eligible patients underwent an endoscopic thyroidectomy and none of the patients required conversion to open thyroidectomy. There were 159 patients in the TOETVA group and 85 patients in the T-TORT group. After PSM, 162 (TOETVA n = 81 and TORT n = 81) patients remained in the study population (Figure 2). There were no significant differences between the 2 groups in terms of sex, age, BMI, presence of Hashimoto’s thyroiditis, tumor size, extent of surgery, or whether to perform CND (Table 1).

Flow chart of inclusion, exclusion, and propensity score matching.
Demographics in T-TORT and TOETVA Before and After PSM.

Abbreviations: CND, central neck dissection; PSM, propensity score matching; T-TORT, three-port in single-incision transoral robotic thyroidectomy; TOETVA, transoral endoscopic thyroidectomy vestibular approach.
In terms of perioperative outcomes (Table 2), compared with TOETVA, the operation time in the T-TORT group was relatively longer (136.14 ± 36.52 minutes vs 122.49 ± 34.85 minutes, P = .012), the postoperative stay was shorter (2.77 ± 0.78 days vs 3.51 ± 0.95 days, P < .001), and POD days 1 and 2 drainage was less (POD1, 56.57 ± 23.29 ml vs 65.12 ± 26.04 ml, P = .029 and POD2, 27.43 ± 25.29 ml vs 38.21 ± 25.09 ml, P = .008). There were no significant differences in terms of bleeding amount, retrieved and metastatic central lymph nodes, VAS, or drainage on the operation day. There was no difference in the incidence of complications between the 2 groups (Table 3). The median follow-up time was 10 months in T-TORT (range 6-21 months) and 15 months in TOETVA (range 6-21 months), no recurrent case was reported in the 2 groups during the follow-up period.
Clinicopathologic, Perioperative Data and Complications in T-TORT and TOETVA Before and After PSM.
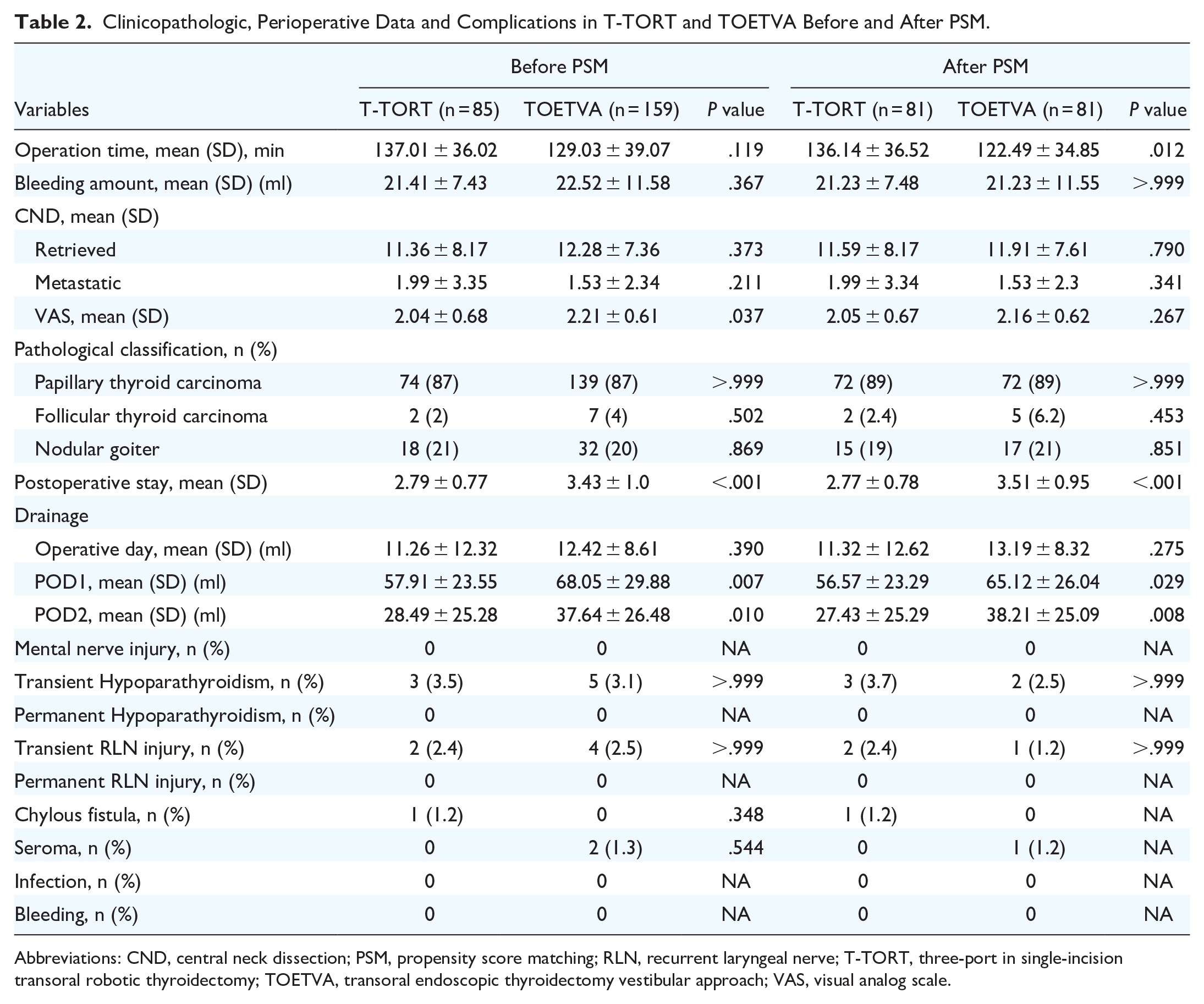
Abbreviations: CND, central neck dissection; PSM, propensity score matching; RLN, recurrent laryngeal nerve; T-TORT, three-port in single-incision transoral robotic thyroidectomy; TOETVA, transoral endoscopic thyroidectomy vestibular approach; VAS, visual analog scale.
Different Studies Comparing Operation Time Between T-TORT, TORT, and TOETVA.

Abbreviations: T-TORT, three-port in single-incision transoral robotic thyroidectomy; TOETVA, transoral endoscopic thyroidectomy vestibular approach.
We used cumulative summation (CUSUM) to analyze the learning curve of 40 consecutive hemithyroidectomy with CND cases and 37 consecutive total thyroidectomies with CND cases in the T-TORT group. Results showed that 16 and 21 cases were needed for the operation time to reach the plateau (Figure 3). Reviewing the scatter plot of the learning curve of total thyroidectomies for 26 patients with CND, as an example, the operation time is gradually shortened with the increase of the number of surgeries (Figure 3C). The learning curve calculated according to CUSUM is shown in Figure 3D. The best fit for the curve was a third-order polynomial with the equation CUSUM equal to −0.034*(Case number) 3 + 0.802*(Case number) 2 + 12.966*(Case number) + 96.987, which had a high R2 value of 0.941. The peak of the fitting curve was the 21st case, indicating that the learning curve for this surgical method was 21 cases. With the peak point as the boundary, the learning curve was divided into 2 phases. Phase 1, the learning period (cases 1-21) was the learning improvement phase, and the CUSUM value continued to rise, indicating that the surgical team was still in the familiar running-in stage. In phase 2, the proficient period (cases 22-37), the CUSUM value decreased gradually, indicating that the surgical team had passed the learning period and the surgical skills were relatively stable. A total of 21 operations were completed to achieve the minimum operation volume of the surgical plateau.
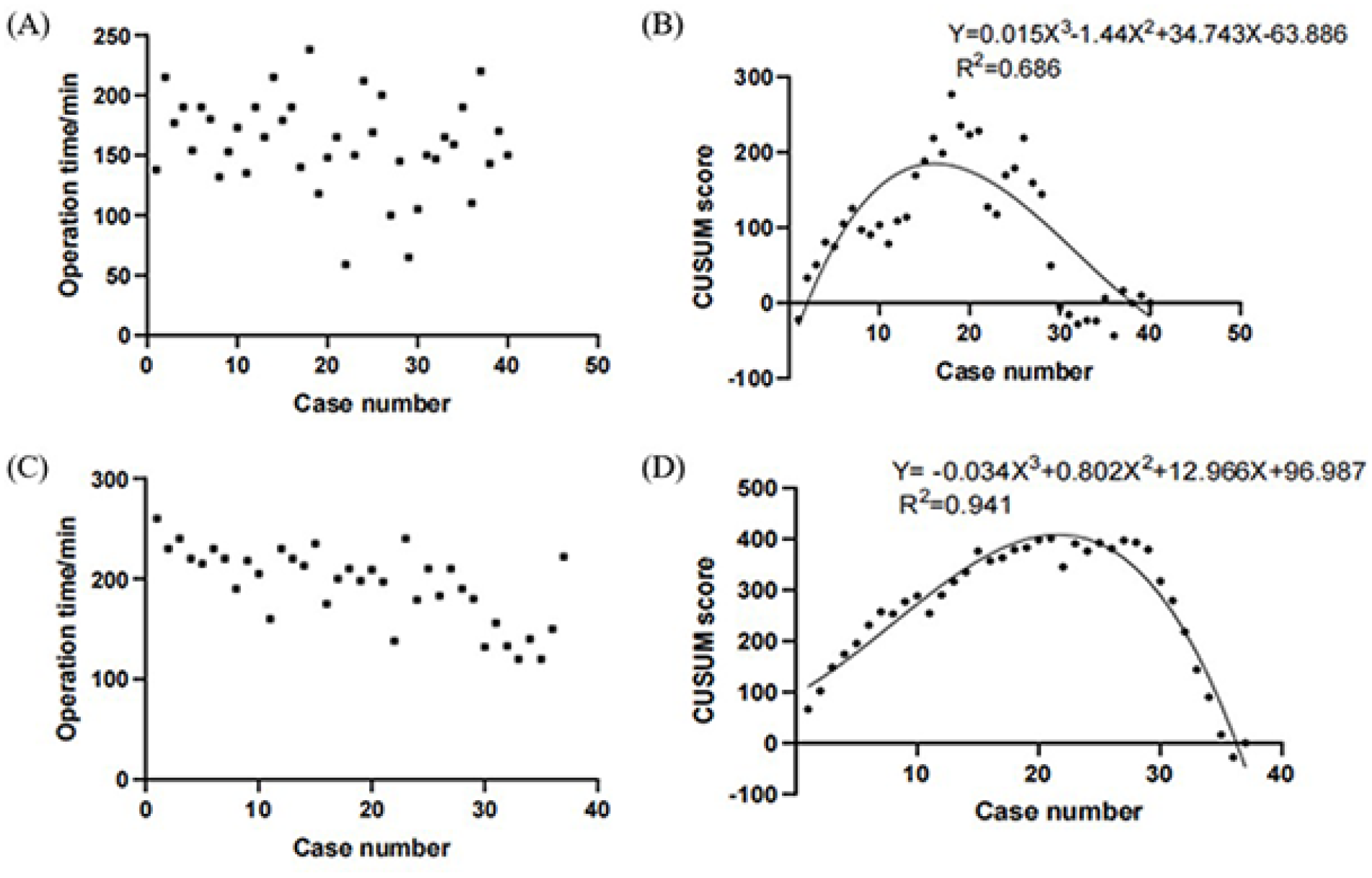
Learning curve analysis. (A) Operation time plotted in chronological order for hemithyroidectomy with CND T-TORT. (B) Cumulative summation test of operation time and fitted curve for hemithyroidectomy with CND T-TORT. (C) Operation time plotted in chronological order for total thyroidectomy with CND T-TORT. (D) Cumulative summation test of operation time and fitted curve for total thyroidectomy with CND T-TORT. CND, central neck dissection; T-TORT, three-port in single-incision transoral robotic thyroidectomy.
Discussion
The literature suggests that T-TORT is superior to TORT in some respects. 17 However, it remains controversial whether T-TORT is superior to conventional transoral microscopic surgery. Therefore, we evaluated T-TORT by comparing it with TOETVA.
The Safety and Feasibility of T-TORT
Operation time is one of the most important indicators to assess the efficiency of an operation. 28 In this study, although there was a statistical difference in operation time between the 2 groups, the difference in mean operation time between them was less than fifteen minutes. Compared to other studies of TORT, the difference in operation time between the T-TORT and TOETVA groups has been significantly reduced (TORT vs TOETVA: 182.33 ± 43.95 minutes vs 158.50 ± 18.42 minutes, P = .035, 16 158.9 minutes vs 106.3 minutes, P < .001, 12 308 [284-388] minutes vs 228 [201-267] minutes, P < .001 29 ) (Table 3). This indicates that the reduction of the transaxillary incision can effectively reduce the operation time, which is consistent with data from another study; TORT versus T-TORT, 166.3 ± 35.4 minutes versus 138.5 ± 34.4 minutes. 17 In addition, we replaced 3 incisions with a single incision in the vestibular area, which made it easier to extract surgical specimens from the vestibular incision and also reduced the operation time. 23 These observations suggest that the operation time may no longer be the major factor to be considered in the clinical promotion of TORT.
Patients with papillary thyroid carcinoma are prone to cervical lymph node metastasis, with an incidence of about 30% to 80%, 30 and thorough central lymph node dissection is helpful to reduce the postoperative recurrence rate. 31 In this study, there were no significant differences in the number of retrieved lymph nodes between the 2 groups. This demonstrates that the T-TORT technique can achieve comparable results to TOETVA in terms of CND. A 2021 study found that the frequency of CND performed was higher with the TORT procedure than with TOETVA. 29 This may indicate that when performing endoscopic CND the surgeon is more willing to choose a robotic platform, this may also be the unique advantage of the robotic system for CND.
For thyroid surgery, the most common complications were RLN injury and hypoparathyroidism.32,33 Multiple meta-analyses have shown that with TOETVA the incidence of temporary hypoparathyroidism ranges from 0.94% to 22.2%, the incidence of permanent hypoparathyroidism ranges from 0% to 2.22%, the incidence of temporary RLN palsy ranges from 1.9% to 8.8%, and the incidence of permanent RLN palsy ranges from 0% to 1.42%.34-36 In the study of Kim et al, 37 only 1 RLN injury occurred in 100 TORT cases and there was no hypoparathyroidism. In 3 comparative studies on TORT and TOETVA, there was no significant difference in the probability of RLN injury or hypoparathyroidism.12,16,29 It is reassuring to see that the incidence of these complications was not different in TORT compared with TOETVA, and even better in some aspects. A study that determined the tonal changes of patients after TORT and thyroidectomy 3 months after surgery 38 showed that the pitch range was wider and the highest frequency of articulation was higher in the TORT group. The conclusion was that TORT can better protect the articulation function compared with conventional thyroidectomy. In our study there were no significant difference was found between T-TORT and TOETVA in terms of transient RLN injury and hypoparathyroidism. Meanwhile, there were no differences in other complications between the 2 groups. The above results provide strong support for the application of T-TORT in clinical practice and confirm its advantages in terms of surgical safety and efficacy.
In addition, According to the American Thyroid Association guidelines 39 and the Chinese Society of Clinical Oncology (CSCO) guidelines 40 we defined a significant increase in thyroglobulin and ultrasonographic findings of a significant mass or enlarged lymph node as indicators of recurrence. In our short-term follow-up, there was no postoperative recurrence in the 2 groups of patients, which proved that both methods had good surgical thoroughness.
The Significance of T-TORT in Enhanced Recovery After Surgery
In recent years, with the emphasis on postoperative rehabilitation, the concept of enhanced recovery after surgery (ERAS) has been gradually applied in the field of thyroid surgery.41-43 In the comparative studies of TORT and TOETVA, it has not been clearly reported that TORT can accelerate postoperative recovery.16,29 In this study, we found that TORT patients seem to have a better recovery. Compared with the TOETVA group the T-TORT group has less postoperative drainage volume and hospital stay. We speculate that it may be related to the following 3 reasons. Firstly, because of the stable shake-filtering robotic arms and high-definition vision, surgeons can sever blood vessels and seal small bleeding sites more accurately. 13 This will reduce the postoperative drainage volume, and less drainage volume means shorter drainage tube indwelling time and inpatient time, especially for Chinese patients who prefer to be discharged after extubation. 44 Interestingly, existing studies suggest that shorter hospital stays may correlate with improved quality of life. 45 The second reason is that there is no additional transaxillary incision. The patient has no postoperative chest wall pain, and postoperative rehabilitation can be performed more quickly. 17 Finally, owing to the flexible multi-angle robotic wrist, the perioral tissues won’t bear too much strain as in a TOETVA procedure that facilitates postoperative eating and recovery. 46
The amount of pain is another indicator of recovery. 47 In this study we found that, although there was no statistical difference in VAS scores between the 2 groups, the mean VAS score was lower in the T-TORT group. Interestingly, before PSM, the VAS scores in the T-TORT group were significantly lower than those in the TOETVA group. This may be the result of a smaller sample due to PSM, and this result needs to be confirmed by further large sample studies. In summary, T-TORT can result in less drainage volume and a shorter postoperative stay, which is of great significance for ERAS.
Learning Curve of T-TORT
Compared with conventional endoscopic surgery, robotic-assisted surgery has some unique difficulties and challenges, the most important of which is the lack of tactile feedback, and it takes more time to replace the robotic arm during the operation.48,49 The robotic-assisted transoral approach is also considered to be more difficult to learn than other remote-access approaches. 50 This results in a long learning curve for the TORT procedure. Two studies have reported a learning curve of 25 cases to reach a plateau for experienced surgeons using TORT.12,29 Another study found that the TORT learning curve was 52 cases in the CUSUM operation time analysis. 51 In this study the learning curve of T-TORT is 16-21 cases, which was not much different from the learning curve of TORT. Based on our clinical experience we have found that intraoperative bleeding is the most critical problem affecting the operation time. This is because the hemostatic device needs to be continually changed. Unlike in endoscopic surgery where surgical instruments can be changed quickly, it takes more time to change surgical instruments during this robotic-assisted surgery. Frequent bleeding will increase the operation time and affect the completion of the learning curve. Therefore, it is necessary to avoid bleeding as much as possible during the operation. This requires making full use of the amplification effect of the robotic system to predict and deal with each blood vessel that may cause bleeding, resulting in a bleed-free surgery for fast and efficient surgical results. This requires a surgeon with extensive experience with endoscopic thyroid surgery and a sufficient knowledge of the anatomy of the thyroid gland. So we recommend extensive experience with TOETVA or TORT as a prerequisite for performing T-TORT.
Prospect and Future of T-TORT
The promotion of the transoral approach is largely due to patients’ demand for beauty. Young females tend to reject having a scar on the neck and breast area. Obvious scars on the neck are even considered “social shame” in some Asian areas. 52 A study showed that Americans were willing to pay an average extra of $10,116 to avoid surgical scars on the neck. 53 All of this reflects the high priority society places on avoiding thyroid surgery scars.
In our study, T-TORT demonstrated shorter postoperative hospital stays and fewer POD, suggesting its advantage in ERAS. However, T-TORT has drawbacks such as longer operation time and higher medical cost. Due to varying regional economies, not all patients can afford the expenses associated with T-TORT. While T-TORT eliminates the cost of an additional robotic arm compared to the conventional TORT, its overall expenses still significantly exceed those of TOETVA, hindering its widespread clinical adoption. We believe that future advancements in robotic platforms and reductions in healthcare costs may facilitate the development and utilization of T-TORT. However, at present, the overall advantages of T-TORT over TOETVA are not particularly evident. Surgeons should exercise caution and conduct thorough evaluations before opting for T-TORT.
There are still some limitations in this study. Firstly, this was a single-center study. Second, the sample size was relatively small and the follow-up period was not long enough. Finally, the cost of T-TORT is typically higher than TOETVA in China, and some expenses may not be covered by medical insurance. Patients in the T-TORT group generally have better economic conditions compared to those in the TOETVA group. Differences in economic status may lead to variations in lifestyle and cognitive factors, potentially introducing some baseline bias between the 2 groups.
Conclusion
In this preliminary study, we validated the safety and feasibility of T-TORT. While T-TORT shows potential advantages in shorter hospital stays and faster recovery, its longer surgical times and higher costs may limit its widespread adoption, particularly in economically constrained regions. Surgeons should carefully evaluate the benefits and drawbacks of each technique, considering individual patient factors. Future research focusing on long-term outcomes and cost-effectiveness will provide further insights into the optimal approach to transoral thyroidectomy.
Footnotes
Acknowledgements
We gratefully acknowledge the writing assistance from Dr. Stephen P. Brooks, the chief science editor for Phoenix Translations of Austin TX, USA.
Authors’ Contributions
Xiaoyong Wen, Conceptualization, Formal analysis, Data Curation, Visualization, Writing – Original Draft. Shiwei Zhou, Conceptualization, Formal analysis, Data Curation, Visualization, Funding acquisition, Writing – Original Draft. Hui Li, Investigation, Data Curation, Validation. Funding acquisition. Peng Wu, Investigation, Resources, Funding acquisition. Wu Li, Investigation, Resources, Funding acquisition. Zhiyuan Wang, Data Curation, Resources. Lu Zhang, Data Curation, Resources. Jigang Li, Data Curation, Resources. Xiaowei Peng, Writing – Reviewing and Editing, Supervision, Project administration.
Consent for Publication
Written informed consent was obtained from the patient for publication and any accompanying images.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author, [Xiaowei Peng], upon reasonable request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Hunan Provincial Natural Science Foundation of China (Grant No. 2023JJ40419, 2023; 2023JJ60331, 2023), Hunan Cancer Hospital Climb Plan (Grant No. ZX2020002, 2020; ZX2021004, 2021; 2020NSFC-B007, 2020), Changsha Municipal Natural Science Foundation (Grant No. kq2208153, 2023) and Scientific Research Project of Hunan Provincial Health Commission (Grant No. 202204015634, 2022).
Ethical Approval and Informed Consent Statements
The study was approved by the Medical Ethics Committee of the Hunan Cancer Hospital (2023, No. 20). All patients agreed to the use of their personal statistics for clinical research and signed an informed consent.
Supplemental Material
Additional supporting information is available in the online version of the article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.