
Abstract
Background
Injury to the recurrent laryngeal nerve (RLN) and parathyroid glands (PGs) are the most common and serious complications during the transoral endoscopic thyroidectomy vestibular approach (TOETVA), and their exposure and protection are the most important factors affecting the operation time. Here, we report a novel anatomical landmark and surgical method to shorten the operative time and reduce the chance of injury to the RLN and PGs.
Methods
According to the different exposure methods of the RLN, patients were divided into the experimental group (from top to bottom, E-group) and the comparison group (from outside to inside, C-group), and 1:1 propensity score-matching (PSM) was performed. The demographics, operative data, postoperative data, and postoperative complications were analyzed by comparing the 2 groups.
Results
After PSM, a total of 206 patients were included. Except for tumor size, there were no significant differences between the 2 groups in terms of sex, age, body mass index, presence of Hashimoto’s thyroiditis, or extent of surgery. Compared with the C-group, the operative time, in minutes, of the E-group was significantly shorter (hemithyroidectomy with central neck dissection (CND), C = 111.81 ± 25.83 vs E = 100.52 ± 16.47, P = .002 and bilateral thyroidectomy with CND, C = 177.87 ± 36.61 vs E = 156.05 ± 25.60, P = .004), the exposure time, in minutes, of the RLN was reduced (hemithyroidectomy with CND, C = 23.31 ± 7.07 vs E = 11.41 ± 2.75, P < .001 and bilateral thyroidectomy with CND, C = 45.64 ± 14.84 vs E = 21.76 ± 5.57, P < .001). The rate of postoperative temporary PGs and RLN injuries were also reduced (transient hypoparathyroidism, C = 13% vs E = 4%, P = .023 and transient RLN palsy, C = 10% vs E = 2%, P = .017). In addition, the remaining parameters such as the amount of bleeding, number of lymph node metastases, postoperative hospital stay, visual analog scale pain score, recurrence rate, and other complication rates were not significantly different between the 2 groups.
Conclusion
It is safe and feasible to construct Thyroid-RLN Entry Triangle (Peng’s Triangle) for PGs and RLN protection in TOETVA. It is beneficial to shorten the operation time and reduce postoperative complications, both worthy of clinical promotion.
Trial Registration
This study was registered at the Chinese Clinical Trial Registry (UIN: ChiCTR2300067673, https://www.chictr.org.cn) in accordance with the World Medical Association’s Declaration of Helsinki, 2013.
Keywords
Introduction
In recent years, with the popularization of the concept of a national health examination, the global incidence rate of thyroid cancer is increasing year by year, and the incidence rate for females remains significantly higher than for males. 1 Surgery is the main way to treat thyroid cancer. However, conventional/open thyroidectomy (ConT) inevitably leads to a visible scar on the neck, which affects the appearance, brings psychological and mental pressure to female patients, and even affects the normal life of some patients. 2 With increasing demand by patients for postoperative aesthetics, endoscopic thyroid surgery is a rapidly developing surgical option. 3 Nakajo et al. and Wang et al. first reported the application of transoral endoscopic thyroidectomy vestibular approach (TOETVA) in 2013.4,5 Its safety and efficacy have been well documented, and the transoral approach is a truly scarless procedure with better cosmetic results and a therapeutic outcome. 6
With the improvement of surgical techniques and the application of new techniques, the incidence of complications in thyroid surgery has been greatly reduced. However, surgical complications, mainly injury of the recurrent laryngeal nerve (RLN) and parathyroid glands (PGs) can still seriously affect the curative effect and bring physical and psychological harm to patients. 7
Recurrent laryngeal nerve injury (RLNI) is one of the major postoperative complications of thyroid surgery that can seriously affect the prognosis of patients. Unilateral RLNI usually leads to impaired vocal function of patients and bilateral RLNI leads to impaired respiratory function, which can be life-threatening in severe cases. 8 Occurence of RLNI may be caused by transection, clamping, ligation, compression, traction, thermal injury, or ischemia. 9 Therefore, protection of the RLN is very important in thyroidectomy.
The PGs play a vital role in calcium regulation and homeostasis and the preservation of the PG during neck surgery is very important to avoid postoperative hypoparathyroidism. 10 It has been reported that patients with permanent hypoparathyroidism have increased morbidity and mortality and a decreased quality of life. 11 Accidental damage to the PG or autotransplantation has been reported in up to 22% of patients undergoing total thyroidectomy. 12 Although there are several guidelines and publications reporting on the protection and management of PGs during thyroidectomy, the intraoperative identification and protection of PGs relies heavily on the subjective determination of the surgeon. 11
In ConT, the RLN is often identified by some common anatomical markers, such as the tracheoesophageal sulcus, the inferior horn tip of the thyroid cartilage, the inferior pole of thyroid, the thyroid suspensory ligament, and so on. 13 However, in TOETVA, there are no appropriate anatomical landmarks to help distinguish the RLN and PG, which is one of the reasons for the long and difficult operation. 14
In this report, we define a new anatomical landmark from which we have developed a new surgical procedure. This study also determined differences in the feasibility and safety of new procedures by comparing demographics, surgical data, postoperative data, and postoperative complications between different surgical procedures.
Materials and Methods
Study Cohort
This was a retrospective cohort study performed at a single tertiary-level academic health care institution. There were 292 patients admitted to our hospital who underwent TOETVA from March 2020 to May 2021 who were recruited in this study. Nine patients with other types of thyroid cancers or benign nodules were excluded, 11 patients were diagnosed with pT2-3 stages and excluded, 7 patients were excluded after being lost to follow-up, and 1 patient was excluded due to anatomic abnormalities of RLN (nonrecurrent). Together, a total of 264 patients with thyroid papillary carcinoma were selected as the study subjects and were divided into an experimental group, the E-group (n = 138), and a comparison group, the C-group (n = 126), according to different RLN exposure methods. The E-group had the upper approach (Thyroid-RLN Entry Triangle (Peng’s Triangle) approach), and the C-group had the lateral approach. All the surgeries were performed by the same surgeon at the Hunan Cancer Hospital, Changsha, China. The study was approved by the Medical Ethics Committee of the Hunan Cancer Hospital and subjects gave informed consent to the work. In addition, this study was registered at the Chinese Clinical Trial Registry (UIN: ChiCTR2300067673, https://www.chictr.org.cn) in accordance with the World Medical Association’s Declaration of Helsinki, 2013. This study was compliant with the STROBE guidelines. 15
The Inclusion and Exclusion Criteria Were as Follows
Inclusion Criteria
Age over 18.
Postoperative pathological diagnosis was differentiated thyroid cancer.
Maximum tumor diameter less than 2.0 cm.
Normal preoperative laryngoscopy findings.
Exclusion Criteria
History of neck surgery or radiotherapy.
Hyperparathyroidism or hypoparathyroidism.
Conversion from endoscopic surgery to open technique.
Tumor invasion of adjacent structures or severe tissue adhesions.
Anatomic abnormalities of the RLN discovered during surgery.
Clinically evident lateral neck lymph node or distant metastasis.
Loss to follow-up or patient withdrawal from the trial.
Surgical Procedure
Preoperative Preparation
Under general anesthesia, the patient was placed in a supine position with arms adducted and fixed in position. The neck was maintained in a slightly overstretched position, and a neurological monitor was placed through the mouth tracheal intubation. A Cefazolin, 2.0 g, infusion was given 30 minutes before the surgery.
Incision Design
Gauze was inserted into the mouth to prevent blood aspiration. The middle line of the inferior labial frenulum was marked with a suture, and the endotracheal tube was fixed to prevent de-tubing. A 5 cm incision in the mucosa was made, beginning at the midpoint of the vestibule 1 to 1.5 cm inferior to the gingival edge, and the mental nerves were exposed bilaterally.16,17
Building the Tunnel
The first space was bluntly separated to the position of the thyroid cartilage using a dissection stick. A 10-mm trocar was placed in the midpoint of the vestibule and two 5 mm trocars were separately inserted into the vestibule lateral or medial to the medial branches of the mental nerve at the level of the first front molar. A 10-mm endoscope was then inserted into the trocar for observation, CO2 was injected, and a constant pressure of 6 to 8 mmHg was maintained. An electric coagulation hook or harmonic scalpel was used to create the second space (working space). The lateral border of the sternocleidomastoid muscle and the superior sternal notch are then fully exposed.
Suspension
The linea alba cervicalis was severed by an electric coagulation hook and the gap between the thyroid and banded muscle separated on the affected side. A lymphatic tracer was injected, and the strap muscles were suspended parallel to the upper margin of the isthmus with sutures and fixed on an all-round hook.
Severing Isthmus and Superior Thyroid
The thyroid isthmus was transected with a harmonic scalpel after dissection of the thyroid gland from the trachea. Part of the sternothyroid muscle was transected to expose the cricothyroid space. The branches of the upper pole vessels are then severed with an ultrasonic scalpel. The upper pole is then completely dislocated (Supplemental Video 1).
Exposure of the RLN and Upper PG
Experimental Group (the Thyroid-RLN Entry Triangle (Peng’s Triangle) Approach)
Elevating the upper pole of the thyroid gland the dorsal margin of the gland formed an arc line (A), which formed a triangular region with the inferior margin line of the cricothyreoideus (B) and the lateral fascial frenulum (C) (Figure 2A). The nerve entry point (NEP) of the RLN is located within a 0.5 cm sector near the intersection between A and B, and the tunnel of the RLN can be easily separated at the intersection by blunt dissection with the separating forceps to locate the NEP of the RLN (Figure 2B). We call this the “Thyroid-RLN Entry Triangle (Peng’s triangle)” (Supplemental Video 2). The signal of the RLN can be detected quickly in this triangle by a neuromonitoring instrument. Then, the tunnel of the RLN is gradually established and expanded with the separating pliers. Under safe conditions (more than 1 mm away from the RLN), 18 the adjacent tissues, including the upper PG on the outside of the tunnel, can be dissected close to the thyroid capsule with an ultrasonic scalpel (Supplemental Videos 3 and 4).
Almost all of the upper PG can be preserved in situ.
Comparison Group (the Lateral Approach)
After severing the upper pole of the thyroid gland, the middle thyroid vein was dissected to expose the common carotid artery. Between the common carotid artery and the thyroid gland, the tissue fascia on the lateral side of the thyroid gland was gradually separated and dissected from the outside to the inside with the separating forceps, and the inferior thyroid artery was dissected. The location of the RLN was explored with the assistance of a neuromonitor. Surrounding fascia was sequentially dissected, and the inferior thyroid artery was ligated. The RLN was dissected upwards along the tracheoesophageal groove until the NEP was exposed. The gland was pulled to the contralateral side, and then the RLN was moved laterally. The berry ligament was severed under safe conditions. Attention was paid to identifying and protecting the upper PG during the whole operation.
Protect the Inferior PG
The inferior PG was preserved by dissecting along the RLN tunnel with attention to the blood supply of the inferior arterial branches.
Central Neck Dissection
According to the scope of central neck dissection the prelaryngeal lymph nodes, pretracheal lymph nodes, and paratracheal lymph nodes will be cleaned. The lower border is the suprasternal fossa (superior border of the innominate artery), the outer border is the common carotid artery, and the inner border is the medial trachea. 19
Closure
The operation site is then flushed and then checked for bleeding. The drainage tube is placed, the vestibular incision sutured, and a local pressure dressing performed. 16
Postoperative Management
Twenty-four hours after surgery ice and headband pressure were applied to the neck and chin skin to relieve swelling and bleeding. Perioperative antibiotics were administered intravenously for 24 hours to avoid infection. An oral liquid diet was started 6 hours after surgery and the drainage tube was removed when the volume was less than 15 ml/day. The vocal fold function was examined by laryngoscopy before discharge. Outpatient follow-up was performed at 1-month, 3-months, 6-months, and 1 year postoperatively. Patients with hoarseness were assessed for vocal fold function with laryngoscopy. Voice disorder assessment and laryngoscopy were performed by an ENT doctor. If patients develop hoarseness, we recommended them to the Voice Training and Rehabilitation Department for vocal rehabilitation treatment.
Observation Indexes and Evaluation Criteria
The observation indexes were as follows: (1) Demographic and clinical characteristics of patients, including age, sex, body mass index (BMI), presence of combined thyroiditis, diameter of the largest tumor (mm), and extent of surgery. (2) Surgical data, including intraoperative blood loss, number of lymph nodes dissected and metastases, operation time, and exposure time of the RLN (defined as the time from dissection of the superior thyroid artery to the endoscopic exposure of the RLN). (3) Postoperative data, including the postoperative visual analog scale (VAS), postoperative drainage volume, postoperative hospital stay, and recurrence. The postoperative re-examination results included thyroglobulin (Tg), anti-Tg antibodies, thyroid stimulating hormone, ultrasonography of the neck operation field, etc. A significant rise in Tg and a significant mass or enlarged lymph nodes on ultrasonography were used as indicators of recurrence. 20 (4) Complications included transient and permanent RLN palsy, transient and permanent hypoparathyroidism, infection, seroma, subcutaneous emphysema, mental nerve injury, chylous fistula, and bleeding. Clinical hypoparathyroidism was defined as biochemical hypoparathyroidism that is accompanied by symptoms and/or signs of hypocalcemia. 11 Transient hypoparathyroidism and RLN palsy were defined as occurring for less than 6 months after surgery. Permanent hypoparathyroidism was defined as subnormal intact parathyroid hormone serum concentrations more than 6 months after the operation, requiring calcium and calcitriol supplementation. Permanent RLN palsy was defined as failure to recover vocal cord function within 6 months. 21
Statistical Analysis
All data were statistically analyzed using SPSS 25.0 software (IBM SPSS Statistics 25 software (Armonk, NY: IBM Corp.)). Propensity score-matching (PSM) was performed to reduce patient selection bias and to adjust for differences in baseline clinical characteristics. Propensity values were calculated by establishing a logistic regression analysis model, in which demographics and clinical characteristics were the predictors in a model of the odds of being allocated to either the E-group or the C-group. According to our clinical experience, 6 factors that may affect surgical outcome and postoperative recovery, including patient sex, age, BMI, presence of Hashimoto’s thyroiditis, tumor size, and extent of surgery were selected as covariates. After including all the above variables, we performed 1:1 PSM using the nearest neighbor method with a caliper width of 0.05 of the standard deviations of the logit of the propensity score. The standardized mean difference (SMD) was used to report the balancing before and after PSM. Differences between groups were compared using the Student’s t-test for numeric parameters and the Chi-squared test for non-numeric parameters. Statistical significance was accepted at a P value <.05 or SMD <0.1. 22
Results
Demographics and Clinical Characteristics
During the study period, 264 eligible patients underwent a hemithyroidectomy/bilateral thyroidectomy and central neck dissection and none of the patients required conversion to open thyroidectomy. There were 126 patients in the C-group and 138 patients in the E-group. After PSM, 206 (C-group n = 103 and E-group n = 103) patients remained in the study population (Figure 1), and the 2 groups were well balanced in terms of the 6 covariates. Patient demographics and clinical characteristics are summarized in Table 1. After PSM, except for diameter of the largest tumor (mm) with an SMD = 0.13, there were no significant differences observed between the 2 groups in terms of sex, age, BMI, presence of combined thyroiditis, and extent of surgery (Table 1).

Trial flow diagram of propensity score-matching.
Demographics and Clinical Characteristics from the C and E Groups Before and After PSM.

Abbreviations: BMI, body mass index; CND, central neck dissection; PSM, propensity score-matching; SD, standard deviation; SMD, standardized mean difference.
Surgical Data
Table 2 shows the surgical characteristics. There was no significant difference in the amount of bleeding between groups. However, the operation time and RLN exposure time were considerably shorter in the E-group than in the C-group. In addition, the number of retrieved central lymph nodes was greater in the E-group than in the C-group, but the number of metastatic lymph nodes did not differ significantly between the 2 groups (Table 2).
Surgical Data from the C-Group and the E-Group Before and After PSM.

Abbreviations: CND, central neck dissection; PSM, propensity score-matching; RLN, recurrent laryngeal nerve; SD, standard deviation.
Postoperative Data
Table 3 summarizes the postoperative-related indicators of the patients. There were no significant differences in VAS, postoperative drainage volume, or postoperative hospital stay between the 2 groups, and no recurrence occurred in either group (Table 3).
Postoperative Data and Related Complications from the C-Group and the E-Group Before and After PSM.
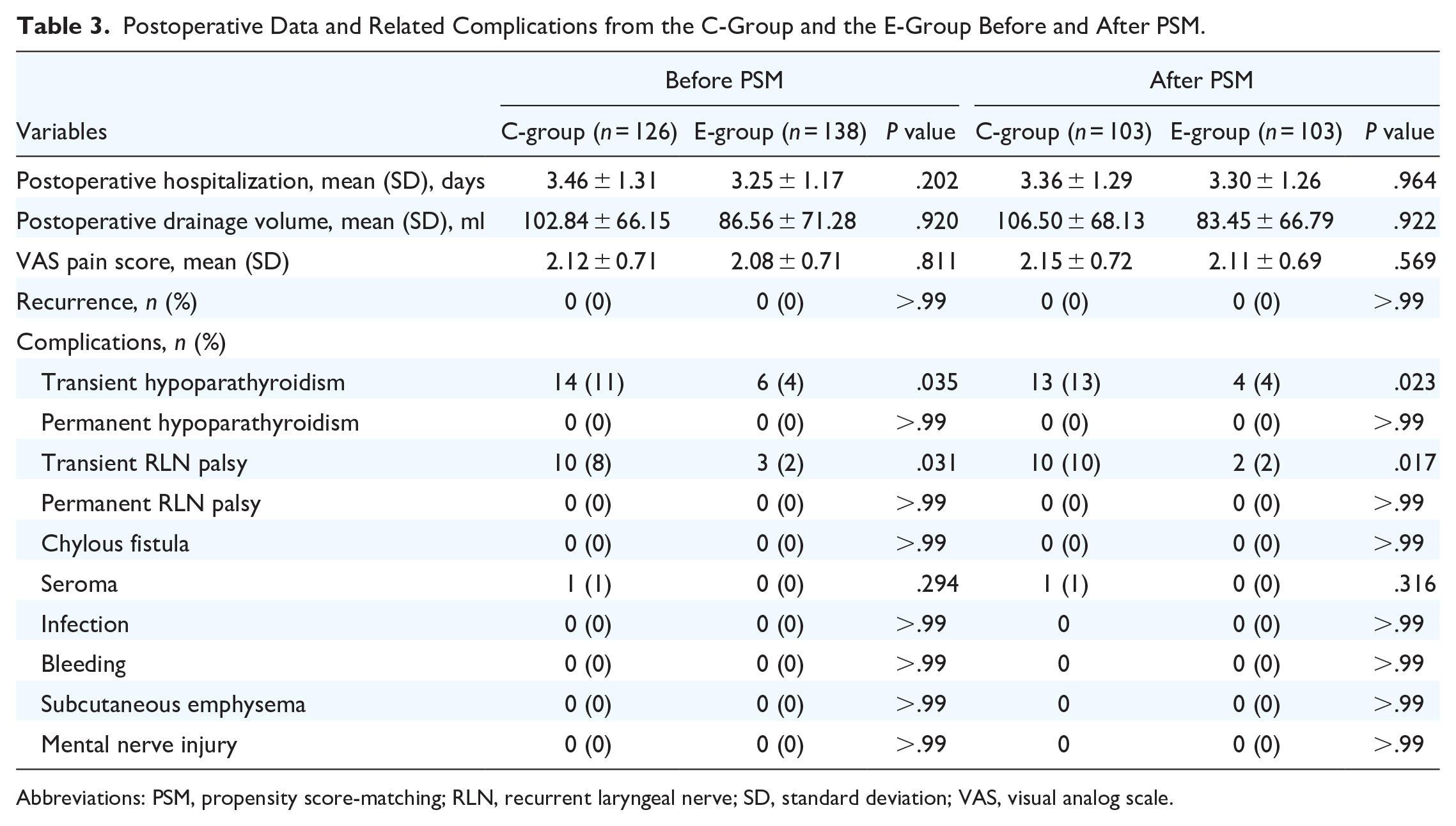
Abbreviations: PSM, propensity score-matching; RLN, recurrent laryngeal nerve; SD, standard deviation; VAS, visual analog scale.
Complications
Postoperative complications are shown in Table 3. The overall complication rate included transient and permanent RLN palsy, transient and permanent hypoparathyroidism, infection, seroma, subcutaneous emphysema, mental nerve injury, chylous fistula, and bleeding. There was no permanent RLN palsy or hypoparathyroidism in any of the patients. The rate of transient RLN palsy and hypoparathyroidism in the E-group was significantly lower than in the C-group. There was no significant difference in the incidence of other complications between the 2 groups (Table 3).
Discussion
TOETVA is more in line with the principle of natural orifice transluminal endoscopic surgery, it has the advantage of better visualization, better surgical completeness, and no scarring on the body surface after surgery. 23 However, due to the visual field and operation direction, the operation is difficult and the operation time is long, which seriously affects the popularization and application of this operation. 23 To solve the above problems many surgeons have been optimizing the original procedure.24-26 All of these improvements are intended to reduce the difficulty of surgery, shorten the operation time, and decrease the incidence of surgical complications. In the current study, we report a new anatomical landmark and compared the safety, thoroughness, and feasibility of different surgical procedures for TOETVA.
When a new surgical procedure is adopted the most important thing is to evaluate its safety and feasibility. 27 The RLN is a critical nerve that provides motor function to the muscles of the larynx, including the vocal cords. Any damage to this nerve can result in vocal cord paralysis, which can cause hoarseness, difficulty speaking, and in severe cases, difficulty breathing. 28 To minimize the risk of RLN injury during thyroid surgery, several preventive measures have been developed. These include visual identification and dissection of the RLN, intraoperative nerve monitoring, and the use of neuromuscular blocking agents to reduce the stress on the RLN during surgery. 29 Additionally, the use of transcutaneous laryngeal ultrasonography or electronic laryngoscope before and after surgery to monitor the changes in the patient’s vocal cords may also help doctors to diagnose and treat in a timely manner. 30
Similarly, the exposure and protection of the RLN is also one of the difficulties in TOETVA, 31 although many studies have shown that there is no significant difference in the rate of RLNI in TOETVA compared with ConT.21,32-34 Due to the top-down surgical perspective, the traditional anatomical landmarks used in ConT may not be as applicable, leading surgeons to often opt for a top-to-bottom approach in RLN dissection. 35 However, current practices heavily rely on individual surgeon experience, lacking standardized guidelines for this procedure.
The NEP of the RLN serves as a pivotal landmark for RLN identification during thyroid surgery, positioned at its apex. Considering the top-down surgical perspective of TOETVA, prioritizing the exposure of this entry point may be particularly advantageous for TOETVA procedures. Currently, anatomical references utilized for nerve localization encompass the superior PG and the thyroid cartilage. During TOETVA procedures, reliance is primarily on the superior PG for localization. However, due to the anatomical classification of the superior PG, its position in relation to the RLN was not constant. 36 Through initial autopsy studies (Figure 3) and subsequent clinical surgical studies, we have consistently observed that the NEP is located within a triangular region formed by the dorsal margin of the thyroid gland, inferior margin line of the cricothyreoideus, and the lateral fascial frenulum, facilitating identification through blunt dissection (Figure 2). We have denominated this region as “Thyroid-RLN Entry Triangle (Peng’s Triangle).” In this study, we found that establishing “Peng’s triangle” followed by RLN exposure markedly enhanced the precision and efficiency of RLN dissection, consequently reducing operative and exposure durations (Table 2).

The schematic diagram. (A) The construction of “Thyroid-RLN Entry Triangle (Peng’s Triangle).” (B) The location of the NEP of the RLN. NEP, nerve entry point; RLN, recurrent laryngeal nerve.

Anatomical study of “Thyroid-RLN Entry Triangle (Peng’s Triangle).” (A) Lifting the upper pole of the thyroid gland. (B) Constructing “Thyroid-RLN Entry Triangle (Peng’s Triangle).” (C) The NEP of the RLN. NEP, nerve entry point; RLN, recurrent laryngeal nerve.
Studies have shown that the most important complications of TOETVA are hypoparathyroidism and RLN injury. 37 Multiple meta-analyses have shown that the incidence of temporary hypoparathyroidism ranges from 0.94% to 22.2%, the incidence of permanent hypoparathyroidism ranges from 0 to 2.22%, the incidence of temporary RLN palsy ranges from 1.9% to 8.8%, and the incidence of permanent RLN palsy ranges from 0 to 1.42%.34,38,39 In our study, there was no permanent PG or RLN injury with either procedure. Compared with the lateral approach, the rate of temporary PG injury and RLN injury rate in the E-group were significantly lower because the construction of “Peng’s triangle” could preferentially expose the NEP of the RLN and the superior PG. This indicates that the surgical method had an excellent protective effect on the PG and RLN. Notably, during the learning stage, some cases of permanent serious complications were reported in 2020, 17 but with the improvement of technology, the incidence of complications gradually decreased. In this study, intraoperative neuromonitoring was performed for all patients, which may be the major reason why neither group of patients developed permanent PG or RLN injury.
There were no significant differences in the 2 groups of patients in terms of the amount of intraoperative bleeding, postoperative hospitalization, postoperative VAS, postoperative drainage volume, and postoperative recurrence because the 2 surgical methods differed only in the exposure of the PG and the RLN. Likewise, there was no significant difference in other complications such as wound infection, hematoma, or chylous fistula. Benefiting from the exposure of the mental nerve during the operation, there was no mental nerve injury in either group. 17 In addition, in this study, more central cervical lymph nodes (CCLN) were dissected in the E-group because the project team updated the detection method of the CCLN. In the E-group, the central CCLN specimens were separated 1 by 1 after removal, while in the C-group, the CCLN specimens were not processed in this way.
There are still some limitations to our study. First, this was a retrospective cohort study. Although PSM was performed to reduce selection bias/confounding by indication, patient selection bias and confounding differences still existed between the 2 groups and there were relatively few cases. Furthermore, the assessment of postoperative RLNI relies on postoperative laryngoscopy. However, a small number of patients with normal voices declined postoperative laryngoscopy due to cost or personal preference. Although these patients did not report hoarseness or other related symptoms during follow-up, the lack of exact data from laryngoscopy precludes the exclusion of potential RLNI. In addition, we did not perform a professional assessment of the patient’s respiratory and swallowing functions, which may lead to an underestimation of RLN injury. 40 Finally, follow-up was relatively short to observe long-term tumor recurrence after surgery.
Conclusions
In this study, we found that the use of the “Thyroid-RLN Entry Triangle (Peng’s Triangle)” as an anatomical marker largely solved the problem of exposing the PG and RLN during TOETVA, significantly reduced the difficulty of the operation, shortened the operation time, and decreased the complication rate, all of which are worthy of clinical promotion. However, to rigorously establish its safety and comprehensiveness, a large-scale, prospective trial with extended follow-up is necessary.
Footnotes
Acknowledgements
We gratefully acknowledge the valuable advice and kind help regarding anatomy from Professor Aihua Pan, Department of Anatomy and Neurobiology, Central South University Xiangya School of Medicine. We gratefully acknowledge the writing assistance from Dr. Stephen P. Brooks, the chief science editor for Phoenix Translations of Austin TX, USA.
Author Contributions
Shiwei Zhou, Conceptualization, Formal analysis, Data Curation, Visualization, Writing – Original Draft, Funding acquisition. Hui Li, Investigation, Data Curation, Validation. Peng Wu, Investigation, Resources, Funding acquisition. Wu Li, Investigation, Resources, Funding acquisition. Zhiyuan Wang, Data Curation, Resources. Lu Zhang, Data Curation, Resources. Jigang Li, Data Curation, Resources. Xiaowei Peng, Writing – Reviewing and Editing, Supervision, Funding acquisition, Project administration.
Availability of Data and Materials
The data that support the findings of this study are available from the corresponding author, [Xiaowei Peng], upon reasonable request.
Consent for Publication
Written informed consent was obtained from the patient for publication and any accompanying images.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the science and technology innovation of Program of Hunan Province (Grant No. 2020SK51107, 2020), Hunan Provincial Natural Science Foundation of China (Grant No. 2023JJ40419, 2023; 2023JJ60331, 2023), Hunan Cancer Hospital Climb Plan (Grant No. ZX2020002, 2020; ZX2021004, 2021; 2020NSFC-B007, 2020), Changsha Municipal Natural Science Foundation (Grant No. kq2208153, 2023) and Scientific Research Project of Hunan Provincial Health Commission (Grant No. 202204015634, 2022).
Ethics Approval and Consent to Participate
The study was approved by the Medical Ethics Committee of the Hunan Cancer Hospital (2022, No. 119). In addition, this study was registered at the Chinese Clinical Trial Registry (UIN: ChiCTR2300067673, ![]() ) in accordance with the World Medical Association’s Declaration of Helsinki, 2013. This study was compliant with the STROBE guidelines.
15
All patients agreed to the use of their personal statistics for clinical research and signed an informed consent.
) in accordance with the World Medical Association’s Declaration of Helsinki, 2013. This study was compliant with the STROBE guidelines.
15
All patients agreed to the use of their personal statistics for clinical research and signed an informed consent.
Supplemental Material
Additional supporting information is available in the online version of the article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.