
Abstract
Objectives
The recurrence rate of T4a papillary thyroid cancer (PTC) is relatively high, but research on the prognosis of T4a PTC is rarely investigated. This study aims to analyze the prognosis of T4a PTC patients with recurrent laryngeal nerve (RLN) invasion.
Methods
Univariable and multivariable Cox proportional hazard models were employed to identify prognostic factors for the progression-free-survival (PFS) of PTC patients. A nomogram was constructed based on essential prognostic factors to predict the risk of disease progression in T4a PTC patients with RLN invasion.
Results
A total of 418/602 (69.4%) T4a PTC patients with RLN invasion underwent surgery, the 5-year PFS rate was 89.8%. The multivariable analyses showed that age ≥55 years, preoperative vocal cord paralysis (VCP), microvascular invasion, and the number of cervical lymph node metastases (CLNM) >10 were prognostic risk factors of PFS in T4a PTC patients with RLN invasion. Our nomogram provided good discrimination, with a C-index of 0.778 in the training set and 0.793 in the validation set. No statistical difference (P = .918) was found between PFS and the surgical methods of RLN. By following up on the patient’s voice condition, the RLN function was restored in approximately 82.7% of patients after RLN separation.
Conclusion
T4a PTC patients with RLN invasion are prone to disease progression under the following conditions: age ≥55 years old, preoperative VCP, microvascular invasion, and CLNM >10. The RLN nerve preservation surgery does not increase the risk of disease progression.

Introduction
Thyroid cancer is a common malignant tumor within the endocrine system, with papillary thyroid cancer (PTC) being the most prevalent type of thyroid neoplasm. Generally, individuals diagnosed with PTC carry a good overall prognosis; however, 10% to 15% of PTC cases are locally advanced, leading to a high risk of recurrence in the local region, distant metastasis, and mortality.1-4 According to the AJCC eighth edition staging system, T4a cancer is defined as the extrathyroidal extension (ETE) into the subcutaneous soft tissue, larynx, trachea, esophagus, or recurrent laryngeal nerve (RLN). 5 Patients diagnosed with T4a PTC tend to have a poor prognosis. Previous studies show that the 10-year disease-specific survival (DSS) rate for T4a PTC patients aged ≥ 55 years ranges between 60% and 70%. 5 Additionally, the 10-year recurrence rate in T4a PTC patients is approximately 29.9%. 6
The RLN is the most frequently invaded in T4a PTC patients. 7 However, the surgical procedure in the RLN region is a complicated and challenging technique. Preserving nerves during surgery may result in residual tumors, whereas complete resection of tumors may lead to vocal cord dysfunction, and even difficulty breathing, which significantly affects the quality of life of the patient. 8 Therefore, it is necessary to establish a predictive model for the prognosis in T4a PTC patients with RLN invasion. This model will facilitate early diagnosis and treatment and ultimately play a pivotal role in optimizing treatment strategies and improving the overall health of patients.
Patients and Methods
Patients
A consecutive cohort study of patients with T4a PTC at the China National Cancer Center(CNCC)/Cancer Hospital Chinese Academy of Medical Sciences between January 2010 and December 2022 was retrospectively recruited. The following were the inclusion criteria: (1) All patients had pathologically confirmed PTC and received surgery; (2) patients had T4a disease; (3) patients pathologically confirmed RLN invasion. The following were the exclusion criteria: (1) synchronous distant metastases. (2) incomplete clinicopathological information or lost to follow-up. A total of 418 patients with T4a PTC with RLN invasion were ultimately included (Supplemental Figure 1). The ethics committee of the CNCC has approved the study and written consent was obtained from all patients (Figure 1).
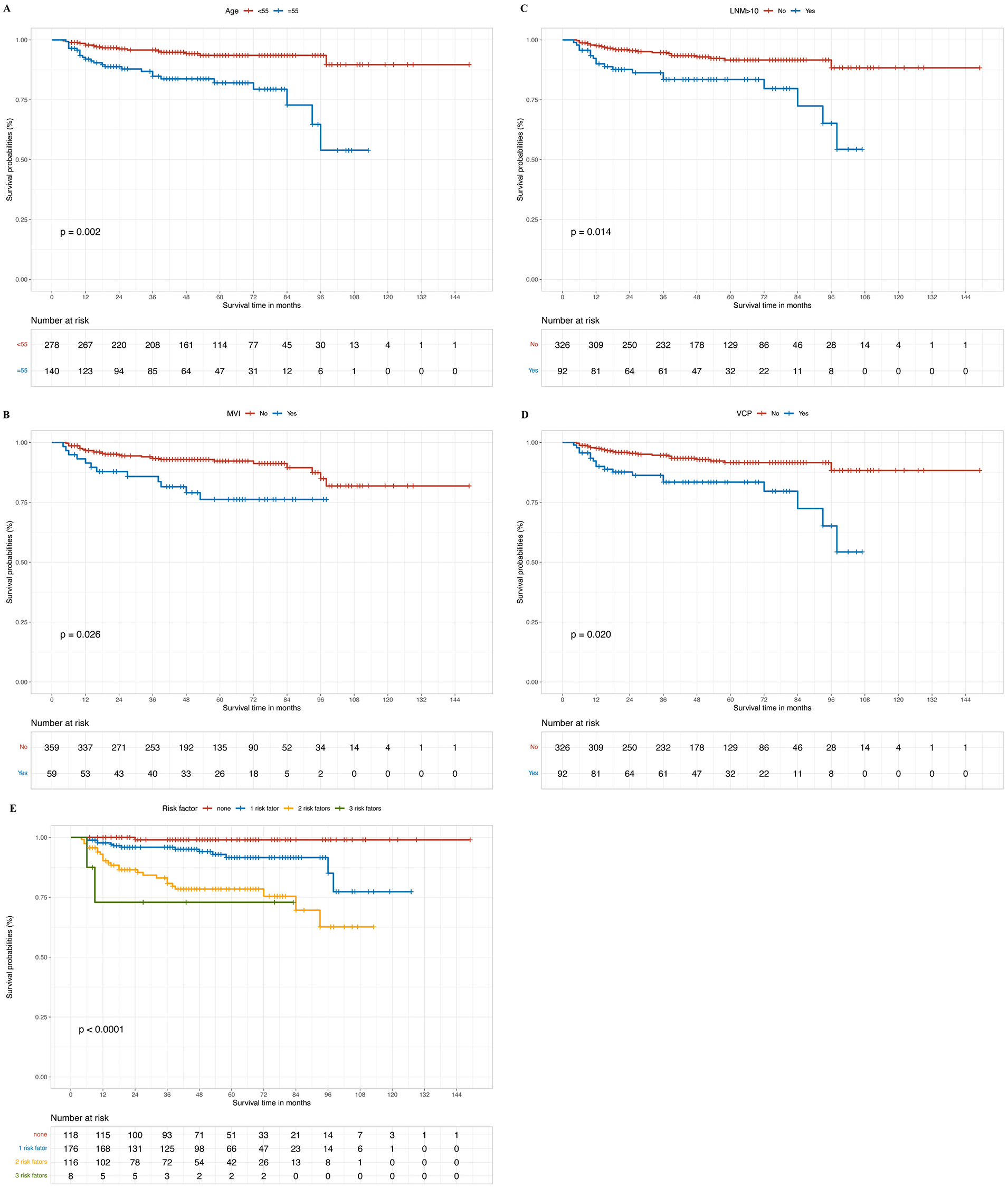
Kaplan–Meier estimates of disease-free survival according to (A) age (B) MVI (C) number of CLNM >10 (D) preoperative VCP (E) different risk factors. MVI, microvascular invasion; CLNM, cervical lymph node metastases; VCP, vocal cord paralysis.
Methods
Clinicopathologic characteristics of all patients were recorded and analyzed, including age, sex, preoperative vocal cord condition, primary tumor size, RLN invasion location, surgical methods of RLN, trachea/esophagus/larynx invasion, N stage, tumor characteristics (multifocality/extracapsular spread), exist Hashimoto thyroiditis/nodular goiter, pathology, microvascular invasion, thyroid surgery method, lymph node dissection method, postoperative radiotherapy, and received radioactive iodine (RAI). Histopathological slides for each case were reviewed by two pathologists from our institution. All of the specimens were assessed for diagnosis using the AJCC eighth edition criteria for PTC classification. Microvascular invasion, also known as microvascular tumor thrombus, mainly refers to nests of cancer cells seen under a microscope in the lumen of blood vessels lined by endothelial cells. RLN invasion is defined as the tumor’s slight invasion or adherence to the epineurium. The tumor tissue and epineurium are delicately separated from the nerve in such cases. Pathological biopsy confirms infiltration of the epineurium by papillary thyroid carcinoma. Alternatively, during surgery, if it is observed that the tumor completely envelops the nerve and separation is not possible, the affected nerve is sacrificed and removed along with the tumor. Pathology examination subsequently confirms the tumor’s invasion of the nerve.
Outcomes and Follow-Up
The primary outcome isprogression-free-survival (PFS) defined as the period from primary surgery to the date of local recurrence or distant metastasis disease during the follow-up time. Local recurrence was confirmed by puncture pathology or after surgery, and distant metastasis was verified by nuclear bone scan, magnetic resonance imaging, or computed tomography. Follow-up was performed according to National Comprehensive Cancer Network recommended schemes and included postoperative outpatient or telephone interviews. The last follow-up date was the date of death or April 10, 2023, whichever came first.
Statistical Analysis
To investigate the impact of various variables on PFS, we utilized univariable and multivariable Cox proportional hazard models. Statistically significant factors (P < .05) identified by univariate analysis were included in the multivariate analysis. A nomogram for predicting PFS was drawn based on the independent predictors identified by multivariate Cox regression analysis. All 418 patients were divided into training and test sets in a ratio of 7:3 (Supplemental Figure 1). The Cox regression analysis was employed to generate hazard ratios (HR) and their associated 95% confidence intervals (95% CIs). The significance level was set at P < .05. R software version 4.3.1 was used for Cox regression analysis and construction and evaluation of the nomogram. The bootstrap method was used for internal and external validation to evaluate the prediction model’s performance. The bootstrap-corrected PFS rates were calculated by averaging the Kaplan‒Meier estimates based on 2000 bootstrap samples. Discrimination was estimated by Harrell’s concordance index (C-index = 0.5-1). The calibration curve mainly reflected the consistency between the predicted risk of the model and the observed risk. All statistical tests were 2-sided in all results, and P-values <.05 were considered statistically significant.
Results
Patient Characteristics
A total of 418 T4a PTC patients with RLN invasion were enrolled. The clinicopathologic features of the patients are summarized in Table 1. There were 158 (37.8%) male patients, 140 (33.5%) aged ≥55 years, 62 (14.8%) patients with a primary tumor size ≥4 cm, and 92 (22.0%) patients with preoperative vocal cord paralysis (VCP). In 177 (42.3%) patients, the site where the primary tumor invaded the RLN was the larynx entry point. Notably, tracheal invasion was observed in 144 (34.4%) patients, esophageal invasion in 141 (33.7%) patients, laryngeal invasion in 13 (3.1%) patients, and microvascular invasion in 59 (14.1%). Multifocality tumors were observed in 238 (56.9%) patients. There were 73 (17.5%) and 291 (69.6%) patients with Hashimoto thyroiditis and nodular goiter, respectively. According to the pathological classification, classic, follicular, diffuse sclerosing, clear cell, solid, tall cell, oncocytic, and mixed PTC were observed in 266 (63.6%), 34 (8.1%), 6 (1.4%), 2 (0.5%), 100 (23.9%), 1 (0.2%), 4 (1.0%), 5 (1.2%) patients, respectively. In terms of N staging of recurrent tumors, 52 (12.4%) patients were classified as N0, 104 (24.9%) patients as N1a, and 257 (61.5%) patients as N1b.
Clinical and Pathologic Characteristics of All T4a PTC Patients with RLN Invasion.

Abbreviations: PTC, papillary thyroid cancer; RAI, radioactive iodine; RLN, recurrent laryngeal nerve.
The median follow-up time was 52 months. By the end of the follow-up period, disease progression occurred in 41 (9.8%) patients, including 34 cases of local recurrence and 11 cases of distant metastasis. Among patients with local recurrence, recurrence in lateral cervical lymph nodes was found in 16 patients, recurrence in the surgical bed in 13 patients, and recurrence in the upper mediastinum in 5 patients. The lung was the most common metastatic organ, with lung metastases in 9 patients and bone metastases in 5 patients.
Predictive Factors for PFS
According to univariable analysis, PFS was highly correlated with the following factors: age (HR = 3.790, 95% CI: 1.973-6.974, P < .0001), primary tumor size (HR = 3.660, 95% CI: 1.934-6.927, P < .0001), preoperative VCP (HR = 2.960, 95% CI: 1.597-5.486, P = .001), surgical methods of RLN (HR = 2.007, 95% CI: 1.061-3.795, P = .032), laryngeal entry point invasion (HR = 0.394, 95% CI: 0.188-0.826, P = .014), tracheal invasion (HR = 3.407, 95% CI: 1.816-6.389, P < .0001), esophageal invasion (HR = 1.917, 95% CI: 1.039-3.539, P = .037), laryngeal invasion (HR = 4.061, 95% CI: 1.592-10.359, P = .003), microvascular invasion (HR = 2.781, 95% CI: 1.413-5.473, P = .003), number of cervical lymph node metastases (CLNM) >10 (HR = 1.978, 95% CI: 1.070-3.655, P = .030), and postoperative RAI (HR = 3.035, 95% CI: 1.345-6.848, P = .007) (Table 2). Based on the multivariable Cox analysis, factors such as age ≥55 years, preoperative VCP, microvascular invasion, and number of CLNM >10 were independent risk factors for PFS. Specifically, patients with age ≥55 years (HR = 3.191, 95% CI: 1.553-6.558, P = .002), preoperative VCP (HR = 2.337, 95% CI: 1.141-4.783, P = .020), presence of microvascular invasion (HR = 2.318, 95% CI: 1.104-4.866, P = .026), and CLNM >10 (HR = 2.480, 95% CI: 1.204-5.108, P = .014) were more likely to experience disease progression.
Cox Univariable and Multivariable Analysis for Progression-Free-Survival.

Abbreviations: CI, confidence interval; HR, hazard ratio; RAI, radioactive iodine; RLN, recurrent laryngeal nerve.
Oncological Outcomes
The 5-year cumulative PFS rate of all T4a PTC patients with RLN invasion was 89.8%. The median interval between surgery and disease progression was 50 months (range: 4-149 months). The 5-year PFS rate was 93.5% in patients under 55 years and 82.1% in older patients (Figure 1A). The 5-year cumulative PFS rates in patients with preoperative VCP and microvascular invasion were 83.4% and 76.2%, respectively (Figure 1B and D). In addition, Kaplan–Meier analysis showed that patients with CLNM >10 had a worse prognosis. Additionally, the 5-year PFS rate for patients with more than 10 CLNM was 84.4%, whereas the PFS rate in patients with less than or equal to 10 CLNM was 93.1% (Figure 1C). Additionally, the 5-year PFS rates in patients with no risk, 1 risk factor, 2 risk factors, and 3 risk factors were 99.0%, 91.6%, 78.4%, and 72.9%, respectively (HR = 3.116, 95% CI: 1.977-4.919, P < .0001) (Figure 1E).
Nomogram Construction and Validation
All 418 patients were divided into training and test sets in a ratio of 7:3 (Supplemental Figure 1). The prognostic nomogram for T4a PTC patients was created in the training set, which was then validated in the testing set. Nomogram models were developed by incorporating several factors, including age, preoperative VCP, microvascular invasion, and number of CLNM >10 to predict the risk of disease progression in T4a PTC patients with RLN invasion in 2 sets (Figure 2). Harrell’s C-index of the model in the prediction of disease progression in the training set and validation set were 0.778 (95% CI: 0.700-0.857) and 0.793 (95% CI: 0.654-0.933), respectively. The calibration plots showed good consistency between the actual and nomogram-predicted PFS (Figure 3).
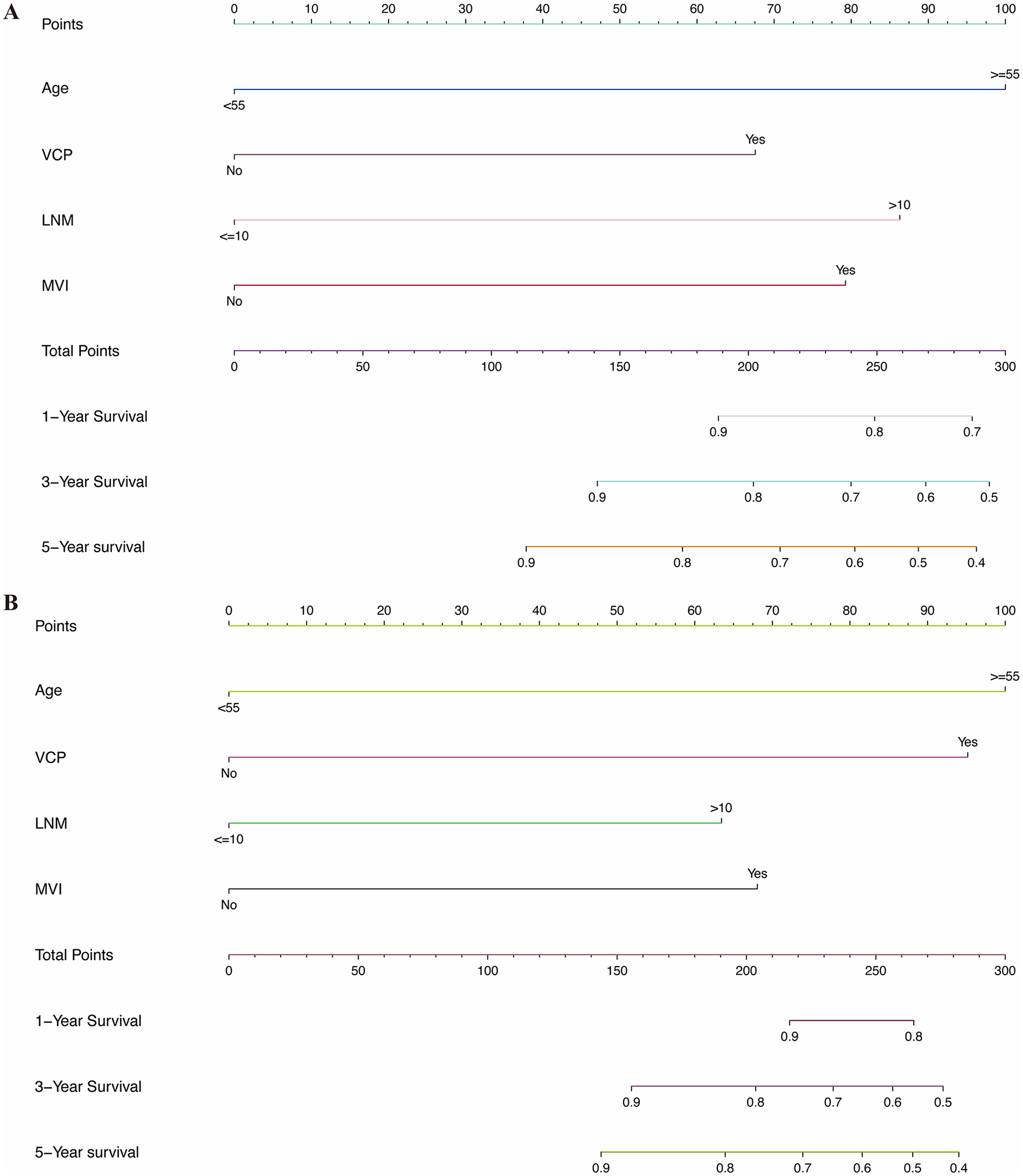
Nomogram for predicting 1-, 3-, and 5-year disease-free survival after surgery. (A) training cohort (B) testing cohort. VCP, vocal cord paralysis;LNM, lymph node metastases; MVI, microvascular invasion.

The AUCs of nomogram model in (A) training cohort; (B) validation cohort for predicting disease-free survival. The 1- (C), 3- (D), and 5- (E) year calibration curves in training cohort. The 1- (F), 3- (G), and 5- (H) year calibration curves in validation cohort.
Risk Stratification
The T4a PTC patients with RLN invasion were divided into a high-risk group and a low-risk group based on the risk scores of the nomogram model, with the median risk score used as the cutoff in the training set and verified them in the test set. This simple classification can help determine appropriate treatments for patients. According to the risk scores from both nomogram models, T4a PTC patients with RLN invasion in the low-risk group all had better PFS than those in the high-risk group (P < .0001) (Figure 4).

Kaplan–Meier curves of disease-free survival for patients in high-risk and low-risk groups in (A) training cohort; (B) testing cohort.
Prognosis and the Voice of Patients on RLN Surgical Procedures
In this cohort, 218 (52.2%) patients underwent RLN separation, and 200 (47.8%) patients underwent RLN resection or resection and anastomosis (Table 1). Based on the univariable analysis, the 5-year PFS rates were 92.5% and 87.0% in patients who underwent RLN separation and RLN resection or resection and anastomosis, respectively (HR = 2.007, 95% CI: 1.061-3.795, P = .032). Conversely, according to the multivariable analysis, RLN surgical methods were not associated with the risk of disease progression (HR = 0.964, 95% CI: 0.474-1.958, P = .918) (Table 2).
Among patients with preoperative VCP by laryngoscope, 28 (12.8%) patients underwent RLN separation, and 64 (32.0%) patients underwent RLN resection or resection and anastomosis. After surgery, hoarseness was observed in 133 (61.0%) and 177 (88.5%) patients in the separation and resection groups, respectively. In the late follow-up, hoarseness persisted in 23 patients in the separation group (10.6%) and 67 patients (33.5%) in the resection group (Table 3). The median follow-up time was 50 months. In the RLN separation group, the RLN function was restored in 82.7% of patients, and their voices almost returned to normal.
Association Between Voice and RLN Surgical Method.

Abbreviations: RLN, recurrent laryngeal nerve;VCP, vocal cord paralysis.
Discussion
Approximately 5% to 15% of patients with PTC progress to stage T4a with low long-term survival rates.9-12 In this cohort study, the 5-year cumulative PFS rate of all T4a PTC patients with RLN invasion was 89.8%. Our result is consistent with a previous study. 13 We assessed the association between risk factors and PFS in 418 T4a PTC patients with RLN invasion, and the results showed that age ≥55 (HR = 3.191), preoperative VCP (HR = 2.337), microvascular invasion (HR = 2.318), and CLNM >10 (HR = 2.480) were associated with an increased risk of T4a PTC disease progression.
Based on the AJCC classification system, the 10-year DSS of T4a patients aged ≥55 years ranges from 60% to 70%, and the 10-year DSS rate for patients aged <55 years (without distant metastases) is between 98% and 100%. 1 Ito et al. discovered that age, particularly over 55 years of age, was correlated with the cause-specific survival rate of T4a PTC. 14 Moreover, 2 studies discovered that age (above 55 years) was a risk factor for postoperative recurrence in PTC patients with RLN invasion.13,15 Our study also identified that age ≥55 years was associated with poor PFS in T4a patients with RLN invasion. Therefore, special attention should be paid to this population, particularly older patients.
Two small sample-size studies reported that preoperative VCP was not an independent risk factor for recurrence in T4a patients with RLN invasion.13,16 A recent study of ≤1 cm PTC found that preoperative VCP was a predictor of RLN invasion, and that patients with RLN invasion had poorer recurrence-free survival. 17 Our analysis revealed that preoperative VCP increased the risk of disease progression in T4a PTC patients with RLN invasion. Additionally, our study first proved that the presence of microvascular invasion increased the risk of disease progression by 2.318 times in T4a PTC patients with RLN invasion.
Previous studies reported that the number of metastatic lymph nodes was not related to recurrence.18,19 In contrast, another study discovered that PTC patients with 5 or more metastatic lymph nodes have a significantly higher risk of recurrence (19% vs 8%). 20 According to the 2015 ATA guidelines, CLNM >5 is an important prognostic factor for PTC patients. 21 However, no studies investigate the effect of the number of CLNMs on the prognosis of T4a patients with RLN invasion. Our study revealed that T4a patients with RLN invasion who had CLNM >10 showed a significantly higher risk of disease progression than those with CLNM ≤10. Moreover, the 5-year PFS rates of T4a patients with RLN invasion who had CLNM >10 and patients with CLNM ≤10 were 84.4% and 93.1% (P = .014), respectively.
Several studies have developed models to predict the prognosis of PTC patients22,23; however, no studies have reported a prediction model for T4a patients with RLN invasion. In this study, a nomogram model was established using variables identified through multivariable Cox regression analysis. The C-index value of the model was 0.778, suggesting favorable predictive performance. In addition, all patients were divided into high-risk and low-risk groups for subgroup analysis, and the results showed that patients in the low-risk group had a significantly lower risk of disease progression than those in the high-risk group. The results further validate the strong predictive capacity of our model. Our model can assist clinicians in identifying individuals with a low risk of disease progression and thus developing more conservative surgical approaches to preserve their organ function and improve their overall quality of life.
The optimal surgical approach for papillary thyroid carcinoma invading the RLN remains controversial, particularly concerning the decision to perform nerve shaving. RLN shaving is technically challenging, and even if the nerve remains intact, it may result in organ dysfunction.24,25 Hence, the impact of nerve preservation on the long-term survival of patients’ needs to be further investigated. Previous studies have suggested that the RLN should be preserved as much as possible.26,27 A recent study reported that 73 of 171 T4a patients with RLN invasion underwent RLN separation or partial layer resection, with an RLN retention rate of 42.7%. 13 Previous studies indicated that RLN function was preserved in more than 80% of patients after nerve shaving, and their voices nearly returned to normal.28,29 Regarding the impact of RLN surgical methods on the prognosis of patients, many studies demonstrate similar recurrence and survival rates in patients on RLN separation or partial layer resection compared to those on full resection.16,30-32 In our study, the RLN retention rate was 52.2% (218/418), and nerve preservation did not increase the risk of disease progression. Additionally, in the RLN separation group, the RLN function was restored in 82.7% of patients, and their voices nearly returned to normal.
There are several limitations to this study. First, it is a retrospective design, and potential confounding factors may affect prognosis. Second, the incidence of T4a PTC disease is low, which results in a limited number of studies reporting this disease. Besides, the surgical skills of different surgeons may affect the patient’s prognosis. In addition, while internal verification of the nomogram model showed certain feasibility, external validation is still required. Unfortunately, obtaining data from external sources for verification is currently challenging. Nevertheless, we are committed to securing external data for validation in the future.
Conclusions
This study reveals that at age ≥55 years, preoperative VCP, microvascular invasion, and the number of CLNM >10 were associated with a higher risk of disease progression in T4a PTC patients with RLN invasion. The model constructed based on these factors can help clinicians identify high- and low-risk patients, thereby developing appropriate treatment strategies and improving the prognosis of patients with T4a PTC with RLN invasion. Additionally, the preservation of the RLN nerve does not increase the risk of disease progression.
Supplemental Material
sj-docx-1-ohn-10.1177_19160216251314750 – Supplemental material for Nomogram Predicting Progression-Free Survival in Locally Advanced Papillary Thyroid Cancer with Recurrent Laryngeal Nerve Invasion
Supplemental material, sj-docx-1-ohn-10.1177_19160216251314750 for Nomogram Predicting Progression-Free Survival in Locally Advanced Papillary Thyroid Cancer with Recurrent Laryngeal Nerve Invasion by Yixuan Song, Yudong Ning, Han Li, Yuqin He, Yang Liu and Shaoyan Liu in Journal of Otolaryngology - Head & Neck Surgery
Footnotes
Acknowledgements
None.
Data Availability
All data generated or analyzed during this study are included in this published article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was funded by National Natural Science Foundation of China (Grant No. 81902728) and Beijing Hope Run Special Fund of Cancer Foundation of China (Grant No. LC2017L04, No.LC2020B11).
Ethical Statement
Each patient signed the informed consent document before the study.
Supplemental Material
Additional supporting information is available in the online version of the article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.