
Abstract
Aerobic (cardiopulmonary) exercise training improves fitness and limits the progression of motor signs in Parkinson's disease. Individualized development of exercise prescriptions relies upon accurately measured peak heart rate (HR). Cardiopulmonary exercise testing (CPET) is the only methodology to objectively confirm an individual's peak HR. This test is important in individuals who may have autonomic dysfunction, which may manifest as chronotropic incompetence. Without CPET's confirmation of maximal effort, there is no way of knowing whether exercise prescription in those with chronotropic incompetence is accurate. CPET also provides information regarding cardiorespiratory fitness, which can motivate patients to exercise to prolong health.
Plain language summary
Aerobic exercise training has been shown to be an important part of the overall treatment plan for Parkinson's disease. It is important to develop an exercise training plan based on an individual's abilities and personal response to exercise to ensure that the plan is safe, feasible, and effective. The best way to measure somebody's response to aerobic exercise is through a cardiopulmonary exercise test, which confirms maximal effort and provides the highest level of confidence in the resulting exercise plan. This test has the added benefit of measuring fitness, which can help guide discussions and motivate those with Parkinson's disease to work towards maintaining health across the lifespan. This paper outlines important considerations for cardiopulmonary exercise testing and provides key reminders regarding the test itself as well as how to use these data to guide exercise in Parkinson's disease.
Keywords
Introduction
We have recently published a commentary entitled “Advice to People with Parkinson's in My Clinic: Exercise,” in which we provide an exercise prescription consisting of four key components, including aerobic exercise, resistance/weight training, flexibility exercise, and neuromotor exercise. 1 This multi-faceted approach to exercise in Parkinson's disease (PD) has been shown to positively impact motor and non-motor features of PD.2,3 This review will focus on aerobic exercise, which has been shown to be safe, effective, and most likely to be disease-modifying in those with PD. Participation in aerobic exercise, especially at a vigorous intensity, requires confidence in the assessment of peak heart rate (HR) during exercise testing which allows the development of individualized exercise prescriptions. We and others have shown that a subset of people with PD have a blunted HR response to maximal exercise,4–6 also known as chronotropic incompetence (CI). 7 Simply put, CI is the inability to achieve 85% of age-predicted maximal HR (APMHR). 8 This raises the important question of how people can determine the best HR to exercise at their optimal intensity? In this commentary, we make the case that cardiopulmonary exercise testing (CPET) is highly advisable for, at a minimum, the subset of people with PD who have CI or evidence of autonomic dysfunction following clinical evaluation. This will give people with PD the most accurate HR for aerobic exercise prescriptions. CPET has the added benefit of also providing a current assessment of overall cardiorespiratory fitness (CRF), and for that reason, all people with PD, regardless of CI status, would benefit from a CPET. The proposed benefits of CPET provided throughout this commentary must be balanced against potential limitations in the form of cost, access, or other health system-specific factors; however, ongoing and future research will continue to address these questions to promote increased CPET utilization.
Importance of cardiorespiratory fitness
CRF is a component of physical fitness and refers to an individual's ability to utilize oxygen to support physical activity and exercise. 9 The study of CRF began a century ago, 10 and since then a robust body of literature has repeatedly demonstrated that higher CRF is strongly and independently associated with decreased cardiovascular disease risk factors11,12 and all-cause mortality in healthy individuals13,14 and those with cardiovascular risk factors.15,16 These relationships resulted in a landmark 2016 publication from the American Heart Association, in which there was a call for CRF to be used as a clinical vital sign to aid in risk factor assessment for chronic disease. 17 The importance of routine assessment of CRF for evaluating prognosis is underscored by the volume of studies highlighting the associations between both baseline CRF18–21 and longitudinal trends in CRF 22 and risk for mortality. Importantly, data suggest that individuals with PD may experience a greater risk for cardiovascular events, including acute myocardial infarction 23 and stroke. 24 Improvements in CRF have been demonstrated concurrently with improvements in motor score in PD, 25 and, taken together, these data highlight that increased CRF is critically important for multiple health outcomes and disease progression in those with PD.
Further, there is a documented decrease in CRF in people with PD compared to age-matched people without PD, 6 which highlights the added importance of increasing or maintaining CRF in people with PD. The reduced CRF in PD is likely multifactorial due to disease-specific impairments and reduced physical activity.26,27 Specifically, cardiovascular autonomic dysfunction, which is seen in a third of people with PD28,29 and results in abnormal blood pressure and heart rate responses during exercise, 30 may cause decreases in oxygen delivery to active muscles and oxygen utilization, ultimately causing reduced CRF and exercise intolerance. Abnormal blood pressure patterns (e.g., orthostatic hypotension and supine hypertension) in people with PD are also independently associated with an increased risk of cardiovascular diseases 31 and brain white matter lesions.32,33 Orthostatic hypotension is the most common manifestation of cardiovascular autonomic dysfunction in PD and can be easily identified in the clinical setting by the measurement of postural changes in blood pressure.34,35 Therefore, systematic screening for orthostatic hypotension has the potential to identify people with PD at high risk of reduced CRF.
Effects of heart rate-guided aerobic exercise training on cardiorespiratory fitness and PD-specific clinical outcomes of interest
Aerobic exercise intensity can be dosed based on submaximal percentages of measured peak HR, peak oxygen consumption (VO2max), power (e.g., Wattage on a cycle ergometer), or subjective markers of effort during exercise (e.g., the “talk test” 36 or specified ratings of perceived exertion (RPE)). 37 Some aerobic exercise interventions in PD have relied upon exercise prescriptions based on percentages of peak HR, consisting of participation in moderate intensity (60–65% of peak HR) or vigorous intensity (80–85% of peak HR).25,38–42 Aerobic exercise guidelines for PD recommend participation in vigorous intensity exercise, with additional recommendations for those who are deconditioned or have more advanced PD to attempt to progress to vigorous intensity exercise over time. 1 Participation in such vigorous aerobic exercise has been effective in increasing VO2max 25 and minimizing the anticipated worsening of motor signs and symptoms of disease.25,43,44 These aerobic exercise-driven effects in PD represent clinically relevant outcomes which promote maintenance of independence and function over time as the disease progresses. Participation in individualized vigorous intensity aerobic exercise relies upon accurate assessment of peak HR from which target HR ranges can be calculated. Put another way, any erroneous assessment of peak HR leading to an under- or over-estimation of an individual's peak HR will result in a potentially suboptimal or unsustainable aerobic exercise prescription.
Methods to evaluate peak heart rate during exercise testing
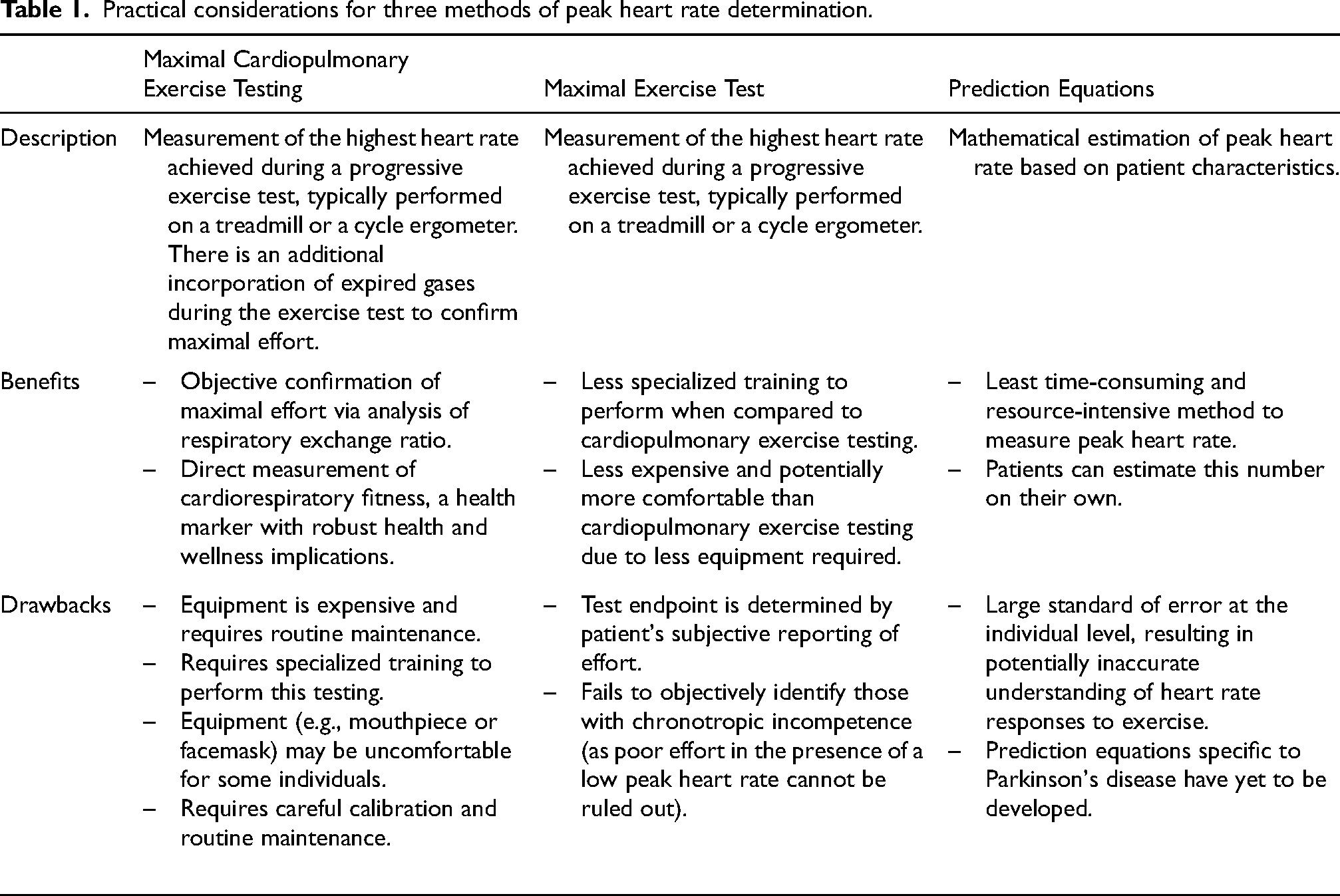
Peak HR can be determined by three related but separate methodologies, which are further detailed in Table 1. The first is CPET, which incorporates the direct quantification of expired gases during maximal aerobic exercise testing45,46 and has been demonstrated to be safe and well-tolerated in older adults. 47 This allows the calculation of respiratory exchange ratio (RER), calculated by dividing the volume of carbon dioxide produced by the volume of oxygen consumed (VCO2/VO2). 48 RER is an objective marker of effort during CPET, and therefore peak HR data obtained during a CPET with a maximal RER reflects an objectively confirmed peak HR. 49 Application of CPET as the basis for development of aerobic exercise prescriptions has been demonstrated to directly result in improvements in clinical outcomes of interest and CRF in those with recently diagnosed PD.25,43 The second method is a maximal exercise test without measurement of gas exchange. This technique relies upon subjective assessment of the individual's level of effort, often relying upon the individual's RPE. Reliability of RPE-dependent determination of maximal effort has been demonstrated to be low, 50 increasing the risk for recording a submaximal HR and underdosing an aerobic exercise prescription. The third method is the application of peak HR prediction equations, which have been developed based on the well-documented reduction in peak HR with age.51–54 While these equations represent the least resource-intensive approach to determination of peak HR, they also have variability at the individual level. Commonly used peak HR prediction equations in healthy individuals have been shown to miscalculate measured peak HR by 11–12 bpm, with additional error observed when the equations are applied to males and those with higher body mass index. 55 Further, data suggest that traditionally used APMHR equations may underestimate peak HR in older adults. 52 Additionally, there have been no published studies regarding the function of these equations in people with PD. Although CPET is the gold standard, if it is not available, maximal exercise test or predictive equations can be used so long as pre-exercise screening processes based on current exercise participation, chronic disease status, and review of active symptoms are implemented to ensure safety during initiation of an aerobic exercise prescription. 56
Practical considerations for three methods of peak heart rate determination.
How cardiopulmonary exercise testing is performed
CPET is performed using indirect calorimetry via analysis of expired gases during the completion of a graded exercise test protocol. Testing equipment includes a facemask or mouthpiece and tube to direct expired gases into a metabolic cart. 45 Special consideration must be given to this equipment utilized during CPET, as accurate measurement of peak ventilation depends on adequate fitting of the facemask or mouthpiece to limit any amount of air escaping equipment seals thereby reducing recorded volumes. Testing equipment also includes gas concentration and ventilation analyzers in the metabolic cart itself to quantify volumes of oxygen and carbon dioxide expired during testing. 45 An integral component of CPET is an exercise ergometer to systematically increase the work rate at pre-determined intervals to elicit a maximal effort during the CPET. This is most commonly a treadmill or cycle ergometer, with the selection of mode depending on clinical characteristics and balance/gait mechanics of the person being tested, resources available at the testing site, and purpose of the CPET. Selection of CPET mode is also informed by the functional ability of the individual being tested, with individuals who may be in more intermediate or advanced stages of PD being more appropriately tested on a cycle ergometer. Of note, though, measured VO2max has been shown to be 10–15% lower on a cycle ergometer when compared to a treadmill,57,58 largely due to differences in muscle mass being used and general familiarity involved with exercise between the two modes. Additional equipment includes a method of HR monitoring (typically a HR strap, or, less commonly, either an electrocardiogram monitor or pulse-oximeter) and charts to assess subjective effort during testing (including the RPE and rating of perceived dyspnea, as appropriate). 45 Blood pressure is assessed at each stage during CPET to ensure a normal hemodynamic response to increasing intensities of aerobic exercise. Special considerations involved with CPET in PD may include the use of a gait belt or other gait assistive device, as CPET protocols typically increase percent grade on the treadmill overtime and therefore may result in gait instability and balance limitations that prevent completion of the test. Importantly, completion of the CPET does require that the individual has adequate neuromuscular control and coordination to perform exercise of increasing intensity throughout the test, and PD-related limitations may result in barriers to safely and feasibly performing CPET.
Value of additional cardiac and pulmonary metrics obtained via cardiopulmonary exercise testing
In addition to the VO2max and measured peak HR values obtained from CPET, this evaluation of aerobic exercise capacity provides a wealth of clinically relevant and prognostically important information. First, application of electrocardiogram (ECG) monitoring of the heart's electrical activity, when ordered as part of the test, allows identification of potential abnormal cardiac responses to submaximal and maximal exercise. Specifically, evaluation of ectopy (e.g., premature atrial or ventricular contractions) during and after exercise and directly comparing to ECG recordings taken prior to CPET may predict future adverse events. 59 Further, ECG tracings allow for analysis of the ST segment and potential T wave inversion, which may provide evidence for potential myocardial ischemia or distress. 45 The RER-guided determination of maximal effort obtained during CPET may yield these electrocardiographic changes at peak exercise, which may not present at submaximal intensities. An additional HR metric obtained following completion of CPET is HR recovery. Both HR recovery at 1 min post-CPET 60 and late HR recovery 61 have been identified to be independently associated with risk for all-cause mortality. These HR-derived metrics are of particular importance in PD, a population in which cardiac autonomic dysfunction is well-documented. 30 Importantly, however, ECG monitoring is not required by ACSM guidelines in the performance of CPET and does not need to be used in people with PD who have undergone ACSM pre-exercise participation clearance. 56
Other clinically significant variables derived from CPET include markers of pulmonary function. These include the oxygen uptake efficiency slope, which represents the global function or impairment of the pulmonary, cardiovascular, and skeletal muscle systems during exercise testing. 62 CPET also provides data regarding ventilatory threshold (VT), or the submaximal point at which ventilation increases disproportionately to further increases in oxygen consumption to compensate for the buildup of metabolic byproducts. This value serves as an indicator of training status, with untrained adults typically surpassing the VT between 45% to 65% of VO2max 63 whereas trained individuals approach the VT at higher percentages, signifying a greater ability to metabolically process the end products of aerobic exercise. 64 Increasing one's VT, independent of improvements in VO2peak, would represent positive training adaptations and result in improvements in quality of life for those with PD. Ventilatory efficiency, quantified as VE/VCO2 slope, represents efficiency in the clearance of metabolic byproducts during aerobic exercise and remains understudied in PD. 65 VE/VCO2 values of <30 at peak exercise are considered normal, 66 whereas values exceeding this threshold are likely indicative of an underlying chronic health condition. For instance, values >60 have been documented in heart failure, pulmonary hypertension, and chronic obstructive pulmonary disease patients with advanced disease severity,67–69 and such values may indicate poor prognosis in patient populations. Elevated values observed during CPET in people with PD would similarly correlate with exercise intolerance and indicate poor prognosis.
Some studies have found an increased risk of cardiac arrhythmias (i.e., atrial fibrillation) in PD. 70 CPET, coupled with ECG monitoring, may improve the detection of cardiac arrhythmias in people living with PD and facilitate simple treatment decisions such as use of blood thinning medications. Similarly, shortness of breath is not uncommon in PD. Respiratory impairments are likely multifactorial due to wearing-off and dyskinesias with dopaminergic drugs, rigidity and kyphosis that PD patients experience, anxiety, abnormal central and peripheral chemoreflex function, and dysregulation in brainstem structures that control respiration. In combination with spirometry, echocardiography, or radiographic procedures, CPET adds complementary information by measuring physiologic parameters during submaximal and maximal exercise and may help with accurate identification of the cause of dyspnea. For example, exertional dyspnea may be related to deconditioning, which can be detected by CPET. In summary, in addition to accurate determination of maximum heart rate, CPET can provide a wealth of electrophysiological and pulmonary information that can be used to determine one's readiness for exercise participation, and further to assess one's longer-term physiological response to an exercise prescription via follow-up testing. The important data obtained through CPET provide the clinician with invaluable insights into these body systems and can inform potential follow-up communications with the broader medical team, if warranted.
Effects of chronotropic incompetence on aerobic exercise prescription in PD
Objective confirmation of effort during aerobic exercise testing is of paramount importance as there is a subset of adults who demonstrate CI, which is defined as an inability to achieve 85% APMHR. 7 Evidence suggests that upwards of 10–15% of individuals recently diagnosed with PD demonstrate CI, 4 and that this CI is associated with decreased CRF. There are no data measuring frequency of CI in people with PD further along in the disease, but we hypothesize the frequency increases with disease progression. It is important to note that CI is present in some people with PD because of autonomic nervous system impairment, independent of medication. CI can also be caused by a variety of medications including beta blockers, among others. Regardless of the cause, the presence of CI results in a subset of the PD population for which maximal exercise testing without cardiopulmonary analysis and/or the use of peak HR prediction equations yield inaccurate exercise prescriptions and frustration in implementing the exercise prescription. In this subset of individuals with CI, CPET is the only way to maintain full confidence that recorded peak HR values ≤85% of APMHR are not a direct result of submaximal effort. Further, confirmation of true peak HR via CPET in those with CI avoids an inappropriate, unsustainable, frustrating, and potentially unsafe aerobic exercise prescription based on HR prediction equations.
Two scenarios related to abnormal HR responses during aerobic exercise testing and training are illustrated in Table 2. For an individual with CI (Person A), relying on APMHR in the development of an aerobic exercise prescription would result in an unrealistic and potentially unsafe prescribed HR zone 19–25 bpm above the individual's appropriate values. Because this individual cannot possibly reach the prescribed HR zone, they may injure themselves trying or they may become frustrated with a HR-guided exercise prescription they cannot possibly achieve. A complete CPET analysis of this individual is included in the Supplemental Material. Conversely, in an individual with a measured peak HR substantially higher than APMHR (Person B), relying on APMHR when creating an aerobic exercise prescription would result in a prescribed intensity lower than what has been shown to benefit PD clinical outcomes of interest (e.g., motor score and VO2max). Practical challenges associated with HR-guided exercise prescription would result in this person under-exercising. In this example, reliance on APMHR would result in the prescribed HR zone being 1–8 bpm below appropriate values. It is important to note that while data suggest poor outcomes and prognosis in clinical populations with chronotropic incompetence, 71 the potential clinical implications of an exaggerated chronotropic response have yet to be fully explored. At present, an exaggerated peak HR response to CPET highlights the limitations of simple prediction equations to calculate peak HR.
Representation of the effects of chronotropic incompetence and exaggerated chronotropic response in aerobic exercise testing and training.
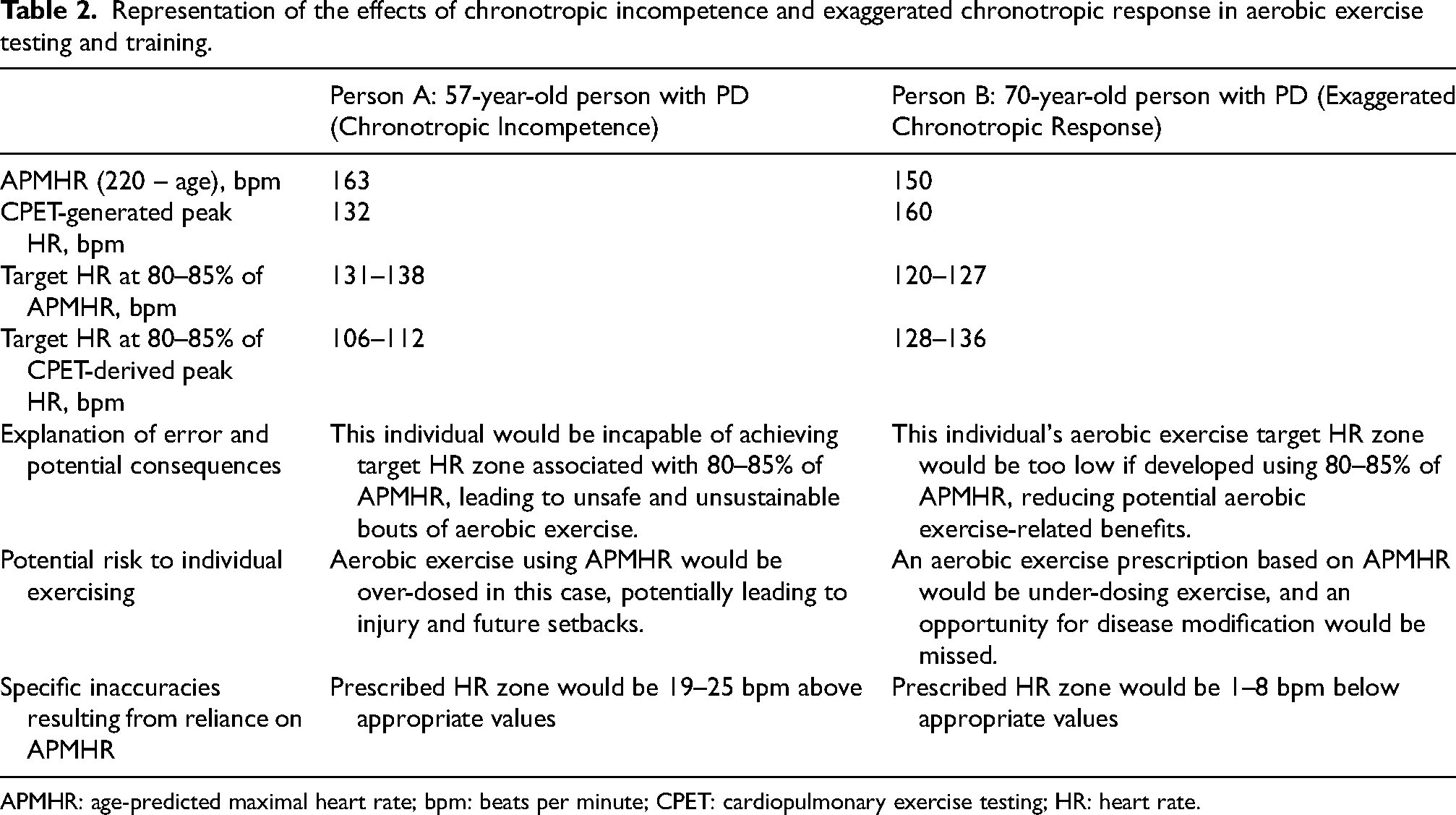
APMHR: age-predicted maximal heart rate; bpm: beats per minute; CPET: cardiopulmonary exercise testing; HR: heart rate.
Both of these scenarios have been observed in an aerobic exercise training study in individuals with early PD. 4 Figure 1 illustrates results of CPET-derived peak HR data in this population. In the study sample of 128 CPETs, 24 (18.8%) showed evidence of CI, as defined by a failure to achieve 85% of APMHR during maximal exercise. These individuals are reflective of “Person A” in Table 2. A total of 85 individuals (66.4%) showed a normal chronotropic response to exercise, defined as a measured peak HR value between 85–105% of APMHR. Lastly, 19 individuals (14.8%) exhibited an exaggerated chronotropic response to exercise, defined as greater than 105% of APMHR. These individuals are reflective of “Person B” in Table 2, and clearly illustrate the limitations associated with application of prediction equations for calculation of peak HR. Taken together, these data suggest that over a third of individuals recently diagnosed with PD have HR responses to CPET that deviate from what one might expect based on age. These individuals highlight the importance of using CPET to determine maximum HR for the purposes of developing an aerobic exercise prescription.
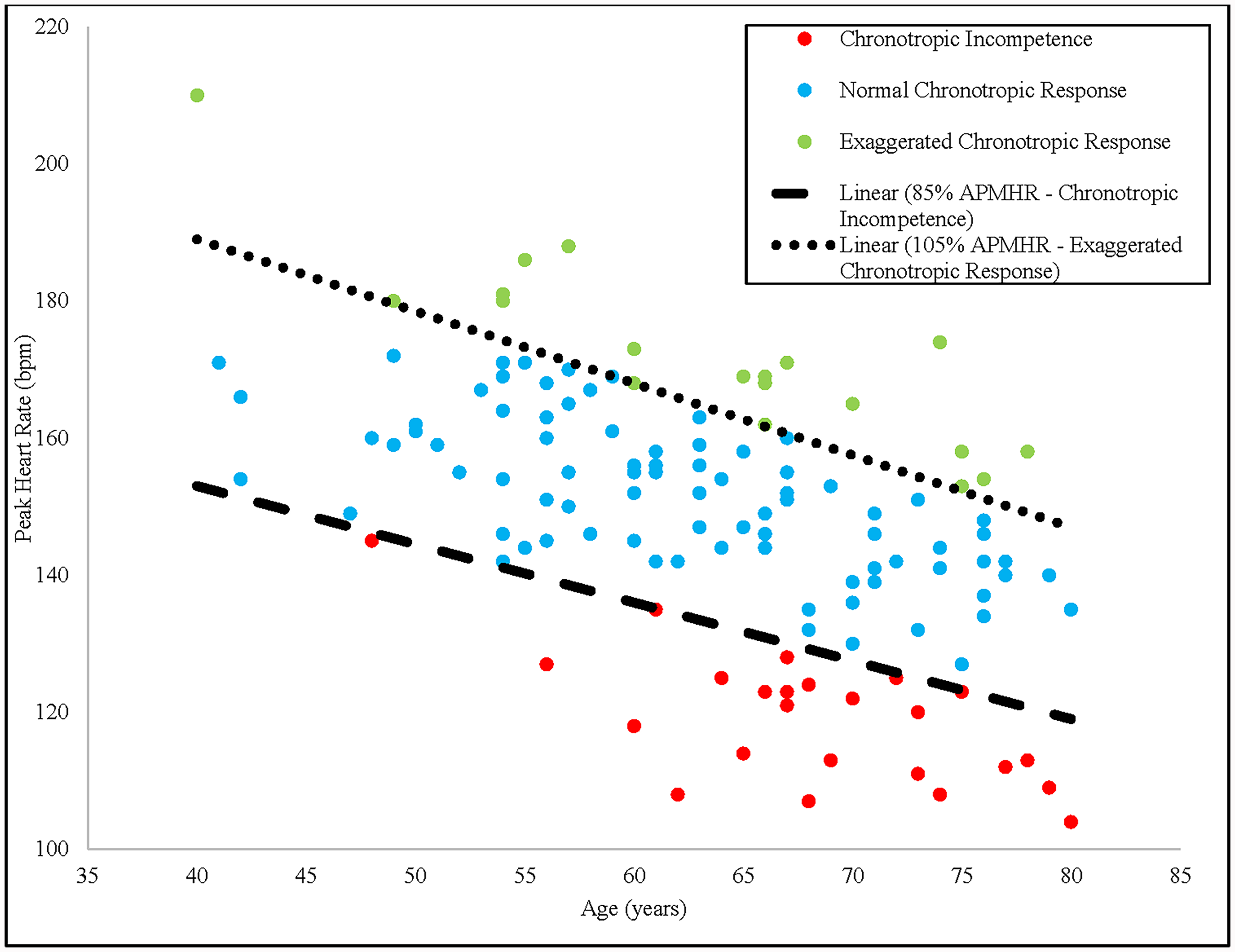
Association between age and peak heart rate during baseline CPET in SPARX by chronotropic response to maximal exercise. Data points above the top dotted line represent exaggerated chronotropic responses to exercise (≥105% of APMHR), whereas data points below the bottom dotted line represent evidence of chronotropic incompetence to exercise (≤85% of APMHR). Data points in between the dotted lines represent normal chronotropic responses to exercise (85% to 105% of APMHR). CPET, cardiopulmonary exercise testing; APMHR, age-predicted maximal heart rate.
Additionally it has recently been shown that these individuals with chronotropic incompetence can achieve similar clinical and fitness improvements as those with normal chronotropic status. 72 Analyses of mean data from this representative study sample reveal that reliance upon APMHR in the development of high intensity aerobic exercise prescriptions in those with CI or exaggerated chronotropic responses to CPET results in inappropriate HR ranges. Those with CI in this study would have been expected to exercise between 26–27 bpm above the HR range developed from 80–85% of their objectively measured peak HR, increasing risk for musculoskeletal injury or potential frustration at a perceived inability to meet study requirements. Conversely, those with exaggerated chronotropic responses would have been expected to exercise between 12–13 bpm below the HR range developed from 80–85% of their objectively measured peak HR, resulting in widespread underdosing of aerobic exercise.
What we tell people with PD in our clinic
We tell all people with PD in our clinic that if they are proactive in maintaining their health (rather than reactive in responding to disability) it is possible for them to journey through their disease with a quality of health that can approach that of someone without PD. We suggest they obtain a maximal CPET for two reasons. First, if they are engaged in or thinking of starting HR-guided aerobic exercise, it is possible they may have a HR that is lower or higher than that determined by age-based formulae. As such, we suggest they consider getting a CPET to obtain an accurate measure of their peak HR to guide their aerobic exercise prescription and work towards attainment of the clearly established general and PD-specific health benefits derived from this approach to exercise. Second, assessment of their VO2max will serve as a marker of baseline health from which they can be motivated to improve over time. The evidence is clear that there are strong associations between maintenance of independence, overall health, cognitive status, and VO2max.16,73,74 Clinicians who utilize CPETs to obtain VO2max will be better equipped to counsel their patients with PD regarding lifelong implications of fitness, including the potential to achieve future goals and maintain one's ability to participate in physical activities of daily living. VO2max is a modifiable health parameter and minimizing the expected age-related decrease in VO2max over time promotes improved health outcomes. 75
Our prior work has shown maximal exercise testing and vigorous intensity aerobic exercise to be safe and effective in both minimizing the well-documented progression of PD symptoms and increasing cardiorespiratory fitness over time. 25 What remains to be done is (1) educate both patients and physicians that maximal CPETs are recommended and possible in people with PD and (2) find places for our patients to obtain a CPET. It is important to note that in the U.S., CPET is covered by Medicare and by select insurance companies. However, despite insurance coverage, it is the experience of the authors that CPETs obtained for individuals with PD outside of a research setting can be challenging to obtain. At most institutions, CPET capability is housed within the cardiovascular department and often booked out quite far with individuals at high risk of ischemia taking priority. It is possible that CPET may also be obtained within high end fitness centers, exercise science departments, and selected physical therapy programs. The authors recognize that there are significant challenges with CPET accessibility and that research studies focusing on implementation are required to more fully understand the feasibility of CPET-guided aerobic exercise prescriptions for the individuals with PD on a national scale. Further, research regarding cost-effectiveness of CPET implementation internationally is warranted to better understand how CPET may be utilized around the world, especially in low- and middle-income countries in which resources to support CPET may be scarce. These important factors and logistical considerations exist as potential barriers to the widespread utilization of CPET necessary to fully realize the American Heart Association's call for inclusion of CRF as a routinely measured vital sign. 17 Ultimately, research to date strongly supports utilization of CPET when available to provide the highest quality aerobic exercise prescriptions and to positively impact the long-term health of those with PD.
Supplemental Material
sj-docx-1-pkn-10.1177_1877718X251330814 - Supplemental material for Advice to people with Parkinson's in my clinic: Get a cardiopulmonary exercise test
Supplemental material, sj-docx-1-pkn-10.1177_1877718X251330814 for Advice to people with Parkinson's in my clinic: Get a cardiopulmonary exercise test by Garett J Griffith, Kathleen E McKee, Guillaume Lamotte, Nijee S Luthra and Daniel M Corcos in Journal of Parkinson's Disease
Footnotes
Acknowledgements
The authors have no acknowledgments to report.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The research reported in this publication was supported by the National Institute of Neurological Disorders and Stroke and the National Institutes of Health under Award Numbers U01NS113851 and K23NS123506. Research is also supported by the National Institutes of Health’s National Center for Advancing Translational Sciences, Grant Number UL1TR001422. It is also supported by a generous philanthropic gift in honor of Howard Gilbert and a gift from the JCS Family Foundation.
Data availability
Data sharing is not applicable to this article as it is a commentary, and no datasets were generated.
Conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.