
Abstract
Purpose
This study aimed to compare the immediate functional impact of wearing ankle foot orthoses (AFOs) designed using the Optimal Segment Kinematics and Alignment approach to Rehabilitation (OSKAR method) versus wearing standard ankle foot orthosis (AFO)-footwear in children with spastic diplegic cerebral palsy.
Methods
Ten participants, ages seven to 13 years, from local pediatric clinics in a large suburban area participated in the study. Each participant wore both types of orthoses in a randomized order. This was determined by participants choosing a sealed envelope containing a sticker indicating which orthosis to be worn for the first data collection. Participants were assessed using three functional outcome measures: 1) the Pediatric Balance Scale (PBS), 2) Standardized Walking Obstacle Course, and 3) the Six-Minute Walk Test. Non-parametric Wilcoxon signed rank tests were used to compare outcome scores between the two conditions.
Results
Total scores on the PBS were significantly higher when wearing the OSKAR AFO-footwear combinations (AFOFCs) (median = 50.50) versus standard AFOFCs (median = 47.00), T = 26.50, p = 0.034, r = 0.95, but all other immediate functional scores were comparable between conditions.
Conclusions
AFOFCs designed using the OSKAR method may improve functional balance and should be considered when determining the orthotic prescription. These exploratory findings emphasize the need for further investigation of the effectiveness of OSKAR AFOFCs in children with spastic diplegic cerebral palsy (CP).
Introduction
Conservative interventions including physical therapy and bracing with orthotic devices such as ankle foot orthoses (AFOs) are typically the first treatments of choice for children with spastic cerebral palsy (CP).1,2 The goal of ankle foot orthosis (AFO) use is to improve ankle/foot alignment and stability, as distal control during gait is thought to influence proximal stability.3,4 Favorable changes in function of children with CP have been reported with AFO use5–8; however, supporting research consists of mostly low to moderate quality studies and often lacks specificity related to AFO details. 9
Investigations that have included the design of solid (fixed) AFOs noted the AFO's ankle angle to be either 0 degrees (standard/plantigrade) or a few degrees of dorsiflexion.10–13 A standard, or plantigrade, ankle joint alignment in an AFO can be problematic if a child lacks available range of motion in the ankle from short muscle length of the gastrocnemius, as is common with spastic CP. 14 An improperly aligned AFO may compromise function by causing excessive hip and knee joint flexion or extension, poor foot posture, undue stress to soft tissues and joints, pain, and noncompliance with wearing the AFOs.15,16
There is a lack of consensus and standardization for the type of AFO design required to meet the specific needs of children with CP.16–18 Additionally, researchers have found that healthcare professionals lack confidence in prescribing orthoses and making decisions related to orthotic intervention.17,19 Clinicians and consumers agree that “ideal orthotic management” should be tailored to individual patient needs and goals.19,20
Biomechanical optimization and tuning of AFOs have been suggested to improve gait kinetics and kinematics in children with gait impairments.21–24 Owen described orthosis optimization using the Optimal Segment Kinematics and Alignment approach to Rehabilitation (OSKAR method). 15 The goal of this method involves thorough assessment of body structure/function and use of published algorithms to determine orthotic and footwear specifications. This is in addition to realizing child/family goals for orthotic use. The objective of the OSKAR method is to optimize segmental alignment by choosing an appropriate AFO design, angle of the ankle, shoe design, and shank to vertical angle (SVA), along with ensuring optimal segment proportions. Tuning, or making small adjustments to AFOs and footwear, may be necessary to achieve optimal segmental alignment and the most appropriate SVA.15,23–25
Lower leg orthoses are typically worn with a shoe resulting in an AFO-footwear combination (AFOFC). A small number of studies have examined the use of AFOFCs designed and tuned using the OSAKR method versus standard AFOFCs in children with CP who exhibit limited ankle dorsiflexion.21,22,26–28 Most of the current evidence is related to the impact of optimizing orthoses on joint range of motion and gait variables; however, there is a paucity of research examining the impact of AFO optimization on functional outcomes.
Optimal segmental alignment and control have the potential to provide improved efficiency and stability during gait, which could improve function.29–33 In a recent longitudinal study comparing OSKAR to standard AFOFCs in children with CP, gait priorities and total Pediatric Balance Scale (PBS) scores were significantly higher when wearing OSKAR AFOFCs. 21 Bayón et al. concluded that individuals with CP desire to improve walking in real-life activities and noted that assessment of biomechanics in a gait laboratory may not be a true representation of functional performance in daily settings.19,34,35 To examine the immediate functional impact of AFOs designed using the OSKAR method, the aim of this exploratory study was to compare performance on functional outcome measures when wearing OSKAR AFOFCs versus standard AFOFCs in a laboratory modified to mimic real-life settings with obstacles, turns, and varied walking surfaces. Total PBS scores of ambulatory children with CP were collected along with scores on a standardized obstacle course that measured walking capacity within a simulated household/community environment. Distance walked in six minutes was also measured.
Methods
This exploratory, repeated measures study was approved by the Institutional Review Boards of three academic institutions and a large pediatric health system. Consent and assent forms were reviewed and signed by parents and children, respectively.
Participants
A convenience sample of 10 participants with spastic diplegic CP, ages seven to 13 years, were recruited from local pediatric clinics in a large suburban area. The inclusion criteria were 1) diagnosis of spastic diplegia, Gross Motor Function Classification System (GMFCS) levels I, II, or III 36 ; 2) lacking ankle dorsiflexion to neutral by at least five degrees (mild contracture) with knee extended; 3) knee or hip flexion contracture 10 degrees or less; 4) lower extremity Modified Ashworth Scale scores of two or less in gastrocnemius and hamstring muscles; 5) ability to walk 10 meters or greater at least 20 times; 6) having normal or corrected functional vision; and 7) ability to follow directions in English. Children were excluded from this study if they had 1) undergone surgery in the past six months or received Botox injections in the last three months; 2) other medical diagnoses that could impact their ability to safely participate in testing; 3) scoliosis greater than 25 degrees27,37; or 4) a diagnosis of athetoid, ataxic, or dyskinetic types of CP. 38
Equipment/procedures
Participants were evaluated by an experienced physical therapist and pediatric orthotist. Custom molds of lower legs and feet in non-weight-bearing were taken for both orthotic conditions. Careful alignment of the hindfoot and midfoot was attempted in all orthotic molds to maintain optimum tri-planar bony alignment of the foot in addition to consideration of symmetry, height, weight, and activity level. In the OSKAR AFO, orthotic design was guided by OSKAR algorithms to optimize the angle of the ankle based on assessment of muscle tone and muscle length of the gastrocnemius. 15 Custom molds for standard AFOs were casted with a 0-degree or plantigrade ankle angle.
Over a two-week period, OSKAR AFOFCs and standard AFOFCs were fabricated in an orthotic laboratory. Both types of AFOs were a fixed design and made from polypropylene plastic with original, uniform thickness of materials ranging from 0.125 to 0.1875 inches based on individual height, weight, and anticipated stresses applied to the plastic. Following published algorithms, trimlines of plastic were adjusted to provide flexible and rigid design based on the child's gait pattern. 15 For example, a shank angle in midstance with insufficient incline (<5 degrees) requires a more flexible toe plate to reduce the knee extension moment in mid- to late-stance, whereas a shank angle with excessive incline (>15 degrees) requires a more rigid toe plate to create more ground reaction force to facilitate the knee extension moment. 39 Forefoot alignment was assessed to optimize alignment and control of the midfoot and hindfoot in the AFO. Participants with a rigid forefoot varus required accommodative forefoot posting to provide stability and maintain midfoot and hindfoot alignment.
Participants returned to the orthotic clinic and were fitted with OSKAR and standard orthoses and footwear (Figure 1). Billy high top shoes were provided as footwear in this study as soles are flexible and all sizes have a firm heel counter with a similar durometer for ease of modification, and the high-top shoe design easily accommodates AFOs. 40
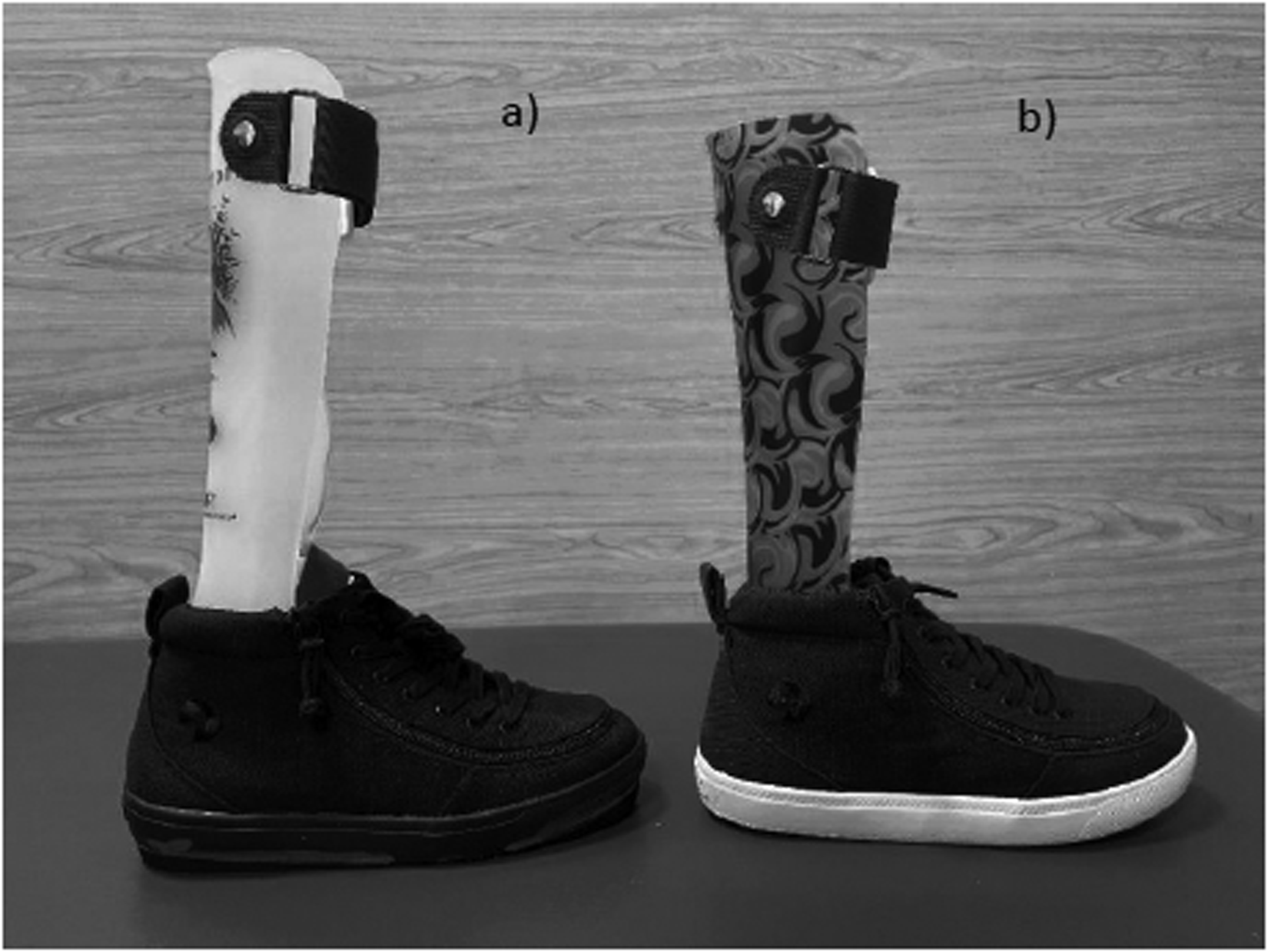
AFOFCs worn in study. (a) OSKAR AFOFCs and (b) Standard AFOFCs. Photos used with permission (K. Barner, CPO, personal communication, January 26, 2024). AFOFC: ankle foot orthosis-footwear combination; OSKAR: optimal segment kinematics and alignment approach to rehabilitation; CPO: certified prosthetist orthotist.
The OSKAR AFOFCs were tuned using video analysis to evaluate SVA in midstance. Internal and/or external heel lifts were added to the shoes with a goal of achieving 10 to 12 degrees of shank incline to align the knee vertically over the middle of the foot. Participant videos were viewed in standing and walking. OSKAR AFOFCs were then adjusted, or tuned, to achieve an optimal SVA that facilitated shank angles and trunk alignment close to typical in the sagittal plane. Some participants required sole modifications on the shoes to promote optimal transitions into and out of midstance 15 (Table 1). The standard AFOFCs were fabricated to achieve a 90-degree (plantigrade) fixed AFO ankle angle with no tuning and a 0-degree SVA. If needed, adjustments were made in both AFOFC conditions to equalize leg length/foot length and match the “A” or “B” design noted in the OSKAR algorithm. 41
Physical exam results and OSKAR AFOFC design.
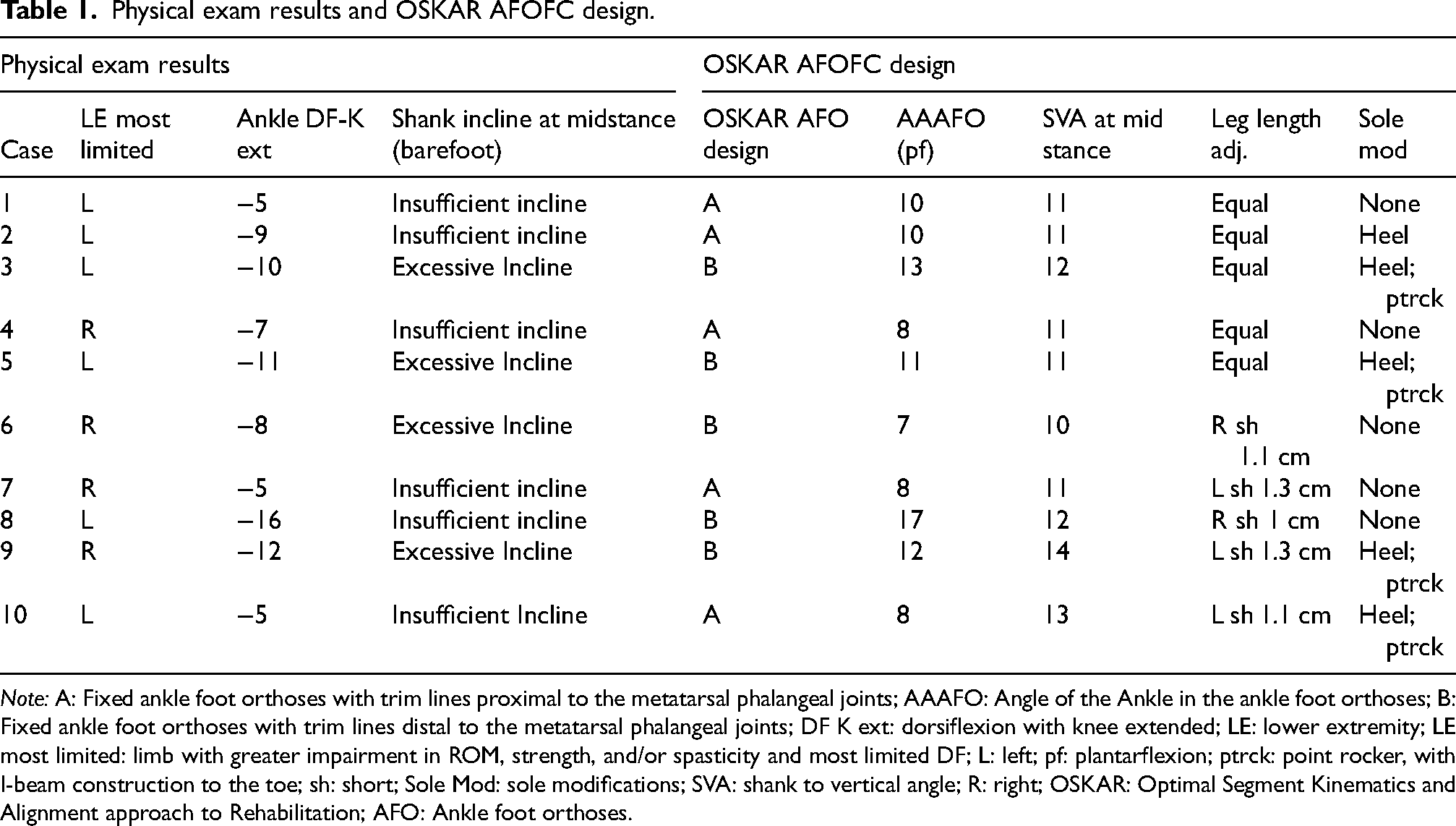
Note: A: Fixed ankle foot orthoses with trim lines proximal to the metatarsal phalangeal joints; AAAFO: Angle of the Ankle in the ankle foot orthoses; B: Fixed ankle foot orthoses with trim lines distal to the metatarsal phalangeal joints; DF K ext: dorsiflexion with knee extended; LE: lower extremity; LE most limited: limb with greater impairment in ROM, strength, and/or spasticity and most limited DF; L: left; pf: plantarflexion; ptrck: point rocker, with I-beam construction to the toe; sh: short; Sole Mod: sole modifications; SVA: shank to vertical angle; R: right; OSKAR: Optimal Segment Kinematics and Alignment approach to Rehabilitation; AFO: Ankle foot orthoses.
Once participants were fitted with their AFOFCs, the two sets of orthoses and shoes were marked with different stickers for distinction. To randomize the order of the brace conditions for data collection, participants chose a sealed envelope containing a matching sticker for the corresponding orthotic condition that would be worn first. Participants were assessed in both orthotic conditions using the following function-based outcome measures: 1) PBS, 2) Standardized Walking Obstacle Course (SWOC), and 3) Six-Minute Walk Test (6MWT).
The PBS was created from the Berg Balance Scale, a functional outcome measure used with adults. 42 The PBS includes 14 items reflecting static and dynamic balance—sitting balance, standing balance, sit to stand/stand to sit, transfers, stepping, reaching forward, reaching to the floor, turning and stepping on/off an elevated surface. Scores for each item are recorded on a 5-point Likert scale (0 to 4) for a maximum score of 56. Test-retest reliability of the PBS is extremely high (intercorrelation coefficient [ICC] [3,1] = 0.998) as is inter-rater reliability (ICC [3,1] = 0.997) in children with motor impairments. 43 Chen et al. have validated its use for assessment of balance in children with CP.21,44–48 Participants performed the PBS in an 8’ × 8’ space in an exercise lab on a hard tile floor. All 14 items were administered using the supplies listed on the scoring form, following the instructional steps for each item. The highest score out of three attempts on each item was recorded on the PBS scoring sheet to calculate the total score.
The SWOC examines function within different environmental conditions that simulate real-life situations. It requires walking on a short, turning path under different conditions. The walkway has three directional turns and participants must step over an axillary crutch and walk around a trash can. There is also a visually stimulating mat and a shag rug to walk across. An armchair is placed at one end of the walkway and a bench without arms is placed at the other end, both adjusted to a height that provides the participants with 90 degrees of hip and knee flexion in sitting. High inter- and intra-rater reliability have been reported for recorded times on the SWOC (ICC 0.99 and ICC 0.83–0.97, respectively). The SWOC demonstrates good concurrent validity with the Timed Up and Go for use with children, with significant correlations (p < 0.05) for time. Scores are reported as the amount of the time (seconds) needed to complete the course. Additionally, number of steps to complete the course and number of steps off the course are counted for each pass. Three conditions are assessed: 1) typical walking, 2) walking wearing sunglasses, and 3) walking holding a lunch tray. 49 The SWOC was performed in a large, open space on a marked course. Participants completed two trials for each condition to achieve an average score. All walks were timed and scored using video recordings.
First used in children with severe cardiopulmonary conditions, the 6MWT is a sub-maximal walking test of functional exercise capacity. 50 Participants are instructed to walk at a self-selected speed for six minutes, with administrators counting laps and/or measuring distance. Standardized instructions for test administration are provided as well as approved statements of encouragement. Participants are allowed to slow down, stop, or rest as needed; however, the timer continues. 51 Excellent test-retest reliability was noted on the 6MWT (ICC = 0.98),52,53 as well as validity (r = 0.948; p < .001) and reproducibility (r = 0.87; p = .007; ICC = 0.80) in children with CP. 54 Reference values for the 6MWT in children with CP have been recorded.38,55,56 A 30-meter track was created on a compressed rubber floor to conduct the 6MWT. Participants were instructed to walk around the course at a self-selected speed with a goal of walking as far as possible in six minutes. At the end of six minutes, walking distance was recorded in meters. The 6MWT was administered only once in each condition.
Data analysis
IBM SPSS Statistics for Windows, version 28, was used to perform statistical analysis. Descriptive statistics were calculated for participant characteristics and outcome measures (see Tables 2 and 3). Continuous variables were inspected for normality, outliers, and missing data. Non-normal distributions were noted within the PBS and SWOC data sets when viewing histograms and there were several significant Kolmogorov-Smirnov values. However, skewness and kurtosis were acceptable (<±2). 57 One outlier was found: Case 10 in the ordinary SWOC data. The outlier was included in the analysis because the corresponding z-value (2.24) was not extreme and, with the small number of participants, it was important to include all cases.58,59
Participant characteristics.
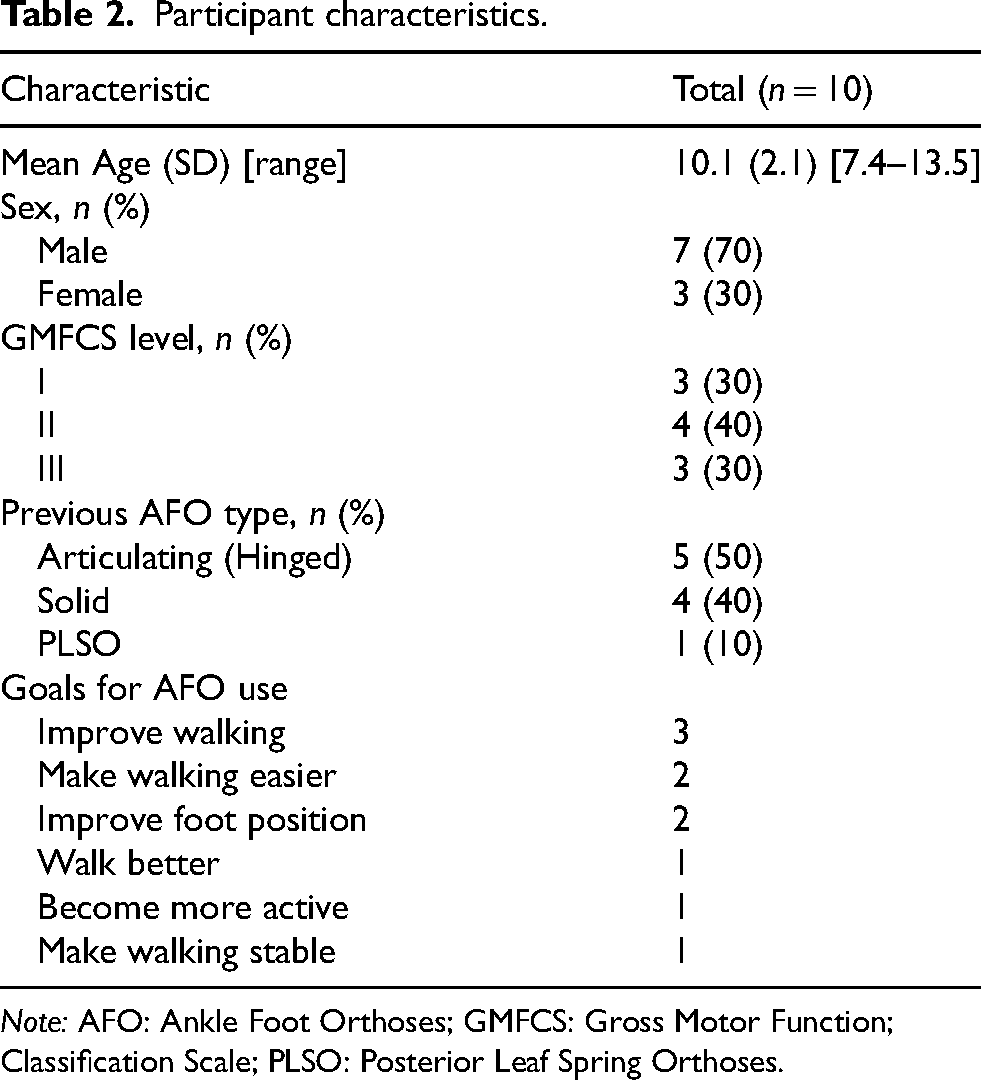
Note: AFO: Ankle Foot Orthoses; GMFCS: Gross Motor Function; Classification Scale; PLSO: Posterior Leaf Spring Orthoses.
Summary statistics for outcome measures (dependent variables).
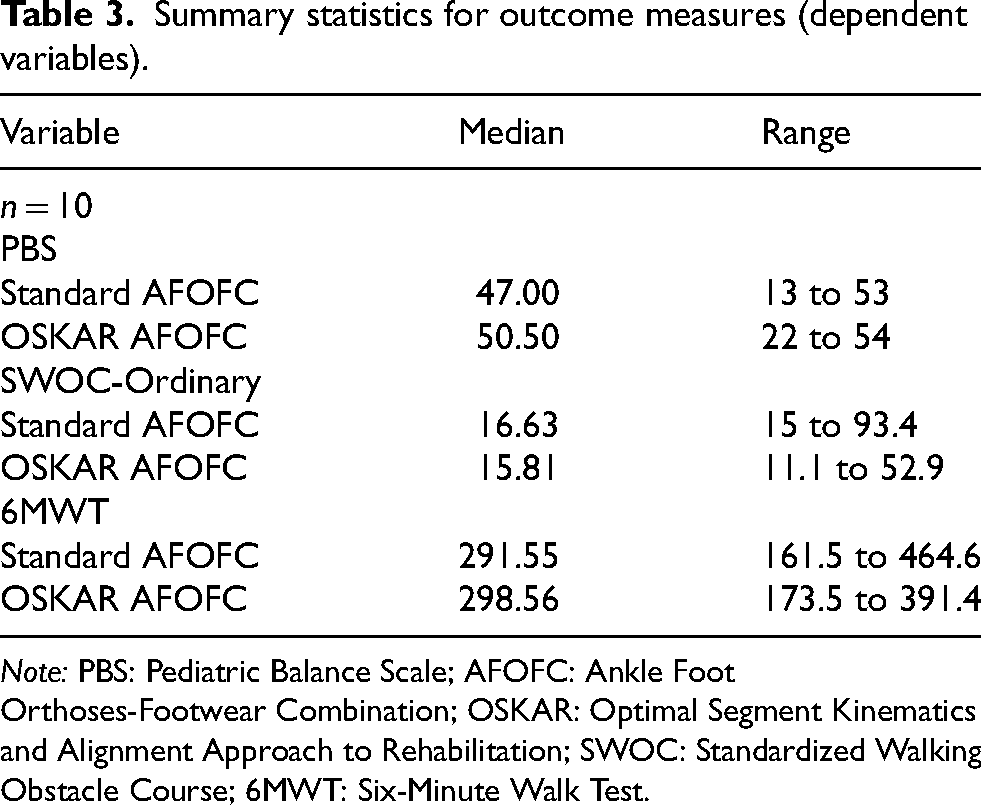
Note: PBS: Pediatric Balance Scale; AFOFC: Ankle Foot Orthoses-Footwear Combination; OSKAR: Optimal Segment Kinematics and Alignment Approach to Rehabilitation; SWOC: Standardized Walking Obstacle Course; 6MWT: Six-Minute Walk Test.
Due to the small sample size and normality violations noted upon data examination, non-parametric analysis was performed using Wilcoxon signed rank test. 60 An alpha level of ≤0.05, two-tailed, was used to identify significant differences. Effect sizes for quantitative variables were calculated using r. 61 Scores from the PBS and 6MWT were analyzed for all participants. The mean time of the two trials for the ordinary SWOC walk was used for analysis as all participants were able to complete this condition successfully. Participants who required an assistive device could not complete the tray-walking activity (n = 4), and scores in the sunglasses walk showed little to no variation between conditions.
Results
Significant differences in PBS scores were found between the two AFO conditions with greater total PBS scores recorded when wearing OSKAR AFOFCs (median [Mdn] = 50.50), versus wearing standard AFOFCs (Mdn = 47.00), p = 0.034. Differences in total scores on the PBS (3.50) did not exceed the minimally clinically important difference (MCID) of 5.83. However, three of the 10 participants exceeded the MCID for the total PBS score in children with CP. Additionally, the MCID for PBS static scores (2.92) was surpassed by two participants, and four participants exceeded MCID for PBS dynamic scores (2.92). 44 There were no significant differences in scores on the SWOC or the 6MWT in the two orthotic conditions. Although nonsignificant, median walking time on the SWOC was slightly lower (faster) in the OSKAR AFOFCs (15.81 s) compared to standard AFOFCs (16.63 s). Distances for the 6MWT were similar, but slightly longer for OSKAR AFOFCs—298.56 meters for the OSKAR condition and 291.55 meters for the standard AFOFCs (Outcome data is summarized in Table 4, with individual case data exhibited in Figures 2, 3, and 4.).
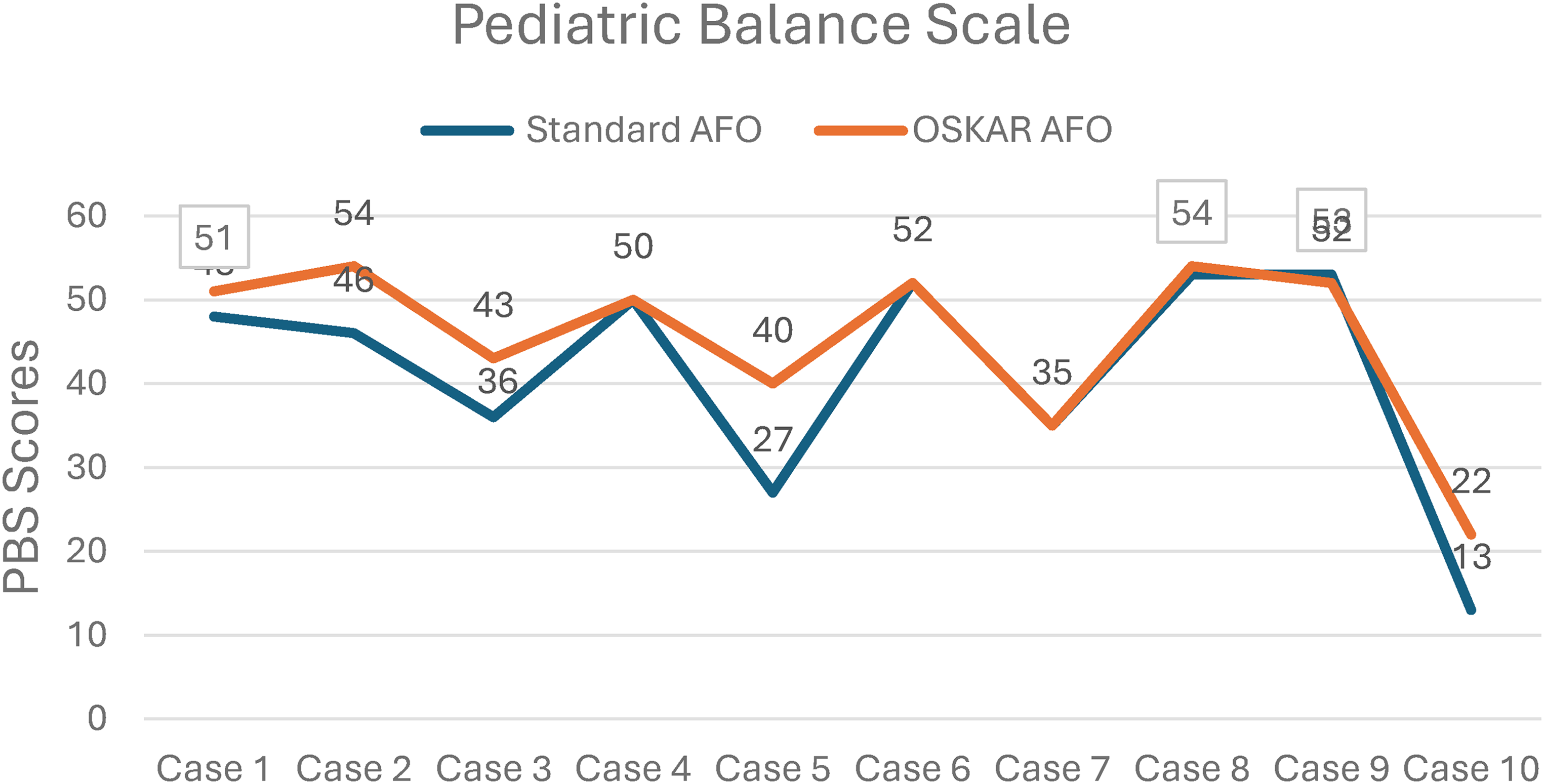
Total scores on the pediatric balance scale by case. AFO: ankle foot orthosis; OSKAR: optimal segment kinematics and alignment approach to rehabilitation.
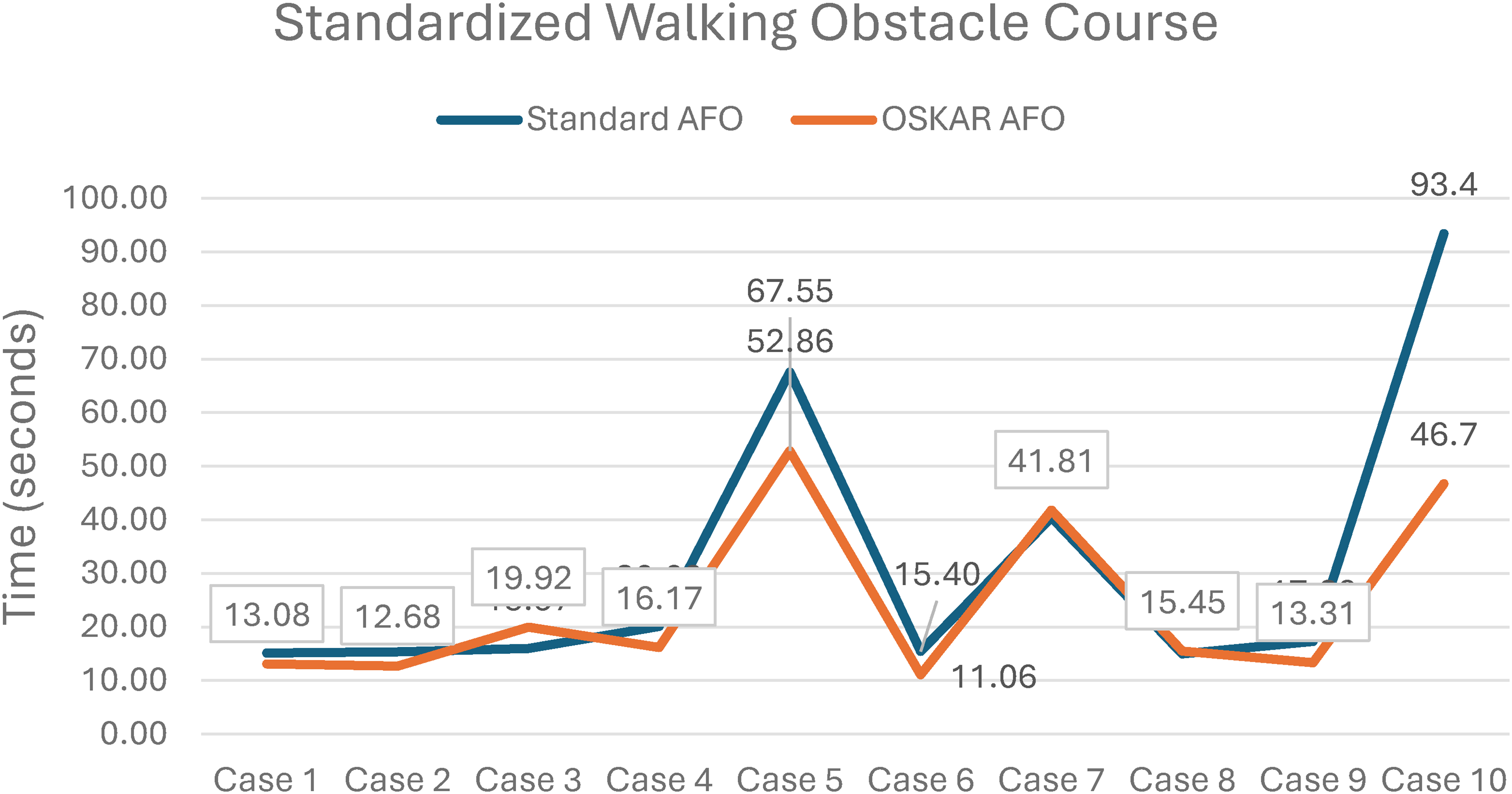
Mean walking time on the standardized walking obstacle course by case. AFO: ankle foot orthosis; OSKAR: optimal segment kinematics and alignment approach to rehabilitation.
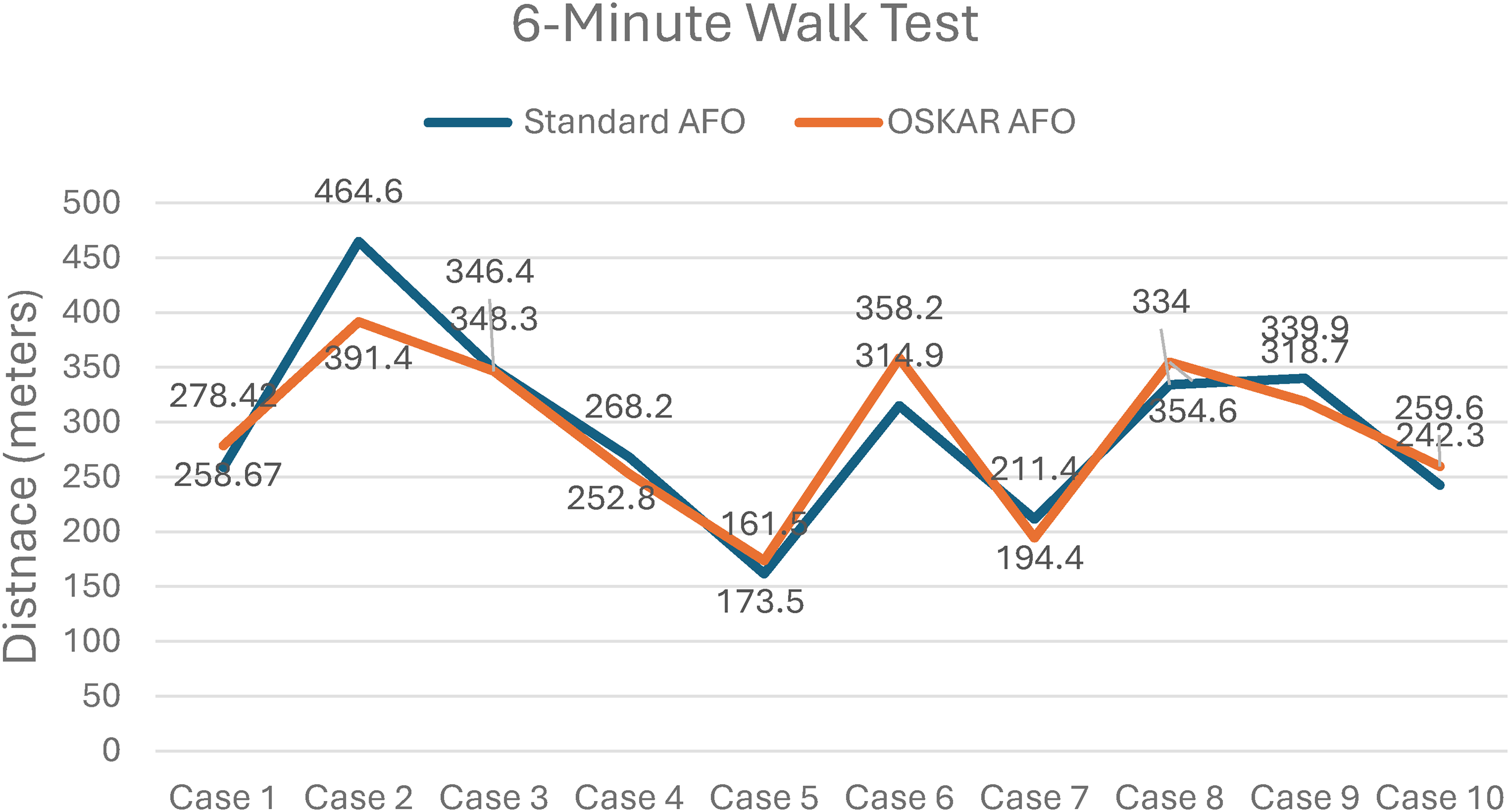
Mean walking distance on the six-minute walk test by case. AFO: ankle foot orthosis; OSKAR: optimal segment kinematics and alignment approach to rehabilitation.
Summary of results from Wilcoxon signed-rank tests.
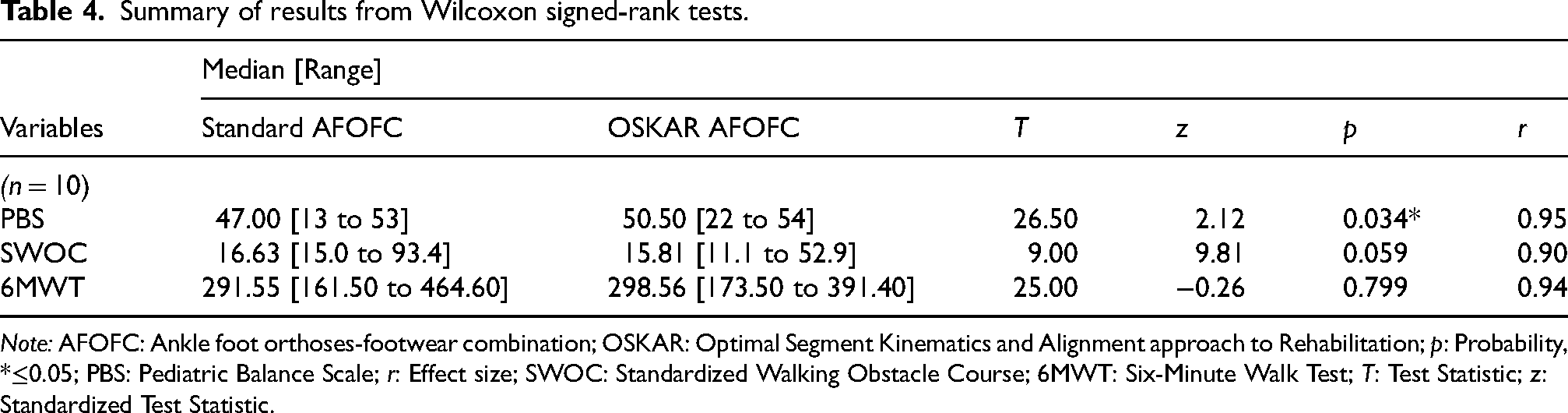
Note: AFOFC: Ankle foot orthoses-footwear combination; OSKAR: Optimal Segment Kinematics and Alignment approach to Rehabilitation; p: Probability, *≤0.05; PBS: Pediatric Balance Scale; r: Effect size; SWOC: Standardized Walking Obstacle Course; 6MWT: Six-Minute Walk Test; T: Test Statistic; z: Standardized Test Statistic.
Discussion
This exploratory study examined functional outcome scores of children with CP when wearing two different orthoses—AFOFCs designed using the OSKAR method and standard AFOFCs with a plantigrade, or neutral, position of the ankle. Participants were assessed using the PBS, SWOC, and 6MWT. Results indicate that wearing AFOFCs designed using the OSKAR method may positively affect balance scores.
Findings from this study are similar to results from other research that evaluated balance when wearing AFOFCs designed using the OSKAR method versus wearing standard AFOFCs. Bjornson et al. noted significantly greater PBS scores after wearing OSKAR AFOFCs for three months and PBS scores exceeded the MCID of 5.83. 21 In the present study, mean change in PBS scores may not have reached the MCID because of the cross-sectional design of the methods. Scores were collected on the same day the participant received the AFOFCs, which did not allow time for potential functional change that may have occurred in response to the orthotic design.
There was a large effect size associated with the significant finding in the total PBS scores (r = 0.95). Effect size for comparison of PBS scores in this study were higher than effect sizes in similar studies involving AFO use in children with CP.62,63 While the effect size suggests a potentially meaningful relationship, replication with a larger cohort is necessary to confirm the robustness of this finding. 58
Investigators in the present study surmised that improved PBS scores when wearing the OSKAR AFOFCs could be attributed to careful attention to segmental alignment in the OSKAR AFO-footwear prescription. In a similar study of children with CP, researchers found that wearing AFOs designed using the OSKAR method reduced loss of balance in standing. 37 There is evidence that impaired balance significantly affects activities of daily living in children with CP. 64 Orthoses that improve balance in upright could promote greater independence, participation, and safety. Results from the present study support current evidence that AFOFCs designed using the OSKAR method may positively affect functional balance.
The authors found no studies that compared different orthoses using the SWOC. Kott and Held examined the influence of walking in orthoses versus barefoot in children with CP using the PBS and the SWOC and found no significant differences. 65 No descriptions of the type or design of the orthoses worn in the study were provided 65 ; however, average SWOC walk times wearing orthoses were very similar to median walk times in the present study.
The lack of differences in SWOC times may be due to several factors. First, participants did not have any time to acclimate to the new AFOFCs in either condition, which did not allow a transitional period to recognize any possible functional changes that might occur over time. Second, the variability in functional ability of the sample could have contributed to the lack of differences. Participants were observed to walk at their self-selected, comfortable speed, potentially demonstrating habituation of their familiar walking pattern. 66 Another possible influence of walking speed could be a feed-forward system of locomotion evidenced by the central pattern generator phenomenon. Thought to elicit rhythmic coordination of muscle activity, central pattern generators influence reflex activity during phases of walking. Consistent afferent input over time facilitates or inhibits alpha motor neurons to produce predictable patterns of movement 67 and could override potential impacts of a new orthotic design. Third, there is limited research using the SWOC with pediatric populations,49,65 indicating a potential lack of evidence about the measure's sensitivity to detect differences and provide a framework for comparison of results. Alternative assessments of dynamic gait function may need consideration in future research.
Interesting anecdotal evidence was gathered from video gait assessment during the SWOC trials. Researchers observed improved segmental and postural alignment in a majority of participants when wearing OSKAR AFOFCs, although alignment was not assessed in this study. Additionally, gait parameters were not measured in this study; however, more visible heel contact and gait rocker activity were observed in the OSKAR condition when compared to gait with standard AFOFCs. The authors hypothesized that observed positive changes in postural alignment and gait parameters could be due to the emphasis placed on optimizing the angle of the ankle to accommodate for shortened gastrocnemius muscle length in the OSKAR method.
Tuning footwear to achieve an optimal SVA could also account for alignment changes observed in the side-by-side video. Previous researchers found that tuning to achieve an optimal SVA directs the ground reaction force through the knee joint, closer to what would be expected in typical gait.21–24,26,39,62,68 With ground reaction forces closer to typical, minimal muscle activity is required to maintain upright posture. 62 This optimized segmental alignment and foot contact could account for the improved fluidity and efficiency of movement observed when walking in the OSKAR AFOFC. Future studies are needed to assess alignment and gait parameters when walking in orthoses designed using OSKAR algorithms versus standard orthotic conditions.
Although the median walking distance on the 6MWT was slightly further in the OSKAR condition, six participants, including two with excessive incline at midstance, walked further in the standard AFOFCs. Inclusion criteria mandated that participants wore standard orthoses in the six months before the study. The long-term use and familiarity with standard orthoses may have contributed to the greater walking distance in this condition. Longitudinal studies are needed that would allow participants time to acclimate to the AFOFCs, which could potentially yield more robust differences.
Results from the 6MWT also could have been influenced by confounding variables, including the order of the AFO condition, level of fatigue, or distractibility during the six minutes. Order of AFO condition may have been a factor as seven of 10 cases walked further in the first condition, four in OSKAR AFOFCs and three in the standard AFOFCs. This may suggest that participants were tired during the second 6MWT. Similarly, fatigue may have impacted the distance walked in the 6MWT in both conditions as all data collection was performed during a single session. Distractibility, common in data collection with children, also may have influenced walking distance during the 6MWT. Future studies should consider collecting data over several sessions for a maximum duration of an hour to reduce the risk of fatigue and potentially improve focus on the task.
Children with spastic CP are unique but often receive standard, plantigrade AFOs (ankle angle at 90 degrees) that contribute to poor biomechanics, undue stress to soft tissues and joints, pain, and mid-foot collapse.8,15,16 Orthotic intervention was listed by individuals with CP, their caregivers, and providers as one of the top 16 desired areas of research. 69 Most conventional orthotic prescriptions are based on incomplete algorithms, or more commonly, observation and non-standardized approaches. 17 A need exists to improve provider knowledge of orthotic assessment and prescriptions, and establish standardized assessments to guide AFO-footwear interventions for children with spastic CP. Biomechanical optimization and tuning of AFOs has been suggested to improve gait and impact function in children with gait impairments.21–24,26,27 Understanding gait biomechanics and typical function provides a blueprint for individualized, effective orthotic prescription and management to optimize walking as close as possible to typical.
Future considerations
Findings from this exploratory study may provide preliminary data for larger, future studies. Exploring functional differences when wearing OSKAR AFOFCs could include any number of outcome measures. Different research designs, such as grouping participants based on gait pattern as well as motor ability, could inform orthotic decisions to enhance body structure/function and activity. Correlations among and between variables such as age, GMFCS level, and functional scores may provide useful data for orthotic use as well as prognostic information. Additionally, longitudinal studies would allow an adequate adjustment period and time for motor learning in new AFOFCs.
Limitations
Potential limitations of this study were identified. The small sample size, although consistent with similar studies, yields low statistical power to generalize results to related populations. 70 Recent research involving AFOs designed following the OSKAR algorithms included samples of five to 19 children with CP.21,22,26,27 Variability of symptoms and functional ability, which is well-documented in children with CP, possibly influenced results despite attempts to limit this study to ambulatory children with CP and use a repeated measures design.58,63 Additionally, this cross-sectional, single-session design did not afford participants the time to adjust to the new AFOs and there was no adjustment for multiple comparisons. Children received AFOs on the same day as data collection to improve consistency of comparisons and reduce the impact of attrition; however, the lack of any AFO adjustment period possibly affected outcomes. There is also the possibility of a carryover effect as both orthotic conditions were assessed on the same day during the same session, not allowing for a “washout” period.58,62
Inclusion criteria dictated that participants had been using plantigrade AFOs for the past six months. Habituation from previous AFO use could have impacted walking patterns, selective motor control, alignment, balance, and gait efficiency in the new AFOs, all of which possibly influenced results. 66 There could have been some measure of acclimation to the new orthoses that occurred during data collection, which lasted between one and two hours, potentially impacting functional ability at the latter portion of data collection. Fatigue was also a factor as participants presented with different levels of walking ability and endurance. Several participants had slight difficulty completing the second 6MWT. Because all data were collected in a cross-sectional design, longitudinal effects of AFOFCs on function were not examined in this study.
Conclusion
This study provided evidence that optimizing orthoses using the OSKAR method may improve balance in children with CP. Understanding the effects of different AFOFCs on balance and walking capacity in children with spastic CP is important as functional ability can influence participation in daily life.46,71 Clinicians are encouraged to explore decision algorithms from evidence-based guidelines and advance their knowledge of orthotic prescriptions for children with CP. Additional training and collaboration among therapists and orthotists regarding orthotic prescriptions could provide clients with optimal segmental alignment. This could affect overall function when wearing AFOs. Generalizations of the results of this exploratory study are limited, but findings could provide insights for future research. Larger studies are needed to investigate the impact of OSKAR AFOFCs using additional functional outcome measures.
Footnotes
Acknowledgements
Many thanks to Kennesaw State University for the use of their facilities. Special appreciation goes out to physical therapy students who assisted with research: Travis Irving, Kolsom Lamb, Erin Leatherman, Griffin Lewallen, Erin Roberts, and Selam Tezera. The authors thank all the participants and parents for their willingness to participate in this study. Also, many thanks to Carol Miller, PT, PhD, for her editorial support.
Ethical approval
This study was approved by the Institutional Review Boards of Kennesaw State University, Children's Healthcare of Atlanta, Texas Woman's University, and Philadelphia College of Osteopathic Medicine. Consent and assent forms were reviewed and signed by parents and children, respectively.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by funding from the Research Department at PCOM-GA.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental data
Available upon request from the corresponding author.