
Abstract
PURPOSE:
For children with cerebral palsy (CP) and equinus, the conventional practice of setting the ankle angle in an ankle-foot orthosis (AA-AFO) at 90
METHODS:
Ten children with CP and equinus (15 limbs with AFOs), and 15 typically-developing (TD) children participated. For the children with CP, solid AFOs with iAA-AFOs (range
RESULTS:
Net responses to iAA-AFOs were positive for 60% of limbs and negative for 40%. Knee variables (GVS and peak extension, flexion, and midstance moment) were most positively affected, and foot-floor angle and vertical ground reaction force were most negatively impacted.
CONCLUSION:
Individualized AFO prescription and iAA-AFOs can impact gait biomechanics for some children with equinus, compared to conventionally-prescribed AFOs. Optimizing dynamic alignment for walking may further improve outcomes.
Keywords
Introduction
Cerebral palsy (CP) describes a group of permanent motor disorders resulting from an injury to the developing fetal or infant brain [1]. Amongst children with CP, one of the most common gait impairments is equinus [2] – a condition associated with triceps surae spasticity and static or dynamic contracture, planovalgus or cavovarus foot deformities, and gait impairments. These include excessive stance phase plantarflexion, instability, knee hyperextension, decreased shock absorption, and poor swing leg clearance [3, 4]. Muscle shortening may alter plantar flexor length-tension curves and impair the muscle’s mechanical ability to produce force [3, 5]. Foot deformity and altered biomechanics may cause musculoskeletal stress, strain, and pain (e.g., in feet and knees), affecting long-term ambulation and functional outcomes [3, 6, 7].
Ankle-foot orthoses (AFOs) are often prescribed to improve joint motion and gait patterns for children with equinus. Optimal AFO prescription is a complex and challenging process that aims to match the child’s characteristics (e.g., gait pattern, clinical findings) to the mechanical/design characteristics of the orthosis, such as AFO type (e.g., solid AFOs intended to prevent ankle motion, or articulated and flexible designs which allow motion), and the angle of the ankle in the AFO (AA-AFO) [8, 9, 10]. However, there is a lack of consensus regarding the best AFO type, AA-AFO, and method of clinical decision-making for children with equinus. Some authors recommend either solid or articulated AFOs with partially-defined indications [11]. Others (including a review article) provide more specific guidance – for example, AFOs should fully accommodate gastrocnemius length [9, 12, 13], and that articulated AFOs are contraindicated for children without appropriate gastrocnemius length and stiffness (i.e., resistance to passive stretch due to hypertonicity) to allow
The AA-AFO is another aspect of the AFO prescription that can be individualized. Traditionally, AA-AFOs are set at 90
If the AFO type and AA-AFO do not fully accommodate the length and stiffness/hypertonicity of the gastrocnemius musculotendinous unit, several compensations may occur. Knee extension may be limited at initial contact (IC) or during stance [10, 15, 22], and subtalar pronation may compensate for restricted ankle dorsiflexion. When the subtalar joint pronates, alignment of the talonavicular and calcaneocuboid joint axes allows more dorsiflexion at the mid-tarsal joint compared to when the subtalar joint is neutral or supinated [23]. Without adequate ankle passive range of motion (PROM), the forces applied during dorsiflexion motion are more likely to stretch the small, extensible midfoot ligaments than the Achilles tendon [22]. This makes it difficult to selectively target stretching forces to the ankle joint and suggests that an excessively dorsiflexed AA-AFO (relative to the available PROM) may promote hyperpronation and/or midfoot break, lever arm dysfunction, and future pain [22]. This rationale warrants discussion about inconsistent AFO type and AA-AFO section practices in the literature which inconsistently consider gastrocnemius length [9, 10, 15, 19].
Thus, for children with CP, orthotic intervention may be more effective when AA-AFOs are individualized based on gastrocnemius length and stiffness [8, 10, 19]; however, evidence-based guidelines are lacking [8, 23]. Even when plantarflexed AA-AFOs have been reported (e.g., references [8, 26, 27]), the rationale for determining the specific angles has not been described. Although a clinical algorithm has been proposed to determine the AA-AFO in a solid AFO [26], it has not been experimentally evaluated to date. Despite potential for solid AFO designs to address many of the biomechanical challenges associated with equinus, articulated and flexible designs remain prevalent in conventional prescription practices, habitually preferred by clinicians who assume they promote function and a more natural gait pattern [27, 28]. Therefore, this study compared the effects of two AFO conditions on gait for children with CP and equinus: 1) solid AFOs with optimized static alignment and individualized AA-AFOs (iAA-AFOs) that accommodated gastrocnemius length and stiffness of each involved limb, and 2) the child’s conventionally-prescribed AFOs (“Usual AFOs”). It was hypothesized that, compared to the Usual AFOs, the iAA-AFOs would promote foot and shank segment kinematics (i.e., foot-floor angle and SVA), and knee and hip joint kinematics and kinetics in the sagittal plane that were closer to reference values for age-matched typically-developing children. We did not expect that spatiotemporal values (e.g., velocity) would be impacted.
Methods
Participants
Participants were 10 children with CP (6–18 years; median
The study was approved by the Research Ethics Boards of the Former Regina Qu’Appelle Health Region and University of Saskatchewan. All children provided informed assent and parents/guardians provided informed consent to participate.
Procedures
Clinical assessment and determination of individualized AA-AFO
A registered physiotherapist with 15 years’ pediatric rehabilitation experience (KJK) assessed each child’s lower limb alignment, gait, ROM, and tone [21, 29, 30]. AA-AFOs were determined according to a clinical algorithm [10, 21, 26]. Accordingly, as a proxy for gastrocnemius musculo-tendinous length, ankle dorsiflexion PROM was measured with the knee extended and the foot in fully pronated, neutral, and supinated positions. The most restricted measurement determined the iAA-AFO; the angle was further plantarflexed if necessary to optimize triplanar bony alignment of the foot or if excessive force was required to overcome gastrocnemius stiffness to maintain this optimal bony alignment [10, 21, 26]. Ankle dorsiflexion ROM in knee flexion was also assessed to compare the influence of the soleus and gastrocnemius (Appendix B). Dorsiflexion PROM was measured using an iPad (Apple Computers, Inc., Cupertino, CA, USA) and the goniometry application (DrGoniometer, CDM S.r.L, Este, Italy) shown to have a degree of reliability comparable to traditional goniometry [31]. The Gross Motor Function Classification System (GMFCS) [32] was used to classify the motor abilities of each participant with CP.
Orthoses and footwear
For all children in the CP group, solid AFOs with iAA-AFOs were fabricated from 3/16” polypropylene according to standard practice of the orthotics department, with ankle trimlines anterior to malleoli. Apart from the AA-AFO (which was individualized according to the clinical examination), the design of these solid AFOs was standardized as much as possible to reduce the number of confounding variables without excessively impairing the child’s gait pattern. Each orthosis had tibial and ankle straps, and trimlines distal to metatarsophalangeal joints. The orthotist added an ethylene-vinyl acetate (EVA) heel wedge equal to the child’s iAA-AFO to create a vertical bench alignment (i.e., vertical alignment of the calf segment of the AFO with the AFO standing upright; Fig. 1). Also, the orthotist assessed the bench alignment according to standard practice, estimating a straight line along the calf segment of the AFO between the projected location of child’s lateral malleolus and fibular head. The physiotherapist (KJK) measured the ankle angle of each iAA-AFO to confirm that it matched the ROM measurement used to determine the iAA-AFO within 5
Photo of AFO with vertical bench alignment and the ankle angle in the AFO (AA-AFO) in 25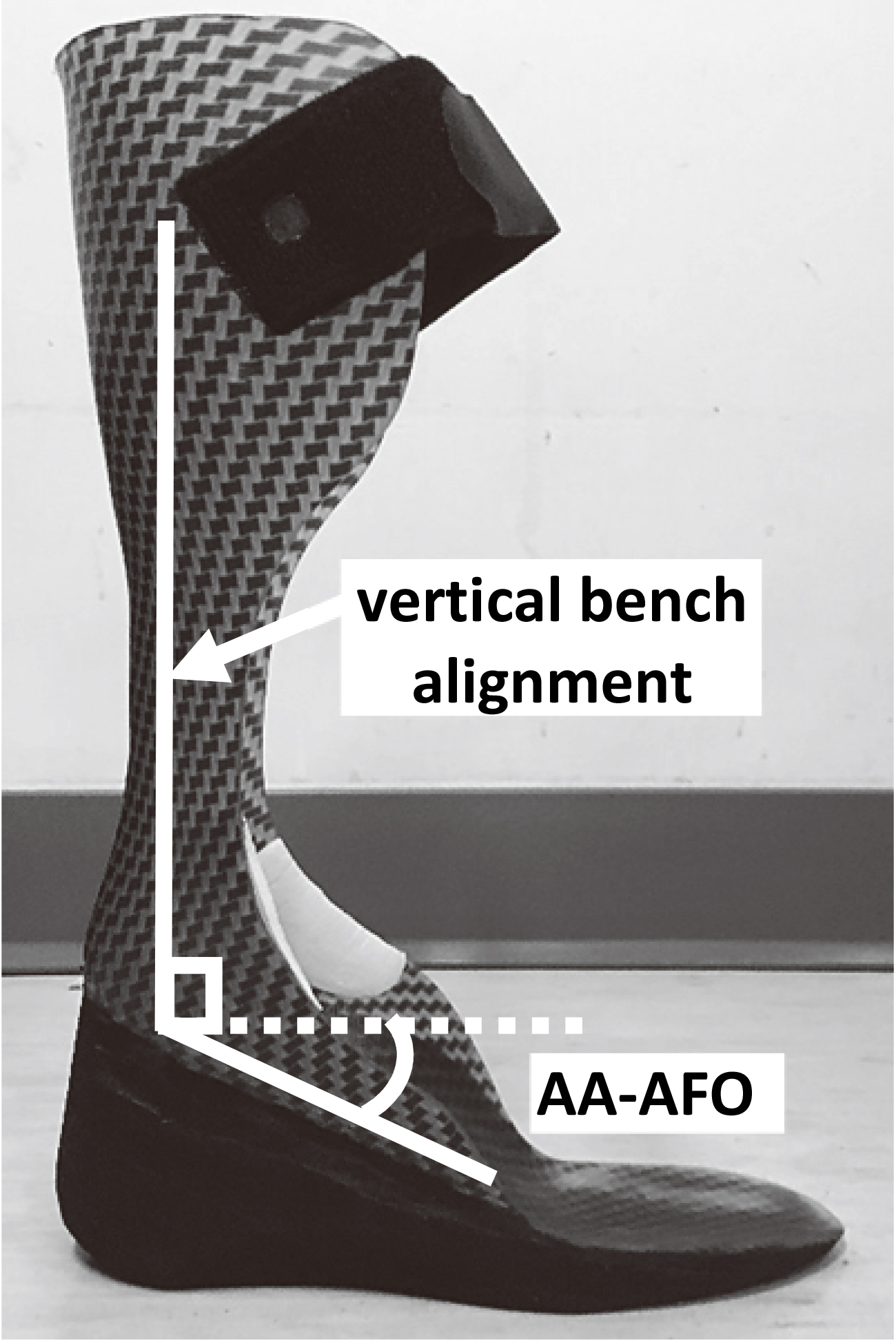
To reduce footwear-related gait variation, all participants except one wore Rebound mid-top skate shoes (DC Shoes, Inc.) in both orthotic conditions. These shoes had a 0 mm heel-sole differential (HSD) and were deep enough to accommodate multiple heel wedge heights. Participant 10 wore New Balance 636 shoes with 5 mm HSD (New Balance, Boston, MA, USA) due to discomfort in the study shoes. Shoes were laced securely to minimize AFO motion.
Each AFO-FC was statically aligned by the first author prior to gait testing. Participants stood on a force plate (50.8 cm
Screen shot of shank to vertical angle (SVA) measurement using DrGoniometer app. Photo shows the AFO from Fig. 1 in a statically aligned AFO-footwear combination (AFO-FC). Labels indicate location of wedge (used to adjust SVA) and point loading rocker (PLR). SVA is measured as the angle between the dashed line along the anterior tibia on the app and vertical (i.e., 9.4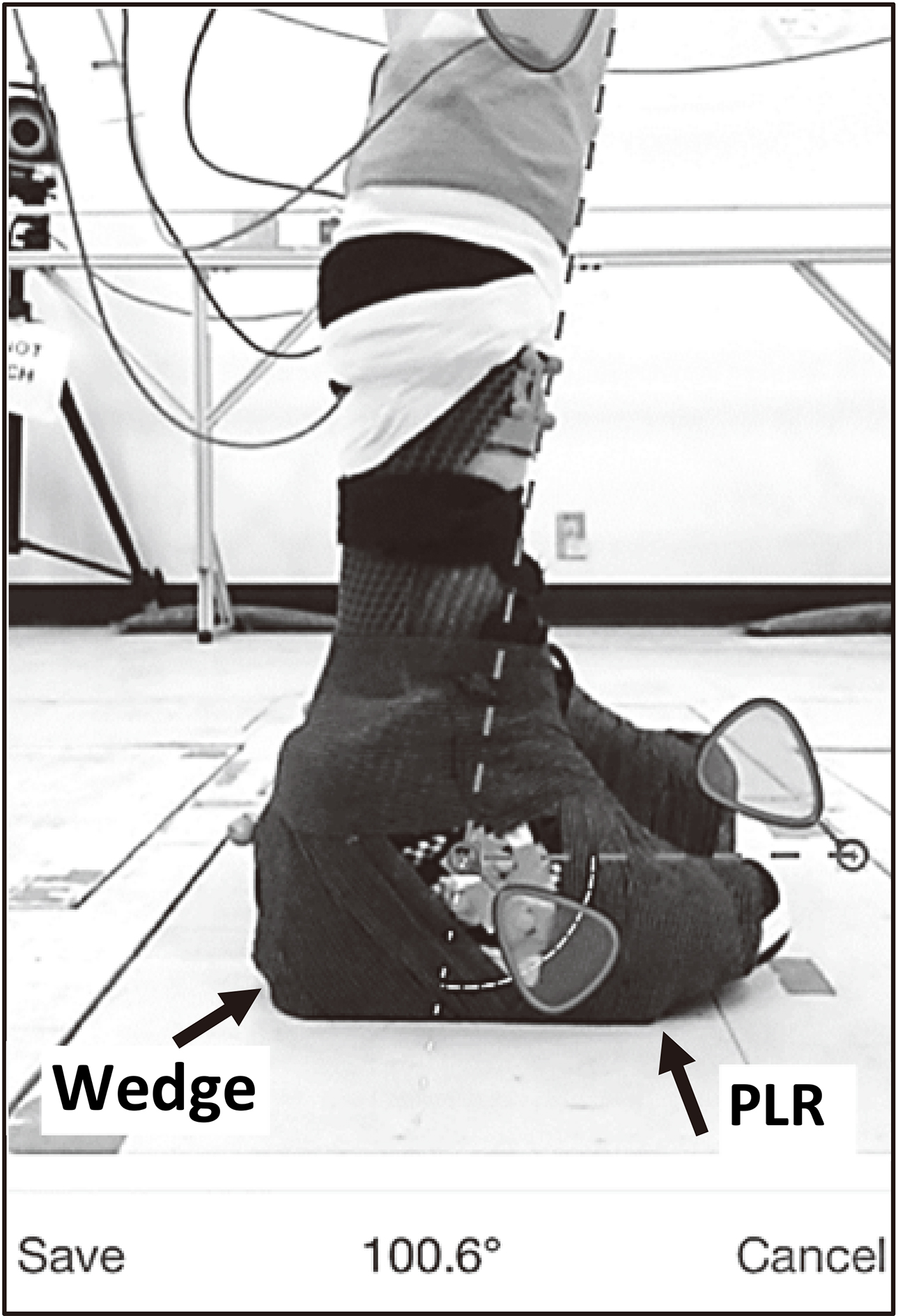
Variable names and descriptions for stance phase kinematic and kinetic variables
Note: Children with bilateral CP wore orthoses on both legs, and children with unilateral CP wore an AFO on the affected limb. F: Female; M; male; y: years; m: months; GMFCS: Gross Motor Function Classification System [29]; DF: Dorsiflexion range of motion (measured with knee extended); n/a
Characteristics of participants with CP
Note: Children with bilateral CP wore orthoses on both legs, and children with unilateral CP wore an AFO on the affected limb. F: Female; M; male; y: years; m: months; GMFCS: Gross Motor Function Classification System [29]; DF: Dorsiflexion range of motion; n/a
Three-dimensional lower limb kinematics were collected using an 8-camera motion capture system (Vicon Nexus, Centennial, CO, fs
Shoe and foot, defined as two different coordinate systems, were both tracked with the same shoe-based marker cluster. The shoe coordinate system was generated from a static pose with the dorsal axis aligned vertically and the medio-lateral axis perpendicular to the plane defined by the dorsal axis and the heel-to-toe vector. The foot coordinate system was then established by rotating the shoe coordinate system about its medio-lateral axis based on the AA-AFO and any attached heel wedges. For the TD participants, shoe and foot coordinate systems were coincident.
Ankle joint kinematics were defined as the relative angle between shank and foot coordinate systems. SVA was calculated between the long axis of the shank and vertical axis in the sagittal plane. Foot-floor angle was defined between the heel-toe axis of the shoe coordinate system and horizontal plane.
Kinematic and force plate data were combined using standard inverse dynamics techniques [34] to calculate 3D joint moments for the ankle, knee, and hip. Segment parameters for inverse dynamics calculations were estimated using published data [35].
Analyses
Motion analysis data were processed and visually inspected using Vicon Nexus 2.0 (Centennial, CO, USA) and custom routines in MATLAB R2017a (MathWorks, Natick, MA, USA). Stance phase data from three to six trials were ensemble averaged for each affected limb and condition and for each TD participant. Kinetic data were not collected for participant 9 because short step lengths precluded force plate contact with only one foot. Data from TD participants were combined into three age-bands (6–8, 10–13, and 15–18 years).
Peak ankle, knee, and hip kinematics and joint moments and individual gait variable scores (GVS) [36] were calculated for the entire stance phase (Table 1). GVS, a gait quality index, was calculated as the mean root-mean-square difference between each trial of the child’s stance phase data and the mean of the appropriate TD age-band group stance phase data. The GVS was selected due to its potential to provide more information about changes in the variables of interest [37], an advantage over global gait indices which have not demonstrated adequate sensitivity or specificity to detect changes with orthotic intervention [38].
Because of wide within-sample variability, group means were not emphasized [39]. For the children with CP, data for each affected limb during stance phase were analyzed visually using descriptive statistics. For each limb, the mean, SD, and confidence interval (90%CI) were calculated for Usual AFO and iAA-AFO conditions. A difference between conditions was defined as no overlap of 90%CIs. Differences were considered to indicate positive responses for the iAA-AFO if iAA-AFO condition values were closer to the mean of TD data than the Usual AFO condition. iAA-AFO values farther from the TD mean than the Usual AFO condition were considered negative responses. Overlapping 90%CIs indicated no difference between conditions (i.e., equivocal). If values for both conditions were within one SD of the TD mean, the results were also considered equivocal (within normal limits). The number of responses in each category (positive, negative, and equivocal) were summed for each limb for all 25 kinematic, kinetic, and spatiotemporal variables combined. Limbs were considered net positive responders if more variables were affected positively than negatively. Conversely, net negative responders demonstrated more negative than positive responses. Cohen’s d was calculated using a pooled SD as an effect size measure quantifying the magnitude of each positive and negative response. Effect sizes of 0.8 or greater were considered large effects [40].
Wilcoxon signed-rank test compared ankle dorsiflexion (Ankle_DF), plantarflexion (Ankle_PF) and Ankle_GVS between conditions to confirm the effectiveness of AA-AFO experimental manipulation. Ankle plantarflexion was reported as negative while dorsiflexion was defined as positive.
Statistical analyses were completed using SPSS Statistics version 24.0 (IBM Corp., Armonk, NY, USA), and MATLAB R2017a (MathWorks, Natick, MA, USA). Statistical significance was set at an
Characteristics of the Usual AFOs and iAA-AFOs, and description of adjustments made during the static alignment process
Characteristics of the Usual AFOs and iAA-AFOs, and description of adjustments made during the static alignment process
AA-AFO: Ankle angle in the AFO; SVA: Shank to vertical angle (optimized and measured in standing); PF: Plantarflexion; DF: Dorsiflexion; SMO: Supramalleolar orthosis; MTP: Metatarsophalangeal joints; PLR: Point loading rocker.
Physical assessment
Physical examination findings for each participant with CP are presented in Table 2 and the Appendix. Median dorsiflexion PROM was
Individual variable response profiles by limb according to net response: A. Limbs with net positive response; B. Limbs with net negative response. Effect size (Cohen’s d) values inside red and green boxes indicate magnitude of positive and negative responses
Individual variable response profiles by limb according to net response: A. Limbs with net positive response; B. Limbs with net negative response. Effect size (Cohen’s d) values inside red and green boxes indicate magnitude of positive and negative responses
Representative knee flexion/extension kinematics for two limbs for both AFO conditions during stance phase (from initial contact to terminal contact): A) positive response (participant 10, right limb); and B) negative response (participant 1, left leg). Shaded area denotes data from age-matched typically developing children 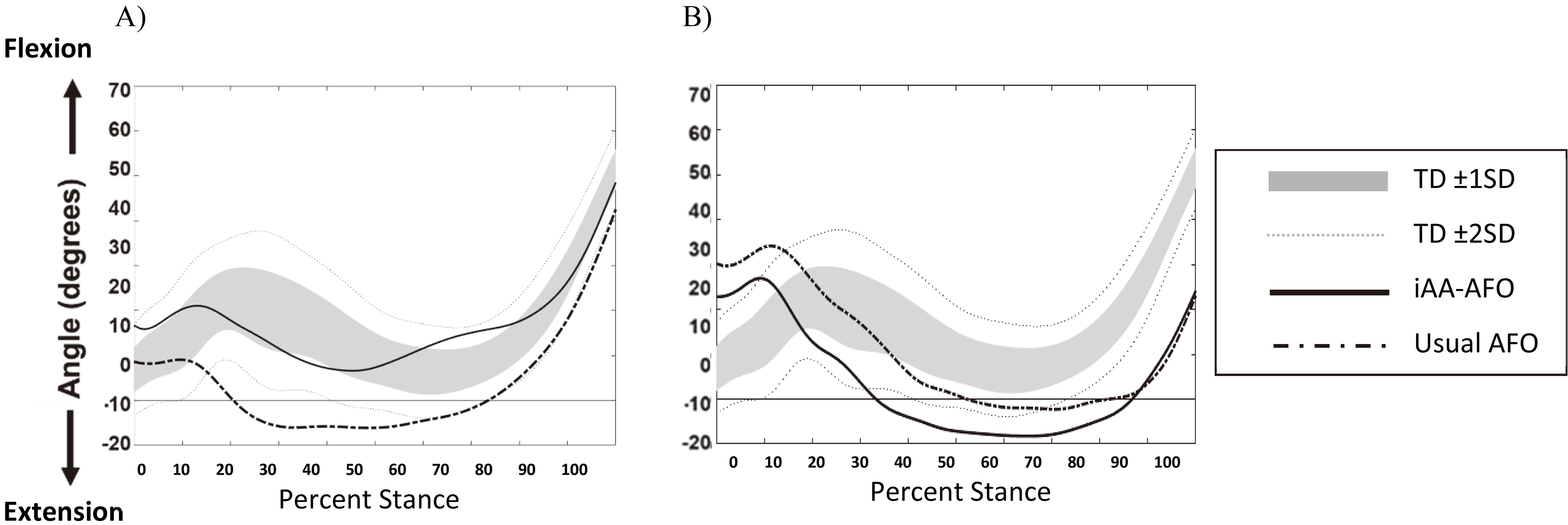
Participants wore orthoses on 15/20 limbs. Table 3 describes the Usual orthoses. All except three Usual AFOs had 0
Kinematics and kinetics
Ankle kinematic variables
Median AnkleDF was 12
Knee, hip, segment, and spatiotemporal variables
Of the 15 limbs, 9 (60%) were net positive responders, 6 (40%) were net negative responders (Table 4). For these 25 variables, 12/15 limbs demonstrated
Variables most often affected positively were: KneeExt (40%), GVS_knee (33%), KneeMom_TMSt (31%), and KneeFlex (27%) (Fig. 3, Table 4, Appendix). GVS for the foot-floor angle (GVS_FFA) (33%), GVS for vertical GRF (GVS_VF) (23%), and HipROM (20%) were most often negatively affected. Spatiotemporal variables were minimally impacted, and effects were greater at the knee than hip. Effect sizes for positive and negative responses ranged from 1.5 to 17.7 and
Discussion
This study evaluated the effects of solid AFOs with iAA-AFOs and optimized static alignment on gait for children with CP and equinus. Results were mixed, with a net positive result for 5/10 children (60% of limbs), a net negative response for 2/10 children (40% of limbs), and one positive and one negative limb response for 3/10 children. While 9/10 children (12/15 or 80% of limbs) had some positive change with the iAA-AFOs, 8/10 children (11/15 or 73% of limbs) also showed some negative change. Although the results suggest that individualized prescription can potentially alter gait mechanics compared to conventionally prescribed AFOs, we were unable to identify the factors predicting or contributing to each child’s result. For those limbs that improved, the greatest effects were observed for knee kinematics and kinetics. Positive and negative effects for the hip, FFA, and SVA were observed with equal frequency, while spatiotemporal effects were equivocal. Our hypothesis was therefore partially supported, although the variation in individual responses makes it difficult to generalize about group response [41]. The results may assist clinicians in making more evidence-based, individualized orthotic decisions, and inform future research on this complex topic.
These results highlight potential proximal effects of a statically aligned solid iAA-AFO that considers gastrocnemius length and stiffness. The most frequently observed benefits – namely, more typical knee kinetics and kinematics at initial contact and throughout stance phase – may have important implications, given that many interventions for children with CP target knee ROM and gait kinematics. It is difficult to draw conclusions about the specific biomechanical differences between the Usual AFOs and iAA-AFOs, due to the variety of Usual AFO designs worn by participants and the individualized adjustments involved in statically aligning the iAA-AFOs; but in the iAA-AFO condition, it is likely that the solid AFO design and the individualized AA-AFOs both impacted gait outcomes. The solid iAA-AFOs may have facilitated better control of the GRF relative to the knee (and therefore, better control of shank and knee kinematics) in comparison to the more flexible Usual AFOs. At the same time, the iAA-AFO may have affected dynamic ankle and knee joint coupling; similarly, increased knee extension at initial contact has been observed after gastrocnemius-soleus tenotomies for equinus [42].
In practice, AFO-FC prescription is an iterative, multidisciplinary process [28], involving a series of opportunities for assessment, gait training, and biomechanical adjustments to the AFO-FC. Although the static alignment of the AFO-FCs was optimized during standing, limbs that responded negatively to the iAA-AFO might have benefitted from further AFO-FC tuning to optimize alignment for walking. While most participants demonstrated gait patterns that have been classified as amenable to tuning (e.g., knees extended and
Adequate AFO stiffness also influences proximal mechanics [18, 44]. Although the solid AFOs were intended to prevent ankle motion, visual analysis of ankle joint kinematics in this study suggested that most solid AFOs were not stiff enough to maximize SVA control and optimize proximal effects. For some participants, excessive ankle plantarflexion at loading response (
The ubiquity of the 90
These results suggest that AFO prescription is more complex than the literature portrays. Recommendations based on gait pattern or topographical distribution may imply that orthotic prescription is simpler for children with higher levels of motor function [41]. For example, several authors suggest that articulated AFOs are more effective than solid AFOs for children with hemiplegia [41, 45]. Our results did not substantiate this presumption. However, all three children with hemiplegia who wore articulated AFOs demonstrated a net positive response to the solid iAA-AFO. Our results are consistent with reports that orthotic goals are not preferentially achieved for children in higher functioning (i.e., lower) GMFCS levels [46]; for example, only 57% (4/7) of limbs for children at GMFCS level I responded positively, comprising 44% of the positive responder group. In practice, selection of articulated vs solid AFOs appears inconsistent for children at lower GMFCS levels, while solid AFOs may be consistently recommended for children with more severe motor impairments [27].
Clinical algorithms have been used in medicine since the 1970s to describe and personalize intervention, and reduce trial-and-error decision making [47, 48]. Although clinicians endeavor to individualize AFO prescriptions for children with CP [27], decision-making is complex. Presently, this process is variable and relies on trial-and-error and anecdotal evidence [28], indicating a need for clinical practice guidelines [48]. Similar to other complex aspects of rehabilitation for children with CP (e.g., [44]), algorithms are likely to be valuable in the development of evidence-based guidelines for orthotic intervention.
The algorithm used to determine the iAA-AFO is unique for this purpose; however, as it is based on theoretical justification, clinical experience, and expert opinion, a systematic literature review and further research would help link recommendations with evidence. A future step may be to create an algorithm to guide visual gait analysis for tuning and biomechanical optimization following iAA-AFO fitting.
Limitations
The small sample size (which included children with both hemiplegia and diplegia) and variety of Usual AFO types preclude conclusions about the reasons underlying participants’ responses to the solid AFO with iAA-AFO. Replication with larger samples, comparison only to solid AFOs, and statistical modelling may help to identify factors affecting individual responses and reduce confounding factors such as differences between motor impairment (e.g., between GMFCS levels and unilateral vs bilateral involvement), and in AFO design. Experimental evaluation of the algorithm used to determine the AA-AFO would be beneficial to assess its reliability and validity. For example, the methodology assumes the ankle measurements are a proxy for gastrocnemius length; however, other tissues may be involved as well. Future research on individualized orthotic intervention should examine biomechanical, motor learning, and functional changes with task-oriented training along with the effects on community walking and participation.
Finally, the extent to which the AFOs controlled pronation or midfoot break is unknown. Dorsiflexion PROM was greater with the foot pronated than supinated for 12/15 limbs, and visually, most feet pronated during barefoot gait (Appendix). Uncontrolled pronation and midtarsal joint dorsiflexion may explain how AnkleDF values in the Usual AFOs surpassed clinically measured PROM for many participants. A large lever arm in terminal stance also contributed to stance phase ankle dorsiflexion; however, concomitant motion and chronic strain at joints other than the ankle (e.g., subtalar pronation or midtarsal dorsiflexion) [22, 23] could potentially contribute to long-term foot pain – a prevalent concern for adults with CP [6]. As clinicians may assume that dorsiflexion occurs at the talocrural joint in conventional 90
Conclusion
This study demonstrates that statically aligned solid AFOs with individualized AA-AFOs can impact gait for some children with CP and equinus, compared to conventionally prescribed AFOs. The observed positive and negative effects highlight the complexity of orthotic assessment and prescription, along with the potential to alter gait and address biomechanical goals by individualizing orthotic prescription. In addition to static optimization, objective evaluation to optimize dynamic alignment of iAA-AFOs for walking and consideration of AFO design stiffness may further improve outcomes. Future development of evidence-based guidelines that incorporate clinical algorithms is an important step toward consistent high-quality, individualized orthotic care for children with CP.
Footnotes
Acknowledgments
The authors would like to thank the children and families who participated and the orthotists at the Saskatchewan Abilities Council and Wascana Rehabilitation Centre who assisted with orthotic fabrication and fitting. Thanks also to Ali Bell for valuable statistical consultation and Aaron Awdhan for assistance with motion analysis testing. This work was funded by the Pedorthic Research Foundation of Canada and a joint award from the Physiotherapy Foundation of Canada and the Neurosciences Division of the Canadian Physiotherapy Association. The funders were not involved in any aspect of study design, data collection, analysis or interpretation, or in writing the publication.
Conflict of interest
The authors have no conflict of interest to report.
Appendix
Clinical assessment findings for participants with cerebral palsy: A. Clinical assessment findings for non-weightbearing lower extremity alignment
A.
Child (limb)
Forefoot posture
Foot flexibility
Knee extension PROM
Thigh-foot angle
Femoral anteversion
Duncan ely test
Thomas test
LLD
1 (R)
WNL
Flexible to neutral
yes
WNL
1 cm short
1 (L)
Equinus
Flexible to neutral
0
WNL
WNL
WNL
WNL
–
2 (R)
Moderate MTA
Flexible
0
0
WNL
WNL
WNL
1.5 cm short
3 (R)
Equinus
Fixed
0
WNL
WNL
WNL
2 cm short
3 (L)
WNL
Flexible to neutral
0
WNL
WNL
WNL
–
4 (R)
Severe MTA
Fixed
10
0
Yes
Positive
–
4 (L)
Severe MTA
Fixed
0
5
WNL
WNL
WNL
0.5 cm short
5 (L)
WNL
Flexible
0
0
Yes
WNL
WNL
1 cm short
6 (R)
Equinus
Flexible
0
2
WNL
Positive
1 cm short
7 (R)
Hallux valgus; Mild MTA
Flexible
0
15
WNL
WNL
WNL
1.5 cm short
8 (R)
Severe MTA
Fixed MTA
0
WNL
Positive
WNL
0.5 cm short
9 (R)
Moderate MTA
Flexible
10
0
WNL
WNL
1 cm short
9 (L)
Moderate MTA
Flexible
0
Yes
WNL
WNL
–
10 (R)
Moderate MTA
Flexible to neutral
0
5
WNL
WNL
WNL
–
10 (L)
Moderate MTA
Flexible to neutral
0
5
WNL
WNL
0.5 cm short
B. Modified tardieu scale
Child (limb)
Hip extension
Hip abduction
Hip external rotation
Hip internal rotation
Knee extension
Knee flexion
Ankle DF at 90
Ankle DF at 0
R1
R2
R1
R2
R1
R2
R1
R2
R1
R2
R1
R2
R1
R2
R1
R2
1 (R)
WNL
45
30
30
WNL
45
0
45
WNL
WNL
0
0
1 (L)
WNL
45
30
30
WNL
35
0
50
WNL
WNL
0
2 (R)
50
WNL
25
65
WNL
65
WNL
55
WNL
WNL
0
0
2 (L)
3 (R)
WNL
WNL
WNL
WNL
WNL
35
WNL
WNL
WNL
WNL
5
0
3 (L)
WNL
WNL
WNL
WNL
WNL
45
WNL
WNL
WNL
WNL
WNL
5
10
0
4 (R)
WNL
WNL
WNL
30
WNL
55
WNL
70
WNL
WNL
WNL
5
4 (L)
WNL
WNL
WNL
30
10
40
WNL
70
WNL
WNL
WNL
5
5 (R)
70
70
5 (L)
WNL
WNL
WNL
WNL
WNL
75
WNL
60
WNL
WNL
WNL
WNL
5
6 (R)
WNL
WNL
WNL
WNL
WNL
60
WNL
40
WNL
WNL
WNL
7
6 (L)
7 (R)
WNL
WNL
WNL
WNL
WNL
70
WNL
70
WNL
WNL
WNL
6
0
7 (L)
8 (R)
WNL
WNL
WNL
WNL
WNL
WNL
WNL
WNL
WNL
WNL
15
25
2
8 (L)
9 (R)
WNL
WNL
WNL
WNL
WNL
WNL
WNL
WNL
WNL
WNL
0
0
15
8
9 (L)
WNL
WNL
WNL
WNL
WNL
WNL
WNL
WNL
WNL
WNL
0
0
18
0
10
10 (R)
WNL
WNL
WNL
WNL
WNL
60
WNL
45
WNL
WNL
WNL
10
3
10 (L)
WNL
WNL
WNL
WNL
WNL
50
WNL
50
WNL
WNL
WNL
10
0
R: Right; L: Left; KF: Knee flexion; KE: Knee extension; KHE: Knee hyperextension; DF: Dorsiflexion.
C. Gait observations
Child (limb)
Foot contact and knee posture at initial contact
Foot posture in stance phase
Foot progression angle in stance phase
SVA in stance
Gait classification
1 (R)
Forefoot
Pronation, midfoot break
30
internal
Excess incline
Group V – asymmetrical: Crouch gait on R; True Equinus on L
1 (L)
Forefoot; excess KF
Neutral; mild pronation
Neutral
WNL
2 (R)
Flatfoot
Inversion/supination, midfoot break, excessive pronation
Neutral
WNL
Type 2A – True equinus/plus neutral knee
3 (R)
Flatfoot, foot slap, and KF
Calcaneovalgus, pronates excessively
Neutral
WNL
Group I – True equinus
3 (L)
Heel and mild KF
Mild pronation
Neutral
WNL
4 (R)
Forefoot or flatfoot
Calcaneovarus
Internal
Excess incline
Group IV – Crouch in early to midstance
4 (L)
Heel
Calcaneovarus
Neutral
Excess incline
5 (L) Left
Forefoot
Equinus, inversion, hindfoot varus; rarely achieves heel
Excess incline
Type IV
contact
6 (R)
Flatfoot
WNL
Neutral
WNL
Type 2A – True equinus plus neutral knee
7 (R)
Flatfoot
Cavus with forefoot equinus; pronates excessively
Excess incline
Type 3 – True equinus with jump knee
8 (R)
Forefoot, knee and hip flexion
Supination
Insufficient incline
Type 2B – True equinus/plus recurvatum knee – H
9 (R)
Forefoot, and with KHE
Cavus
Excessive incline
Group III – Apparent equinus
9 (L)
Forefoot
Midfoot break
10 (R)
Forefoot contact and KF
Midfoot break; hindfoot varus; supinates or pronates
Insufficient incline
Group I – True equinus with recurvatum
10 (L)
Forefoot contact and KF
Midfoot break; supination
Insufficient incline