
Abstract
Purpose
The purpose of this study was to quantify quality of life (QOL), workplace bullying, discrimination and harassment among pediatric physiatrists.
Methods
Pediatric physiatrists (N = 389) were invited to participate in an online survey. Demographic data were collected as were the World Health Organization Quality of Life assessment (WHOQOL-BREF), the Negative Acts Questionnaire Revised (NAQ-22), and an adapted version of the Chronic Work Discrimination and Harassment Scale (aCWDHS). Means and standard deviations, one-sided t-tests, chi-squared and ANOVA tests were calculated with the p-value set a priori at 0.05.
Results
The average WHOQOL-BREF score was 76.49/100. Seventeen percent of pediatric physiatrists met the threshold score of 33 for being bullied at least occasionally. The average score on the aCWDHS was 49.31. Disabled pediatric physiatrists reported statistically lower QOL scores (t = 2.356, p = .010), more workplace discrimination and harassment (t = 2.502, p = .010), and more workplace bullying (t = 2.139, p = .022). Low QOL scores were correlated with the scores on the aCWDHS and NAQ-22.
Conclusion
Addressing workplace bullying, discrimination, and harassment could potentially improve the QOL of pediatric physiatrists, especially those with disabilities who report a disproportionate amount of mistreatment.
Introduction
Pediatric physiatrists are physicians dedicated to improving the health and functioning of children with disabilities and typically work at academic medical centers with large catchment areas. 1 The field is primarily made up of women and includes more physicians who identify as being disabled compared to other specialties. 2 Due to the high rates of workplace bullying, discrimination and harassment among physicians,3–6 the purpose of this study was to quantify quality of life (QOL), workplace bullying, and discrimination and harassment among pediatric physiatrists in the United States. The hypothesis was that physicians who identify as women, those from minoritized races or ethnicities, those with disabilities, and those with sexual orientations other than heterosexual would experience more workplace bullying, harassment, and discrimination. Further, it was hypothesized that those who experienced more workplace bullying, harassment, and discrimination would report lower QOL scores.
Methods
As part of a larger study, pediatric physiatrists (N = 389) were invited to participate in an online survey (Institutional Review Board approved in the exempt category) about their practices. Demographic data were collected as were the World Health Organization Quality of Life assessment (WHOQOL-BREF), 7 the Negative Acts Questionnaire Revised (NAQ-22), 8 and an adapted version of the Chronic Work Discrimination and Harassment Scale (aCWDHS). 9 The WHOQOL-BREF is a 26 item instrument that measures QOL in four domains: physical health, psychological health, social relationships, and environment. 7 Each item is scored on a five-point ordinal scale, then the average score is taken for each domain and transformed linearly to a 0–100 scale. 7 Subsequently, the average of the scores from the four domains was calculated. 7 The NAQ-22 measures the amount of workplace bullying, reported as “never,” “now and then,” “monthly,” “weekly,” or “daily.” 8 A score of 33–45 indicates occasional bullying, and a score above 45 is considered severe workplace bullying. 10 The aCWDHS is scored from zero indicating no discrimination or harassment to 65 indicating all types of measured discrimination at least weekly. 9 Means and standard deviations were calculated. One-sided t-tests, chi-squared tests, and ANOVAs (Kruskal Wallace tests were performed in place of ANOVAs when sample sizes were small) were calculated with the p-value set a priori at 0.05. Data from pediatric physiatrists who did not answer certain demographic questions or who selected “do not wish to disclose” were eliminated from analysis for that specific demographic characteristic. All analyses were conducted on SPSS Version 28.0.
Results
Of the 389 pediatric physiatrists invited to participate, 301 consented and also met inclusion criteria of actively practicing pediatric rehabilitation medicine (retired pediatric physiatrists and pediatric physiatrists in training were excluded, as were any physiatrists mis-identified as practicing pediatric rehabilitation medicine during recruitment), yielding an overall response rate of 77.4%. Of the 301, 270 answered the WHOQOL-BREF, NAQ-22 and/or the aCWDHS and were included in these analyses for a final completion rate of 69.4%. People who identified as women made up 71.2% of pediatric physiatrists who disclosed their gender identity, 72.8% identified as White, and nearly all who disclosed their sexual orientation identified as heterosexual (90.9%). A small percentage disclosed a disability (8.4%).
As shown in Table 1, pediatric physiatrists had an average overall WHOQOL-BREF score of 76.5. Those who disclosed a disability had statistically significant lower overall average QOL (t = 2.356, p = .010) as measured on the WHOQOL-BREF as well as lower scores in the physical (t = 2.158, p = .021) and social domains (t = 2.064, p = .020). Pediatric physiatrists who reported a sexual orientation other than heterosexual had overall average WHOQOL-BREF scores that were not statistically significantly different from their heterosexual peers, but demonstrated significantly lower scores on the psychological domain (t = 1.799, p = .037). There were no significant differences in scoring of pediatric physiatrists on the WHOQOL-BREF by gender, race and ethnicity, religion, or academic rank.
WHOQOL-BREF, NAQ-22 and aCWDHS by demographic characteristics.
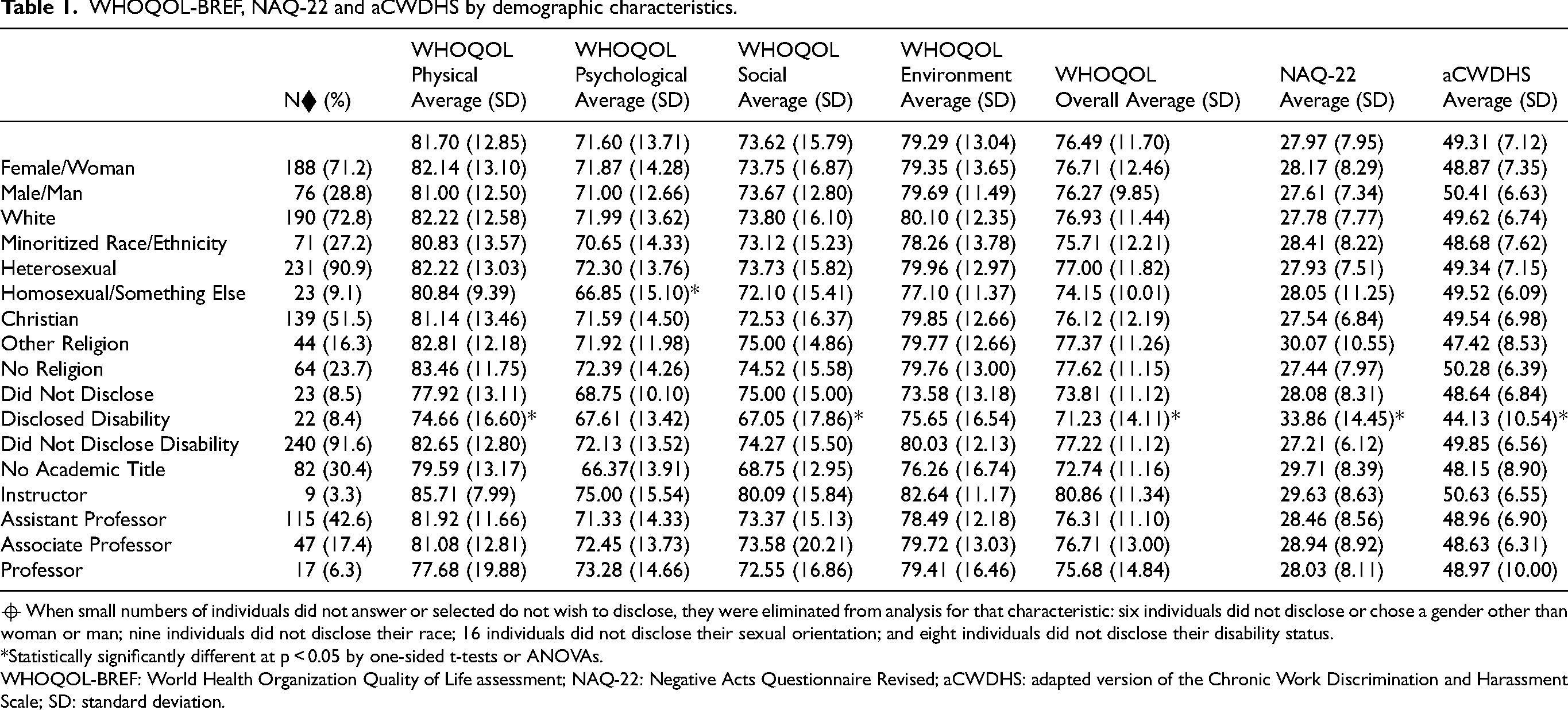
⌖ When small numbers of individuals did not answer or selected do not wish to disclose, they were eliminated from analysis for that characteristic: six individuals did not disclose or chose a gender other than woman or man; nine individuals did not disclose their race; 16 individuals did not disclose their sexual orientation; and eight individuals did not disclose their disability status.
*Statistically significantly different at p < 0.05 by one-sided t-tests or ANOVAs.
WHOQOL-BREF: World Health Organization Quality of Life assessment; NAQ-22: Negative Acts Questionnaire Revised; aCWDHS: adapted version of the Chronic Work Discrimination and Harassment Scale; SD: standard deviation.
The average bullying score on the NAQ-22 was 27.97 (Table 1). Disabled pediatric physiatrists had the highest average NAQ-22 score and were the only demographic group who met this measure's threshold for workplace bullying. They demonstrated statistically higher scores than their non-disabled peers (t = 2.139, p = .022). Among all pediatric physiatrists, 82.63% had scores below 33, 13.51% had scores between 33–45, and 3.86% had scores greater than 45 which indicates severe bullying. The average workplace discrimination and harassment score on the aCWDHS was 49.31. Again, only disabled pediatric physiatrists demonstrated statistically higher scores on the aCWDHS (t = 2.502, p = .010) compared to their non-disabled peers.
Lower WHOQOL-BREF scores were correlated with bullying (NAQ-22 score) (ρ=−.275, p < .001) as well as workplace discrimination and harassment (aCWDHS score) (ρ=.316, p < .001). As shown in Figure 1A, 12.3% of the variation in the environmental domain score of the WHOQOL-BREF was explained by the NAQ-22, while the NAQ-22 had lower predictive capability for the physical (8.6%), psychological (1.6%), and social (1.9%) domain scores. Similarly, as shown in Figure 1B, 16.9% of the variability in the environmental domain score of the WHOQOL-BREF was explained by the aCWDHS score. The aCWDHS had less predictive power for the other domain scores: physical (8.4%), psychological (4.9%) and social (5.1%).
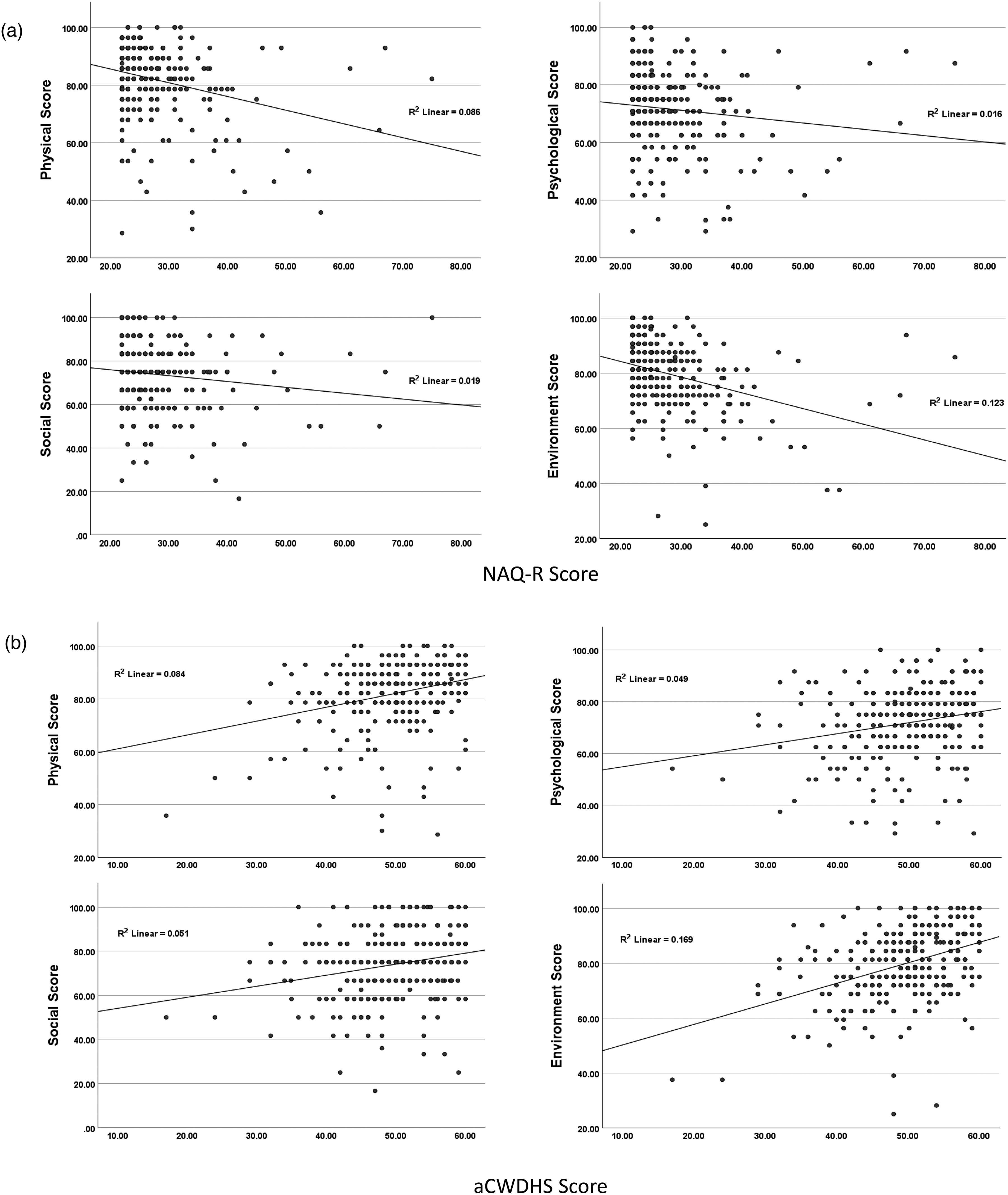
A. WHOQOL-BREF domain scores by NAQ-R score. B. WHOQOL-BREF domain scores by aCWDHS score.
Discussion
Bullying, discrimination, and harassment are common in the health care physician workforce.11,12 Pediatric physiatrists were not immune to this mistreatment and had bullying scores within the range of other physician specialties. 4 The WHOQOL-BREF scores were similar to those found in a study of health care workers by Gholami et al. 13 The finding that disabled pediatric physiatrists had lower WHOQOL-BREF scores is also consistent with the Gholami study. 13 Unlike other studies,14,15 this one did not find that women reported more discrimination and harassment than men within pediatric physiatry. This may be in part because gender-based harassment is more common in male-dominated environments. 16 Also unlike other studies,17,18 minoritized race/ethnicity or sexual orientation were not associated with discrimination, harassment, or bullying. The findings for disabled pediatric physiatrists are consistent with the findings of Meeks et al., who identified that disabled physicians experience higher rates of workplace mistreatment. 11 Ableism (discrimination, mistreatment, or prejudice against individuals with disabilities) 19 can impact the well-being and career development of disabled physicians. 20 Just as the field of medicine has been reckoning with sexism and racism, there are calls to address ableism to improve inclusion.11,20 In these analyses, lower QOL scores were correlated with being bullied and experiencing workplace discrimination and harassment. Notably, disabled pediatric physiatrists reported more bullying and more discrimination and harassment in the workplace. This suggests that disabled pediatric physiatrist might report better QOL if mistreatment in the workplace was eliminated, especially in the environment domain.
This study had notable limitations. First, because of the small size of the field of pediatric physiatry, the study may have been inadequately powered to detect differences, indicating the need for additional research in this area. For example, in this study, women had higher aCWDHS scores indicating more harassment and discrimination than men, but the difference was not statistically significant. Also, small numbers of respondents opted not to answer certain questions, which lowered the sample size for those comparisons. Stigma around gender identity, sexual orientation, disability, and religion could be contributing factors related to non-disclosure.21,22 Second, and similar to other studies, response bias may have been a factor, although, of note the response rate was above 60% which is generally considered optimal because non-response bias is minimized. 23 Third, disabled pediatric physiatrists may have had invisible disabilities that were not specifically reported which may impact how they are perceived and treated by others. Lastly, 8.4% of pediatric physiatrists disclosed disabilities in this survey, a much higher prevalence than physicians generally, of whom only 3.1% self-identify as disabled. 24 It is not surprising that the field of pediatric rehabilitation medicine is attractive to physicians with disabilities due to the focus of the specialty on functioning and promoting inclusion.
Conclusion
In this study of pediatric physiatrists, those with disabilities reported statistically higher rates of bullying and workplace discrimination and harassment. Disabled pediatric physiatrists also reported lower QOL scores on the WHOQOL-BREF. The NAQ-22 and the aCWDHS more strongly predicted the environmental domain score of the WHOQOL-BREF than the other three domains. This indicates that mitigating workplace bullying, discrimination, and harassment should be prioritized because it may have the potential to optimize pediatric physiatrists’ QOL, especially for disabled pediatric physiatrists.
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.