
Abstract
PURPOSE:
The aim of the study was to evaluate the Assessment and Orientation Treatment Program for children and adolescents with disabilities treated at the Center Teletón Uruguay from the perspective of the patients and their parents based on several patient reported outcome measures: health related quality of life (HRQOL), treatment satisfaction, family impact, and emotional distress.
METHODS:
The sample consisted of all the 126 dyads of children/adolescents with ages ranging from 2 to 18 years and their primary caregivers who entered the program from April to October 2012. A set of instruments were filled out by children and parents before and six months after the program. T test for paired samples for continuous variables and McNemar’s test for categorical variables were used to assess changes pre and post intervention.
RESULTS:
There was a high prevalence of depression and anxiety in the caregivers. In the second evaluation, improvements that were statistically significant only for the caregivers were observed in the HRQOL of children, adolescents and caregivers.
CONCLUSIONS:
The patient reported outcome measures used were effective in detecting changes in several areas of the quality of life of children observed by their caregivers and in their own quality of life after the intervention.
Introduction
The increasing prevalence of disability among children and adolescents highlights the importance of establishing a specific approach for dealing with the problem among these age groups. Studies on the impact of disability on the health-related quality of life (HRQOL) of caregivers show that they bear a high physical and emotional burden and have poorer physical and mental health when compared to the general population. Additionally, significant correlations between levels of burden and psychosocial well-being are observed [1]. Similar results could be seen among children.
Over the years, numerous public and private stakeholders have collaborated to develop policies and programs aimed at improving the functional status, social integration, participation, and general well-being of patients with disabilities and their families [2]. Uruguay has followed this path, showing a strong drive to improve the availability of resources, equity and accessibility. When designing and evaluating programs, it is crucial to understand the perspective that children and adolescents with disabilities have on their well-being and quality of life. A recent study concluded that including the child’s perspective was not only a human right, but also a source of substantial input for the implementation of public policies aimed at promoting their rehabilitation [3], both within and also outside of a medical setting. An example of this is a study on factors associated with the process of children with disabilities transitioning to a new school which recommended considering what those children prioritized, as well as their fears and concerns with regards to the new school. The study suggested granting them a proactive role in the transition process, allowing for discussion with teachers and peers encouraging them to consider topics beyond the realm of disability [4].
The importance of conducting assessments on the quality of life of children regardless of their parents’ perspective has been stated in Latin-America. Several instruments have been developed and validated to assess their quality of life and well-being [5]. However, no reports on the well-being and quality of life of children with disabilities were identified [6].
The objective of the present study was to assess the outcome of a rehabilitation program (Assessment and Orientation Treatment Program or TVO by its Spanish acronym) by Centro Teletón, Uruguay, from the perspective of children, adolescents, and their primary caregivers (PCs). TVO includes most participants admitted to Centro Teletón, for which the institution allocates a considerable amount of human and material resources. This is something that might not be reflected in mobility and functional status outcomes given the severity of certain disabilities. As a result, healthcare professionals and stakeholders were interested in the impact the TVO might have on other dimensions such as the perception of well-being, burden of care and overall satisfaction. Hence, these might have a significant impact on the way the program is assessed by the Institution and influence the manner in which resources are allocated.
We expected that the program, in all its dimensions, might have a considerable impact on the HRQOL of children with disabilities and their PC. Additionally, we expected to find a correlation between the quality of life reported by children/adolescents and the well-being of their PC. Finally, it is believed that including the perspective of patients based on self-reports would provide a more complete picture of the outcomes and, in turn, help improve interventions.
Materials and methods
A longitudinal study was designed to collect data on the HRQOL of children and adolescents with disabilities, and on the HRQOL satisfaction with treatment, family impact, and emotional distress of their PCs, both prior to being admitted to a rehabilitation program (T0) and 6 months after the intervention (T1). The TVO participants were admitted according to a set of inclusion and exclusion criteria defined by the institution and determined during an initial interview.
The TVO is a multimodal approach consisting of four consecutive 4-hour daily sessions (16 hours total) aimed at providing assessment and guidance for all participants, children and PCs. Initially, a multidisciplinary team made up of physiatrists, a social worker, physiotherapists, occupational therapists, a speech therapist, a psychologist and a teacher thoroughly evaluated each patient and provided guidance for the child/adolescent and their PC. The interventions followed a step-by-step protocol that allowed for consistency across individual treatments. In all cases, a follow-up assessment was scheduled to evaluate and eventually modify the therapeutic approach.
The pathologies included in the program were neurological conditions of the central and peripheral nervous system such as chronic encephalopathy (cerebral palsy), children at high risk for neurological conditions, traumatic brain injury, spinal injuries (e.g., trauma, myelomeningocele), degenerative CNS diseases, and neuromuscular conditions (muscular dystrophies, congenital myopathies, plexopathies).
Prior to and six months after the end of the program the children and their PCs completed a battery of questionnaires consisting of the Pediatric Quality of Life Inventory Version 4 (PedsQL V4) for children and parents, the PedsQL Specific Family Impact Module (FIM), and the World Health Organization Disability Assessment Schedule II (WHO-DAS II). The Hospital Anxiety and Depression Scale (HADS) was filled out only by PCs.
The
The Spanish version of the World Health Organization Disability Assessment Schedule II (WHO-DAS II) was used to measure the health status and functional capacity of PCs. It is an internationally validated assessment tool based on the International Classification of Functioning, Disability and Health (ICF) [10]. In this study, the 12-item short version (WHODAS 12), which provides data on global disability among the six dimensions of Understanding and Communication, Mobility, Self-care, Interpersonal Interactions, Activities of Daily Living, and Social Participation, was used.
The
Sociodemographic data were obtained from the participants.
Statistical analyses
Frequencies, mean and standard deviations were calculated to describe the sociodemographic data. Cronbach’s alpha was calculated to assess the reliability of the instruments in our sample. Its coefficients between 0.60 and 0.69 were considered acceptable. Values of 0.7 and higher were considered good. To assess pre and post intervention changes, paired samples t-tests for continuous variables and the McNemar’s test for categorical variables were used.
Ethical considerations
Ethical approval was obtained by the Research Ethics Committee of the Hospital de Clínicas of the Universidad de la República, Uruguay, and informed consent was independently requested from children/adolescents and their parents. Participation was entirely voluntary for all participants, and subjects were informed that they could refuse participation or withdraw from the assessment session at any time. Neither patients nor their caregivers received any benefit, monetary or otherwise, for participating in the study.
Results
The sample consisted of all the patients included in the TVO between April and August 2012 as well as their PC. The description of the sample at baseline and follow-up is shown in Fig. 1.
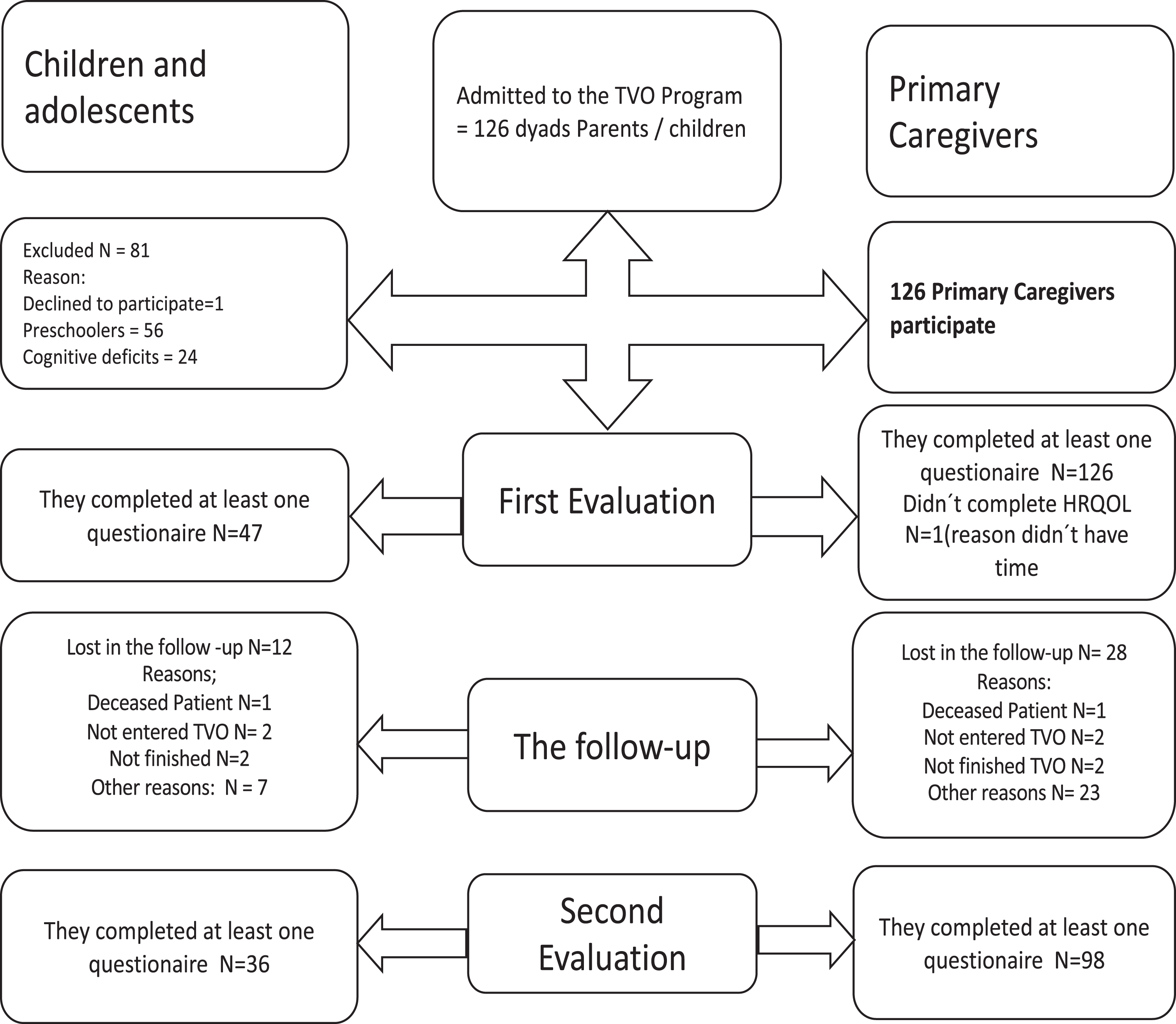
Flow chart of the data collection procedure.
At T0, 126 dyads of children/caregivers were assessed. As for the children, 56 (44.4%) were toddlers, so questionnaires were answered only by their parents, and 70 (55.5%) were children and adolescents aged 5–18 years. Among the latter, 20 (28.6%) were young children (5–7 years), 28 (40 %) were children (8–12 years) and 22 (31.4 %) were adolescents (13–18 years): 47 (67 %) of them completed at least one of the questionnaires, while 23 (43 %) did not respond due to severe disability. The response rate among caregivers at T0 was 100% considering that at least one questionnaire was filled out, although the parent of one toddler declined participation during the assessment process. 28 caregivers (22.2%) and 12 children (26.5%) did not complete the follow-up questionnaires. Children and caregivers who dropped out of the study did not differ in age and PedsQL scores at T0 with the exception of the Emotional Well-being subscale scores of the parents that were significantly lower at T0 in those missing at follow up (Mean score 58.9 points for those missing at T1 vs. 69.0 points for those who completed the survey at T0 and T1; t-test p = 0.045).
Socio-demographic data of the sample are shown in Table 1. The mean age of children and adolescents was 7 years (SD: 4.8 years). Regarding the schooling of children and adolescents, it should be noted that 45 (35.7%) children did not attend school, 64 (50%) attended school or high school, and 17 (13.5%) attended a special education school. In 80.2% (n = 101) of cases the mother, mean age of 35.3 years, was the PC; twenty-three point four percent (n = 30) of mothers had not completed secondary or tertiary education, and 36 (28.1%) of them did not have sufficient income to meet their needs.
Sociodemographic data and sample characteristics
The subscale and global scores for all questionnaires showed Cronbach alpha coefficients ranging from 0.62 to 0.99, with variations in different instruments and dimensions (Tables 2, and 4).
PedsQL V4 Children’s Version total scale and subscale mean scores
*The Psychosocial Well-being score is the sum of emotional, social and school subscale scores. PedsQL: Pediatric Quality of Life Inventory Version 4 for Children and Adolescents.
PedsQL V4 Parents’ Version total scale and subscales mean scores of primary caregivers
*The Psychosocial Well-being score is the sum of emotional, social and school subscale scores. PedsQL: Pediatric Quality of Life Inventory Version 4 for Parents.
FIM mean scores of the primary caregivers before and after the intervention
FIM: PedsQL Specific Family Impact Module; Total HRQOL Score is the sum of the physical, emotional, social, and cognitive subscale scores.
The results for the child ratings of the PedsQL are shown in Table 2. Physical well-being had the lowest scores for all ages at T0 and T1. Non-significant changes in the PedsQL subscale scores were observed between T0 and T1 (Table 2).
The HRQOL results of children as reported by their caregivers showed that the physical well-being subscale had the lowest scores for all ages both at T0 and T1. Statistically significant changes were observed in the perspective of PCs regarding the HRQOL of their children in all the dimensions between T0 and T1 (p < 0.05) except for the School dimension (Table 3).
The scores for the HRQOL of PC rated with the FIM showed that the Worries subscale had the lowest scores followed by the Daily Activities subscale. All mean subscale scores showed statistically significant changes at T1 (p < 0.05) (Table 4), with the exception of Emotional, Communication and Worries.
PCs reported improvement in their overall health with 68.2% reporting good or very good health at T1 in relation to 57% at T0; however, these changes were not statistically significant (McNemar’s test p = 0.358). High rates of depression (30%) and anxiety (52%) were observed at T0. A non-significant decrease in the frequency of positive screening for anxiety (McNemar’s p-value = 0.441) and depression was also observed during the follow-up. (McNemar’s p-value = 0.753).
Ninety five percent of respondents reported high satisfaction with treatment as assessed with the HSGM.
There is an increasing need to implement rehabilitation programs that improve the functional status and quality of life of children with disabilities. Most of these interventions have been evaluated based on biomedical or functional parameters. The aim of this study was to describe the outcomes of a rehabilitation intervention from the perspective of children and their PC in order to provide relevant information that healthcare professionals and stakeholders might use in the decision-making process related to improvements in the care process, resource allocation, and funding.
Thus, the main objective was not to measure changes in functional capacity but to detect perceived changes in the HRQOL of patients and their caregivers using patient reported outcome measures (PROMs).
The most impaired dimension in the HRQOL of children and adolescents of all ages was Physical Well-being. While scores for this dimension improved after the TVO, differences were not statistically significant. Similar results were observed in the other dimensions of the PedsQL. Albeit small, the improvements among ratings highlight the importance of continuing to study the impact that specific interdisciplinary based rehabilitation treatments have on the quality of life of children and adolescents with disabilities.
Regarding the caregivers’ perspective on the HRQOL of children and adolescents, the most affected dimension also was Physical Well-being, showing statistically significant improvements at the second assessment. These were also observed in the ratings of all other dimensions of the PedsQL both before and after the TVO intervention with the exception of the School dimension scores.
These results support the assumption that the intervention on the children modified the perception of parents regarding the impact that the disability had on the quality of life of their children.
As for the perception caregivers indicated in their self-reported HRQOL, Worries scored the lowest and Communication scored the highest, both at T0 and T1. We found improvements in several dimensions of the FIM 6 months after the intervention, especially with regards to Daily Activities. No significant changes were observed after TVO in Worries, Communication, and in the Emotional Status subscales. Regarding caregivers’ emotional well-being, measured by the HADS, the results showed a high level of emotional distress among the sample with a positive screening for depression in almost one third of the sample and a positive screening for anxiety in half of the sample. Although changes were not statistically significant, the prevalence of a positive screening for anxiety and depression decreased at T1. High levels of emotional distress have been reported elsewhere. The model of disability of the ICF used in this study highlights how contextual situations such as the emotional state of family members may worsen the condition of disability and consequently the health-related quality of life. These results showcase the need for specific interventions that address the mental well-being of mothers or caregivers [13].
The caregiver’s functional capacity and health evaluated using the WHODAS 12 showed that only 4.7% reported having bad or very bad health at T1, with very good, good or moderate health in 95.3% of cases. When evaluating the six domains of the WHODAS 12, the Social Participation domain was the most affected, with a mean score of 16.40 (SD±21.02) which is considered an extremely low degree of affectation.
It has been reported elsewhere that even if the experience of disability involves the challenges of worrying about the future of children and family burdens. Also, it may also lead to personal and family enrichment. Key factors for these changes are the collaborative relationships between professionals and parents, the identification of family strengths, and the development of perception of control and parental self-determination skills [14].
Several limitations have been identified in the study. Many of the children/adolescents were unable to participate in the survey based on age/condition limitations. Significant changes were reported mostly by parents. This is an important limitation when measuring the HRQOL or other PROM in children or adolescents with chronic neurological conditions.
Even when observations showed significant differences in several self-reported variables after intervention in relation to the initial assessment, limitations of the study design, such as the lack of a control group, were prevented from reaching conclusions about which specific aspects of the intervention were responsible for the shift in scores. The shifts might be related to the improvement in the functional capacity of children. They may also be caused by the influence of the support of the team, or by training the parents, more specifically the mothers, to accept their children’s limitations and handle their difficulties. The fact that most children in the study were toddlers might have had a positive effect on the responses. For example, an evaluation of the families of children with autism in Spain pointed out that the support and guidance of professionals, mainly early after diagnosis, were highly significant when helping parents better understand and accept the disability of their offspring [1, 15]. This highlights the importance of early detection of limitations and of accessibility to rehabilitation programs at the Centro Teletón.
Moreover, a response shift could be explained by other factors such as general satisfaction with the program (as was reported by the majority of caregivers), time invested in educating and motivating parents to delegate care to other members of the family, or due to other supervening variables. Notwithstanding these limitations, and even when relevant information is lacking due to the descriptive nature of the study, research findings may provide guidance on the efficiency of the treatments from the perspective of those who are to benefit the most from these programs.
Some of the findings related to the sociodemographic characteristics of the sample may also provide information on relevant aspects to be considered when approaching this specific population of children and their families.
When considering schooling, 36.7% of the children/adolescents were not included in any educational program. These results are consistent with the UNICEF report which revealed that children with disabilities are generally excluded from education systems [16]. In addition, a report by the World Bank (2006) indicated that only 30% of children with disabilities attended school in Latin America and the Caribbean. When compared to national data, similar percentages are observed, where depending on age group and type of disability, between 30% and 52% are excluded from the educational system. Even though this study showed improvements in the educational inclusion of those with disabilities, much still needs to be done to eliminate social, geographical, and architectural barriers. A research study conducted in New Delhi showed that children with disabilities were less likely to start school and more frequently dropped out of school before completing high school than some without disabilities. This proves that the learning process is not inclusive in practice. The education gap is wider for girls, economically disadvantaged children and those from households where parents have no formal education [17].
International studies have described the impact that caring for people with disabilities has on health and working status, leisure, and family ties of PCs. In this study, mothers, many of which were single parent figures, were PCs in most cases. A large percentage of them were housekeepers with low education and low income. A regional study reported economic instability, frailty of support networks, a higher perception of health disorders, extensive time and dedication to activities of informal care and an overload of functions for caregivers [18, 19].
Additionally, the existing obstacles to access and keep formal job positions have an impact on the financial situation of families. Results showed that family income was just enough to cover needs in 46.9% of the cases, and 28% of cases reported struggling financially. This suggests that the difficulties arising from the overload of taking care of children with disabilities are associated with unfavorable financial situations. A report by the World Bank (2011) indicates that disability is more common in financially unfavorable contexts, emphasizing that the prevalence of disability is higher in low-income vs high income countries. Additionally, the report states that people with low income, low education and who are unemployed, as is the case for the subjects in our sample, are at higher risk for developing a disability [20].
These factors are most significant when designing programs to address the problem of disability from a global perspective. The project “Situation of People with Disabilities in Contexts of Poverty: Quality of Life and Quality of Care” carried out in Uruguay in 2008 concluded that people with disabilities are more likely to remain poor because of the barriers they face accessing the employment market. They are less likely to become involved in and have an influence on the political decision-making processes in their communities. The project also found a greater number of women living in poor neighborhoods with lower incomes in relation to men, raising their children as single parents and being responsible for the care of their children and elders [21, 22].
Conclusions
Differences were observed in the HRQOL reports made by the caregivers before and after the rehabilitation interventions. The high percentage of toddlers participating in the study is a positive aspect of the TVO as it indicates there is early access to rehabilitation programs facilitating early detection of difficulties or limitations among children.
The level of emotional distress was exceedingly high among the study sample. The emotional status of PCs calls for special attention given its impact, not only on the caregivers’ well-being and health, but also on the quality of care they provide to their children. In addition, the sociodemographic characteristics of the parents showed low levels of education and economic deprivation in many cases. This highlights the need for providing psychosocial support to this population with regards to specific rehabilitation interventions.
As an observational study, it has several limitations as mentioned above. Limitations of the study design were prevented from concluding which specific aspects of the treatment fostered changes. Low response rate is another important methodological flaw in studies using PROMs in children and adolescents with neurological deficits.
As PROMs were included in the evaluation of the rehabilitation program, areas were identified that require special consideration when adjusting current programs and implementing new ones. Similar studies could be implemented to assess other programs.
Footnotes
Acknowledgments
This project was funded by the Sectorial Commission for Scientific Research (Comisión Sectorial de Investigación Científica - Universidad de la República, Uruguay) Grant, and Fundación Teletón.
We gratefully acknowledge Sylvia Pereira, Laura de Castellet, Eloísa González, Gonzalo Méndez, the team of professionals working at Centro Teletón for their trust and cooperation, as well as Ramón Álvarez, Luis Rajmil, and Ben Arnold.
A special thanks to Ana Martegani for her kind assistance in communicating with the children and their families, and in the data collection process.
Conflict of interest
The authors have no conflict of interests to declare.