
Abstract
Research has underscored the agenda-setting and policy implementation advantages associated with the concentration of political and policy-making authority. But to what extent does this concentration of authority within health policy-making institutions determine the early timing and depth of non-communicable disease (NCD) policies? Are other factors within and outside of government more important? Comparing one Latin American country exhibiting a strong concentration of political and policy-making authority, Mexico, to one that does not, Brazil, we find that weaker, fragmented political and policy-making powers in Brazil expedited the creation and implementation of NCD programs. As seen in Brazil, our findings suggest that the factors that account for the earlier adoption of NCD policies and successful implementation are the early institutionalisation of societal interests and pressures within the bureaucracy, the “bottom-up” diffusion of early policy ideas, and international policy recommendations. This institutional, participatory, and ideational approach may provide more important predictors for explaining variation in NCD policies.
Introduction
In the past twenty years, several countries in Latin America have seen the burgeoning growth of non-communicable diseases (NCDs), such as obesity, type-two diabetes, heart disease, and cancer. The product of transitions to free markets, the importation of high caloric junk foods, changes in daily lifestyle, and even climate change are factors that have contributed to these ailments. For the most part, the region has taken the NCD situation seriously with governments voicing concern and working with international health organisations, such as the World Health Organization (WHO) and the Pan-American Health Organization (PAHO), to improve policy responses.
In a region that has struggled with the consolidation of democracy, unstable political institutions, and endemic corruption, essentially no scholarly research to our knowledge has explored the institutional designs – for example, executive, legislative, and delegated constitutional powers – shaping the timing and depth of NCD policies in Latin America. With regard to timing, this article is interested in comparing the countries of Brazil and Mexico and exploring which of these countries was the first to prioritise the creation of NCD prevention and treatment programmes, such as obesity, type-two diabetes, tobacco consumption, and cancer, and why this occurred. And with respect to depth, we examine if Brazil or Mexico were capable of successfully implementing their NCD policies; we describe this success in implementation, depth, as the national Ministry of Health’s (MoH’s) commitment to working closely with state governments to enforce policy requirements while working with families and/or schools to achieve this outcome.
In this article, through our comparison of Brazil and Mexico, we critically evaluate hypotheses in the literature concerning the health policy-making advantages associated with the concentration of political authority, that is, the presence of strong presidential decree authority and bureaucratic policy-making autonomy. Our case study findings suggest that in contrast to the existing literature, in Mexico, this concentration of authority does not lead to the early adoption and successful implementation of NCD programmes.
In contrast, and as seen in the more successful case of Brazil, we found that the presence of participatory institutional and ideational factors appear more important in accounting for differences in the early timing and depth of policy reform. First, the constitutionally-based represenation of civil societal actors within government policy-making committees was important, thus generating a comparatively lower level of bureaucratic autonomy and policy-making influence when compared to Mexico. While this level of autonomy has remained lower in Brazil, it does not mean that the bureaucracy has not been important; indeed, Brazil’s MoH has still played an important role as coordinator of civil societal interests, in turn facilitating civil society's early NCD policy influence. A second differentiating factor is Brazil’s early sub-national policy experimentation and the “bottom-up” diffusion of policy ideas. In addition, it is important to note that the broader health systems context also mattered; that is, differences in Brazil’s and Mexico’s healthcare systems also accounted for differences in these bottom-up diffusion processes. Brazil’s more unified and universal public health system, operating within a decentralised context, namely the Sistema Único de Saúde (SUS, Unified Health System), facilitated policy learning between the states and the national government through SUS’s periodic inter-governmental co-ordinating institutions, whereas Mexico’s excessively fragmented public health system did not provide this process. And, finally, the presence of epistemic communities and their early policy-making influence in Brazil versus Mexico were also important differentiating factors. The positive role that epistemic communities played was shaped by the Brazilian government’s historic commitment to the global and domestic engagement of NCD scientific experts, which was absent in the case of Mexico.
As Table 1 illustrates, when these nations are compared to each other, we find that NCD policies have emerged at an earlier point in time and with greater policy implementation success in Brazil, a nation that exhibits comparatively weaker and dispersed concentrations of political authority in the area of healthcare policy-making.
National Non-Communicable Disease Programmes in Brazil and Mexico (Over Time).
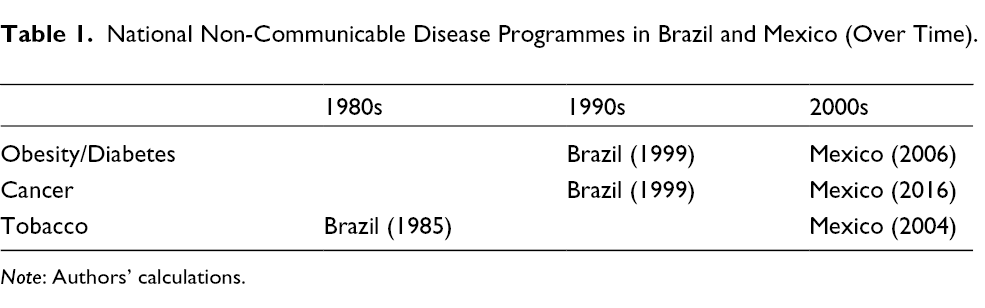
Note: Authors’ calculations.
Methodology
This study conducts a comparative analysis of Brazil and Mexico in order to critically evaluate prevailing theories and their causal mechanisms with respect to the importance of concentrations in political authority in the area of healthcare policy-making. In so doing, our case studies were used to thoroughly assess and validate the efficacy of these theories and their causal mechanisms (Bennett, 2004). Based on our assessment, however, we also strove to discover alternative causal factors not considered in the literature through our case study comparisons (Bennett, 2004).
We selected the cases of Brazil and Mexico in order to provide an in-depth analysis of their critical differences in causality and NCD policy outcomes, while also using these case studies to examine the literature and our proposed alternative theoretical approach. To that end, we conducted a most similar systems design (MSSD), which establishes similarities between nations on several contextual factors while nevertheless illustrating critical differences in causality and outcomes (Landman, 2003). Indeed, these cases were selected because they are two of the largest federations in Latin America (next to Argentina), while also exhibiting high levels of healthcare decentralisation (Homedes and Ugalde, 2009; Rich and Gómez, 2012). Brazil and Mexico are also similar in that they have one of the highest levels of annual sales per capita in sodas and ultra-processed foods in Latin America (Pan-American Health Organization, 2015) – foods that are closely associated with NCDs. Both countries have also recently seen an increase in civil societal activism and social movements in response to NCDs. Despite these similarities, Brazil and Mexico exhibited critical differences in the aforementioned causal factors as well as the timing and depth of NCD policy outcomes.
We also choose the cases of Brazil and Mexico because they have one of the highest levels of obesity, type-two diabetes, and tobacco consumption in the region (see Figures 1 -3), as well as the ease of obtaining data on these ailments due to their high prevalence rate and government attention to them. While we recognise that other countries, such as Argentina, Chile, and Uruguay, also had high levels of diabetes, these cases were not selected for several reasons. First, we decided to focus on two countries, Brazil and Mexico, in order to provide a more in-depth assessment and explanation of the politics of NCD policy reform across three health sectors – obesity, cancer, and tobacco – rather than striving to compare these sectors across several case studies and, in the process, providing a limited analysis and explanation. Second, we were interested in countries with a long history of federalism, decentralisation, and free market reforms – characteristics that were not present in Chile and Uruguay. Third, we choose Brazil and Mexico because one of us has extensive experience living and working in these countries and because we both have a strong understanding of the political factors influencing NCD policies in these countries and throughout the region. Furthermore, it is important to note that Brazil and Mexico were not chosen for their known values on the dependent variable, thus avoiding any form of selection bias.
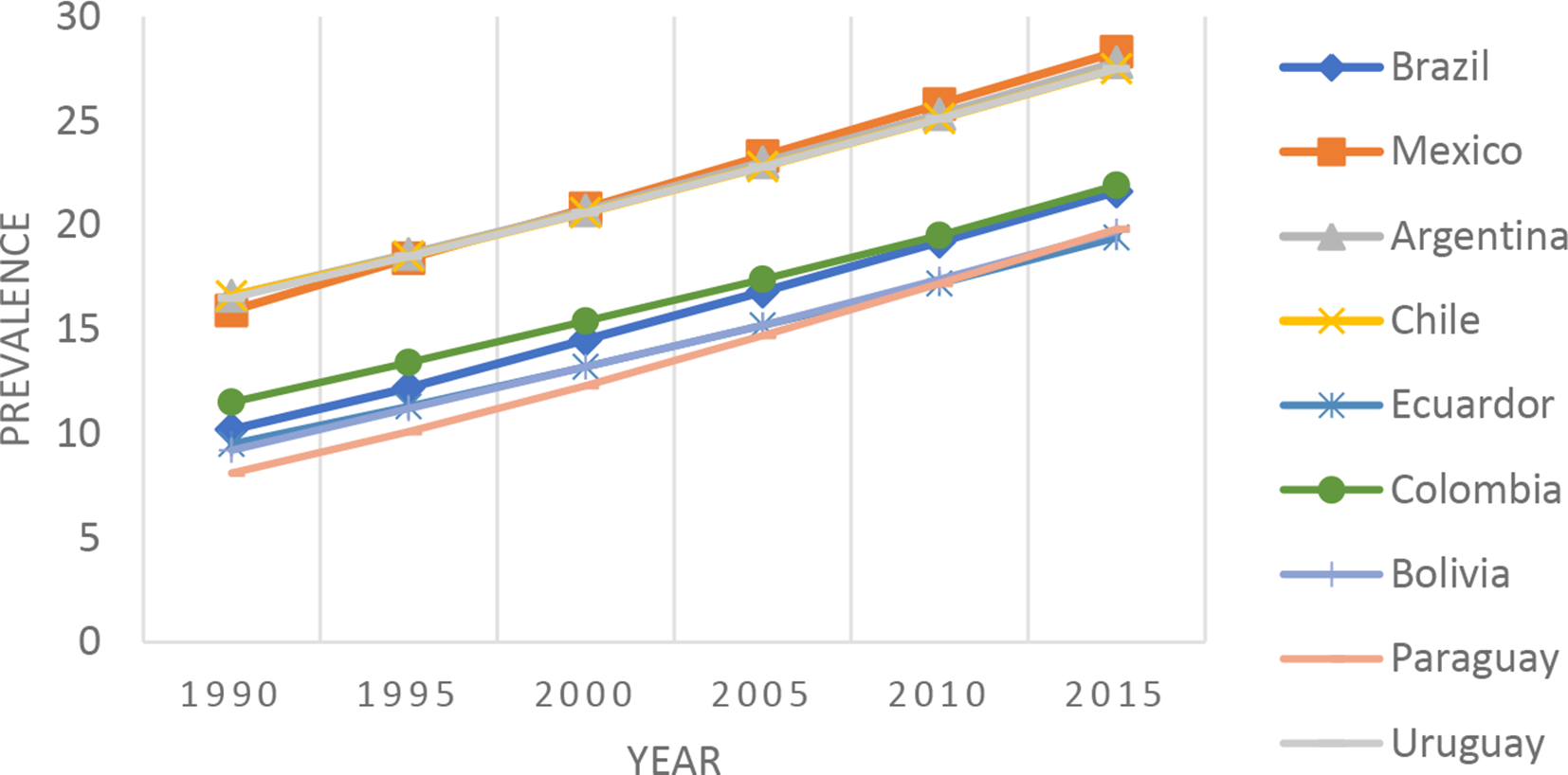
Prevalence of Obesity among Adults in Select South American Countries.
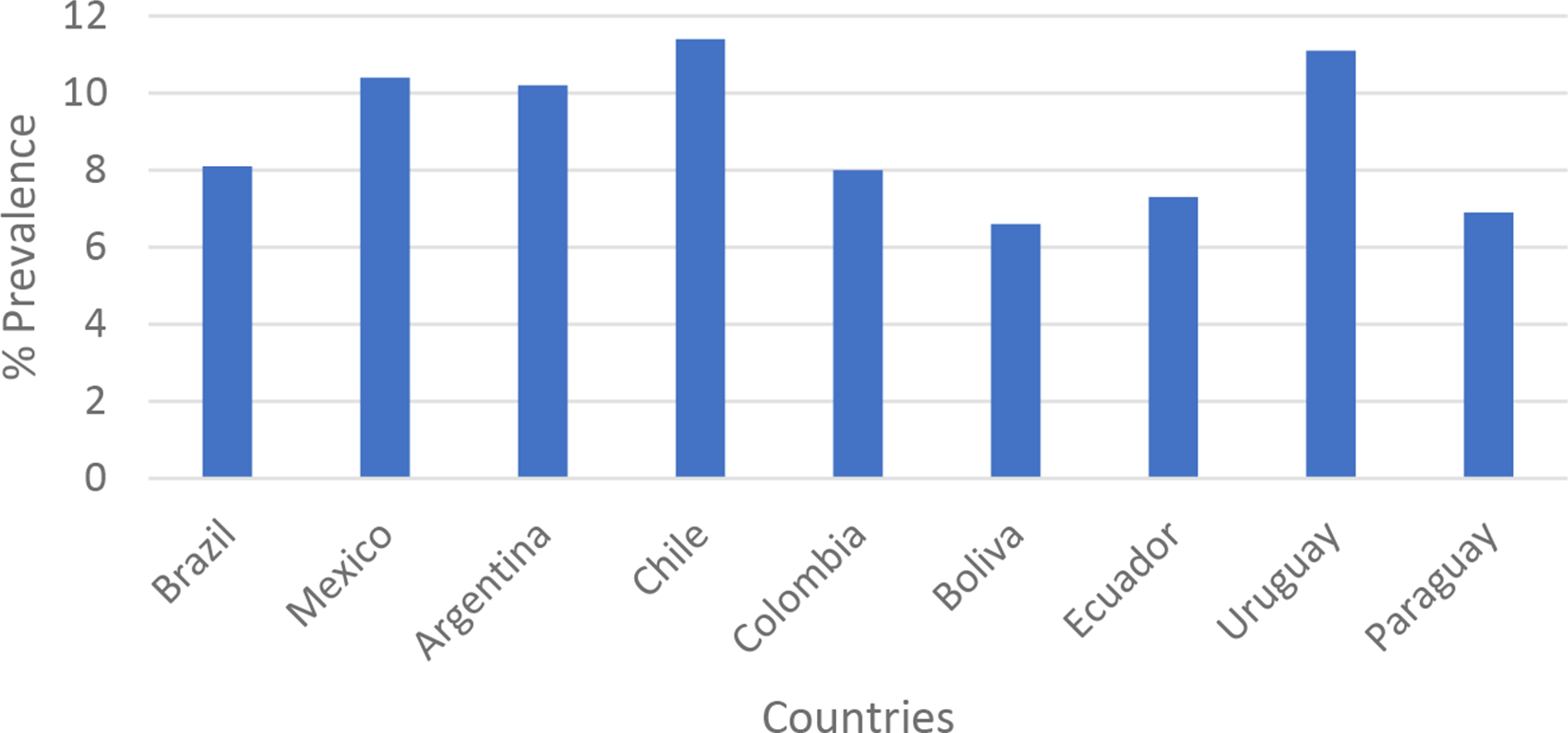
Prevalence of Diabetes in Select South American Countries, 2016.
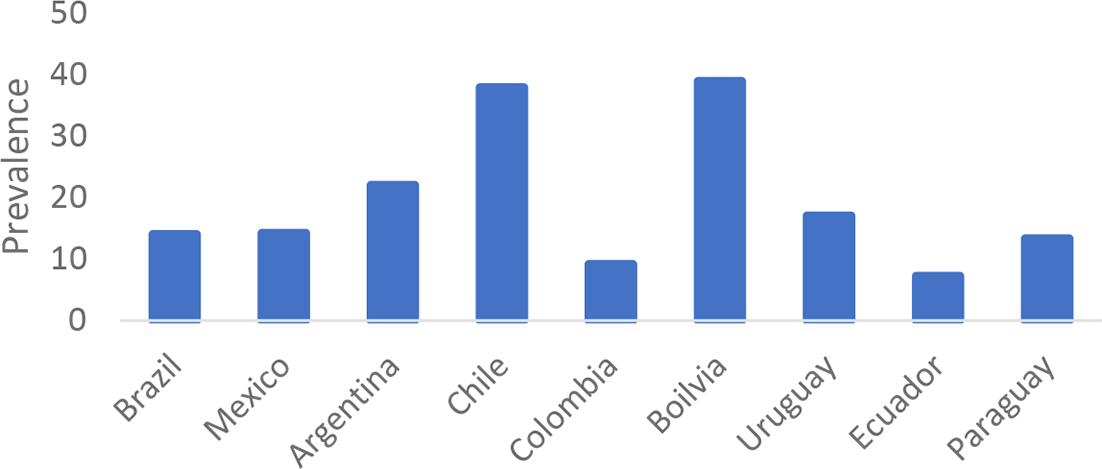
Prevalence of Tobacco Smoking in Select South American Countries, Age-Standardized Prevalence of Tobacco Smoking among Persons 15 years and older (%).
Supportive qualitative data were obtained from a variety of sources, such as peer-reviewed journal articles, books, policy reports, and online news articles in English, Spanish, and Portuguese languages. Quantitative data on disease prevalence and deaths were obtained from government reports and international databases, such as the WHO’s online Global Observatory Database. This study commenced in 2016 and concluded in 2019.
Because qualitative interviews were not conducted in this study, ethics approval from our respective university committees were not required to conduct the research. Working with patients was also not required for this study and, hence, informed consent from patients was not required.
Political Concentration and NCD Policy in Latin America
Researchers have recently investigated the relationship between concentrations of policy-making authority within political institutions, political representation, health policy design, and implementation (Gauri and Khaleghian, 2002, Gómez, 2018a, 2014; Immergut, 1993; McGuire, 2010; Nathanson, 1996). Our assumptions about the public health policy advantages of institutions exhibiting strong agenda-setting powers in health policy reform stem primarily from the historical institutionalism literature in social and public health policy (Gómez, 2006; Nathanson, 1996; Amenta and Skocpol, 1986). These and more recent works on infectious diseases, such as HIV/AIDS, suggest that institutions exhibiting strong concentrations of political authority in the office of the executive (i.e. presidential/prime ministerial) and legislative arena, coupled with low congressional, bureaucratic, and civil societal veto powers, expedite health policy reforms (Gauri and Khaleghian, 2002; Gómez, 2006; Nathanson, 1996).
In this literature, one area of research has examined the importance of presidential constitutional powers, such as executive decree authority, and how this expedites heath policy agenda-setting processes and implementation (González-Rossetti and Ramírez, 2000; Iriart et al., 2001). In this literature, the presidents’ ability to design and create legislation is facilitated by constitutionally delegated decree authority (González-Rossetti and Ramírez, 2000; see also Carey and Shugart, 1998, on this type of decree authority). When these executive powers combine with presidents’ interests and commitment to prioritising healthcare issues, which is often reflected in the usage of executive decree, legislation is quickly designed and implemented (González-Rossetti and Ramírez, 2000). In Argentina, for example, some claim that hospital reform and the regulation of health insurance providers were expedited through the usage of presidential executive decrees, which bypassed legislative veto resistance (Iriart et al., 2001).
Another wing of literature examines the importance of state bureaucratic technical capacity and autonomy. Among other important historical factors that accounted for successful primary care programmes in developing nations, the work of McGuire (2010) shows that nascent democracies with MoHs having strong political support, technical capacity, and autonomy were early policy innovators and capable of successfully implementing primary care programmes in the area of children’s and maternal health. And, as seen in some emerging economies in Africa, such as Zambia, even when other policy actors, such as non-governmental organisations (NGOs), activists, and academics are involved in helping MoH bureaucrats create policy, ultimately the timely creation of NCD policies depends on the latter’s willingness and capacity to do so (Mukanu et al., 2017).
However, our in-depth examination of the politics of NCD programmes in Latin America seems to question the importance of the literature emphasising the agenda-setting and policy implementation advantages associated with a concentration of political and policy-making authority and interest in reform. In light of these theories, our empirical findings instead suggest that those nations exhibiting the earliest, most successful implementation of NCD programmes were those that did not exhibit these institutional advantages in the office of the presidency, legislature, or bureaucracy. Instead, we found that a combination of three factors – first, the constitutionally based representation of civil societal actors within government-sponsored health policy committees; second, early sub-national policy experimentation, policy ideas, and bottom-up diffusion processes; and third, the role of epistemic communities – played a more important role. More specifically, civic representation within government institutions and incessant civil societal pressures for policy reform provided a favourable context for adopting sub-national policy ideas at an early point in time. Additionally, Brazil’s earlier engagement with international and domestic scientific experts and their policy ideas helped to shape the MoH’s interests and commitment to policy reform early on, a process that was absent in Mexico. Thus, in contrast to the existing literature, we found that the early adoption of NCD programmes and their successful implementation were found in Brazil, which exhibited comparatively weaker concentrations of political and policy-making authority. Moreover, we found that without a robust set of civil societal actors to work with, the national bureaucracy will not have the civic allies needed to implement policy through partnerships and sub-national accountability, as seen in Mexico.
Brazil
Presidential and legislative powers in Brazil have dissipated over the years. In 1994, then President Fernando H. Cardoso (1995–2002) agreed to abdicate most of his constitutionally delegated decree-making powers in exchange for opposition political party support to pass economic structural adjustment legislation (Pereira et al., 2006). Negretto (2004) has also shown how a decrease in legislative support and weak presidential veto powers have constrained the president’s agenda-setting influence. The product of an open-list electoral system, Brazil’s fragmented and polarised political party system has also complicated efforts to muster coalitions for economic and social policy reform (Nooruddin, 2011). In this context, especially in light of recent political scandals and changes in government, passing legislation in response to NCDs has been particularly daunting.
At the same time, the MoH’s ability to create and implement legislation has been hampered due to weak presidential and congressional leadership and resolve, in turn failing to provide support for the bureaucracy and its efforts. While specific policy issues, such as HIV/AIDS, received strong political interest and support – due, some claim, to alternative geopolitical interests – when it came to broader health systems reform, this was never the case (Gómez, 2018a). Since the 1990s, the MoH, despite having a high level of technical capacity and normative commitment to policy reform, has not been able to create and fund legislation on its own, has seen a gradual decline in congressional funding support – even under the leftist Luiz Inácio “Lula” da Silva administration (2003–2010), and has consequently been troubled in its ability to monitor and implement NCD programmes at the state level (Mendes and Marques, 2009).
Despite these institutional challenges, since the early 1990s, Brazil’s government somehow succeeded in creating a host of national NCDs programmes. With respect to tobacco control, Brazil’s first National Program for Tobacco Control emerged as early as 1985 (Romero and Silva, 2011), followed by subsequent legislation throughout the early 1990s. At that time, prevention programmes focused on mandating correct labelling and improved warning messages on packages, strict advertising bans, tax and price increases, ultimately contributed to a 46 per cent reduction in adult smoking from 1989 to 2010(WHO, 2015). Efforts to prevent the rise of overweight, obesity, and type-two diabetes also emerged as early as 1999 with the Politíca Nacional de Alimentação e Nutrição (PNAN, National Food and Nutrition Policy). The PNAN introduced several prevention efforts, such as increasing awareness through the media, funding for improved school nutrition, and training for healthcare workers (Monteiro et al., 2002). A phalanx of national programmes emerged up through 2010, focusing on improved nutrition in schools, culminating through the creation of the Plano de Ações Estratégicas para o Enfrentamento das Doenças Cronîcas Não Transmissíveis (DCNT) no Brasil, 2011-2020 (Strategic Action Plan for Tackling Non-Communicable Diseasesa (NCDs) in Brazil, 2011-2020), which addressed several NCDs, for example, obesity, type-two diabetes, and hypertension, and provided funding for additional prevention and treatment services through increased investments in primary care and training (Brazil, Ministry of Health, 2012; Gómez, 2015). Finally, by 2005, efforts were made to address the rise in cancer cases through the National Policy for Oncological Care (NPOC), which provides insurance through SUS for all stages of cancer (Santos et al., 2017). This programme also provides funding to increase awareness of different types of cancer, prevention activities, diagnosis, treatment, rehabilitation, and palliative care (Miranda et al., 2016). In 2013, these services were further strengthened through the 2013 National Policy for Cancer Control and Prevention (NPOC) (Miranda et al., 2016).
When it came to implementing tobacco legislation, as early as 1999 substantive efforts were made to enforce federal laws through ANVISA (Agência Nacional de Vigilância Sanitária [the National Public Health Surveillance System]) and INCA (Instituto Nacional de Câncer [the National Cancer Institute]), which, in turn, manages the National Commission of Tobacco (subsequently renamed in 2003 as the National Commission for the Implementation of the WHO Framework Convention for Tobacco Control [CONICQ, Comissão Nacional para a Implementação da Convenção-Quadro]) (Iglesias et al., 2007). INCA co-ordinates and works closely with the State health secretariats (SES) to ensure effective policy implementation, facilitated by the creation of State Working Agreements providing SES with technical training (Iglesias et al., 2007). Studies reveal that most municipal health agencies have succeeded in adopting federal laws and consistently working with INCA to achieve this goal (Iglesias et al., 2007).
With respect to overweight, obesity, and type-two diabetes, implementation efforts were further aided with the creation of the Núcleo de Apoio á Saúde da Família (NASF, Family Health Support Center) in 2008. Comprised of a group of therapists, nutritionists, and psychologists, NASF primary care teams, which are contracted, funded, and managed by the national MoH, follow up with the patients initially served by SUS’s primary care Family Health Program to ensure that they are adhering to the latter’s medical treatment procedures and lifestyle changes (Jaime et al., 2011). Finally, studies reveal that SUS has done a good job of guaranteeing and implementing access to cancer prevention and treatment services through public hospitals and centres, such as the High-Complexity Centers of Oncology, which date back to 1998 (Cecilio et al., 2015; Floriani, 2008); nevertheless, more effort is needed to address regional inequalities in care.
Historically, particularly during the Gutelio Vargas dictatorship (1930–1945), the MoH had a great deal of centralised policy-making autonomy, influence, and success in eradicating disease (Hochman, 1998). Beginning with the transition to a participatory form of democracy during the 1980s, however, it seems that the MoH began to take on a different role, acting more as a co-ordinator and representative of ideas and interests from civil society, such as through the pro-democratic sanitarista (sanitary) movement (which advocated for healthcare as a human right), during the agenda-setting process (Falleti, 2009).
Indeed, during the formation of the aforementioned Strategic Action Plan , Hallal et al. (2014) claim that the General Coordination of Non-Communicable Diseases and Injuries (CGDANT), which was located within the MoH, co-ordinated the Strategic Action Plan’s creation. The Strategic Action Plan was the product of a dialogue with other federal agencies and civil society, while society’s views, including NCD patients, were incorporated into the Strategic Action Plan (Hallal et al., 2014). A report by the MoH also explains that this plan “… counted on the collaboration of education and research institutions, several ministries of the Brazilian government, members of NGOs … associations of chronic disease patients, among others,” and that organising several meetings with these actors were necessary in order to “… gather suggestions from the different sectors of society to come up with intervention plans …” (Brazil, Ministry of Health, 2011: 8). Even before the Strategic Action Plan was created, however, Malta et al. (2016) claim that when the MoH devised its National Health Promotion Policy in 2003, which influenced several of the aforementioned NCD programmes, its emergence and subsequent transformation benefited from partnerships and suggestions from civil society, such as academic researchers, councillors, and workers (Malta et al., 2016).
Therefore, rather than maintaining its tradition of being a centralised, powerful and autonomous bureaucracy, since the transition to democracy, it appears that Brazil’s MoH has played the important role in acting as a co-ordinator and supporter of civil society’s views and NCD policy preferences. In this context, civil society could rely on the support of MoH bureaucrats when devising healthcare policy. For as Falleti (2009) explains, this health policy-making process was facilitated by the fact that many sanitarista members had infiltrated the highest tiers of the federal bureaucracy during the 1970s and 1980s, thus sustaining society’s ongoing policy influence. This finding supports other researchers’ claims that the bureaucracy still plays an important role in devising public health policy (Harris, 2017; Rich, 2019).
But why was Brazil’s government capable of achieving an early agenda-setting response to NCDs and why was it successful in implementing policy? These outcomes are particularly puzzling if we consider the presence of low levels of bureaucratic autonomy, weak national political institutions, and the fragmentation of presidential and legislative powers in the domain of healthcare policy.
Three important factors stand out. First, social health movements and NGOs succeeded in helping build an early policy consensus within the MoH. Beginning in the 1960s, there emerged a social health movement dedicated to addressing the harmful effects of tobacco (Portes et al., 2018a). During the 1970s, a social movement led by medical professionals also began to emerge with the goal of minimising and controlling tobacco usage. During this time, this movement worked with national politicians to create the 1985 federal Advisory Group for Tobacco Control, conveniently situated within the MoH (Instituto Nacional de Câncer, 2020; Jaques, 2010). Through this Advisory Group, medical doctors and influential senators proposed several policies prohibiting the usage of tobacco products in public places, private areas, public transportation, and in designated areas; this group built a consensus and presented a bill on these policy ideas in 1986, which was presented to the Congress and President José Sarney (Jaques, 2010). Moreover, the Advisor Group recommended and contributed to the formation of Brazil’s firstnational program for tobacco control in 1986 (and provided subsequent technical assistance to it; Portes et al., 2018b), as well as creating Brazil’s first national day to combat smoking campaign (Jaques, 2010). When it came to tobacco control, as early as 1996, NGOs also played a prominent role in helping emphasise the creation of national prevention programmes through the first Brazilian Congress for Tobacco Control (Iglesias et al., 2007). NGOs, such as the Brazilian Medical Association (AMB, Associação Médica Brasileira), and the Alliance for Tobacco Control Health Promotion (ACT, Promoção da Saúde), have also periodically worked with the Congress to propose amendments to existing legislation, have helped to implement programmes introduced by the National Program for Tobacco Control, and have played a vital role in advocacy (Mirra and de Carvalho, 2017; Portes et al., 2018a).
With respect to overweight and obesity, as early as the 1970s, women’s groups were also instrumental in working with the MoH and the Congress to raise early awareness about the importance of improved nutrition, especially for women and children, and access to good quality food (Gómez, 2018a). By 1993, a social movement also emerged, known as the Ethics and Politics of Action of Society Against Hunger, Misery, and Life, to form the CONSEA (Conselho Nacional de Segurança Alimentar e Nutricional [National Counsel for Food and Security]); Jornal da USP, 2019). Located within the office of the presidency, CONSEA was a national consultative body comprised of activists and health officials, with a focus on food security and nutrition, grounded in human rights principles. Although CONSEA closed in 1994 due to a political transition, during the Fernando H. Cardoso administration, civil society worked with and within government through the Programa Comunidade Solidaria (Community Solidarity Programme), via federal constitutional decree, with a focus on poverty and hunger eradication (Ministério da Saúde, 2006); through its representation in this programme, society’s interests, ideas and values helped shape the MoH’s first national NCD programme, the PNAN (Bomtempo Birche de Carvalho et al., 2011). CONSEA re-emerged in 2003 under the Lula administration and served as a participatory institution in dialogue with the government (Bomtempo Birche de Carvalho et al., 2011). Still located within the office of the presidency (Leão and Maluf, 2012), CONSEA continuously advocated and negotiated with the Lula administration to introduce nutrition and NCD programmes, such as securing funding for the Programa Nacional de Alimentação Escolar (PNAE, National Programme for School Nutrition; Leão and Maluf, 2012), which is critical for helping combat childhood obesity.
Efforts to prioritise the creation of a national cancer programme during the 1990s also benefited from several NGOs throughout Brazil (Perez et al., 2014). In addition, work by Deprá et al. (2015) revealed that civil society took advantage of a partnership with the executive branch and presence within national representative institutions, such as the Conselho Nacional de Saúde (CNS) (National Health Council) and the MoH’s CONITEC (Commisão Nacional de Incorporação de Tecnologias no Sistema Único de Saúde [National Committee for Health Technology Incorporation]), which focuses on health technology assessment, to inform the public, monitor policies, and exert pressure on the executive branch for access to breast cancer medicine via SUS.
Civil society has also played a proactive role in monitoring and holding municipal health departments accountable for policy effectiveness. This has been facilitated by the presence of municipal health councils, guaranteeing the representation of civil societal interests in policy-making and budgeting (Victora et al., 2011). These councils continue to be critical for holding municipal health officials accountable for the implementation of NCD programmes (Gómez, 2018b).
At the same time, state and municipal governments were leading the way in devising NCD prevention programmes, ultimately motivating the MoH to pursue similar kinds of policies. With respect to tobacco control, during the 1980s, several states, such as Salvador and Rio Grande do Sul, began to create their own anti-tobacco legislation, which was adopted by several other cities and eventually the national government (Portes et al., 2018a; Romero and Silva, 2011). Indeed, during the 1980s, Rio Grande do Sul was innovative in creating its state program to combat smoking (Portes et al., 2018a; Romero and Silva, 2011). As Romero and Silva (2011) note, São Paulo was also an early policy innovator, creating several anti-tobacco measures, such as a state law banning smoking in public offices, while creating its own program to control tobacco within the state’s secretariat of health. Furthermore, in 1979, meetings were held in São Paulo between regional leaders, scientific associations, and representatives from the University of São Paulo and the Brazilian Medical Association (AMB), to create the first national program against smoking in Rio that year; this programme served as the basis for the National Program for Tobacco Control within the MoH (Mirra et al., 2009). Indeed, Jaques (2011) writes that the national programme was based on the programmatic work and meetings in 1979, led by the BMA, and that the idea for the national programme – emerging from São Paulo that year – was discussed in a national symposium in 1986. Furthermore, in 1980, the state of Paraná created its own policies, such as the Greve do Fumo (“smoke strike”), and provided an example for the first Federal Law on tobacco control in 1986 (Romero and Silva, 2011).
With respect to overweight, obesity, and type-two diabetes, the cities of São Paulo and Rio experimented with improved nutritional and physical activity programmes in schools, well before the aforementioned national programmes. According to Reis et al. (2011), for example, states such as Santa Catarina began to monitor and regulate the quality of foods sold in canteens via state law; other states, such as São Paulo, Rio Grande do Sul, Paraná, and Mato Grosso, followed suit. Thus, in the case of Brazil, this bottom-up diffusion process joined and built upon the presence of proactive civil societal actors within government to incentivise the prioritisation of NCD programmes.
These bottom-up diffusion processes were facilitated by the structure of Brazil’s healthcare system. Brazil has a unified, single-payer public health insurance system, SUS, which is decentralised and provides universal health insurance coverage. While the federal government, states, and municipalities finance SUS (though with the municipalities bearing most of the financial burden in recent years), since 2000, the municipal governments have borne the responsibility of administrating and implementing health policy (Gómez, 2011; Rich and Gómez, 2012). A key governance aspect of this unitary system, however, comprises the inter-governmental (national-state) and inter-regional (between-state) institutions that allow for the sharing of policy recommendations and are important for formulating the MoH’s policy agenda. The MoH, for example, organises the Conselho Nacional de Saúde (CNS, National Health Council), which meets each month, as well as the annual Conferencia Nacional de Saúde (CONASEMS, National Health Conference), which provides additional venues through which national, state, and municipal healthcare officials can share policy experiences and recommendations (da Silva and Lima, 2019). The CNS is comprised of government officials, private health insurance representatives, and civil societal actors (academics, healthcare activists), with the latter playing a key role in policy agenda-setting processes (da Silva and Lima, 2019). Furthermore, through the Colegiados ou Comissões de Gestão Regional (Collegiate or Regional Management Committee), state and municipal health secretariats periodically meet to share policy experiences, provide recommendations, learn, and, in some instances, provide technical assistance (Souza and Bomfim de Souza, 2017). These institutional venues have been instrumental for facilitating sub-national governments’ ability to share critical NCD policy experiences and for bottom-up policy diffusion to occur.
Finally, epistemic community experts helped in shaping the MoH’s interest in NCD policies at an early point in time. As Haas (1992) explains, epistemic communities are distinguished by their command of specific technical knowledge and similar principled beliefs in policy reform, which, in periods of uncertainty, incentivise politicians to turn to them for advice. Similarly, in Brazil, the MoH was historically committed to working with scientific experts within international organisations, such as PAHO and WHO, to obtain advice and guidance when devising NCD policies. For example, as early the 1970s, Brazil’s Food and Nutrition Surveillance System (SISVAN, Sistema de Vigilância Alimentar e Nutricional) – which monitored the country’s nutritional situation and food consumption patterns, particularly for those most at risk – was a product of recommendations from WHO, PAHO, FAO, and UNICEF (Brazil, Ministry of Health, 2006). PAHO was also an instrumental partner in helping design NCD programmes early on in Brazil, emphasising nutrition and food programmes, diabetes prevention and management, promoting physical activity, and surveillance (Brazil, Ministry of Health, 2006). Indeed, PAHO organised “discussion forums” when Brazil’s aforementioned PNAN on nutrition was being designed (Brazil, Ministry of Health, 2006, page 55). PAHO also worked early on with Brazil’s National Tobacco for Control Program to implement the 2003 Framework Convention on Tobacco Control Program (FCTC), on issues such as regulating tobacco advertising, new taxes, and warning labels on packages (Pan American Health Organization, 2012).
This commitment to working with these epistemic communities was in large part shaped by the government’s historic commitment to multi-lateralism in global health. Since the early twentieth century, the government was committed to displaying solidarity with the international community in learning about new policy ideas and working with other nations to eradicate disease and improve population health (Gómez, 2018a).
Mexico
In contrast to Brazil, historically Mexico has had a dominant political party system since the 1930s, governed by the Partido Revolucionario Institutional (PRI, Institutional Revolutionary Party). With the exception of a brief six-year period when the opposition, the Partido Acción National (PAN, National Action Party), won the presidency under Vincente Fox (2000–2006), the PRI occupied the office of the presidency and most of the Congress (Crespo, 2004). In contrast to Brazil, political power is heavily centralized in Mexico, with most powers found in the Congress and office of the presidency. While Mexico’s presidents do not have access to executive decree authority, they do exercise strong reactive veto powers, while the president’s role as leader of the governing majority PRI in the Congress in the past often facilitated their ability to pass preferred legislation (Peschard-Sverdrup and Rioff, 2005). Indeed, when the PRI dominated both the Congress and senate until 1997, essentially all policy-making powers resided in the office of the presidency (Peschard-Sverdrup and Rioff, 2005). In recent years, however, the president’s powers under a divided Congress have declined, and – when combined with the rise of opposition parties – have required the president to obtain opposition support for major policy legislation (Peschard-Sverdrup and Rioff, 2005). Nevertheless, the president and the PRI continue to retain considerable veto powers, helping maintain the status quo, while informally the president’s appointment of ministers and future presidents continues to secure their political power and policy-making influence (Edmonds-Poli and Shirk, 2016).
When it came to the creation of NCD policies, however, notwithstanding this concentration of political and policy-making authority and interests in reform (especially before 1997), policy agenda-setting was considerably delayed. With respect to tobacco control, for example, national programmes were not drafted until January 2004, through the Congress’s Law for the Protection of the Health of Non-Smokers in the Federal District, only to be rejected via presidential veto that same year (Tobacco Facts, 2018). That same year, however, the congress ratified the international FCTC agreement, leading to several taxation policies on cigarettes, warning labels, and restrictions on advertising (Reynales-Shigematsu et al., 2015). In 2008, the Law for the Functioning of Commercial Establishments prohibited smoking in enclosed public places, while the Senate created the General Law on Tobacco Control, mandating designated smoking areas in all establishments (Reynales-Shigematsu et al., 2015).
When compared to Brazil, efforts to address overweight, obesity, and type-two diabetes were also considerably delayed. In 2006, the government’s first attempt to increase awareness and prevention through media outreach was conducted via the PrevenIMSS programme; and yet, the National Social Security Institute (IMSS, Instituto Mexicano de Seguro Social) failed to co-ordinate with the Secretary of Health (SoH) and other federal insurance agencies, thus limiting PrevenIMSS’s potential (Barquera et al., 2013). In 2010, the Congress then created the National Agreement for Healthy Nutrition (ANSA, Acuerdo Nacional para la Salud Alimentaria), which sought NCD prevention through the regulation of the fast-food industry, promotion of behavioural lifestyle changes, and improved nutrition in schools (Barquera et al., 2013). Finally, in 2014, the SoH created the National Strategy for the Prevention and Control of Overweight, Obesity, and Diabetes, which promoted lifestyle changes and improved primary care services and fiscal policies, such as imposing a soda tax (Gómez, 2017).
The establishment of national cancer control programmes was the most delayed, however, notwithstanding the fact that cancer was the third leading cause of death in Mexico (Reynoso-Noverón et al., 2016). It was not until 2016 that the government considered the creation of the National Program for Cancer Control (Reynoso-Noverón et al., 2016). Until then, Mexico’s fragmented healthcare system, consisting of several national insurance programmes (as will be discussed shortly), provided cancer prevention and treatment services on their own, without any effort to co-ordinate between these federal programmes (Strasser-Weippl et al., 2015).
Furthermore, notwithstanding Mexico’s concentration of political authority, policy implementation has not been successful across these NCD sectors. With respect to tobacco control, the SoH has failed to adequately work with the states and local communities in order to enforce the aforementioned tobacco legislation, while its voluntary approach to inducing corporate compliance to federal regulations has not been effective (Novotny and Mamudu, 2008; Thrasher et al., 2008). Instead, researchers find that activist NGO groups have done a better job of linking these policies with increased civil societal support and compliance through aggressive public media campaigns (Gneiting, 2016).
The SoH’s efforts to work with the state governments in order to enforce regulations that prevent overweight, obesity, and type-two diabetes, especially among children, such as limiting the sale of sugary/fatty foods in schools and advertising, also appear to fall short of meeting national policy objectives (Théodore et al., 2018); this has mainly been due to the industry’s – once again – voluntary agreement with the government and the provision of self-regulation (Barquera et al., 2013) processes, seemingly done to avoid further industrial opposition, placate corporate interests, and maintain political support. In contrast to what we saw in Brazil, moreover, the SoH and its public primary care system, mainly through Seguro Popular (Popular Insurance) and IMSS, have not developed any programmes to work closely with families and/or schools in order to ensure that SoH programmes are enforced and meet the latter’s goals (Gómez, 2018b; Théodore et al., 2018). However, the Congress’s decision to impose a soda tax in 2013 has been enforced and thus far has yielded some positive results in reducing the consumption of soda products, though more so in the urban areas (Sanger-Katz, 2017). Finally, because Mexico’s National Program for Cancer Control is so new – providing insufficient time to assess the resulting prevention, treatment, and cancer registry endeavours – not enough time has elapsed to assess if it has been successfully implemented (DePinho and Hawk, 2016; Lazcano-Ponce et al., 2016).
But why was Mexico so delayed in prioritising the creation of NCD programmes and ineffective at implementing them? One reason has to do with the type of state–civil societal partnership that exists. That is, despite the strong concentration of political authority and interest in policy reform, in contrast to what we saw in Brazil, historically the government was never committed to working closely with civil society and other external actors, such as labour unions, when it came to health policy decision-making processes, a process that was dominated by the office of the president (Gonzalez-Rossetti, 2001); this, in turn, failed to provide much needed information as well as generate ongoing pressure on politicians to create and implement policies in a timely manner. Especially in the areas of tobacco control, for example, some claim that civil society’s role in the policy process has been dubious, which may be a reflection of the government’s top-down corporatist governance structure (Thrasher et al., 2008). This dilemma may also reflect civil society’s disbelief in their ability to influence policy given the general lack of a tradition where society’s views are taken seriously, such as in the areas of food policy (Rosenberg, 2015). While NGOs such as El Poder del Consumidor were successful in increasing awareness about obesity and pressured the government to adopt a soda tax (El Poder del Consumidor, 2011), these efforts are new, and no evidence suggests that this organisation had a direct impact on policy design. Moreover, in this context, civil society has not played an important role in helping state and municipal healthcare agencies monitor and implement policy effectively.
In addition, the historic absence of “bottom-up” diffusion processes hampered the early prioritisation of NCD programmes. When compared to Brazil, efforts to decentralise financial resources and administrative responsibilities were considerably delayed, emerging mainly in the mid-1990s, increasing over time (Gómez et al., 2008). By 2006, the federal government retained approximately 43 per cent of the budget for public sector spending, whereas in 1990, it controlled 60 per cent; by this point in time, moreover, the federal government increased fiscal transfers for the financing of health and other social welfare policies, such as infrastructure (Gómez et al., 2008). However, the states and municipalities have, for the most part, still been dependent on the central government for determining funding allocations and policy decisions in the area of public health (Arredondo and Orozco, 2006). In this context, lacking adequate policy-making autonomy, local governments did not engage in early NCD policy innovations, promoting new ideas in tobacco control, obesity, and cancer prevention adopted at the national level. To date, essentially all of the NCD programmes mentioned earlier were created at the national level first, with policy recommendations subsequently imposed onto the states. The absence of these “bottom up” diffusion processes, then, did not contribute to early policy innovations, as seen in Brazil.
And yet, the structure of Mexico’s healthcare system has also hampered bottom-up policy diffusion from occurring. In contrast to what we saw in Brazil, Mexico has a fragmented healthcare system, with several public and private healthcare providers. In the public sector, insurance providers include IMSS, Seguro Popular, Instituto de Seguridad y Servicios Sociales de los Trabajadores de Estado, ISSSTE (State Employees' Social Security and Social Services Institute, and Pemex (a Mexican state-owned oil company). Furthermore, these public providers differ as to which level of government manages their finances and administration, with Seguro Popular primarily controlled by the state governments and the rest by the federal government (Homedes and Ugalde, 2009). And in contrast to what we saw in Brazil, there exists no well-co-ordinated, consistent inter-governmental co-ordinating body that facilitates discussion and policy learning between the national and state governments. Instead, there has tended to be a great deal of conflicting interests and lack of co-ordination between the national and state governments over the provision of insurance programmes and coverage for NCD programmes (Barraza-Lloréns et al., 2002).
Finally, in contrast to what we saw in Brazil, epistemic communities of NCD policy experts did not have an early influence on NCD policies in Mexico. To the authors’ knowledge, Mexico’s SoH never participated in international PAHO or WHO conferences on NCDs during the 1990s or early 2000s. Instead, it appears that the government’s engagement with international scientific health experts, and thus the latter’s NCD policy influence, emerged after NCDs had already become a national government priority. For instance, it was not until after the creation of the aforementioned ANSA on obesity and diabetes prevention that the SoH started to work with PAHO. At that time, the SoH worked with PAHO through a task force regulating the marketing of junk foods to children (Barquera et al., 2013). Mexico subsequently engaged PAHO NCD experts through a 2011 international workshop organised in Mexico, attended by several other countries and international agencies, on NCD economic implications and policy prioritisation (Hospedales et al., 2012).
But why was this the case? First, unlike Brazil, we found no evidence suggesting that Mexico had a long history of engaging in global health diplomatic relations, striving to work with other nations to combat disease and to increase its international reputation in health. While Mexico has certainly co-operated with international health agencies, such as the UN, Organization of American States (OAS), and regional entities such as the Mesoamerican System of Public Health, both with respect to receiving and donating technical support (WHO, 2016), these efforts are more recent. Second, historically healthcare policy-making has been a political elite-driven process, where presidents and secretaries of health have never sought external technical advice, either from healthcare experts or from civil societal actors (Gonzalez-Rossetti, 2001).
Conclusion
This study has compared the countries of Brazil and Mexico to assess similarities and differences in the timing and depth of NCD policy reform; it is the first article of its kind. It took as its point of departure the assumption, based on the existing literature, that the centralisation of political and policy-making authority and interest is necessary for achieving the timely creation and implementation of public health policies. Nevertheless, the case of Mexico found that these institutional preconditions do not guarantee this kind of policy response. In the absence of strong civil societal pressures institutionalised through representative institutions, bottom-up diffusion through sub-national policy innovation, and ideational influence of international epistemic communities early on, policies were considerably delayed and ineffectively implemented.
In contrast, the case of Brazil suggests that democracies exhibiting low levels of centralised political and policy-making authority can demonstrate early responses to NCDs and effectively implement policy. In Brazil, this response was the product of well-organised social health movements and NGOs that consistently pressured national presidents, legislators, and the bureaucracy for a timely response to obesity, type-two diabetes, cancer, and tobacco control; these pressures, moreover, were facilitated through guaranteed civil societal representation within the Congress and the MoH, undergirded by the 1988 democratic constitution solidifying these participatory rights in policy-making processes. During this period, the bureaucracy also played the important role of co-ordinating these ideas and interests, despite its low level of policy-making autonomy when compared to Mexico. Furthermore, early state government experimentation with prevention programmes generated incentives for national political leaders to introduce similar policy measures early on, thus establishing bottom-up policy diffusion.
Finally, with respect to bottom-up diffusion, Brazil and Mexico’s broader health system context also mattered. When compared to each other, Brazil’s more unified SUS system facilitated policy discussions between the MoH and the state governments through well-established, consistently organised inter-governmental co-ordinating institutions. However, this process was absent within Mexico’s excessively fragmented healthcare system, which hampered the national government’s ability to potentially benefit from these diffusion processes.
Several theoretical and policy lessons emerge from our study. First, our findings suggest that the fusion of centralised political and health policy-making authority with government interest in reform, as seen in Mexico, is insufficient for ensuring a timely and effective policy response to NCDs. Without the incorporation of civil societal views and incessant pressures on policy-makers, as seen in Brazil, this fusion of authority and interest will not translate into timely and effective policy action, precisely because politicians are not held accountable for their actions while having little motivation to learn from early sub-national policy innovations. Second, this article suggests that the constitutionally based representation of civil societal interests and accountability, interests that are facilitated and well-co-ordinated by bureaucratic structures, when combined with bottom-up diffusion processes, may be more important predictors of the early timing and depth of NCD programmes in Latin America – and perhaps other developing nations. This further suggests that future NCD policy studies should emphasise selecting and comparing nations based on the presence of these variables in order to distinguish between different types of institutionalised civic representation and diffusion processes and their impact on the timing and depth of policy reform. While civic representation may be present, future research will need to assess whether or not sub-national governments vary in their ability to devise new policy ideas and initiate and/or engage in policy diffusion processes (Berry and Berry, 2014).
With respect to policy implementation, the case of Brazil suggests that national bureaucrats need access to civil societal allies, such as NGOs, that can hold local governments accountable for implementing national programmes. This finding comports with other research making similar claims with respect to government response to infectious diseases, such as HIV/AIDS (Rich and Gómez, 2012).
There were, nevertheless, several limitations with our study, requiring further research. First, we could have included other countries that exhibited Brazil’s institutional characteristics. While there may not be other countries in Latin America with a combination of Brazil’s fragmented political authority structure and high level of NCD prevalence, future research could compare Brazil with countries outside Latin America. Second, we could combine our focus on NCDs with infectious diseases, such as HIV/AIDS, to see if the global and domestic threats and urgency of the latter prompt a more timely, in-depth response in countries exhibiting a centralisation of political and policy-making authority; this, in turn, would suggest that it is not the design of institutions and power structures, but perhaps elite perceptions, fears, and interests, prompted by mysterious, deadly diseases garnering considerable international pressures, that prompt early policy reform efforts (Gómez, 2018a). In contrast, the absence of these perceptions and global pressures for NCDs may depend on the institutionalisation of civil societal pressures, accountability, and bottom-up diffusion processes.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author Biographies
E-mail:
E-mail: