
Abstract
In recent years, Brazil has been highly revered for its response to HIV/AIDS. Despite the government's delayed response, why and how did the national AIDS program eventually become so successful? This is even further puzzling when one considers the challenges associated with Brazil's decentralized response to healthcare needs, lack of subnational resources and political will to effectively implement AIDS policy. This article maintains that Brazil's successful response eventually required the strategic centralization of national AIDS bureaucratic and policy authority, entailing policies designed to aid local governments while creating fiscal policies incentivizing sub-national compliance with the national bureaucracy and more effective policy implementation. Taking advantage of renewed political support, kindled by international pressures and the president's reputation-building pursuits, the sources of AIDS officials’ success, however, resided not in their technical and financial prowess, but in their ability to forge historically-based partnerships with civic AIDS NGOs and social movements sharing like-minded ideational beliefs in policy centralization. This article also discusses how these findings contribute new insights into theories addressing the reasons for centralization, as well as the ideational sources of gradual institutional change.
Introduction
Understanding the politics of government response to health epidemics has emerged as an important area of scholarly research. Of recent interest is how nations having adopted decentralized approaches to health policy implementation are coping in their ability to contain the spread of HIV/AIDS (Lieberman 2009; Gauri and Lieberman 2006). Given the noted challenges associated with decentralization's impact on policy responses to HIV/AIDS and other diseases (Nathanson 1996; Rich 2009; Gómez 2011), how can nations, especially large democratic federations, overcome these constraints and eventually amass a successful government response? What are some of the innovative strategies that national governments within decentralized federations can take to increase their central policy influence amidst decentralization processes?
Examining the case of Brazil, this article argues that successful government responses to HIV/AIDS entail the gradual centralization of bureaucratic and policy-making processes amidst health policy decentralization. That is, in a context where municipal governments are financially, administratively, and politically incapable of adequately implementing prevention and treatment policy, 1 Brazil's successful response eventually required the gradual expansion and strengthening of the national AIDS bureaucracy (henceforth, the national AIDS program 2 ), which included the delegation of policy-making autonomy, the creation of regulatory institutions, funding for human resources, the provision of universal prevention and treatment policy, as well as the creation of fiscal transfer programs increasing central bureaucratic authority while incentivizing local governments to more effectively implement policy. Taking several years to accomplish, and as Figure 1 illustrates, these outcomes comprise the dependent variable of interest: centralized bureaucratic and policy reform.

AIDS Cases and Deaths in Brazil (1980–Present)
Of course, this is not to say that decentralization can never work and that all municipalities are incapable of adequately implementing AIDS and other healthcare services. As the work of Judith Tendler (1997) shows, some municipalities in the northeast of Brazil, such as in Ceara, have been very effective at achieving this.
Henceforth, the term “national AIDS program” will refer to the bureaucratic agency responsible for devising and implementing AIDS policy.
Nevertheless, contrary to scholarly expectations that democratic institutions, electoral accountability, and civic pressures motivate governments to immediately respond to AIDS (Ruger 2005; Sen 1999), it is also important to note that like many nations the Brazilian government did not immediately respond in this centrist manner. As Figure 1 illustrates, Brazil's delayed response kindled an international response that served as the initial incentivizing causal forces in this article: that is, international criticisms and pressures from international scientists and organizations by the end of the 1980s, followed by the Brazilian President, namely Fernando H. Cardoso's (1994–2002) concern with the government's international reputation as a modern state capable of eradicating AIDS. As seen in Figure 1, this incentivized President Cardoso to delegate more policy-making autonomy while authorizing greater funding for the national AIDS program. Amidst an economic recession, the arrival of funding from international creditors, such as the World Bank in 1993, also provided the means through which President Cardoso could achieve his reputation-building pursuits.
Next, this new level of political support provided a window of opportunity for previously marginalized AIDS officials to engage in a gradual process of centralized bureaucratic and policy reform. Concerned with the limitations associated with decentralization, officials sought centrist ideas and strategies that had a long historic precedent, legitimacy, and proven track record of containing disease. But what did this gradual centralization process look like and how did AIDS officials achieve this? And where did the sources of their legitimacy and influence come from?
As Figure 1 explains, as a subsequent and distinct causal process, where international pressures and reputation-building was not of concern, it is argued that the sources of AIDS officials’ strength resided not in their finances and technical skills, but in their partnership with interest groups, such as non-governmental organizations (NGOs), as well as social movements. More specifically, the national AIDS program's gradual expansion rested on officials’ ability to solidify their partnership with AIDS NGOs and the sanitarista 3 movement. By forming partnerships based on similar ideational beliefs in the importance of a centralized bureaucratic and policy response, ideas and their supportive state-societal partnerships that spanned back to the early-20th century, AIDS officials’ legitimacy and influence substantially increased, in turn helping them obtain ongoing financial and political support. In addition, and as Figure 1 illustrates, beginning in the early-1990s the gradual infiltration of former AIDS NGO members and state AIDS officials into the national AIDS program was needed in order to facilitate and achieve this process; more specifically, their hiring provided yet another advantage for the AIDS program in that it increased the number of AIDS officials committed to policy centralization, helped devise such policies based on experiences obtained from the sub-national level, while bringing with them previously established partnerships with NGOs and the sanitarista community, thus facilitating the program's relationship with these groups.
Created in the 1960s, the sanitarista movement was a leftist civic and political movement dedicated to democratization and providing universal healthcare as a human right.
Methodology
With regards to methodology, this article employed a qualitative single case study design. This study purposely selected on the dependent variable, that is, Brazil's well known successful response to HIV/AIDS, in order to further analyze the case and devise new hypothesis that can be subsequently explored (Collier and Mahoney 1996). Following the method of “causal process observations” (Collier, Brady, and Seawright 2004), the case of Brazil was also used to confirm the efficacy of theories addressing the reasons for bureaucratic and policy centralization by using the author's in-depth contextual knowledge of Brazil to confirm the causal mechanisms that these theories claim lead to centralization. This case was also used to underscore the limitations in the literature discussing centralization as well as the literature addressing the importance of political and constituent support for new reform ideas, with the goal of establishing a deviant case study, helpful for creating new hypothesis (George and Bennett 2005). Yet, because the author did not take the extra step of testing the new hypothesis with other randomly selected cases, theory-building was not the end goal (Eckstein 1975).
With regards to empirical data, the author relied on several sources. First, in-depth interviews were conducted with former elected officials, national AIDS officials, and activists from NGOs; their views and opinions were unknown prior to the interview. Second, archival newspaper clippings were randomly selected and obtained from NGOs in Brazil, while journal articles, books, and reports were used as qualitative evidence. Moreover, this literature was not selected based on any biased views supporting the author's claims, but rather on their high quality – often peer reviewed – discussion of Brazil's response to AIDS.
Decentralization, Centralization, and the Ideational Sources of Institutional Change
In a context where governments are constitutionally committed to decentralization, why do they eventually respond in a centralized manner when health epidemics emerge? This is particularly surprising if one considers the climate of democratic decentralization and international health organizations pressuring for the decentralization of healthcare services (Manor 1999). Recent research nevertheless notes that the reasons why nations eventually pursue bureaucratic and policy centralization is often due to sub-national health policy inefficiencies and delayed responses to disease. First, some scholars underscore a growing trend in Western Europe that decentralization's failure to provide adequate healthcare services eventually requires the central government to claw back health policy decision-making and financing, leaving limited administrative responsibilities to local governments (Saltman 2008; Saltman, Bankauskaite, and Vrangbaek 2007).
Second, others maintain that in response to epidemics, nations pursuing a centralized bureaucratic response are more effective in devising prevention and treatment policies. For example, work by Constance Nathanson (1996) explains that a successful policy response to AIDS and maternal and infant mortality in France depended on the immediate centralization of policy-making autonomy, receptivity to scientific evidence and consulting, as well as a pre-existing political proclivity for centralization. The benefits of policy centralization have motivated others to argue that when providing infant immunization and HIV treatment, non-democratic and/or highly centralized states are more effective than representative democracies in providing these services (Gauri and Khaleghian 2002).
And finally, there is now an international consensus that nations should pursue a centralized response to HIV/AIDS. For example, Lieberman (2009) claims that since the early-1990s, a new “Geneva Consensus” for policy responses to HIV/AIDS has emerged, with the United Nations (UN) recommending governments to strengthen their national AIDS bureaucracy (as well as prevention and treatment services) by ensuring that there is adequate human resources and training (Lieberman 2009). Lieberman goes on to mention that health officials from developing nations have often been pressured into agreeing to adopt these policies, both informally either through policy seminars at UNAIDS conferences or formally through peer pressure (Lieberman 2009).
In this article, Brazil's centralized response to HIV/AIDS supports the aforementioned views that centralization should be pursued when decentralization falls short of effectively rendering healthcare services in response to HIV/AIDS, as well as when trying to facilitate the policy-making process. Yet as the case of Brazil illustrates, centralized bureaucratic and policy reform was not the product of international pressures but rather historically-based domestic ideas and beliefs that centralization should be pursued in response to epidemics. The aforementioned literature overlooks the fact that nations may have a deep historical ideational and political commitment to pursuing a centralized response to eradicating epidemics, and that these historic precedents may be more important than international pressures.
But who are the political, bureaucratic, and civil societal actors involved in this centralization process and what does it look like? Moreover, how and why do historical ideational precedents and bureaucratic-NGO and social movement partnerships facilitate contemporary reform actors’ ability to pursue centralization?
Enhancing our Understanding of the Sources of Institutional Change
It is argued that understanding why gradual institutional change occurs in response to health epidemics requires that we carefully assess the role and influence of interest groups, e.g., NGOs, and social movements in this process. While the mobilization of NGOs and social movements may not succeed in immediately pressuring the national government for reform, the former can nevertheless play a key role at the sub-national and eventually national-level. While AIDS NGOs and state health officials committed to social movements can pressure sub-national governments to create AIDS programs in the absence of federal intervention (Parker 2003), this article also argues that they are important for gradually helping increase commitments to policy centralization at the national level. This occurs when former AIDS NGO members and state AIDS officials desiring a centralized response are hired to work for the national AIDS program, joining other AIDS officials in their commitment to pursuing such a response. This gradual infiltration is needed in order to help the national AIDS program achieve a centralized response. Resembling what Mahoney and Thelen (2010) call subversive change actors, who seek to gradually reform institutions from within based on policy ideas developed elsewhere, 4 these individuals infiltrate the bureaucracy, wait for their time to emerge and when it does, they help pursue policy goals and ideas that they acquired from other areas, such as subnational government (Falleti 2010).
According to Mahoney and Thelen (2010), subversive change actors are those that gradually infiltrate institutions with the ultimate goal of displacing them. Initially, these change actors abide by institutional rules, appearing to support them while pursuing alternative policies on the fringes, e.g., at the sub-national level. According to Mahoney and Thelen (2010), while experimenting with policies and indirectly encouraging others to pursue institutional change, these change actors wait to take advantage of openings within existing institutions, e.g., such as new reform ideas created at the national level, to pursue their alternative policy designs. Subversives therefore bring change as policy developments on the periphery make their way to the center. Therefore according to this definition, subversives join other change actors within pre-existing institutions that are seeking similar types of reforms and coalitions, i.e., those actors that provide a new opportunity space for reforms. Subversives may therefore join and further aid new, pre-existing reform coalitions and policy interests.
In an effort to achieve a centralized response, an enlarged national AIDS bureaucracy eventually strengthens their partnerships with NGOs and social movements, gradually galvanizing their connections through the sharing of similar policy ideas and experiences. AIDS reformers’ ideas are predicated on the following principles: that the state should provide universal healthcare as a human right; that it should implement aggressive prevention and treatment policies; and that it should have a strong partnership with civil society. Eventually this provides national AIDS officials with the NGOs and social movements needed to increase their legitimacy and influence when seeking ongoing financial and political support for a centralized bureaucratic and policy response.
What this in turn suggests is that scholars should pay more attention to the strategies that reformers use to ensure that their ideas lead to bureaucratic and policy centralization, as well as the preexisting historic ideas and coalitions that embolden these efforts. For even if similar reformer-minded individuals gradually infiltrate the bureaucracy, there is no guarantee that this will lead to centralization.
Indeed, this article breaks bread with Lieberman's (2002) and Berman's (2001) assertion that the emergence of new ideas proffered by what Berman calls idea “carriers, entrepreneurs” (Berman 2001: 235) does not guarantee that they will immediately lead to institutional change. As discussed above, long held bureaucratic ideas do not become influential until presidents, prompted by international pressures, start to consider them – or rather, when a new window of opportunity emerges. What therefore leads to the emergence of successful ideas is the rise of new supportive coalitions and influential ideational carriers (Lieberman 2002; Mahoney and Thelen 2010).
But what is lacking in the works by Lieberman (2002) and Berman (2001) is how the history of similar pre-existing ideas and supportive coalitions provides contemporary reformers with even greater legitimacy and influence when pursuing institutional change. That is, how reformers’ ideas resonate with historic beliefs in a centralized response to epidemics, as well as reformers’ establishment of partnerships with NGOs and social movements believing in the same. 5
This does not mean that contemporary ideas reflect preexisting ideas that are passed down over time; such a reproductive process would require reactionary mechanisms and the ongoing passage of legacies generating sunk costs.
As the case of Brazil in this article illustrates, the causal chain in this process proceeds as follows: concerned with decentralization's ineffective response to AIDS, national AID officials emerge with interests in a centralized response; next, they seek out and use AIDS NGOs and social movements that share similar ideas and beliefs, ideas that, unbeknownst to these NGOs and social movements, date back to similar responses in the early-20th century; next, reformers’ knowledge of this history, as well as AIDS NGOs periodically reminding them, generates incentives to continuously work with AIDS NGOs and social movements; this partnership increases the legitimacy and influence of reformers’ ideas, especially when compared to contemporary policy alternatives, such as decentralization. Reformers finally succeed in pursuing a centralized bureaucratic and policy response to AIDS.
The Early Years of the AIDS Epidemic in Brazil
The Brazilian government did not immediately respond to AIDS (Parker, Galvão, and Bessa 1999; Da Costa Marques 2003). The absence of international pressure for a response, the dearth of epidemiological evidence and the challenge of having to respond to multiple diseases convinced the president and several health officials that AIDS did not pose a serious threat (Folha de Sao Paulo 1985; Jornal do Brasil 1985; Gómez 2011). Consequently, there was no political support for those Ministry of Health officials seeking to immediately respond through aggressive prevention and treatment policies (Parker 2003; Gómez 2011; Terto 2008; Da Costa Marques 2003). While the Ministry of Health created a national AIDS program in 1986, and while the program disseminated information about HIV awareness and prevention, it was poorly funded and lacked the capacity to devise effective prevention and ARV (antiretroviral) treatment policies (Teixeira 1997; Parker 2003; Galvão 2000); it isolated itself from the international community under the Fernando Collor (1990–92) administration (Nascimento 2005); while it also neglected to work closely with NGOs (Nascimento 2005).
Under these conditions, NGOs and social movements played a key role in fostering a sub-national response (Parker 2003; Berkman et al. 2005; Teixeira 1997). Interest group mobilization in response to AIDS first emerged in São Paulo, when the gay community pressured São Paulo's State Secretariat for Health, João Yunes (1983–87), for the creation of an AIDS program (Parker 2003). The gay movement's efforts dovetailed nicely and benefited from the presence of a vibrant public health social movement pressing for democratization, the movimento sanitário (henceforth, the sanitarista movement), which emerged in the 1960s emphasizing access to healthcare as a human right, provided by the state, yet controlled through community ownership and participation (Falleti 2010). These efforts helped to construct the state (and nation's) first AIDS program in 1983 in São Paulo (Teixeira 1997; Parker 2003).
They gay movement's success in São Paulo encouraged the creation of several AIDS NGOs (Parker 2003; Biehl 2004). In 1985, the first AIDS NGO was created, GAPA (Grupo de Apoio á Prevencão á AIDS), followed by ABIA (Associacão Brasileira Interdisciplinar de Aids) in Rio in 1986 (Parker 2003). The success of these NGOs led to the emergence of NGOs throughout the nation, such as other GAPA chapters in Minas Gerais, Rio de Janeiro, and Bahia (Parker 2003; Biehl 2004; Berkman et al. 2005). Establishing solidarity through yearly conferences, these NGOs were committed to helping state governments form AIDS programs, which grew in number to approximately eleven by 1985 (Biehl 2004; Parker 2003; Berkman et al. 2005). NGO efforts were complemented with the support of the sanitarista social movement, which gradually infiltrated state AIDS programs and eventually the national Department of Planning in Brasilia (Falleti 2010). Furthermore, though not integral to the initial movement, the religious and business community eventually joined the cause (Parker 2003). By the mid-1980s, a vibrant network of NGOs, voluntary organizations, and civic leaders emerged to increase awareness, combat stigma, discrimination, and fight for the rights of AIDS victims, while helping construct and maintain state AIDS programs (Berkman et al. 2005; Parker 2003).
While state AIDS programs were developing, a cadre of Ministry of Health (MOH) and AIDS officials at the national level were also committed to creating a strong centralized response to the epidemic. Indeed, while most MOH appointees during this period sided with President Sarney and Collor's views that AIDS did not merit a credible threat worthy of an aggressive response, there were other MOH and AIDS officials that were seeking such a response (Teixeira 1997; Chequer 2008; Teixeira 2007; Terto 2008). Since its inception in 1985, these marginalized bureaucratic reformers were committed to responding in a more centralized, top-down manner (Santos Filho 2006; Chequer 2008; Teixeira 2007; Gómez 2011). Their perceptions were influenced by the MOH's long tradition of responding to heath epidemics through the centralized expansion of the public health bureaucracy as well as financial and technical assistance to the states (Teixeira 2007; Gómez 2011; Hochman 1998). Ensconced in this tradition, AIDS reformers believed that it was the state's duty to guarantee universal access to healthcare, a view that comported with the sanitarista community's beliefs and which was enshrine in the 1988 constitution (Galvão 2005; Berkman et al. 2005; Falleti 2010). Nevertheless, a high level of intra-bureaucratic discord and lack of political will limit AIDS reformers’ ability to pursue a centralized response (Gómez 2011).
Former members of AIDS NGOs and state AIDS officials, many of whom were also part of the sanitarista movement, helped to further strengthen the national AIDS program's commitment to a centralized response and policy-making capabilities (Solano 2000; Nunn 2009; Berkman et al. 2005; Biehl 2004). Hired primarily as consultants beginning in the early-1990s, the national AIDS program was gradually infiltrated and staffed with more individuals believing in AIDS reform officials’ centrist bureaucratic and policy ideas (Biehl 2004; Gómez 2011); this, in turn, helped to increase the number of individuals within the program committed to pursuing a centralized bureaucratic and policy response (Nunn 2009; Galvão 2005; Biehl 2004; Berkman et al. 2005). Selected for their extensive policy experience at the state level, these new individuals also facilitated and helped AIDS officials expedite the creation and implementation of more effective, centralized prevention and treatment policies, which were often inspired by policies successfully developed at the state level (Nunn 2009; Camara 2002). Indeed prior to their arrival, these individuals had implemented similar centralization ideas through the creation of state government universalistic prevention and treatment programs; they were therefore in simultaneous agreement with national officials over the idea of the need for a centralized response. Eventually, however, tensions emerged between national and state AIDS officials over issues of sub-national policy autonomy when the national AIDS program began to impose its policy prescriptions onto the states (Parker 2003).
The hiring of new individuals with prior advocacy and policy experiences at the state level also helped to prepare the national AIDS program for its work with AIDS NGOs and the sanitarista community. Indeed Darrah (2006) and Nunn (2009) maintain that many of the new hires had come from leading AIDS NGOs. These pre-existing networks and partnerships would eventually help the national AIDS program meet and work with NGOs. Similarly, Darrah (2006) explains that sanitarista state AIDS officials having developed strong networks of support and partnerships with NGOs and the sanitarista community in their cities took these networks and experiences with them to the national AIDS program. This, in turn, would subsequently facilitate AIDS officials’ usage and sustainability of these partnerships, which these officials could eventually draw from and strategically use (Darrah 2006; Abadia 2003) – a successful effort that I will elaborate on shortly.
International Pressures and Centralization
Scholars note that 1986 marked the beginning of a new international movement in response to AIDS (Lieberman 2009). Shortly thereafter, an outpour of international conferences and heightened media attention started to address the epidemic, as well as individual country responses (Lieberman 2009). Criticisms of Brazil's response emerged during this period. In 1987, Dr. Anthony Fauci, Director of the National Institute of Allergy and Infectious Diseases in the US, criticized Brazil for its lackluster response to AIDS, stating that the government needed to confront the epidemic head-on (O Estado de São Paulo 1987). At a conference on the epidemiology and surveillance of AIDS in Latin America held in Puerto Rico that year, Brazil was singled out as having the worst AIDS scenario in the region (O Estado de São Paulo 1987). Additionally, in 1990 the World Bank stated that if the government did not aggressively respond, it would see 1,200,000 cases of AIDS by 2000 (Brazil, Ministry of Health 2005). In 1993, the World Bank further criticized Brazil for failing to invest enough in its public health infrastructure (Gazeta Mercantil 1994; O Estado de São Paulo 1993).
As an emerging nation eager to reveal its developmental potential, these criticisms provided a new opportunity for Brazil to respond and maintain its historic reputation as a leader committed to combating disease. For in contrast to other developing nations, Brazil had a rich tradition of showing the world that it could respond to epidemics in an effective manner (Peard 1999; Hochman 1998). Historically, during the First Republic (1889–1930), and especially during the latter half of the Getúlio Vargas dictatorship (1940–45), Brazil became world famous for its response to syphilis, malaria, and yellow fever, as well as working with other nations to create the WHO in 1942 (Gómez 2009b).
While reformers in the national AIDS program were already committed to responding to AIDS, these international criticisms had a profound impact on the perceptions of the president and senior MOH officials (Fontes 1999). In an in-depth interview with the former two-term President of Brazil, Fernando H. Cardoso, he stated that in response to international criticisms, the Itamar Franco and his administration was eager to pay more attention to the AIDS situation and to show the world that they could effectively curb the spread of AIDS (Cardoso 2007). Cardoso explained that his response was motivated by the fact that the government had a rich tradition and reputation for being world leaders in the fight against disease (Cardoso 2007). He was interested in maintaining this tradition and further increasing Brazil's reputation (Cardoso 2007). Former AIDS officials and scholars support Cardoso's claim (Chequer 2008; D'Ávila 2008; Fontes 1999). In addition, others note that Cardoso was interested in using Brazil's growing recognition in order to increase his influence over AIDS policy in other nations (D'Ávila 2008; Fontes 1999; Gómez 2009a). Responding through more aggressive policy measures was seen as the primary way to achieve this (Cardoso 2007; D'Ávila 2008; Fontes 1999; Gómez 2011).
But was reputation-building Cardoso's only reason for responding to AIDS? Emerging out of a weak government response in the early-1990s and during his presidential campaign, one would assume that Cardoso tried to use the AIDS situation in order to boost his electoral prospects. Yet recent research shows that at no point did Cardoso campaign on the issue (Gauri and Lieberman 2006). And while Cardoso's Minister of Health, Jose Serra, used his success in developing the national AIDS program as an electoral strategy during his presidential bid in 2002 (Nunn 2009; Lieberman 2009), by that point there was already unwavering presidential and legislative commitment to the program and the most important policies were already in place, such as universal access to ARV medication, implemented in 1996 (Lieberman 2009). Instead, Serra's campaigning on AIDS seemed to draw more attention and support for the program and to reinforce the need to continue to invest in it, though by no means was his electoral strategy a key catalyst for reform (Gauri and Lieberman 2006; Lieberman 2009). Alternatively, one could envision Cardoso tackling AIDS in order to enhance his general popularity. Yet again this cannot be true, since others suggest that he was already highly revered for his success in taming inflation through the Real economic stabilization program, which he created as Finance Minister in 1993, and which many attribute to his presidential win that year (Resende-Santos 1997). Alternatively, one could argue that the AIDS epidemic was an unavoidable issue, generating widespread fear, especially after the fact that it had touched the lives of famous artists, actors, and the upper-class, while epidemiologically the virus was at its peak. The problem with this argument, however, is that AIDS had touched the lives of influential people at a much earlier point in time, and that the government already acknowledged the epidemic (Parker 2003). Thus, it was neither political self-interest nor heightened media attention, fear, and unavoidable epidemiological trends that motivated Cardoso to respond. Instead, it was his personal interest in bolstering the broader image of Brazil as a nation capable of eradicating AIDS.
One of the first things the government did to strengthen its reputation was to increase its attendance at international conferences while inviting officials from international organizations to meet with AIDS officials (Da Costa Marques 2003; Galvão 2000). Throughout the 1990s, officials from the WHO, PAHO, and the World Bank were invited to the MOH in Brasília to discuss Brazil's aggressive prevention and treatment programs (Galvão 2000). In fact it was a time when the government was trying to become the world pioneer in response to AIDS (Galvão 2000).
Nevertheless, having the fiscal capacity to achieve these goals was an entirely different matter. By the late-1980s, fiscal instability and hyperinflation burgeoned (Resende-Santos 1997). By 1988, technocrats predicted that the MOH and the AIDS program would lose approximately thirty percent of its budget (Jornal do Brasil 1989). The World Bank noticed these problems and by 1990 was concerned that Brazil would not have the resources needed to mount an effective response (Brazil, Ministry of Health 2005; Beyrer, Gauri, and Vailancourt 2004; Mattos, Terto, and Parker 2003).
With this in mind the prospect of obtaining a generous loan from the World Bank further increased the president and MOH's interests in strengthening the AIDS program (Barbosa 2008; D'Ávila 2008; Gómez 2011). Presidents Franco and Cardoso could now easily achieve their goal of increasing the government's reputation and influence while providing more resources and autonomy to the AIDS program (Gómez 2011).
After several rounds of negotiation, in 1991 the World Bank offered a loan of 120 million USD, with the possibility of being renewed every five years (Beyrer, Gauri, and Vailancourt 2004). The main objective was to dramatically increase federal prevention programs, medical treatment, regulate the blood supply and fund NGO activities (Beyrer, Gauri, and Vailancourt 2004; Mattos, Terto, and Parker 2003). More important for our interests, the new loan clearly stipulated that part of the money be used for strengthening AIDS administration, more specifically, centralizing policy control, expanding staff size, increasing salaries, and providing technical assistance (Lewis 2006; Mattos, Terto, and Parker 2003; Galvão 2000).
But this puts forth an interesting question. Was it the availability of donor assistance for the AIDS program or the president's interest in reputation-building that prompted Brazil's response? I argue that both were important, though reputation-building, as in other countries (McGuire 2010; Sridhar and Gómez 2010; Gómez 2011), was the main catalyst for reform. Hypothetically, the availability of funding without any interest in reputation-building would not have led to an ongoing centralized bureaucratic and policy response, mainly because no historical precedent, legacies, and incentive for reputation-building would have existed. Alternatively, interest in reputation-building without adequate funding would have led to fiscally constrained attempts to pursue a centralized response. Funding from the World Bank thus provided the means through which to achieve a pre-existing desire to expand the national AIDS program after the rise of international pressures (Gómez 2011); donor assistance was not the primary cause (Gómez 2011).
Under these conditions, MOH and AIDS officials finally agreed that a more centralized approach to AIDS policy should be pursued (Terto 2008; Chequer 2008; Teixeira 2007; Gómez 2011). Additionally, President Cardoso gave the AIDS program greater autonomy and authority to conduct policy without having to obtain approval from other executive branches, establishing a precedent that continues to this day (Gauri and Lieberman 2006; Lieberman 2009; Teixeira 1997; Cardoso 2007; Galvão 2000). To expedite policy-making, the AIDS program was also the only welfare agency allowed to directly request congressional funding without having to follow standard application procedures (Moherdaui 2006).
During this period, AIDS officials also agreed that they needed to increase their regulatory authority over the states (Teixeira 1997). Paulo Teixeira (1997) notes that AIDS officials believed that all states and municipalities had to implement its policy prescriptions from Brasília, that they were, in a sense, calling the shots from above (Teixeira 1997). Teixeira also notes that throughout the 1990s, the AIDS program created the Comissões Municipais de AIDS (Municipal AIDS Commissions), which worked with the national AIDS program to regulate and implement AIDS policies (Teixeira 1997: 63). And this occurred despite the expressed discontent of state and municipal health agencies that already had their own AIDS programs in place (Teixeira 1997: 63). And finally, by the mid-1990s a consensus within the AIDS program that reformers needed to work closely with AIDS NGOs in order to strengthen their ability to control the spread of AIDS (Villela 1999; Massé 2009; Galvão 2000).
But why did this happen? Was it merely the president's change of heart and the World Bank loan that sparked reformers’ interest in finally working closely with civil society? Or was there more to it than that? As the next section explains, there was indeed more.
The NGO and Social Movement Sources of Institutional Change
Understanding Brazil's successful centralized response to AIDS requires that we first address the historic genesis of civic mobilization and partnerships with bureaucratic reformers. Ever since the early-20th century, bureaucrats forged informal pacts with public healthcare movements that had a lot of legitimacy and influence through their participation in international and domestic conferences in order to construct highly centralized, autonomous public health agencies (Carrara 1996, 1997; Hochman 1998; Nascimento 1991).
Indeed, during the turn to the 19th century, in addition to other diseases, TB and syphilis arose as health epidemics. While the government did not immediately respond, due to the presence of multiple diseases and demands on the state, the Liga Contra a Tuberculose (henceforth Liga) and the Sifilógrafo civic movements arose in 1899 and 1915 to increase domestic and international awareness and to encourage a centralized bureaucratic and policy response to TB and syphilis, respectively (Filho 2001; Nascimento 2005, 1991; Carrara 1996, 1997). These movements were comprised of medical doctors, scientists, and healthcare professionals. Through their participation in international and domestic conferences, as well as increased awareness through local advocacy and collaboration with churches and philanthropic organizations, such as the Rockefeller Foundation and the Red Cross, their legitimacy and influence increased (Filho 2001; Nascimento 1991; Carrara 1996; Gómez 2008). In addition to their interest in increasing Brazil's reputation as a nation capable of eradicating disease (Carrara 1997; Peard 1999; Nascimento 1991; Filho 2001), these movements were also closely aligned with the international community's preferences – especially in Western Europe – to expand centralized administration and to provide health services for all (Carrara 1996; Nascimento 1991). To that end, they were unwaveringly dedicated to pressing the government for aggressive prevention campaigns and policy treatment (Carrara 1996; Nascimento 1991; Araujo 1939; Filho 2001), while combating discrimination and racism associated with these diseases (Carrara 1996). And finally, they believed in forging partnerships with bureaucrats to achieve these ends (Gómez 2008).
With a president that was seemingly apathetic to the needs of civil society, the rise of these influential civic movements provided a strong partnership that reform bureaucrats could use to convince the government of the need to strengthen public health institutions – namely the Departmento Geral de Saúde Público (DSP) (1900–1930) and the Ministerio da Educacão e Saúde Público (MESP) (1930–45) (Gómez 2008). Reformers used their partnership with the Liga and Sifilógrafo movements to persuade the president that there was a legitimate and immediate need for pursuing a centralized response (Nascimento 1997, 1991; Carrara 1996). For example, the director of DGSP, Dr. Oswaldo Cruz, engaged in a close partnership with the Liga to propose the creation of a new federal agency focusing explicitly on TB (Nascimento 1997, 1991; Carrara 1996). He and other DGSP and later MESP officials also worked closely with the Sifilógrafo movement to increase the former's capacity to intervene at the local level (Carrara 1996).
It is important to note that national bureaucratic reformers’ ideas and preferences for constructing a centralized response comported with the Liga and Sifilógrafo movement's ideas and beliefs. And similar to what we saw with the sanitarista movement and the national AIDS program decades later, even further beneficial for bureaucratic expansion was the fact that several of these reformers emerged from the Liga and Sifilógrafo movements, further galvanizing their ideas and preferences with these civic movements (Carrara 1999). In the end, public health officials viewed establishing partnerships with these movements as a way to increase their power and ability to construct federal agencies (Nascimento 1991, 1997).
AIDS and the NGO and Social Movement Sources of Institutional Change
In contrast to the historic period, however, when AIDS emerged in 1982 there was a new ideational and political commitment to healthcare decentralization. Though not yet formally decentralized in nature, the belief in this process first occurred with the military governments (1964–85), specifically in 1971 with the creation of the Assistance Fund for Rural Workers, FUN-RURAL, which provide healthcare services to the poor in the hinterland (Fundo de Assistencia ao Trabalhador Rural) (Falleti 2010). The most concrete attempt at decentralization came later with the formation of the Program of Internalization of Health and Sanitary Actions, PIASS (Programa de Interiorizacão das Acões de Saúde e Saneamento) in 1976, which delegated to state health departments the task of constructing public health outposts, as well as clean water and sanitation (Falleti 2010). And in 1982, after sanitarista leaders began to occupy important positions in the government (Weyland 1995; Falleti 2010), it authorized the Integrated Health System, AIS (Acões Integradas de Saúde), which sought to delegate more healthcare responsibilities to the states, to create a universal healthcare system emphasizing primary care provision and increased usage of public sector facilities (Harmeling 1999).
Thus the military gradually became committed to the idea that responding to public health problems should be done through decentralization processes (Merhy 1977; Falleti 2010). The military's receptivity and belief in these ideas was the product of the sanitaristas’ gradual infiltration of highlevel government offices, such as the Department of Planning (Falleti 2010; Weyland 1995). The sanitaristas eventually convinced most government officials that health services should be universally accessible and equitable (Falleti 2010; Lobato 2000; Weyland 1995). Moreover, the military viewed their ideas as important for several reasons: decentralization could increase the military's legitimacy and presence in the hinterland (Lobato 2000; Falleti 2010); it could quell rising rural unrest and opposition (Falleti 2010); and it could provide an inexpensive response to providing healthcare needs (Falleti 2010). These beliefs in turn motivated the central government to rely on AIS and local governments as the first responder to AIDS.
After the re-organization of the national AIDS program and arrival of World Bank funding, however, the national AIDS program's ideational belief in decentralization's effectiveness began to decline. AIDS officials believed that decentralization through SUS was not achieving an effective response to healthcare needs and AIDS (Rich 2009): specifically, a reported shortage of beds in public hospitals (Buss and Gadelha 1996); a lack of funding for crucial biomedical tests (Portela and Lotrowska 2006); the absence of advanced x-ray imaging tests (Portela and Lotrowska 2006); low professionalism in service management, limited operational hours and staff meetings (Portela and Lotrowska 2006). Municipal health departments were also becoming notorious for failing to effectively use SUS funding, while neglecting to ensure that hospitals were rendering AIDS and other services effectively (Rich 2009).
In this context, it is easy to understand that by the mid-1990s, the national AIDS program as well as social movements’ response began to mirror what had occurred during the early 19th century, that is, social movements and health officials pursuing a partnership for a centralized response to epidemics. In reaction to an epidemic that was initially ignored by most political and bureaucratic elites, the well-organized sanitarista movement arose to establish partnerships with national AIDS officials (Galvão 2000; Rich 2009; Massé 2009). As others note, shortly after the World Bank loan the sanitarista movement re-emerged as a more organized, globally-connected social movement working to help strengthen the national AIDS program (Villela 1999; Galvão 2000; Rich 2009; Massé 2009). Similar to the Liga and Sifilógrafo movements, the sanitaristas believed in the following principles: that the public health bureaucracy should be strengthened and expand to provide prevention and treatment services for all (Galvão 2005; Falleti 2010); that civil society play a key role in working with government and implementing policy (Merhy 1977); and that civil society and the government work together to increase domestic and international awareness of the need to provide universal healthcare (Rich 2009). Sanitarista members working on AIDS policy by the 1990s therefore shared similar beliefs in a centralized response to the AIDS epidemic (Nunn 2009). Indeed, Nunn (2009) maintains that although many sanitarista members initially supported a decentralized response during the 1980s, by the 1990s, because of the financial and administrative inefficiencies associated with SUS, they shifted their preferences in favor of policy centralization in order to ensure that policies were effectively implemented. Although there were some sanitaristas in state health departments that were in favor of decentralization (Berkman et al. 2005), mainly in order to safeguard their policy autonomy, by the mid-1990s they were certainly outnumbered by those favoring policy centralization (Nunn 2009). National AIDS officials therefore strategically used the historic idea the majority of the sanitarista's espoused of the central government's responsibility of subsidizing AIDS prevention and treatment policies as a justification for an expansion of the national AIDS program and its interventionist strategies.
As mentioned earlier, working with the sanitarista community was also facilitated by the fact that many of its members, who were prior state AIDS officials, had gradually infiltrated the national AIDS program (Berkman et al. 2005; Parker 2003; Nunn 2009). Their gradual infiltration helped the AIDS program in its ability to obtain the support of other sanitarista members, who were also state AIDS officials (Darrah 2006). While in the national program, these infiltrators maintained their ties with the sanitarista community as well as AIDS NGOs, often times gong back to their states and NGOs they were working with in order to follow up on projects that they had previously started (Darrah 2006). By the time AIDS officials were prepared to seek a centralization bureaucratic and policy response, they had amassed strong connections with the sanitarista community based on these experiences, which not only gave AIDS officials more legitimacy but also facilitated their ability to work with the sanitaristas (Darrah 2006).
During the 1990s, the sanitarista's efforts were further strengthened with the presence of well-organized AIDS NGOs. Perhaps more so than the sanitarista movement, and perhaps more similar to the historic Liga and Sifilógrafo movements, AIDS NGOs were well integrated into the international community, attending a host of AIDS conferences, meeting with NGOs in other nations, and working with international organizations, such as the WHO and UNAIDS, to increase awareness of AIDS and the need for governments to respond (Bastos 1999). At the same time, NGOs worked with donors, such as the World Bank, the UK Department for International Development (DfID), and the USAID to encourage nations to integrate civil society into the policy-making process (Bastos 1999). Like their historic counterparts, then, AIDS NGOs in Brazil substantially increased their popularity and influence and consequently became attractive to national AIDS officials seeking to harness their popularity, expertise, and influence for the centralized expansion of the national AIDS program (Camara 2002; Gómez 2011).
The ideas guiding Brazil's AIDS NGOs comported nicely with the Liga, Sifilógrafo, and sanitarista social movement. That is, AIDS NGOs desired a strong national AIDS program that could easily intervene at the local level, providing them and municipal health departments with the resources needed to increase awareness and prevention, especially for sex education (Teixeira 1997; Gómez 2011). In addition to funding prevention and ARV treatment, the AIDS program also helped NGOs combat discrimination and hatred (Teixeira 1997; Parker 2003). NGOs also believed that the program should work with them in attending international meetings and conferences (Bastos 1999; Rich 2009). And finally, AIDS NGOs preferred the presence of a strong centralized AIDS bureaucracy capable of effectively implementing policy (Parker 2003; Teixeira 1997; Gómez 2011).
In addition to providing similar ideas and interests, the sheer size of AIDS NGOs increased significantly throughout the 1990s (Villela 1999; Camara 2002). Villela (1999) states that within a year or two after the World Bank loan in 1994, at the sixth annual national AIDS NGO conference (VI Encontro Nacional de ONGs/AIDS), more than four hundred civic organizations signed up to work with AIDS NGOs (Villela 1999: 195). With the realization that AIDS NGOs were now supported by the World Bank, there emerged a sudden spurt of NGO activity that continued to expand and provide new employment opportunities for anyone working on AIDS (Massé 2009). At the same time, NGOs had incentives to strengthen their partnership with previously marginalized reformers in the AIDS program working with the World Bank (Massé 2009; Gómez 2011).
In sum, closely aligned with the international community and growing in popularity and influence, reformers in the national AIDS program now had an ample amount of NGO and social movement partnerships that they could harness to justify their continued centralized bureaucratic and policy pursuits. Not only could they continue to draw from the sanitarista movement, but they also had a multitude of AIDS NGOs that they could work with and that shared along with the sanitaristas and AIDS reformers deeply entrenched historical ideas of state intervention and partnerships in response to epidemics.
In addition, reformers’ knowledge of the successful partnerships that emerged between the Liga and Sifilógrafo movement and the state during the early-20th century motivated them to seek out these partnerships (Teixeira 2007; Gómez 2008). For example, in an interview with the former director of the national AIDS program (2002–03), Paulo Teixeira, he explained how working on the AIDS situation often reminded him of the historic Liga movements and the strong historic partnership that public health reformers had with social movements (Teixeira 2007). Other officials working in the AIDS program at the time confirm Teixeira's statement, noting how bureaucratic reformers’ knowledge of these historic pacts motivated them to create a strong partnership with the sanitaristas and AIDS NGOs (Barreira 2009).
AIDS NGOs also helped to periodically remind reformers about the success of these historic partnerships and the rich history of working together through common ideals and interests in a centralized bureaucratic and policy response (Terto 2008; Teixeira 2007; Gómez 2008). This knowledge motivated reformers to resuscitate these historic partnerships (Terto 2008; Teixeira 2007; Gómez 2008). It was believed that doing so would add to their credibility and influence within government (Barbosa 2008; Teixeira 2007).
And finally, it is important to note the importance and significance of the ideas that reformers were working with. As discussed earlier, in contrast to the policy ideas of decentralization as a strategy for responding to AIDS, the ideas AIDS officials shared with the sanitarista and AIDS NGO community were much older, firmly entrenched in traditions that began with the Liga and Sifilógrafo movement (Gómez 2008). Ideational beliefs in decentralization declined while rich historical ideational precedents in centralization and contemporary reformers’ interest in pursuing them gave AIDS officials advocating these ideas greater credibility and influence (Gómez 2008, 2011).
NGO and Social Movement Partnerships and its Centralization Consequences
By using these historically-weighty ideas and coalitions, AIDS reform officials now had the legitimacy, credibility, and leverage needed to press for the continued expansion of the national AIDS bureaucracy and its policies (Barbosa 2008; Teixeira 2007; Gómez 2008, 2011). Sustaining a close partnership with AIDS NGOs and the sanitarista movement has been important for providing reformers with the legitimacy needed to continuously acquire funding from the congress (Barbosa 2008; Teixeira 2007; Gómez 2008, 2011). Since the mid-1990s, this has contributed to an increase in federal spending for the AIDS bureaucracy, such as hiring more administrative staff and consultants, as well as funding for its universal prevention and ARV treatment policies (Gómez 2010). In a climate where international health organizations and donors, such as the WHO and the World Bank, respectively, advocate for the incorporation of civil society into the policy-making process, reformers’ renewed partnership with civil society further strengthened their ability to secure funding (Gómez 2011). As Figure 2 illustrates, not only has congressional spending increased, but it has far surpassed the amount of money given to the AIDS program from the World Bank (Gómez 2011). Figure 2 also shows that spending increased even after the 1998 financial crisis.
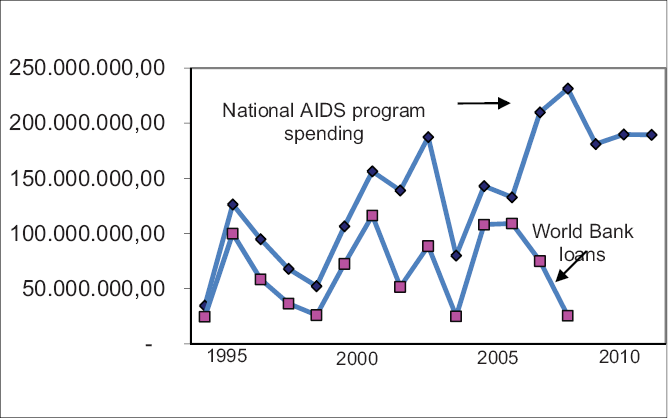
Brazil National AIDS Program Spending vs. World Bank Loans (in million BRL)
Continued support for reformers’ efforts to strengthen the national AIDS program has also lead to new initiatives that maintain a centralized presence even after decentralization has occurred (Barboza 2006; Pires 2006). Notwithstanding the MOH's decision to gradually devolve greater financial responsibilities to the municipalities for AIDS policies in 2001, AIDS officials obtained congressional and MOH support for creating a new program that supplements decentralization by providing discretionary funding to those municipalities in need of financial assistance (Brazil, Ministry of Health 2010; Barboza 2006; Pires 2006). Titled the Fundo-a-Fundo Incentivos program, as long as municipal health agencies adhere to conditionalities imposed by the AIDS program, such as transparency in funding disbursements, commitment to prevention and treatment policy implementation, financial assistance continues (Brazil, Ministry of Health 2010; Barboza 2006). By threatening to reduce funding if municipalities do not comply with these measures, this conditionality helps the national AIDS program maintain its influence while incentivizing municipal governments to more effectively implement policy (Pires 2006; Barbosa 2006). This also suggests that AIDS officials are still questioning the efficacy of decentralization processes, given its fast-pace timing and the managerial and fiscal inefficiencies it has created (Silveira 2007; Couttolenc, la Forgia, and Matsuda 2007). As Figure 3 illustrates, since its creation in 2002, funding from the Fundo-a-Fundo program continues to increase.
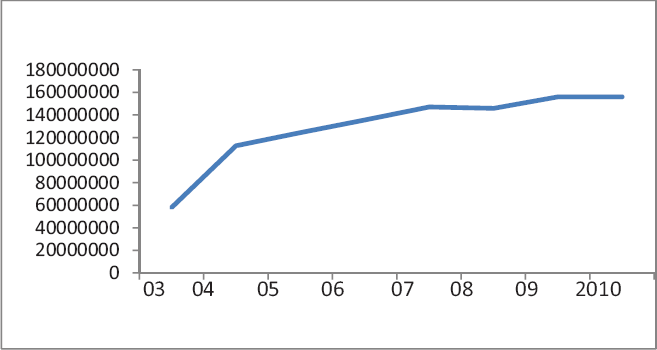
Spending for the Fundo-a-Fundo Incentivos Program (BRL)
Conclusion
When constrained by constitutional commitments to healthcare devolution, reinforced with social expectations and notions of human rights, progressive national AIDS bureaucracies can, as the case of Brazil illustrates, introduce innovative centralization strategies that help ensure effective sub-national policy implementation. This is achieved through the delegation of policy-making autonomy, the creation of federal regulatory institutions, ongoing congressional funding for human resources and universal policy, as well as the creation of conditional fiscal policies incentivizing municipal governments to comply with national bureaucratic mandates. While centralization may be needed in a context of ineffective devolutionary processes, a key lesson that emerges from this study is that centralization by no means suggests a reversal of constitutional commitments to devolution; rather, it strengthens this process by providing much needed financial and technical assistance to municipalities while incentivizing municipal health officials to effectively implement policy.
This study has also shown that sustainable government responses to AIDS may require innovative federal interventions after national bureaucratic and policy responses have occurred. For example, while many nations pursued prevention and treatment policies shortly after AIDS’ emergence, few subsequently created new universal treatment policies as well as conditional fiscal transfer programs designed explicitly for AIDS. As we saw in Brazil, these innovations can help sustain and strengthen national and especially sub-national capacity and commitment to policy implementation. Future studies will need to examine the types of policies that those nations challenged by healthcare devolutionary processes subsequently introduce in order to strengthen their AIDS programs. Such an analysis can also reveal the extent to which national governments are committed to exploring new ways of enhancing their policy response.
Another lesson that emerges from this study is that while international criticisms, pressures, and reputation-building may be important catalysts for reform, contrary to the scholarly literature (Lieberman 2009; Oluonzi and Macrae 1995), Brazil shows that innovative centralization responses to AIDS are not the direct product of these processes. Instead, centralization is the product of domestic AIDS officials seeking to build a strong partnership with like-minded AIDS NGOs and social movements possessing similar historically-based ideas and a rich history of state-societal partnerships in favor of centralized responses to epidemics. This in turns suggests that national bureaucratic capacity arises not from AIDS officials’ technocratic and financial resources, but from their access to NGOs and social movements that they can forge strong partnerships with. When compared to other nations, however, considering how long these centrist ideas and partnerships have existed in Brazil, the latter may be unique in this regard. Future research will need to explore if other nations have similar types of enduring partnerships with NGOs and social movements and to what extent this can help national AIDS officials pursue centralization amidst healthcare devolution. Among those nations most similar to Brazil, such as India, China, and Russia, recent research nevertheless shows that this is not the case (Huang 2006; Lieberman 2009; Gómez 2009b) and that consequently, Brazil may indeed be unique in possessing these close partnerships with AIDS NGOs and social movements.
Theoretically, another lesson that emerges from this study is the role of change actors in gradual institutional change processes. Similar to the recent work on this topic by James Mahoney and Kathleen Thelen (2010), this article has argued that the institutional and political environment shapes the types of change actors that will emerge. Among the four different types of change actors described by Mahoney and Thelen (2010), those individuals that were hired by national AIDS officials from AIDS NGOs and state AIDS programs, many of whom were also members of the sanitarista movement, closely resembled subversive change actors. Responding to new opportunity spaces provided through their hiring into the national AIDS program beginning in the early-1990s, these individuals gradually infiltrated and helped strengthen the program. They did this by increasing the number of individuals within the program committed to a centralized bureaucratic and policy response, while helping formulate centrist policies based on extensive experiences obtained at the state level. Moreover, they also aided the AIDS program by bring within them pre-existing partnerships with AIDS NGOs and the sanitarista community, thus facilitating the program's subsequent usage of these partnerships in order to increase its legitimacy and influence when seeking a centralized response.
What the findings in this article suggests, however, is that more work needs to go into better understanding the historic weight of ideas and coalitional traditions that further embolden subversive actors and their ability to gradually pursue reform. While subversives may quietly establish coalitions among ideological/ political contemporaries (Lieberman 2002; Berman 2001), at times, this may not be sufficient for gradual institutional change to occur. Instead, they need to establish coalitions that are grounded in centralization ideas and partnerships with civil society that have a long history, fame and, thus, legitimacy. In so doing, subversives have a better chance of achieving their desired outcome.
Going forward, researchers and policy makers interested in better understanding institutional change processes may wish to consider studying health epidemics. This is a new area of comparative research that is not only in need of greater insights from social science, but one that can also provide new insights for those interested in studying alternative paths to the reform of the state.