
Abstract
Purpose:
The study aimed to evaluate the risk and contributing factors leading to compensation claims and permanent disability following complications of treatment in the management of paediatric forearm fractures.
Methods:
Data were gathered from the Finnish Patient Insurance Centre (PIC), which reviews all claims regarding potential treatment complications in Finland. PIC grants monetary compensation based on excess pain or permanent cosmetic and/or functional disability. We evaluated all claims concerning paediatric forearm fracture management in children under 16 years of age between 1990 and 2019.
Results:
One hundred and forty-four (58 distal forearm, 55 forearm shaft and 31 proximal forearm) of 226 claims were compensated for a total of 156 separate treatment complications. The overall calculated risk for sustaining a compensated treatment complication was 0.1%. Unsatisfactory standard of surgery was the reason for the compensation in 29/55 children with forearm shaft fractures and delayed diagnosis in 20/31 children with proximal forearm fractures, respectively. Compensation was granted for permanent functional disability to 35 children and for permanent cosmetic disability to 62 children. Permanent functional disability was compensated in 6/58 children with distal, 19/55 with shaft and 10/31 with proximal forearm fractures.
Conclusions:
The risk of sustaining a compensated complication of treatment after a paediatric forearm fracture is low. Forearm shaft and proximal forearm fractures are associated with a clearly higher risk of iatrogenic injuries with permanent disability than distal forearm fractures.
Study Significance:
This paper is significant due to the lack of previous publications on this topic and can contribute to minimizing treatment complications in the future.
Keywords
Introduction
The forearm is the most common fracture location in the paediatric population, with an estimated incidence of 650 per 100,000.1,2 Distal forearm fractures account for approximately 70% of all cases, shaft fractures for 20%, and proximal forearm fractures for 10%.1–4 Most distal forearm fractures are incomplete distal metaphyseal torus injuries, which heal uneventfully.5,6 Half of forearm shaft fractures are both bone fractures.7–9 Preferred treatment of forearm shaft fracture is debated, but surgical treatment has increased, and flexible intramedullary nailing is the most commonly used surgical intervention.7,9–12 The risk of nerve injury as a complication of internal fixation of a forearm fracture is 1.3%. 4 Monteggia and Galeazzi fractures are rare fractures in the paediatric population (incidence 2.9 per 100,000), which is one reason why they pose diagnostic challenges.13,14 A missed forearm fracture, especially Monteggia, during growth may lead to substantial disability later in life. 15
The Patient Insurance Centre (PIC) evaluates all claims regarding potential complications of treatment in Finland and grants monetary compensation based on temporary discomfort, permanent cosmetic disability and permanent functional disability. 16 Functional disability is evaluated based on incapacity classes 1–20, with each class representing a 5% disability. 16 Permanent functional disability is evaluated when the medical adviser, working at PIC, deems it reasonable to assume the results as permanent. The claim ought to be at PIC’s disposal within 3 years from the time when the patient should have been aware of the treatment complication. 16 If dissatisfied with PIC’s decision, a request for re-evaluation by the Traffic and Patient Accident Board can be made. 16
This study aimed to evaluate the risk and contributing factors associated with developing permanent disability following compensated complications of treatment in forearm fractures. Given that most paediatric forearm fractures heal uneventfully, it was hypothesized that the overall risk of permanent functional disability is low.
Methods
Study design
This is a retrospective registry-based study.
Data sources and participants
All claims submitted to PIC between 1990 and 2019 concerning forearm fractures in children under 16 years of age were evaluated. Claims were identified using the International Statistical Classification of Diseases (ICD) diagnosis codes 813 and 818 (ICD-9) and S52 (ICD-10). 17 Relevant procedural codes, including procedures on forearm bones and removal of implants or external fixation devices, were 912, 913, 916, NCJ, NCK, and NCU. All subgroups were included. The data collected included patient age at the time of injury, place and method of treatment, speciality of treating professional, grounds for compensation and any client complaints regarding PIC’s decision to the Traffic and Patient Accident Board. Population data for children under 16 years of age during the study period (mean 985,029; range 931,508–1,036,791; standard deviation (SD) 35,045) were obtained from a national register. 18
PIC’s decisions were independently re-evaluated based on written claims by an observer and a PIC medical adviser, both blinded to the original decisions and holding level 5 expertise in paediatric upper limb trauma. 19 STROBE guidelines were followed.
Outcome
The outcomes were any treatment complications and underlying cause(s).
Statistics
Descriptive statistics were used to summarize the data. Categorical variables were reported as frequencies and percentages. Continuous variables were presented as means with standard deviations (SD) and ranges. Incidence rates were calculated by dividing the number of compensated claims by the national population of children under 16 years of age during the study period, expressed per 1,000,000 children. The risk of a compensated complication of treatment was calculated as the proportion of compensated claims relative to the estimated total number of paediatric forearm fractures.
Results
Between 1990 and 2019, PIC received 226 claims for complications of the treatment of paediatric forearm fractures (Figure 1). Of these, 144 (64%) were granted compensation, giving an annual incidence of a compensated complication of treatment at 5.0 per 1,000,000 (range 0–14.7, SD 4.1), with a peak incidence in 2015 and 2016 (Figure 2). The number of claims submitted increased throughout the study period (Figure 3). The overall calculated risk of a compensated treatment complication after a forearm fracture was 0.1%. The incidence peaked in males at 15 years, and at 13 in females (Figure 4). Among all the compensated cases, 62% (89/144) were male, with the left arm (including 3 bilateral) affected in 63% (90/144). None of the compensated fractures were open fractures. Altogether, 156 treatment faults were found in the 144 claims. The most common reasons for compensation were inappropriate closed treatment (38%, 59/156) and unsatisfactory standard of surgery (37%, 58/156). Most treatment complications arose from regional or district hospitals (53%, 83/156), with orthopaedic surgeons accountable for the majority (26%, 41/156) (Table 1).
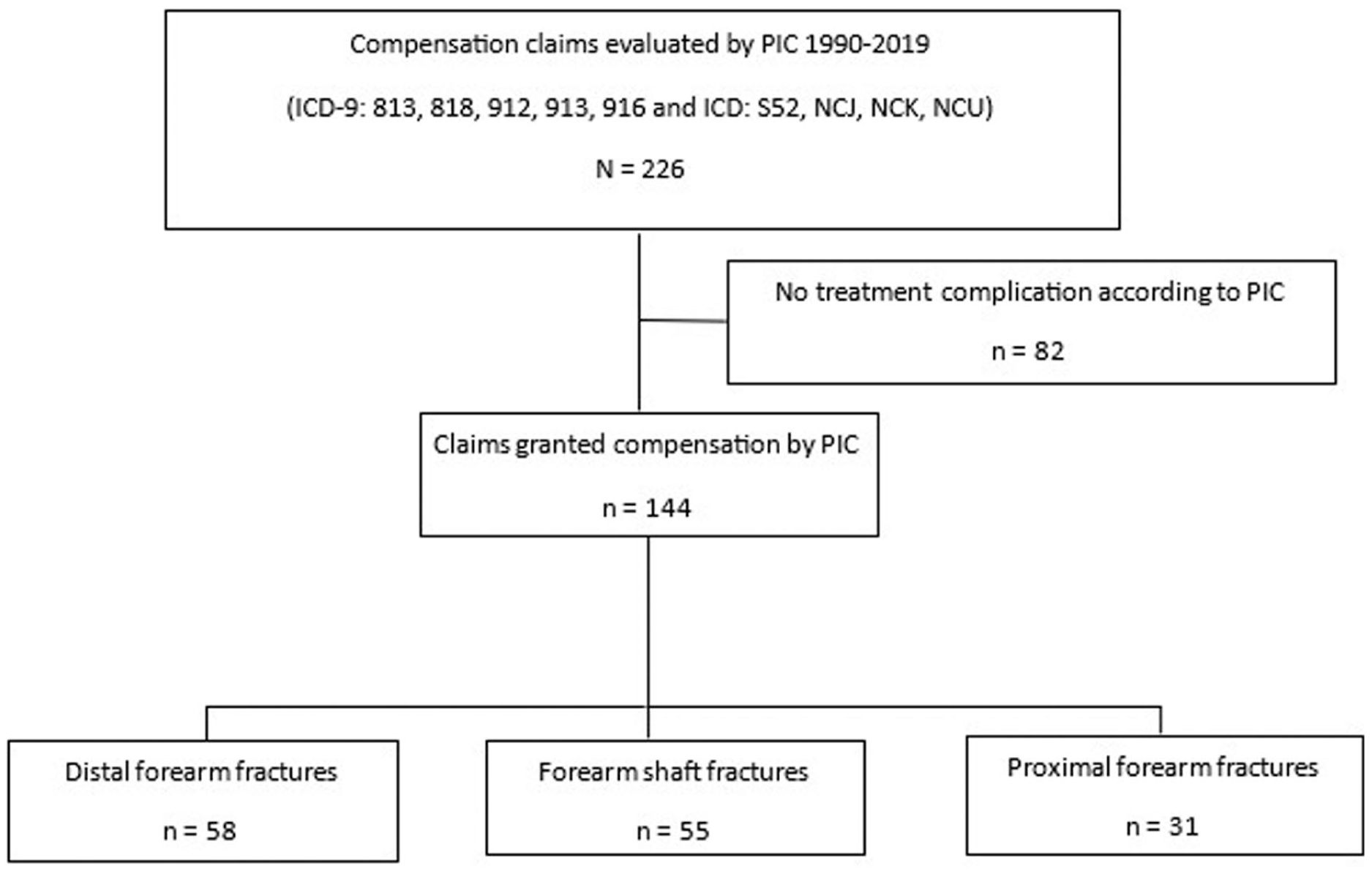
Participant flow as a figure.
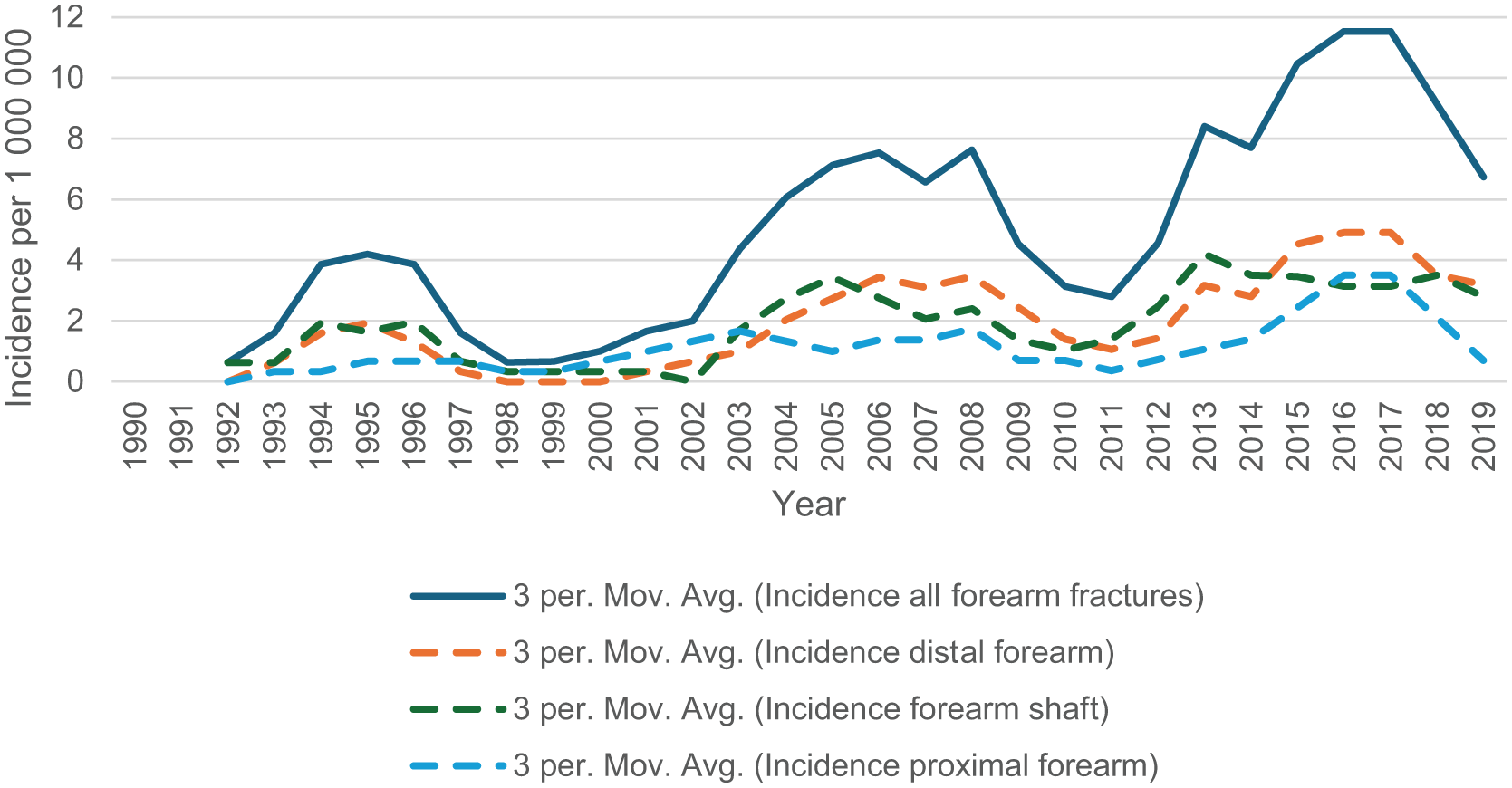
Incidence of compensated complications of treatment in paediatric forearm fractures in Finland (1990-2019).
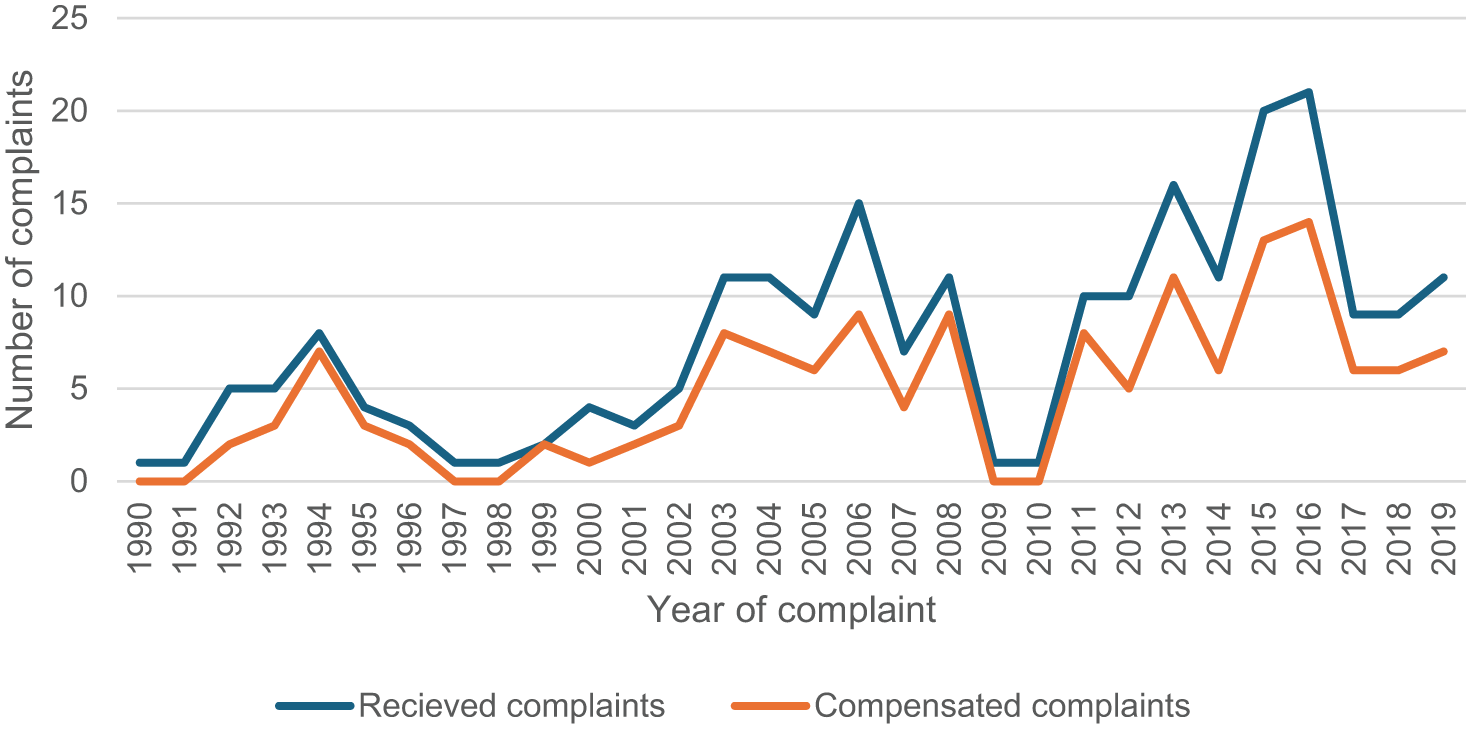
Annual number of peadiatric forearm fracture-related complaints submitted to and compensated by the Finnish Patient Insurance Centre (1990-2019).
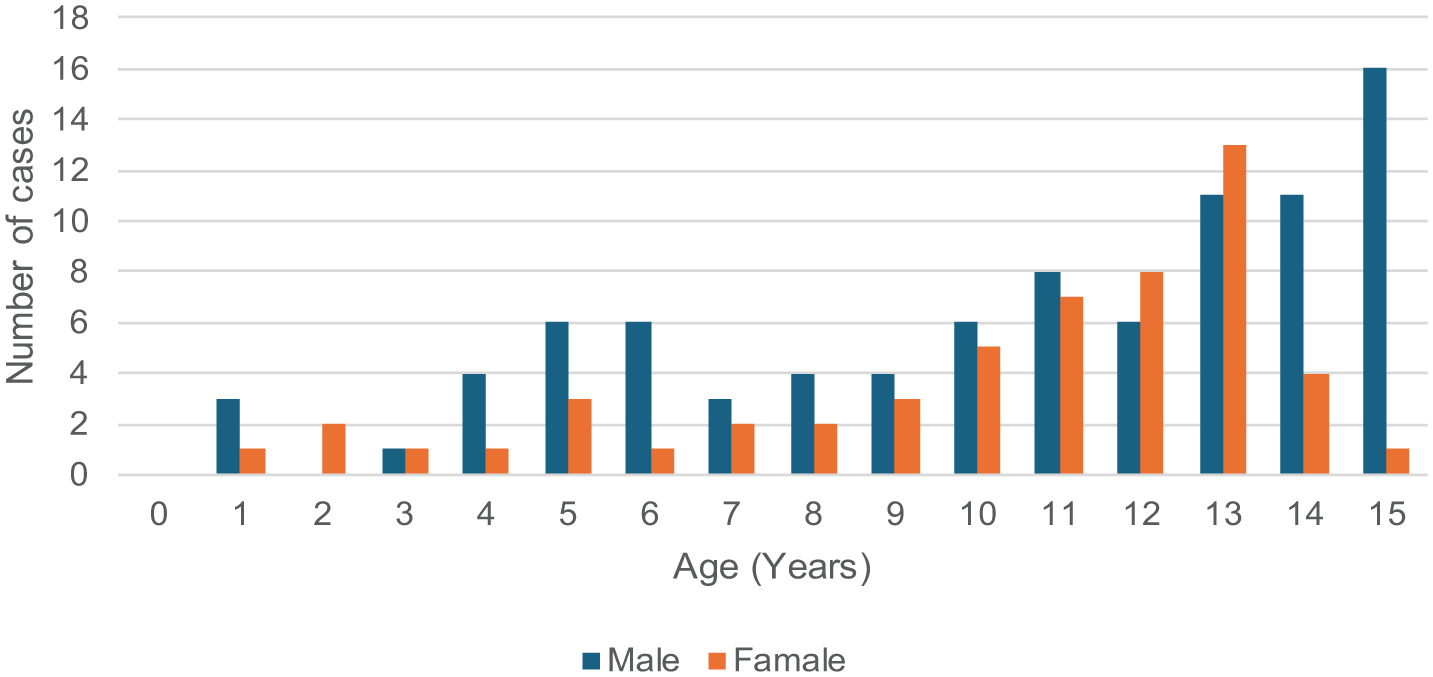
Age and sex distribution of children granted compensation for a complication of treatment after a forearm fracture in Finland (1990-2019).
Reason for compensation by treating profession in compensated complications of treatment in paediatric forearm fractures in Finland (1990–2019).
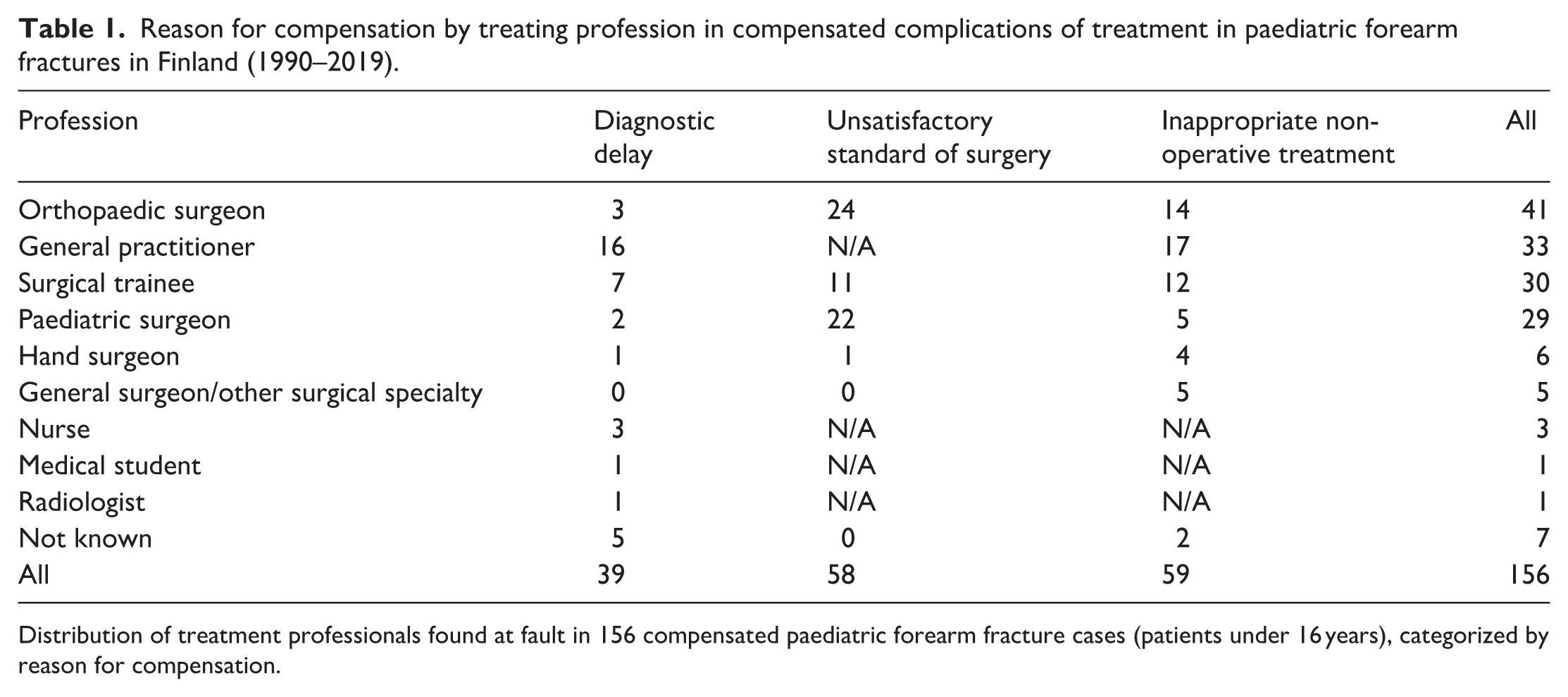
Distribution of treatment professionals found at fault in 156 compensated paediatric forearm fracture cases (patients under 16 years), categorized by reason for compensation.
Distal forearm
Of the 122 claims for distal forearm fractures, 58 were compensated, for a total of 63 treatment complications (three claims were compensated for 2 separate complications, and 1 for three). The annual incidence of compensated complications of treatment following distal forearm fractures was 2.0 per 1,000,000 children (range 0–6.3, SD 2.0), giving an annual risk of 0.04%. The mean age at fracture was 11.1 years (range 1–15, SD 3.5), with boys accounting for 33 cases and the left extremity involved in 34 cases.
Compensation was granted for inappropriate closed treatment in 31 cases. Seventeen were compensated for unsatisfactory surgical standards; inadequate fixation (n = 7), unnecessary anaesthesia (n = 3), inappropriate hardware removal (n = 3), nerve injury (n = 2) and unnecessary surgical procedure (n = 2). In 15 cases, the reason for compensation was a delay in diagnosis: lack of radiographic imaging (n = 13) and failure to detect the fracture (n = 2). Most of the compensated complications of treatment occurred in regional or district hospitals (n = 29) and healthcare centres (n = 19). Eight complications were associated with private clinics and seven with university hospitals (Figure 5). General practitioners (n = 18), surgical trainees (n = 14) and orthopaedic surgeons (n = 10) were the three most common professionals found at fault. Compensation was granted for permanent functional disabilities in 6 cases and for permanent cosmetic disabilities in 19. (Table 2) Three children, who were granted compensation for a permanent functional disability, displayed reduced range of motion (ROM) in the wrist, two displayed pain, one a sensory deficit, one numbness and one reduced strength. Four of the six fractures with permanent functional disability were both bone fractures, and two were radial fractures.
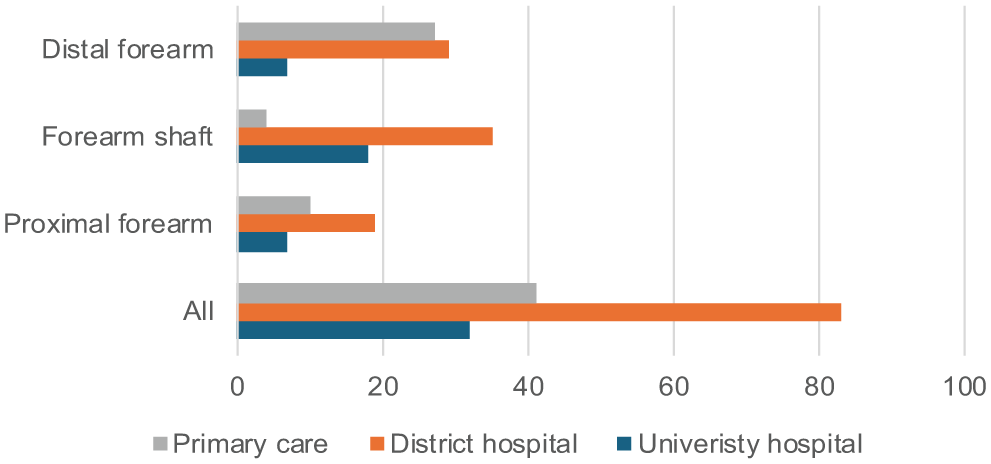
Type of treating unit by fracture location in compensated complications of treatment in paediatric forearm fractures (1990-2019).
Permanent disabilities following compensated complication of treatment in forearm fracture in children (1990–2019).
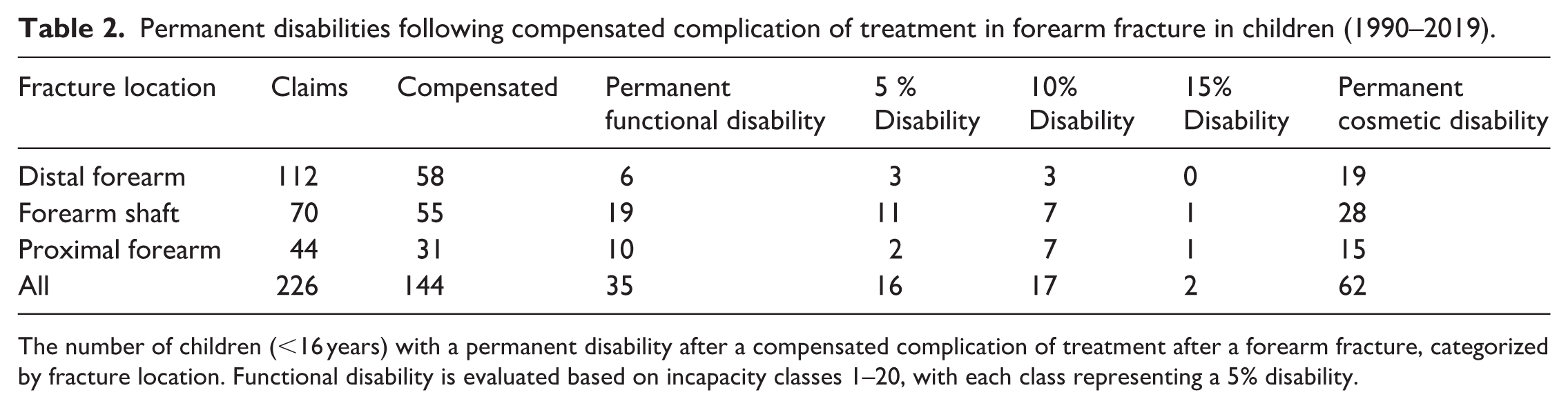
The number of children (<16 years) with a permanent disability after a compensated complication of treatment after a forearm fracture, categorized by fracture location. Functional disability is evaluated based on incapacity classes 1–20, with each class representing a 5% disability.
Forearm shaft
Fifty-five out of 70 reviewed forearm fracture claims received compensation for altogether 57 treatment complications – 2 claims included compensation for errors at 2 separate stages of care. The annual incidence of a forearm fracture-related compensated complication of treatment was 1.9 per 1,000,000 (range 0–5.2, SD 1.7), giving an annual risk of 0.1%. The mean age at injury was 10.7 years (range 1–15, SD 4.0), with male patients, and the left forearm each accounting for 36 cases (1 bilateral fracture). Forty-three fractures were both bone diaphyseal fractures, and 12 involved only the radius, including 2 Galezzi fractures.
In 29 cases, compensation was granted for unsatisfactory standard of surgery, due to inadequate fixation (n = 12), intraoperative tendon (n = 10) and nerve injuries (n = 6), premature hardware removal (n = 2), and 1 intraoperative burn injury. One claim documented three separate intraoperative faults – inadequate fixation, tendon injury and nerve injury. An additional 24 cases were compensated due to inappropriate closed treatment. Delayed diagnosis accounted for four compensated complications of treatment (lack of radiographs n = 2, failure to detect the fracture n = 2). The highest number of treatment complications arose in regional or district hospitals (n = 35), followed by university hospitals (n = 18) and healthcare centres (n = 4) (Figure 5). Orthopaedic surgeons were found at fault in 18 cases, paediatric surgeons and surgical trainees each in 13. Compensation was granted for permanent functional disability in 19 claims and for permanent cosmetic disability in 28 (Table 2). Fifteen children, compensated for a permanent functional disability, showed a reduction in ROM, six showed decreased grip strength, four pain and three impaired thumb extension.
Proximal forearm
Of the 44 claims regarding proximal forearm fractures, 31 were granted compensation for a complication of treatment in a total of 36 distinct events. In three claims, compensation was granted for two separate complications, and in one claim for three. The annual incidence of compensated treatment complication following a proximal forearm fracture was 1.1 per 1,000,000 (range 0–4.2, SD 1.2), giving an annual risk of 0.2%. The mean age at injury was 8.7 years (range 3–15, SD 3.6), with most patients male (n = 20), and the left arm affected in 18 cases.
Diagnostic delay accounted for 20 of the 31 claims: 19 failures to detect a fracture, and 1 failure to obtain a radiograph. In 12 claims, unsatisfactory surgical standards, primarily due to inadequate fixation (n = 9), premature hardware removal (n = 2) and an intraoperative nerve injury were found as reasons for compensation. Closed treatment was found inappropriate in four cases; three fulfilled the criteria for surgical fixation, and in one, a closed reduction was done inadequately.
Notably, 16 of 31 claims (52%) involved Monteggia fractures. Of the Monteggia fractures, 15 were initially missed on the radiographs, and 1 patient underwent unsatisfactory standard of surgery, and in addition subdued an intraoperative motor radial nerve injury. Among the 15 missed Monteggia fractures, four received additional compensation for an unsatisfactory surgical standard, with one undergoing two substandard surgical procedures at two separate surgeries.
Most complications occurred in regional or district hospitals (19/36), followed by healthcare centres (n = 8), university hospitals (n = 7) and the private sector (n = 2) (Figure 5). The three most common treating professionals at fault were as follows: orthopaedic surgeons (n = 13), general practitioners (n = 9) and paediatric surgeons (n = 7).
Ten patients (five Monteggia) received compensation for permanent functional disability. Fifteen (11 Monteggia) received compensation for permanent cosmetic disability (Table 2). The reason for granted permanent functional disability was decreased ROM in the elbow in nine cases, of which two also showed elbow instability. In one case, the functional disability was based on insatiability and pain.
PIC decision and expert opinion
Of the 226 PIC medical advisers reviewing the claims, 108 were paediatric orthopaedic surgeons (48%), followed by orthopaedic surgeons (n = 59), hand surgeons (n = 37), general practitioner (n = 13), internists (n = 2), a paediatric surgeon, a specialist in public health, as well as 5 unknown. The claimant requested a revision by the Traffic and Patient Accident Board in 15 cases (6 primary granted compensation by PIC, and 9 declined). In two cases, both originally declined by PIC, the Traffic and Patient Accident Board found the PIC decision wrongful and granted compensation (one distal radius fracture, where the PIC medical adviser was a paediatric orthopaedic surgeon, and one forearm shaft fracture, where the PIC medical adviser was a hand surgeon).
The medical experts disagreed with PIC’s medical advisers’ decision at re-evaluation in 21 of 226 cases. The experts evaluated that compensation was wrongfully granted in 11 claims and wrongfully denied in 10 claims. In one of these cases, a revision was made by the Traffic and Patient Accident Board, in which the experts agreed with the Board, and in one additional case, the experts agreed with the medical adviser at PIC, but disagreed with the revision made by the Board.
Discussion
This nationwide, 30-year retrospective study found that the overall risk of a compensated complication of treatment after a paediatric forearm fracture was 0.1%. However, when such complications occurred, forearm shaft and proximal forearm fractures were associated with a notably high rate (approximately 30%) of permanent functional disability.
The compensation rate for claims related to paediatric forearm fractures is consistent with previous Finnish studies on treatment complications in paediatric fracture care.20–22 The increasing number of claims observed during the study period likely reflects both improved awareness among families about the possibility of seeking compensation for suspected complications of treatment and a general rise in the number of paediatric orthopaedic procedures. 23 This upward trend is also seen across all claims submitted to PIC. 16
The incidence of compensated treatment complications peaked at an older age in males than in females, a pattern also noted in distal forearm fractures (males: 11–13 years; females: 9–11 years) and paediatric fractures more broadly (males: 14 years; females: 10 years).1,24 Both bone fractures were notably overrepresented among treatment complications (78%) compared to their overall proportion among shaft fractures (50%).7–9 The risk of sustaining a compensated complication of treatment after a forearm fracture was lower than for other paediatric fractures, such as tibial (0.4%), distal humeral (1.1%) and femoral fractures (2.2%), but similar to that seen in paediatric hand fractures (0.1%).20–22,25 This may be explained by the high frequency and generally benign healing of distal forearm and finger fractures, which are the most common fracture types in children.1,2,5,6,26–28
Distal forearm fractures were underrepresented among compensated complications of treatment (40%) compared to their overall incidence in paediatric forearm fractures (approximately 70%). 6 This likely reflects their generally benign nature and the fact that many can be managed conservatively without follow-up. By contrast, forearm shaft and proximal forearm fractures were overrepresented (20% vs. 40% and 10% vs. 20%, respectively). Treatment guidelines for forearm shaft fractures remain poorly defined, despite the increasing use of surgical methods such as flexible intramedullary nailing.7,9,11
Notably, the risk of permanent functional disability was lowest in distal fractures and highest in shaft and proximal fractures (Table 2, Figure 6), underscoring the need for accurate diagnosis and appropriate management in more complex injury locations. Permanent functional disability after a compensated complication of treatment was three times more common in shaft and proximal fractures than in distal ones, likely due to better remodelling potential in the distal forearm. 29 Furthermore, the overall risk of permanent disability after a compensated complication of treatment in forearm fractures (24%) was higher than that reported for paediatric distal humeral fractures (17%). 22
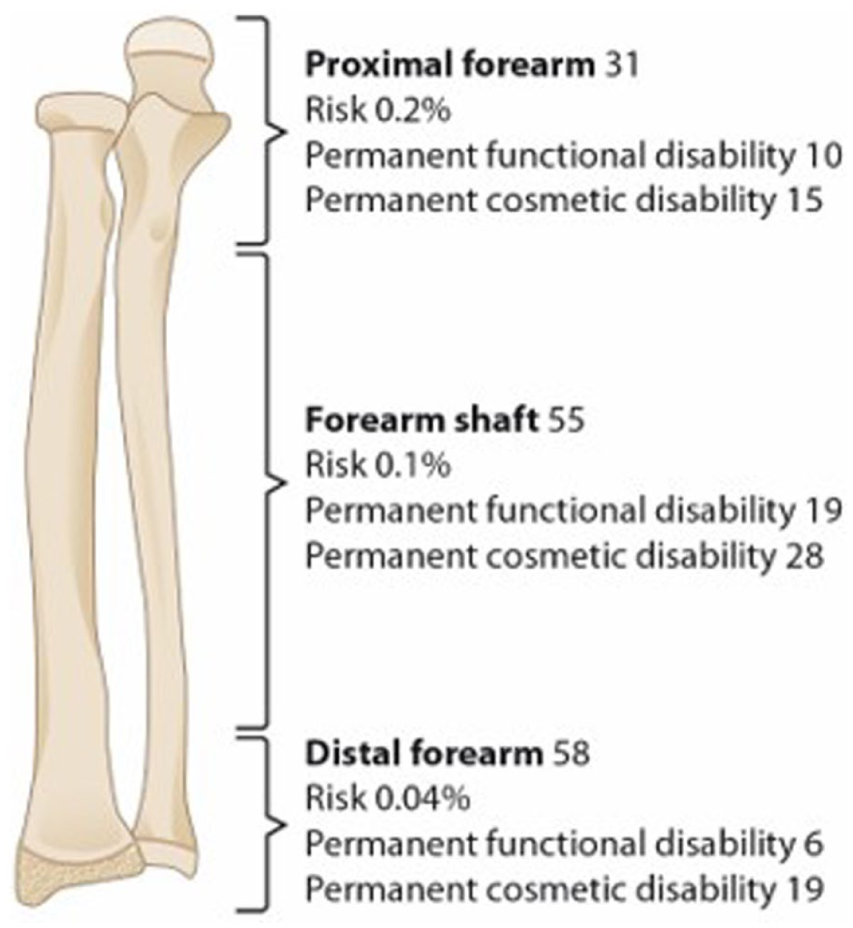
Risk and permanent disability by fracture location in compensated complications of treatment in paediatric forearm fractures (1990–2019).
Monteggia fractures accounted for over half of all compensated complications of treatment in proximal forearm fractures and 11% of treatment complications overall – despite representing only 0.5% of paediatric forearm fractures.13,14 This marked overrepresentation highlights their diagnostic complexity and the potential consequences of missed radiocapitellar malalignment. These findings support routine and systematic assessment of radiocapitellar alignment on all paediatric forearm and elbow radiographs, particularly in younger children. Furthermore, careful consideration of fracture stability and timely referral or consultation in complex shaft or proximal fractures may reduce technical complications. Treatment in higher-volume or university hospitals may reduce the likelihood of treatment complications. Although most complications arose in regional or district hospitals, this likely reflects case volume distribution; however, the lower proportion observed in university hospitals suggests that concentrated expertise and structured supervision may contribute to safer care. Additionally, the medical experts retrospectively agreed with PIC’s decision in 91% of the cases – comparable to the 87% agreement rate documented in a previous study on distal humeral fractures. 22
Strengths and limitations
This study is strengthened by its nationwide scope, inclusion of all paediatric forearm fracture-related claims over a 30-year period, and its focus on patient-centred outcomes such as permanent functional and cosmetic disability. An independent expert review of claims supports the validity of the findings. However, limitations include its retrospective design and reliance on claim documentation rather than original medical records, which limited clinical detail. Not all patients with complications of treatment may have filed claims, likely leading to an underestimation of the true incidence. Variability in medical practice and compensation criteria over three decades may also affect consistency. Finally, the findings are most applicable to countries with similar healthcare and insurance systems and may not fully generalize elsewhere.
Conclusion
In conclusion, the rate of compensated complications of treatment in paediatric forearm fractures is low, particularly for distal forearm fractures and when care is provided at university hospitals. The risk of permanent functional disability is primarily associated with substandard surgical technique in forearm shaft fractures and delayed or missed diagnoses in proximal forearm fractures. These findings highlight the importance of systematic radiographic assessment of the elbow to avoid missed Monteggia fractures and underscore the need for adequate surgical training, supervision, and experience when treating paediatric forearm shaft fractures. Improved recognition of complex injury patterns and adherence to sound surgical principles may reduce avoidable harm.
Supplemental Material
sj-pdf-1-cho-10.1177_18632521261438638 – Supplemental material for Complications of treatment in paediatric forearm fractures: A 30-year review of compensation claims
Supplemental material, sj-pdf-1-cho-10.1177_18632521261438638 for Complications of treatment in paediatric forearm fractures: A 30-year review of compensation claims by Caroline Dikert, Yrjänä Nietosvaara and Petra Grahn in Journal of Children's Orthopaedics
Footnotes
Author contributions
Y.N. designed the study, served as a medical expert and revised the paper. P.G. served as a medical expert and contributed to writing the paper. C.D. collected and analysed the data and served as the primary writer.
Data availability statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.*
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship and/or publication of this article: Y.N. reports a conflict of interest by serving as a medical adviser at PIC.
Funding
The authors disclosed receipt of the following financial support for the research, authorship and/or publication of this article: C.D. received funding from Vappu Uuspään Säätiö for this study.
Ethical statement
Study approval was obtained from the Finnish Patients Insurance Centre. No approval from the ethical board committee was obtained since this was a register-based study.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.