
Abstract
Background:
Medial epicondyle fractures account for 11%–20% of pediatric elbow fractures. While nonoperative treatment is effective, surgery is often recommended for overhead athletes to enhance union rates, valgus stability, and expedited return to sporting activities. Postoperative recovery protocols vary, with traditionally up to 2 weeks of strict immobilization and rehabilitation lasting 6–12 months. This study evaluates the early range of motion (ROM) and accelerated rehabilitation in high-performing youth athletes undergoing surgical fixation.
Methods:
A retrospective review included patients aged 12–17 who underwent medial epicondyle fracture fixation (2015–2023). Those with concomitant injuries were excluded. Recovery was assessed by unrestricted Return to Sports (RTS).
Results:
18 patients (mean age 14) were included. Postoperatively, all wore a hinged elbow orthosis locked at 90° flexion. At 1 week, extension was allowed to −30°, with flexion as tolerated. Physical therapy was initiated, focusing on gentle stretching to full ROM out of the brace. Patients remained in a hinged elbow brace for an average of 4.47 weeks before transitioning to a hinged sleeve or discontinuing brace use. After 4–6 weeks, physical therapy increased with emphasis on strengthening and terminal extension. For the 16 baseball players included, progressive return to throw and hit programs began at an average of 8.6 weeks. All patients returned to sports without restriction at an average of 13.4 weeks.
Conclusion:
Early mobilization and accelerated rehabilitation following medial epicondyle fracture fixation facilitate a faster RTS in high-demand youth athletes.
Levels of Evidence IV:
Case series.
Introduction
Medial epicondyle fractures account for approximately 11%–20% of elbow fractures in patients aged 9–14 years.1–3 These fractures can occur due to various mechanisms, including direct trauma to the elbow, repetitive overhead throwing, or elbow dislocation. 2 In young throwing athletes, the medial epicondyle apophysis and the origin and insertion of the medial ulnar collateral ligament (MUCL) are at risk due to repetitive tensile forces seen across these structures. Medial epicondyle avulsion fractures occur at the MUCL origin. These injuries typically follow an acute-on-chronic pattern, such as after a single throw with a prodrome of elbow soreness. 4 Fractures with minimal displacement and no rotational component can successfully be managed nonoperatively in most patients. This traditionally consists of immobilization of the elbow in a long arm cast for up to 3–4 weeks. 5 However, nonoperative treatment of these injuries with prolonged immobilization may contribute to elbow stiffness 6 and worsening chronic valgus instability 7 in overhead throwing athletes. While most medial epicondyle fractures can be treated nonoperatively, surgical fixation is considered in cases with significant displacement, ulnar nerve entrapment, or in athletes who require a predictable and expedited return to high-demand sporting activities. The threshold for surgical intervention remains controversial, with studies suggesting displacement cutoffs between 3 and 5 mm, though measurement reproducibility is inconsistent.3,4,8 A relative indication for pursuing surgical intervention is in overhead athletes. 2 Due to repetitive microtrauma and excess forces seen across the elbow in these patients, medial elbow instability resulting from these injuries can be career-ending. Surgical fixation has shown lower complication rates and faster Return to Sports (RTS) compared to nonoperative management in this population.2,9
Postoperative immobilization protocols vary significantly, with differences in duration, method, and timing of range of motion (ROM) progression. Initial immobilization aims to minimize edema and protect the healing fracture, particularly in pediatric patients. However, excessive immobilization can lead to increased stiffness and delayed RTS. Studies recommend strict cast or splint immobilization for varying durations prior to switching to a hinged or soft elbow brace, which allows for motion across the elbow while still protecting against valgus forces. 3
RTS timelines also vary in the literature. Some postoperative protocols have patients cautiously RTS at 6–7 months,1,10 while more permissive protocols allow limited practices at 12 weeks. 8 These protocols discouraged returning to full pitching without restriction for 1 year postoperatively. This study describes a more rapid RTS protocol, with only short-term immobilization and rapid return to full sporting activity.
Methods
A retrospective chart review was conducted in patients who underwent open reduction internal fixation of medial epicondyle fractures from August 2015 to September 2023 in concordance with institutional review board approval (IRB #2023-1223). Patients 17-years-old and younger were included in the study. Patients were identified from the electronic medical record database by the International Statistical Classification of Diseases and Related Health Problems (ICD-10) for surgical repair of the medial epicondyle fracture. All active student athletes were included in the study regardless of sporting activity. Patients were excluded if they had concomitant injuries. Patients with developmental, neuromuscular, or autoimmune conditions were excluded.
All medial epicondyle fractures had identifiable displacement on radiographs. All patients underwent surgical repair, including a small incision, identification and protection of the ulnar nerve, reduction of the medial epicondyle fragment back to the humerus using the posterior cortex as a guide to anatomic reduction, and fixation using one or two 3.5 mm screws with washers to secure the fragment. The posterior periosteum was repaired, and the ulnar nerve was not transposed unless there was preexisting subluxation. All the patients included in this study had surgery performed by 1 of 2 attending surgeons.
Postoperative protocol for all patients began with 1 week of immobilization in a hinged elbow orthosis (HEO) locked at 90° of elbow flexion. At the 1-week postoperative visit, physical therapy was initiated, and HEO restrictions were loosened to promote early range ROM. Physical therapy focused on the gentle stretching of the elbow to full ROM out of the brace. Progression of brace tolerances typically followed the pattern of allowing −30° of extension with unrestricted flexion at 1-week postoperative, then allowing an additional 10° of extension per week. At the 4-week postoperative visit, the patient’s HEO was typically downsized to a less restrictive hinged elbow sleeve, or brace use was discontinued entirely. This decision was based on patients’ pain tolerance and progress with physical therapy. After 4–6 weeks, physical therapy was increased with emphasis on strengthening and regaining terminal extension. If pain was well controlled and increased ROM was tolerated at the 8-week postoperative evaluation, sport-specific rehabilitation programs were initiated, including progressive batting/throwing or light pitching programs. Pending a stable postoperative course, patients were typically cleared to return to pre-injury sporting activities without restriction after 12 weeks. Patients unable to clear progressive hitting/throwing or pitching programs were scheduled for additional follow-up visits to reevaluate progress, but no new restrictions were imposed. Additional rehabilitation was recommended for some pitchers, including hip and core strengthening programs for kinetic chain strengthening. Patients were also referred to a nutritionist to optimize their diet.
Postoperative visit notes were evaluated for complications and patient satisfaction. This included postoperative pain tolerance, participation in physical therapy, and participation in a sport-specific rehabilitation program. RTS was defined as full participation in practice and competition at the pre-injury level of play.
Patient data were de-identified in concordance with the institutional review board-approved protocol and stored on a secure password-protected Health Insurance Portability and Accountability Act compliant drive, Box Drive (Box, Redwood City, CA). Extrapolated de-identified data points were recorded on an Excel (Microsoft, Redmond, WA) spreadsheet. Statistical analysis was performed using Excel tools, including statistical max, min, mean, and standard deviation. AI tools were employed for editing, including Grammarly for Microsoft Office, ChatGPT, and Gemini, to assist in revising sections of this article, with the sole aim of improving clarity and readability. However, all AI-generated edits underwent thorough review, editing, and final verification by the authors.
Results
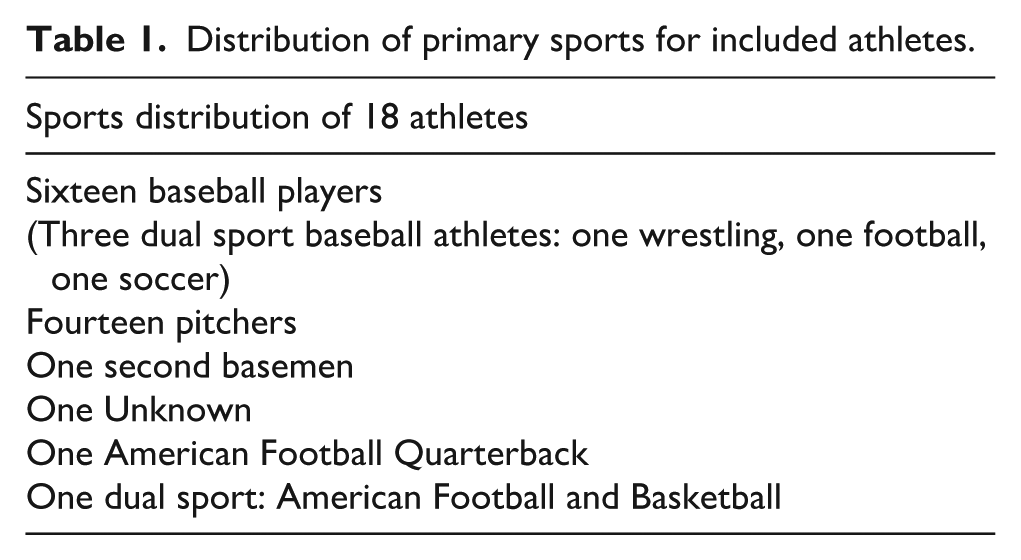
This study included 18 athletes. All patients were males aged 12–17 at the time of the surgery. The mean age was 14 years. 16 out of 18 (89%) patients included in the study were baseball players. Fourteen out of 16 (87.5%) baseball players were pitchers. Three baseball players were dual sport athletes. Two non-baseball athletes were included: one American football quarterback and one dual football/basketball athlete (Table 1).
Distribution of primary sports for included athletes.
Immediately following surgery, all patients were placed into a HEO locked in 90° of elbow flexion. All patients were evaluated at the 1-week postoperative appointment for pain, range of movement out of the brace, and evidence of healing on radiographic imaging. All patients reported that their pain was well controlled with multimodal pain management. Progressive loosening of the HEO tolerances was initiated, and the athlete’s tolerated ROM was used to determine starting recommendations for physical therapy. All patients began physical therapy after 1 week (Table 2).
Average time to recovery milestones.
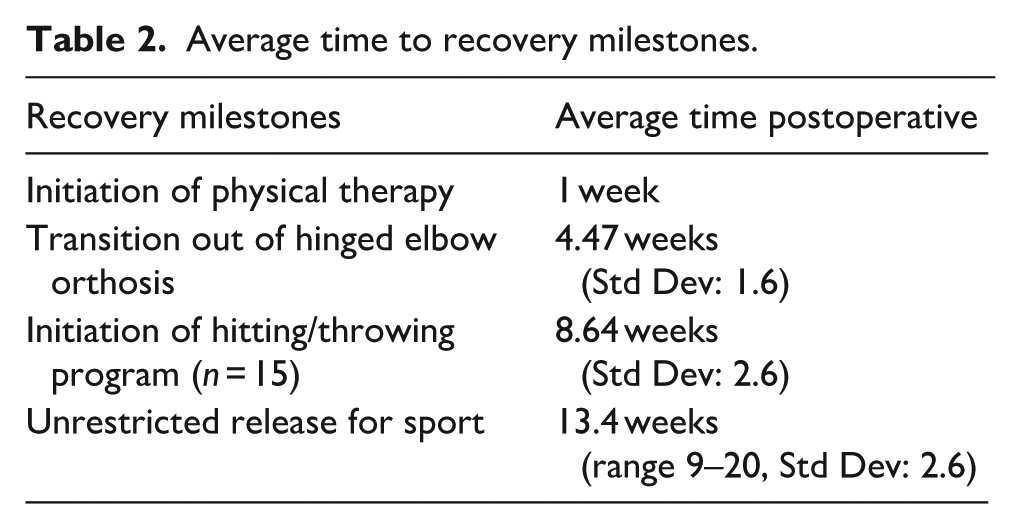
Patients remained in the HEO for an average of 4.47 weeks postoperatively. Most athletes transitioned from the HEO to a less restrictive hinged elbow sleeve before discontinuing all supportive brace use. Five patients in the study transitioned directly from the HEO to no brace. One patient demonstrated full pain-free ROM at his 1-week postoperative visit and was transitioned to a soft sling immediately. Two athletes discontinued all brace use after 4 weeks in the HEO, while two others chose to remain in the HEO for an additional 1–2 weeks before discontinuing bracing.
Figure 1 demonstrates the time spent in each recovery phase before unrestricted RTS by each patient. This includes time in HEO, time in downsized brace or no brace before initiation of progressive hitting/throwing program, and time in progressive hitting/throwing program before unrestricted RTS. The 16 baseball players included in this study started a progressive hitting/throwing program between 4 and 12 weeks postoperative at an average of 9 weeks (Figure 2). Two patients, the dual sport athlete and the American football quarterback, completed ROM and strengthening-focused rehabilitation programs before being released for RTS and therefore did not participate in a progressive hitting/throwing program. The athletes in this study were released for unrestricted RTS at an average of 13.4 weeks postoperatively. All patients successfully returned to their pre-injury sporting activity and level of play without complication. All patients reported satisfaction with the postoperative results and progress in their recovery at the time of release from clinic follow-up.
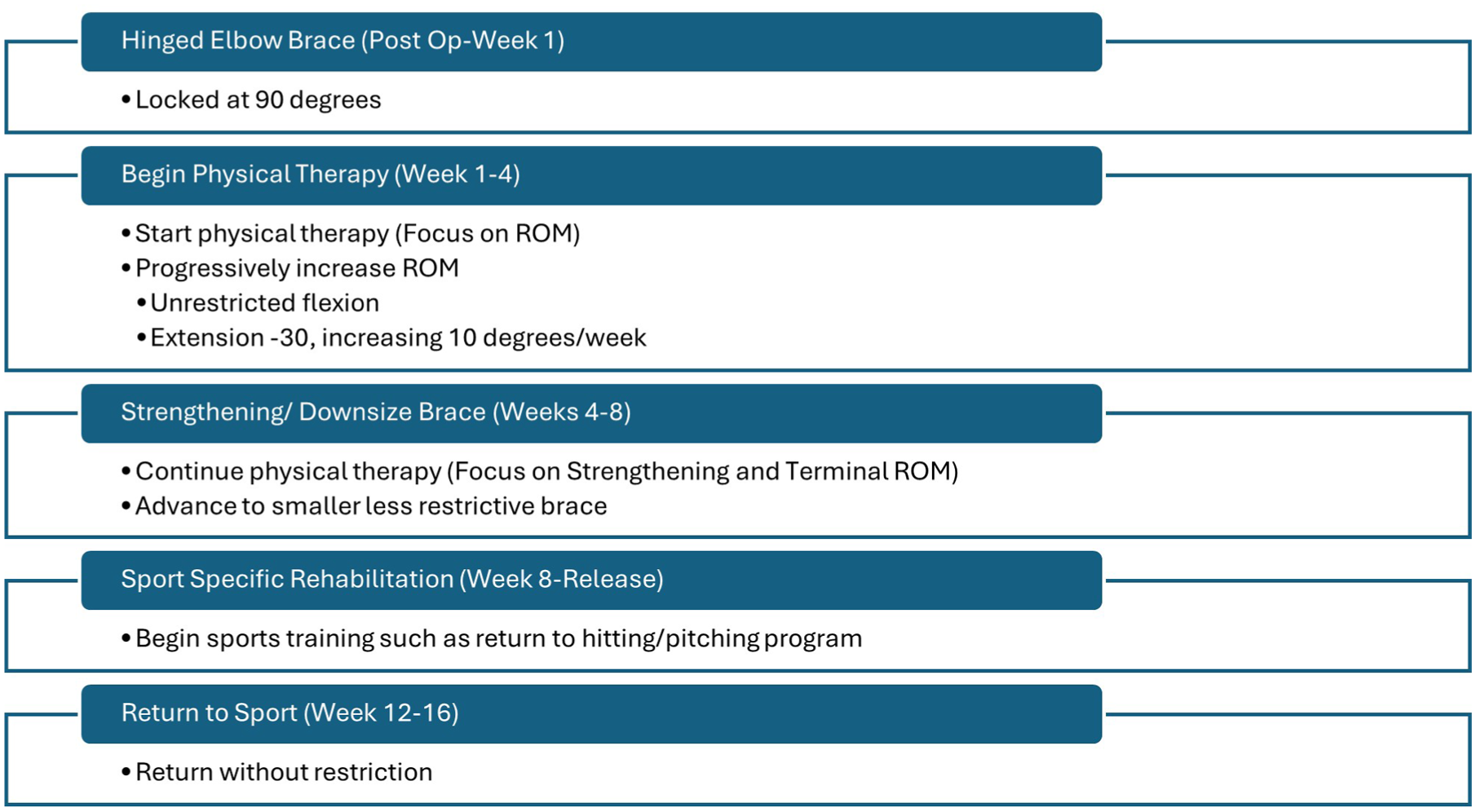
Postoperative recovery protocol.
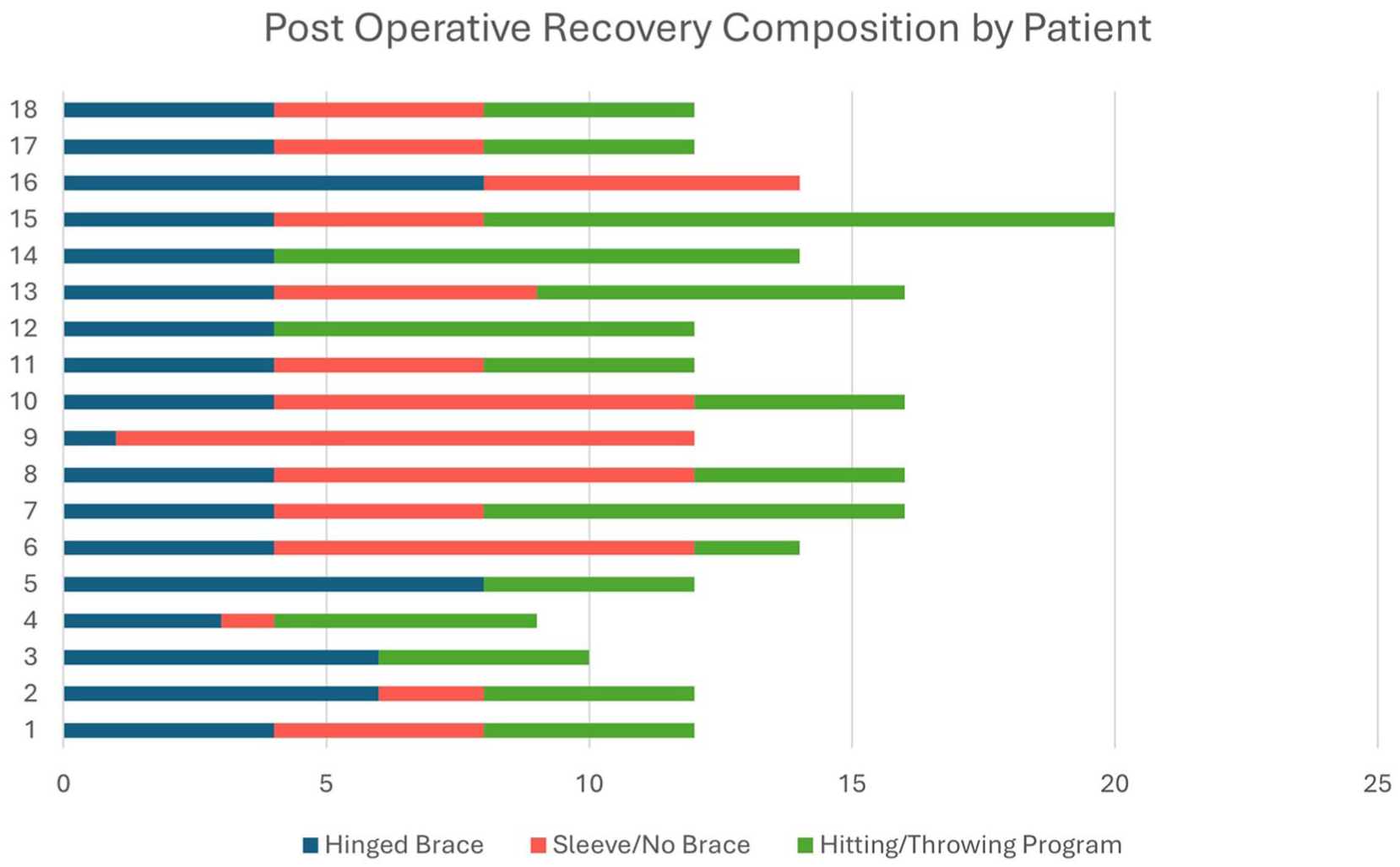
Postoperative recovery timeline and composition before return to sports.
The athletes in the study were followed radiographically until they were released. Except for two patients who were released without restriction at 10 weeks postoperative, at least 12 weeks of postoperative radiographic imaging was obtained for all patients (Figure 3). All athletes in this study achieved a stable union of their medial epicondyle fractures, as demonstrated on postoperative radiographs. One patient developed significant heterotopic ossification requiring arthroscopic debridement 2 weeks after the index surgery. This patient then had an uneventful postoperative course and was released for unrestricted RTS at 14 weeks after the original date of surgery.
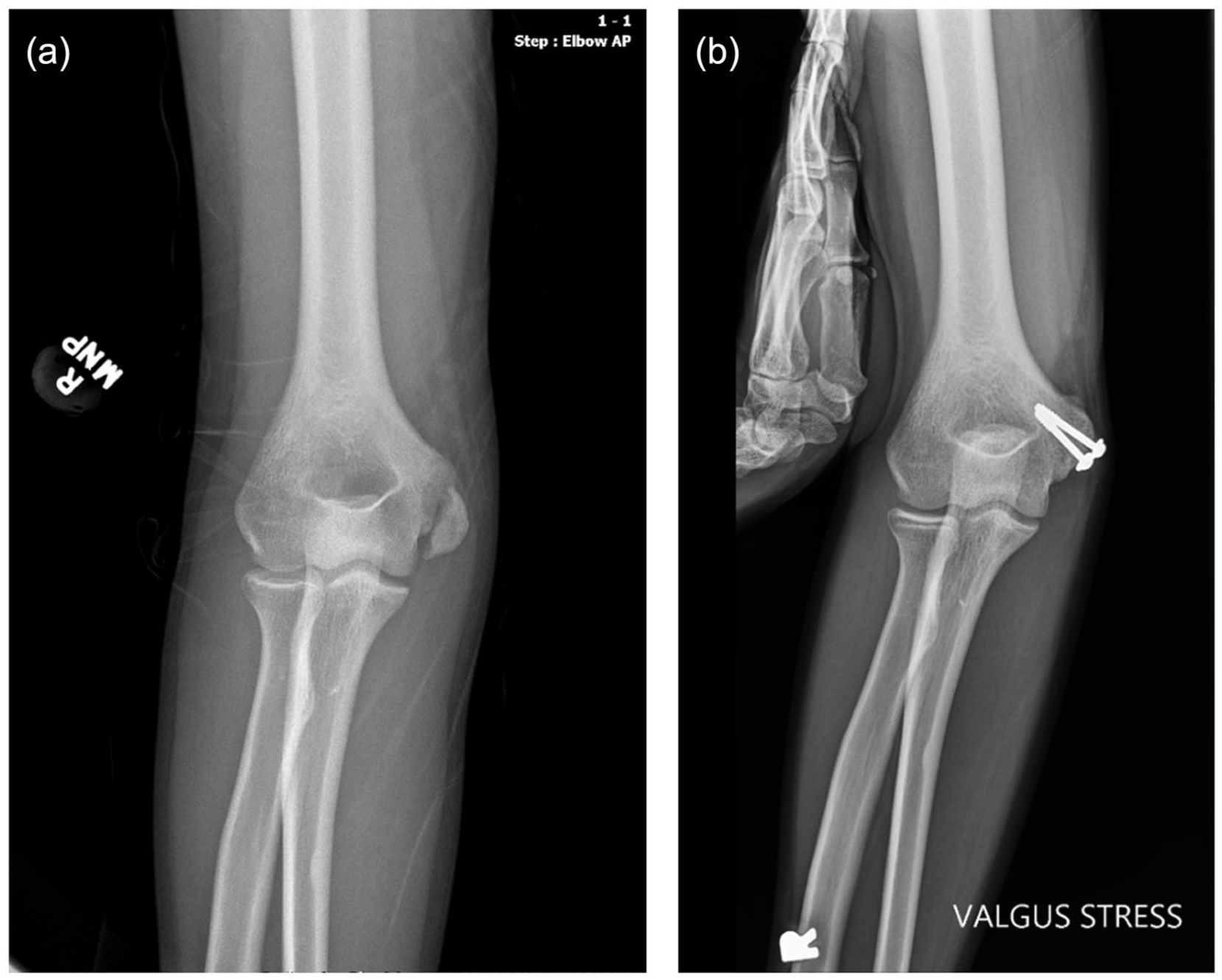
(a) Preoperative anterior posterior (AP) radiograph of the right elbow in a 15-year-old right hand dominant male baseball pitcher and (b) 12-week postoperative AP radiograph under valgus stress demonstrating union.
Discussion
Operative versus nonoperative management for pediatric medial epicondyle avulsion fractures is a controversial topic. There is little consensus concerning postoperative immobilization methods, which vary from hinged braces to casting, lasting up to 4 weeks. Some studies suggest that operative and nonoperative treatments result in similar RTS timelines, typically around 6 months, 11 with a systematic review reporting a best-case average of 3.8 months. 9 A recent randomized controlled trial of 72 patients, the majority of whom were gymnasts and soccer players, reported that nonoperative treatment of minimally displaced medial epicondyle fractures (<2 mm) was noninferior to surgical treatment after 1 year. 12 Nonoperative management of low-energy, minimally displaced fractures was further supported by a case series involving overhead athletes without associated dislocation or significant avulsion injury. 13 With an average time to unrestricted RTS of 13.4 weeks and a low complication rate, this study demonstrates that surgical fixation for displaced medial epicondyle fractures in pediatric athletes, coupled with an aggressive rehabilitation program, can have favorable short-term outcomes.
Time to unrestricted RTS
The athletes included in this study had favorable short-term outcomes and relatively swift recoveries. All 18 patients successfully returned to their pre-injury sporting activity and level of play at an average of 13.4 weeks postoperative. All demonstrated radiographic union of the medical epicondyle fracture at the time of their release. There is a paucity of data in the current literature regarding rehabilitation protocols and RTS after surgical fixation of these injuries in the pediatric athlete population. When compared to the existing literature, the patients included in our study had shorter times to unrestricted RTS than is typically reported. For example, Cain et al. 1 allowed patients to begin ROM exercises after1 week, aggressive strengthening programs after 8 weeks, and light throwing after 16 weeks. However, the authors did not allow athletes to return to unrestricted play until 6 months postoperative, and multiple patients were advised not to pitch during their first season after surgery. The protocol described in Cain et al.’s study was similar to ours in that ROM and physical therapy were prioritized early in the recovery period; however, they were much more cautious in allowing unrestricted sporting activities. In Osbahr et al.’s study, athletes returned to play at similar intervals to those of Cain’s study, which was an average of 7.6 months. For this group, requirements for initiating RTS or throwing programs included radiographic evidence of fracture union, satisfactory upper extremity strength, and pain-free ROM. 10 By contrast, the protocol presented in this study saw all 18 patients return to unrestricted sporting activities by 13.4 weeks (about 3.5 months) postoperative.
Immobilization
Immobilization of the elbow in the immediate postoperative phase is used to support healing, minimize edema, and reduce the risk of incidental trauma. However, prolonged immobilization in the pediatric population can lead to elbow stiffness 6 which may delay RTS. Jones and Beber reported that surgical patients were more likely to regain full ROM compared to those treated nonoperatively, identifying immobilization duration as the only independent predictor of residual stiffness. 14
Published studies vary widely in immobilization strategies, often employing rigid splints or casts for differing durations—from as short as 4 days to as long as 3 weeks.1,3,8,10 In Lee et al.’s 3 study, patients were immobilized in plaster splints for the first 10 days postoperatively, while Cain applied a splint for the first 5 days before transitioning to a brace. Case and Hennrikus 8 began with casting for 4 days before advancing to a brace for an additional 4 weeks.
By contrast, patients in our study were immobilized using a HEO locked at 90° of flexion for only 1 week postoperatively. After 1 week, the brace was unlocked, and restrictions were loosened to emphasize early ROM. This relatively short immobilization period and lack of casting or splinting can decrease the risk of elbow stiffness and avoid soft-tissue complications associated with prolonged casting.
ROM progression
As mentioned, postoperative protocols vary regarding the timing of initiation of passive and active ROM exercises. In our study, elbow ROM was initiated at the 1-week postoperative visit, significantly earlier than the average reported in the literature. A recent systematic review reported a mean initiation time of 2.8 weeks across published protocols, with most studies maintaining immobilization for 2–3 weeks before beginning motion. Our protocol allows for initiation of ROM earlier than other studies discussed, which possibly contributed to our decreased time-to-RTS.1,3,10 Our program, therefore, represents a distinctly accelerated timeline, emphasizing early, protected motion while maintaining fixation stability.
While other studies also prioritized early ROM, initiation of formal physical therapy was limited by the duration and method of immobilization. Lee et al. initiated ROM in their study by having patients move their fingers and hands while splinted for the initial 10 days, which is much more restrictive than our patients, who began physical therapy after 1 week, with emphasis on elbow ROM in an unlocked elbow brace. In Cain et al.’s study, patients began passive and active ROM between 5 days and 3 weeks postoperatively, with full passive ROM encouraged by 8 weeks. In comparison, by an average of 8 weeks, athletes in our study had already advanced to a progressive hitting or throwing program. In most studies, protocols erred on the side of more conservative timelines from immobilization to RTS programming to ensure safe recovery of the patient. Our results suggest that allowing a more lenient immobilization plan and earlier, more aggressive physical therapy can still allow for safe RTS at a significantly earlier time, of an average of 13.4 weeks, versus the reported average of 6–7 months.1,5
Complications
The patients included in our study had a 100% union rate of their medial epicondyle avulsion fractures. One patient developed symptomatic heterotopic bone growth, which required surgical removal 2 weeks after the initial surgery. The heterotopic bone was removed without incident, and this patient still returned to sports after 14 weeks. No patients developed surgical wound complications or had any issues related to symptomatic hardware.
Limitations
One limitation of this study was the COVID-19 pandemic, which occurred during the period included in this case series. In two cases, patients had difficulty obtaining new braces to downsize from the hinged brace due to supply chain shortages. In addition, two patients had difficulty scheduling physical therapy sessions due to staffing issues associated with the pandemic. It is unclear how much of a role the COVID-19 pandemic played in the availability or opportunity to rejoin sports.
As a retrospective study and case series, there was no control group. Furthermore, although all patients reported satisfaction with the postoperative results and progress in their recovery at the time of release, no validated patient-reported outcome measures (PROMs) were employed in this study. A future prospective investigation utilizing a control group and validated elbow PROMs could yield further insights into this topic. Lastly, the patient population included in this study was limited to competitive pediatric athletes, which could pose difficulties when applying our results to the broader pediatric population.
Conclusion
Early mobilization and an accelerated rehabilitation timeline after surgical fixation of medial epicondyle avulsion fractures can expedite RTS in high-demand pediatric athletes. This case series showed a low rate of complications and rapid RTS timelines.
Disclosures: This study was approved by the Institutional Review Board. We employed AI tools, including Grammarly for Microsoft Office, ChatGPT, and Gemini, to assist in revising sections of this article, with the sole aim of improving clarity and readability. However, all AI-generated edits underwent thorough review, editing, and final verification by the authors.
Supplemental Material
sj-pdf-1-cho-10.1177_18632521261423069 – Supplemental material for Let them move: Early range of motion and rehabilitation after fixation of medial epicondyle fractures in adolescent athletes
Supplemental material, sj-pdf-1-cho-10.1177_18632521261423069 for Let them move: Early range of motion and rehabilitation after fixation of medial epicondyle fractures in adolescent athletes by Brian Le, Taylor Troutman, Andre Perez-Chaumont, Felix H Savoie and Timothy Skalak in Journal of Children's Orthopaedics
Footnotes
Acknowledgements
The authors would like to express their sincere gratitude to Todd Nielsen, RN, for his invaluable assistance in facilitating initial access to patient information.
Author contributions
Brian Le: Data collection and analysis, Original draft; Taylor Troutman: Discussion, Editing, Reviewing; Andre Perez-Chaumont: Discussion, Editing, Review; Timothy Skalak: Conceptualization, Supervision; Felix H Savoie: Investigation, Visualization.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr. Felix Savoie receives royalties from CONMED, Exactech, and Zimmer Biomet. For the remaining authors, none were declared.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical statement
The study was conducted in accordance with the Declaration of Helsinki and was approved by the Tulane University Human Research Protection Office Institutional Review Board Committee of Tulane University (no. IRB #2023-1223) on September 21, 2023, with the need for written informed consent waived.
Data availability statement
The data have been hand-collected over many years, and we have plans to write an additional paper with this dataset. We will make the data available to the editors and, upon reasonable request, 24 months after publication of this paper.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.