
Abstract
Purpose
Traumatic elbow dislocation (TED) is the most common injury of large joints in children. There is an ongoing debate on the optimal treatment for TED. We aimed to assess the functional outcome after operative and nonoperative treatment of TED.
Methods
We analysed the medical records of patients with TED treated at the University Children's Hospital, Basel, between March 2006 and June 2015. Functional outcome was assessed using the Mayo Elbow Performance Score (MEPS) and Quick Disabilities of the Arm, Shoulder and Hand (QuickDASH) Sport and Music Module score. These scores were compared between nonoperatively and operatively treated patients.
Results
A total of 37 patients (mean age 10.2 years, 5.2 to 15.3) were included. Of these, 21 (56.8%) children had undergone nonoperative treatment, with 16 (43.2%) patients having had operative treatment. After a mean follow-up of 5.6 years (1.2 to 5.9), MEPS and QuickDASH Sport and Music Module scores in the nonoperative group and operative group were similar: MEPS: 97.1 points (SD 4.6) versus 97.2 points (SD 2.6); 95% confidence interval (CI)-2.56 to 2.03); p = 0.53; QuickDASH Sport and Music Module score: 3.9 points (SD 6.1) versus 3.1 points (SD 4.6); 95% CI 2.60 to 4.17; p = 0.94. We noted no significant differences regarding the long-term functional outcome between the subgroup of children treated operatively versus those treated nonoperatively for TED with accompanying fractures of the medial epicondyle and medial condyle.
Conclusion
Functional outcome after TED was excellent, independent of the treatment strategy. If clear indications for surgery are absent, a nonoperative approach for TED should be considered.
Level of evidence
Level III - therapeutic, retrospective, comparative study
Keywords
Introduction
With an incidence of three to six per 100 000 children, traumatic elbow dislocation (TED) is the most common injury of large joints in children.1,2 In approximately 60% of TEDs, avulsions and fractures of the medial epicondyle, radial neck, or coronoid process are present.1,2 The most common mechanism of trauma leading to TED is falling on the outstretched arm causing valgus stress on the elbow joint and hyperextension of wrist and fingers.2–5 The mean age for TED is about ten years, and male to female ratios cited range from 2:1 to 6:1.6,7,8 Nonoperative management of TED consists of closed reduction and short-term immobilization.9–11 Indications for operative treatment of TED include fragment entrapment in the humeroulnar joint, open fractures, complete elbow instability and vascular lesions.9,11 If such signs are absent, the indication for surgery depends on the surgeon's individual decision.11–15 In this study, we aimed to assess functional outcome after operative and nonoperative treatment of children with TED.
Patients and methods
The study was approved by the Ethics Committee of Northwestern and Central Switzerland (EKNZ 2015-045). Children aged up to 16 years presenting with TED to the University Children's Hospital, Basel, between March 2006 and June 2015 were included. Medical records were analysed for demographic and radiographic data. Analyses included the measurement of the magnitude of displacement of the medial epicondyle from its original anatomical position as shown on anteroposterior radiographs. Furthermore, the type of treatment and postoperative complications were assessed. Exclusion criteria were former fractures or dislocations of the elbow joint, associated injuries proximally or distally to the elbow joint, pre-existing neuromuscular, rheumatological or musculoskeletal diseases, and loss to follow-up.
Nonoperative treatment consisted of closed reduction of the dislocated elbow joint and immobilization by above-elbow cast with the elbow flexed by 90° and the forearm in neutral-pronation-supination position. Operative treatment included reduction of the dislocated elbow joint and open reduction and osteosynthesis of concomitant fractures.
Clinical examination on follow-up included assessment of the carrying angle, range of movement of the elbow joint, ligamentous stability of the elbow joint and range of pronation and supination of the forearm. To determine the extent of the displaced medial epicondyle, the distance between the upper margin of the apophyseal plate of the medial epicondyle at the distal humerus and upper margin of the medial epicondyle on the anteroposterior radiographs was measured. Functional outcome was assessed using the Mayo Elbow Performance score (MEPS; > 90 = excellent; 75 to 89 = good; 60 to 74 = fair; < 60 = poor) and the Quick Disabilities of the Arm, Shoulder and Hand (QuickDASH) Sport and Music Module score (0 to 100 scale, 0 = no functional limitation; 100 = maximum of functional restriction).16–18 Study data were processed using REDCap (Research Electronic Data Capture; international REDCap Consortium) tools. 19 The MEPS and the QuickDASH Sport and Music Module score were compared between nonoperatively treated and operatively treated patients. Additionally, the association between the degree of displacement of the avulsed medial epicondyle before treatment and elbow performance was investigated.
In an additional calculation, we focused on the subgroup of children who sustained TED with avulsion fractures of the medial epicondyle. We allocated patients who suffered TED with concomitant avulsion fracture of the medial epicondyle treated with closed reduction of the TED and immobilization of the arm in a plaster cast to group 1 (n = 8). Children with TED and avulsion fracture of the medial epicondyle and medial condyle treated with reduction of TED and osteosynthesis of the medial epicondyle and condyle were allocated to group 2 (n = 10).
Statistical analysis was performed with R Core Team 2016 (R Foundation, Vienna, Austria). A p-value of < 0.05 was considered significant.
Results
In total, we identified 65 children with TED. Of these, 28 (43.1%) patients were excluded because they met one or more of the exclusion criteria, or because they were lost to follow-up (LTFU). In all, 15 (23.1%) patients refused to take part in the study, and 13 (20.0%) patients were lost to long-term follow-up. Finally, 37 patients were included for analysis (Table 1). In the total population, mean age at injury was 10.2 years (5.2 to 15.3). Overall, 21 (56.8%) patients were treated nonoperatively (mean age 10.3 years (sd 2.5); Fig. 1), while 16 (43.2%) patients were treated operatively (mean age 10.1 years (sd 2.9); Table 1; Fig. 2). Of these, ten (27.0%) patients underwent osteosynthesis of a displaced medial epicondyle, four (10.8%) patients had osteosynthesis of other fractures of the elbow joint, and two (5.4%) patients underwent osteosynthesis of a displaced medial epicondyle and other fractures of the elbow joint. After a mean follow-up of 5.6 years (1.2 to 5.9), all children but one had excellent elbow performance, with a MEPS of 97.1 points (sd 4.6) in nonoperatively treated cases versus 97.2 points (sd 2.6) in operated cases (p = 0.53; 95% confidence interval (CI) -2.56 to 2.03); Table 2). 20 One case in the nonoperative group had 80 points due to pain on extending the elbow joint. The mean of the QuickDASH Sport and Music Module score was 3.9 points (sd 6.1) in nonoperative cases compared with 3.1 points (sd 4.6) in operative cases (p = 0.94; 95% CI -2.60 to 4.17; Table 2). There was no correlation of operative treatment and the degree of displacement of an avulsed medial epicondyle. No association between the extent of the initial displacement of the medial epicondyle and MEPS or QuickDASH Sport and Music Module score was seen.
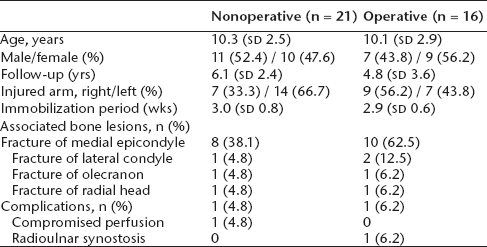
Baseline characteristics stratified by treatment (n = 37). Comparison between groups of children managed by nonoperative treatment of accompanying fractures (n = 21) and the group of children managed by operative stabilization of accompanying fractures (n = 16)

(
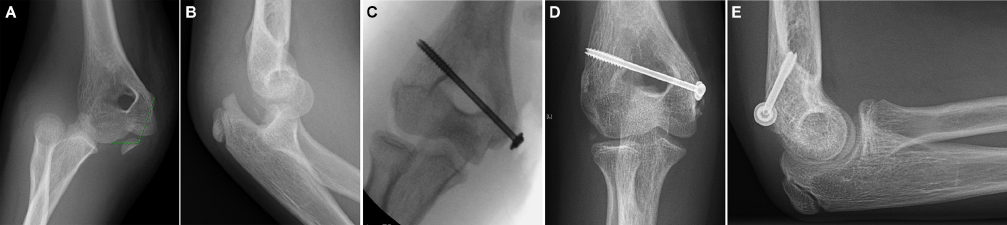
A girl aged 11.7 months fell from a wall onto her outstretched arm; (
Functional outcome of all children with traumatic elbow dislocation (n = 37). Functional elbow performance assessed by Mayo Elbow Performance score (MEPS) and Quick Disabilities of the Arm, Shoulder and Hand (QuickDASH) Sport and Music Module score; difference of mean (n = 37; mean follow-up: 5.6 years). The p-values were calculated using an exact Wilcoxon rank sum test according to Hollander and Wolfe (1999) 21 . Confidence intervals (CIs) were calculated according to Blaker et al (2000) 20

In the subgroup of children who sustained TED accompanied by avulsion fractures of the medial epicondyle and condyle (n = 18), we noted similar functional long-term outcomes for children treated by nonoperative management (n = 8) when compared with the group of children managed by closed reduction of TED and operative stabilization of the avulsed fragment (n = 10; Table 3 21 and Fig. 3).
Functional outcome of the subgroup of children who sustained traumatic elbow dislocation (TED) with concomitant avulsion fracture of the epicondyle (n = 18). Ten of these children underwent closed reduction of TED and operative stabilization of the avulsed fragment, and eight children were managed with nonoperative treatment. Functional long-term outcomes were assessed by Mayo Elbow Performance score (MEPS), and QuickDASH Sport and Music Module score. The p-values were calculated using an exact Wilcoxon rank sum test according to Hollander and Wolfe (1999) 21

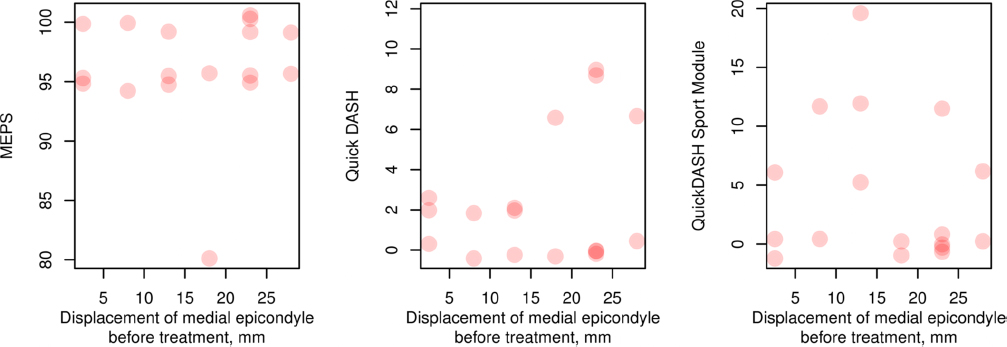
Association between displacement of the avulsed fragment of the medial epicondyle before treatment (in mm) and Mayo Elbow Performance score (MEPS) and Quick Disabilities of the Arm, Shoulder and Hand (QuickDASH) Sport and Music Module score in the subset of children who sustained traumatic elbow dislocation accompanied by avulsion of the medial epicondyle (n = 18).
Two children experienced complications. One nonoperatively treated patient developed a thrombosis of the brachial artery after closed reduction of the TED, which resolved by antithrombotic therapy with dalteparin for seven days. One patient in the group of operatively treated children developed a proximal radioulnar synostosis with the forearm fixed in a mid-pronation position. This patient refused surgical treatment of the synostosis and compensated the lack of pronation and supination with increased shoulder abduction and internal rotation.
Discussion
In this study, functional outcome after TED was excellent, irrespective of the treatment strategy. We assessed functional outcome by using the MEPS and QuickDASH Sport and Music Module score, both of which are widely accepted clinical scores for evaluation of elbow function and the ability to perform sports.16–18 Today, the use of rating systems is a standard part of evaluating treatment results. 19 However, proper validation studies are rare, and the outcome measurement tools might not always be used for appropriate populations of interest. 22
Several different rating systems have been introduced for the elbow joint.17,22–26 We assessed functional outcome by using the MEPS and QuickDASH Sport and Music Module score.16–18 The MEPS is a frequently used practical tool which combines assessment of the subjective (pain) and objective elbow condition.27,28 Additionally, the MEPS has already been used in the paediatric age group.8,14,27,29 Notably, only four items have to be scored to complete the MEPS, which eases the practical implementation. The questionnaire used most commonly for upper extremity injuries is the Disabilities of the Arm, Shoulder and Hand (DASH) score. 30 The QuickDASH is a shortened version of the DASH (11 instead of 30 items) and the QuickDASH Sport and Music Module score is an optional module of the QuickDASH score which is scored separately. 16 Corresponding to the MEPS, only four items are necessary to complete the QuickDASH Sport and Music Module score. Moreover, we considered the simplicity of this rating system and its relation to sports activities beneficial for the practical use of the questionnaire for children and adolescents.
Avulsion fractures of the medial epicondyle represent the most common injury associated with elbow dislocations. 14 One could assume that patients with a higher extent of displacement of the medial epicondyle would be more frequently treated operatively. However, our study did not support this notion. Instead, operative and nonoperative treatments were chosen irrespective of the extent of displacement of the medial epicondyle. Predefined indications for operative treatment of TED are fragment entrapment in the humeroulnar joint, open fractures, obvious elbow instability and vascular lesions.9,11 Displacement of an avulsed medial epicondyle from its original anatomic position in TED may not be an indication for surgery itself. Some authors advocate surgery only in cases of a ‘positive stress test’ after closed reduction of TED. 15 However, this ‘stress test’ is not clearly defined. There are different recommendations for operative treatment of TED depending on the degree of displacement of medial epicondyle (3 mm, 5 mm, 9 mm or ‘significant extent of displacement’). 15 Therefore, the indication for operative treatment of TED with avulsion fracture of the medial epicondyle seems to be based on the surgeon's preference rather than medical arguments.11–15
There is a great technical variety in the measurement of medial epicondyle displacement using plain radiographs.11–15 Regardless of the choice of measurement, clear differentiation between ‘minimally’, ‘moderately’ and ‘significantly’ displaced medial epicondyle is impossible without 3D CT. 31 Therefore, the indication for surgery based on the degree of dislocation of the avulsed medial epicondyle on plain radiographs may be less than ideal.
Our results confirm the findings of the systemic review on operative versus nonoperative management of paediatric epicondyle fractures published by Kamath et al. 12 Kamath et al 12 noted no significant differences regarding the outcome measures ‘pain’ and ‘ulnar nerve function’ between the groups of children treated operatively and nonoperatively. However, they noted a higher rate of bony union in the group treated operatively when compared with the group treated nonoperatively.
The functional demand of the elbow for individual patients represents another factor influencing the choice of treatment.32,33 Some authors recommend surgery in patients performing competitive sports requiring high elbow stability. 9 However, we observed no significant difference in the outcome scores between the nonoperatively versus operatively treated patients. This is in line with different clinical studies reporting return to previous activity levels after nonoperative treatment of TED with concomitant avulsion fracture of the medial epicondyle.34–37
The QuickDASH score, which comprises 11 questions, represents an abbreviated version of the DASH outcome measure score. 38 In accordance with Guyonnet et al 39 we noted that all our patients were able to answer the questions of the QuickDASH questionnaire together with their families without any significant problems.
The functional outcome results measured with the QuickDASH score for the cohort of children who sustained TED with accompanying avulsion fracture of the medial epicondyle or condyle were not significantly better for the group of children who underwent nonoperative treatment (n = 8) than for the group of children who underwent operative treatment (n = 10; p = 0.13). The functional outcome of fractures of the medial epicondyle or condyle in children assessed with the QuickDASH score compares well with the results obtained in a cohort of children who sustained fractures of the radial neck treated by elastic stable intramedullary nails. 39 This finding indicates the benign nature of elbow fractures in children.
One patient of the group of operatively treated children developed a proximal radioulnar synostosis with loss of supination and pronation. In this case, TED was accompanied by a displaced fracture of the radial neck and of the olecranon.
We are aware of some study limitations. These include the retrospective nature of our investigation and the small patient population.
For clear evaluation of medial epicondyle displacement, 3D CT or MRI would have been of great benefit. 31 Moreover, since measurement of the degree of displaced avulsed medial epicondyle is not standardized, we could not compare our results with others. There was no correlation of the degree of displacement of an avulsed medial epicondyle and operative treatment. In this regard we have to state that the measurement of medial epicondyle displacement using standard anteroposterior and lateral radiographs is an imprecise method with poor reliability. 40
In all, 13 (20.0%) patients were LTFU. LTFU is a form of selection bias that is unavoidable in most cohort studies, usually leading to loss of statistical power. 41 In evidence-based medicine, a cutoff of 80% LTFU is used to separate ‘high-quality’ and ‘low-quality’ randomized trials. 42 Different authors have suggested minimum acceptable follow-up rates between 50% and 80%.43,44 Kristman et al 41 demonstrated an unbiased estimate of effect with up to 60% LTFU in cohort studies if data were missing completely at random or missing at random, implying that dropouts were not related to the measured outcome variable. Since in our study the probability that a patient remained in the study did not depend on the outcome, we could assume that the effects of attrition should be low. However, our scope of definitive recommendations or meaningful statistical analysis was limited by LTFU.
Another limitation of our investigation is the comparison between several TED subgroups which not only included elbow dislocations with avulsion fracture of the medial epicondyle and condyle, but also TED complicated by other bone fractures. For more exact comparisons between subgroups, some investigations were repeated for subgroups of patients and thus, the compared subgroups were even smaller. Since there was no blinding of the outcome assessors, there was a risk for detection bias affecting the outcome measurements.
Our study demonstrated that when using clinical judgement to operate or not, there were no significant differences regarding functional outcome.
Conclusions
In our study, functional outcome after TED in childhood was excellent and was independent of the treatment strategy. There was full return to previous activity levels, including sports, after nonoperative treatment of TED with concomitant avulsion fracture of the medial epicondyle. We did not confirm any association of the extent of a displaced medial epicondyle before treatment and functional outcome. If clear indications for surgery, such as fragment entrapment in the humeroulnar joint, open fractures, obvious elbow instability and vascular lesions are absent, a nonoperative treatment strategy for TED in childhood should be considered.
Footnotes
No benefits in any form have been received or will be received from a commercial party related directly or indirectly to the subject of this article.
Ethical approval: This retrospective study was approved by the Ethics Committee of Northwestern and Central Switzerland (EKNZ 2015-045).