
Abstract
Purpose:
Open reduction internal fixation of paediatric medial epicondyle (ME) fractures can be technically challenging. The pull of the common flexor origin, ulnar nerve proximity, narrow ideal screw trajectory and sometimes fragmented epicondyle piece can make reduction difficult and lead to complications. Concern for tenuous fixation can lead to longer immobilization, placing the elbow at risk of stiffness. We describe a modified technique for screw fixation of ME fractures, with the goal of reducing complications and improving the stability of fixation.
Methods:
The modified technique includes insertion of a guidewire and pre-drilling for the screw prior to any fracture reduction, suture-assisted mobilization and control of the ME fragment, and conversion of the suture into a transosseous tension band to augment the screw fixation. A Retrospective chart review of 13 patients treated with this technique was undertaken to report early clinical and radiographic outcomes.
Results:
The average age at surgery was 12 years (range: 6–15). The mean follow-up was 8 months (range: 1–17). There was 100% fracture union with an average time to union of 7 weeks (range: 4–13). All patients obtained a functional range of motion with median flexion of 140° and median extension of 0°. Five patients had screw removal during follow-up. One patient had symptomatic ulnar nerve instability that was addressed at screw removal. There were no other complications.
Conclusion:
This technique improves ease of reduction and increases stability of fixation allowing earlier range of motion. This technique has provided reliable early results in our series of 13 patients.
Introduction
Medial epicondyle (ME) fractures of the elbow account for between 12%–20% of paediatric elbow fractures, most commonly occurring between the ages of 9–14 with a peak incidence between 11–12 years.1–3 These injuries can be secondary to a direct blow, though more frequently represent an avulsion event from an acute valgus or extension load, resulting in concomitant injury to the medial collateral ligament (MCL) and common flexor origin (CFO). 3 In up to 50% of cases, they are seen in combination with an elbow dislocation, in which 15%–25% result in the ME becoming entrapped within the joint. 2
Although debate exists regarding indications for surgical fixation of ME fractures, 1 most authors agree that a subset of these fractures benefit from open reduction and internal fixation.2,4–6
Surgical fixation of ME fractures, however, can be technically challenging. The CFO imparts an anterior and distal vector of pull on the ME piece. Bicortical screw fixation is desired to reduce the incidence of loss of reduction; however, there is only a narrow corridor of bone for the placement of the ideal screw trajectory. A Suboptimal trajectory can lead to guide wire-breakage during drilling, or breach of the olecranon fossa and associated extension impingement. 3 Additionally, the ME fragment can sometimes be small and prone to fragmenting during drilling or screw placement. Tenuous fixation from any of the above factors can prevent early mobilization and increase the risk of stiffness, particularly if the injury is associated with concomitant elbow dislocation.
To prevent and counter these potential complications, we developed a modified screw fixation technique for ME fractures. The primary differences to standard techniques are twofold:
Our focus on separate guide-wire placement and pre-drilling of the distal humerus and the ME piece, prior to any attempts at fracture reduction.
The use of an additional tension-band suture construct to augment screw fixation for increased stability to allow for earlier mobilization.
We also present the early results of the 13 elbows treated with this technique.
Surgical technique
Indication
Incarcerated ME fractures.
ME fractures with associated elbow dislocation.
ME fractures with displacement of >5 mm.
ME fractures in individuals participating in high-risk sports (gymnastics, martial arts, and throwing sports).
Room set up and positioning
The patient is positioned supine with the arm on a radio-lucent arm table. High arm tourniquet is used. The surgeon is at the patient’s axilla and the image intensifier is positioned to enter in line with the arm-table (at 90° to the operating bed; Figure 1).
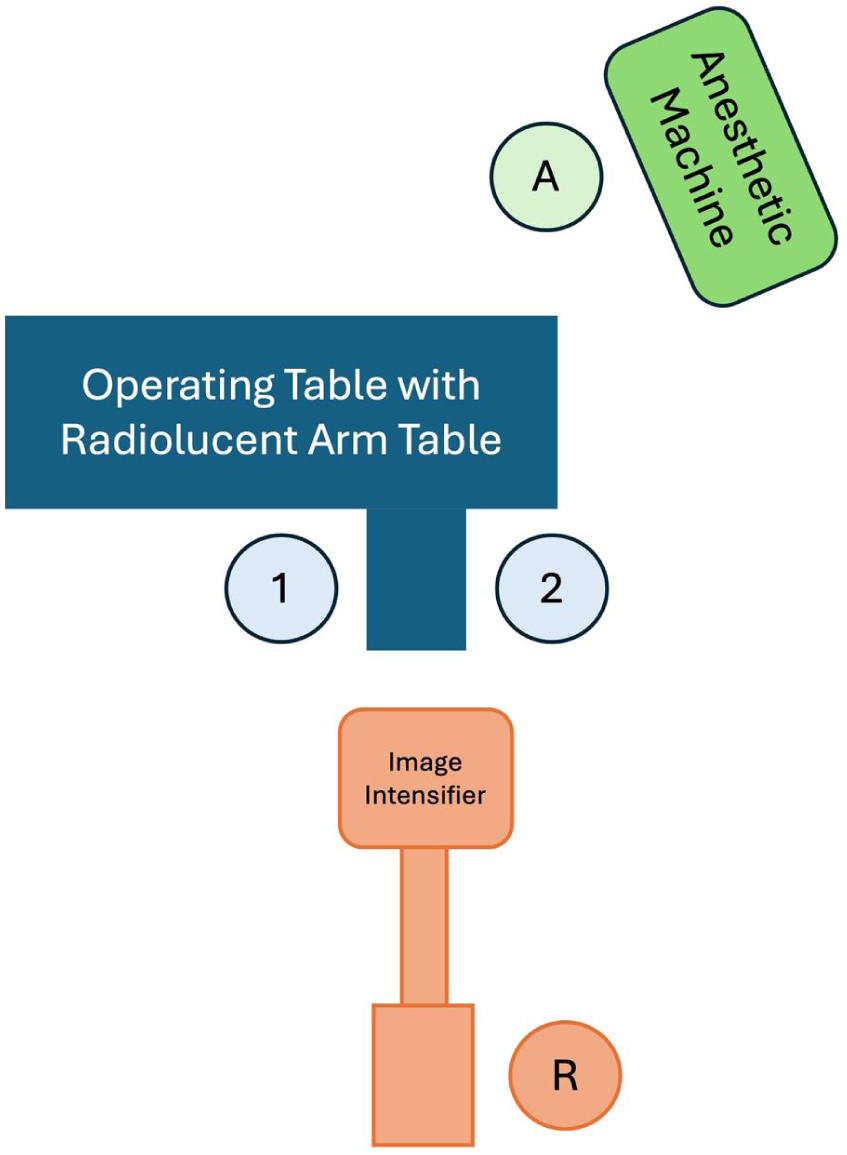
Room set up and patient positioning – Primary Surgeon (1) positioned in the patient’s axilla with the assistant surgeon (2), opposite.
Incision and exposure
A curved, longitudinal incision is made on the medial aspect of the elbow centred just posterior to the native position of the ME, understanding that the fragment usually displaces anteriorly and distally (Figure 2).
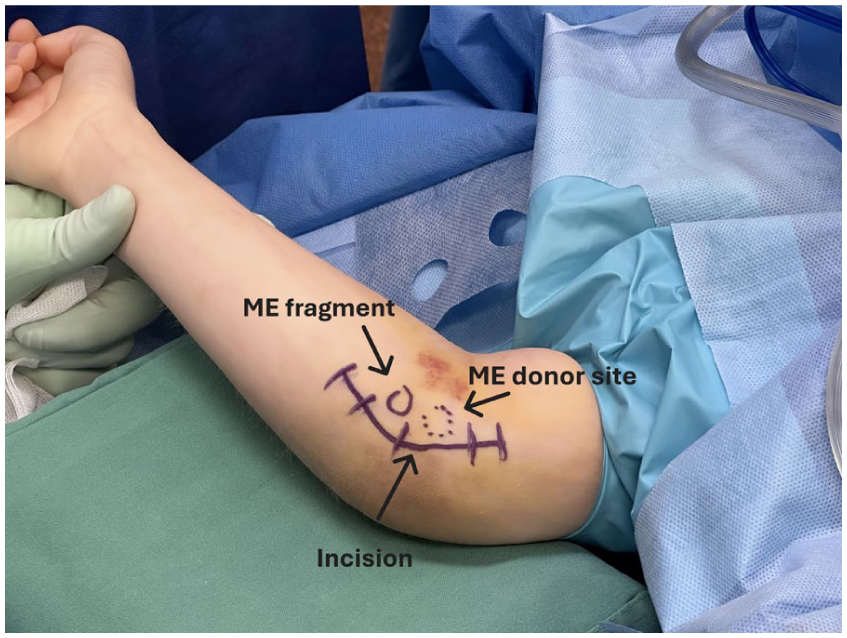
Medial view of the right elbow showing the planned surgical incision.
The ulnar nerve is identified and protected. Dissection of the ulnar nerve should be kept to a minimum to avoid secondary nerve instability. The ME fragment is mobilized and controlled using a non-absorbable suture (1.3 mm SutureTape, Arthrex, Naples, FL, USA) passed at the level of the bone-tendon junction in a locked configuration with a broad footprint (Figure 3). Care is taken during mobilization of the ME fragment such that the underlying MCL is not amputated. In our experience, the MCL is always attached to the ME piece.
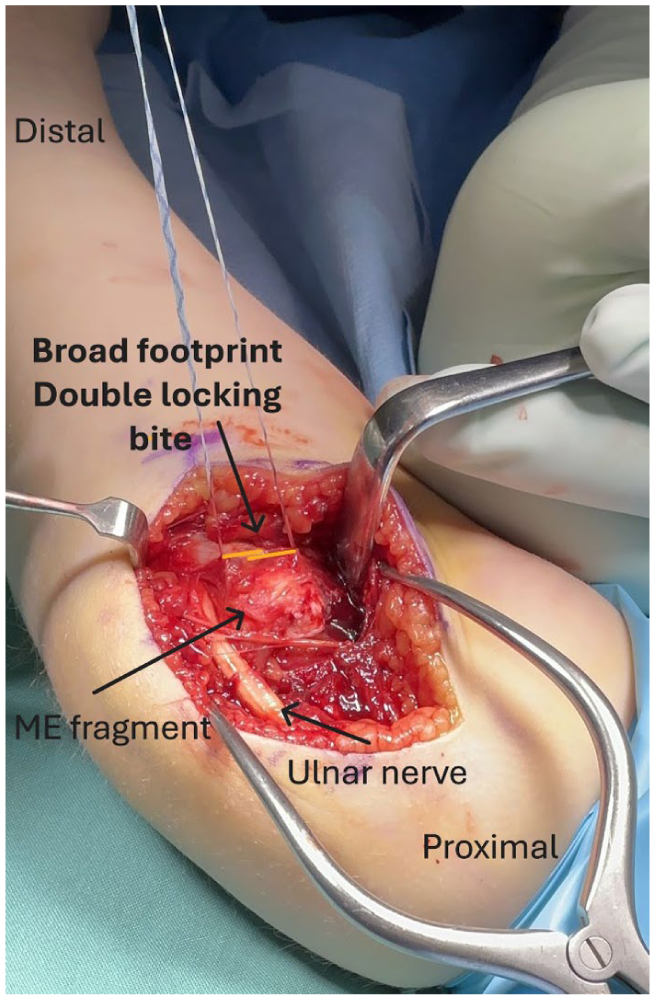
Medial epicondyle fragment controlled using suture.
Humerus preparation and drilling
With the ME fragment reflected distally using the control suture, the fracture bed on the distal humerus is then carefully defined. This area reliably forms an oval shape. The centre of this oval forms the humeral entry point of the guide wire. Making no attempt at fracture reduction, the guide wire for a cannulated, partially threaded screw (DePuy Synthes, Raynham, MA, USA) is placed at this entry point (Figure 4).
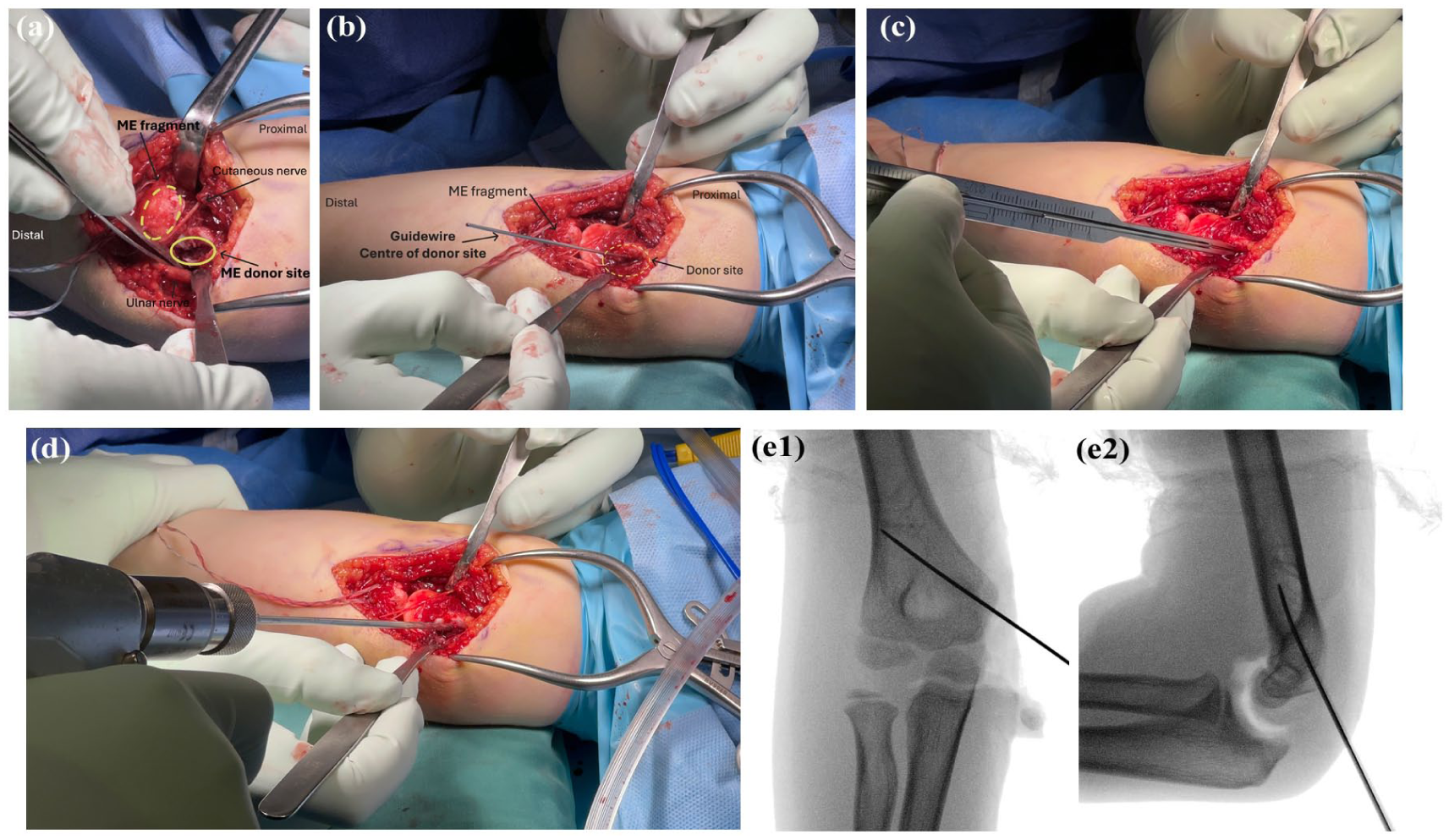
(a) Photo showing the ME fragment, the ME donor site, and the ulnar nerve for orientation. (b) Photo showing the guidewire being placed centrally in the ME donor site on the distal humerus – this is done on reverse to aid identification of the appropriate path within the medial column. Assistant retracting the anterior capsule and ulnar nerve throughout process. (c) photo depicting measurement and then (d) drilling of the donor site (e) Image intensifier images (AP and lateral) with a guidewire passed through the far cortex in the desired corridor.
A 4 mm screw is used for patients under the age of 12, while a 4.5 mm screw is used for those older than 12. A threaded tipped guidewire is used and advanced on reverse. Advancing the wire on ‘reverse’ allows it to find the optimal passage within the medial column and ‘bounce’ off other cortices such as that of the olecranon fossa or posterior cortex of the humerus. This is akin to the use of a pedicle finder in spine surgery to allow the instrument to naturally find its path in the cancellous bone without premature breach of cortex. Once the far cortex is reached, image intensifier is obtained to confirm position and to ensure wire is not curved (thereby risking breakage during drilling). The wire is then passed through the far cortex, and a cannulated drill is run over the guidewire, ensuring the far cortex is drilled. The drill and wire are subsequently removed from the distal humerus.
Medial epicondyle preparation and drilling
The same guide wire is then passed ‘inside-out’ into the ME piece, that is, from the fracture surface (Figure 5). This ensures a central position of the wire/screw in the ME piece and minimizes risk of ME fragmentation. Image intensifier is obtained, noting discrepancy may be observed between the central positioning of the wire under direct visualization versus position of the wire relative to the centre of the ossified portion of the ME, particularly in younger children. If this occurs, the former should be prioritized, as this constitutes the true centre of the ME. Taking care to protect the ulnar nerve, the ME is then drilled over the guidewire.
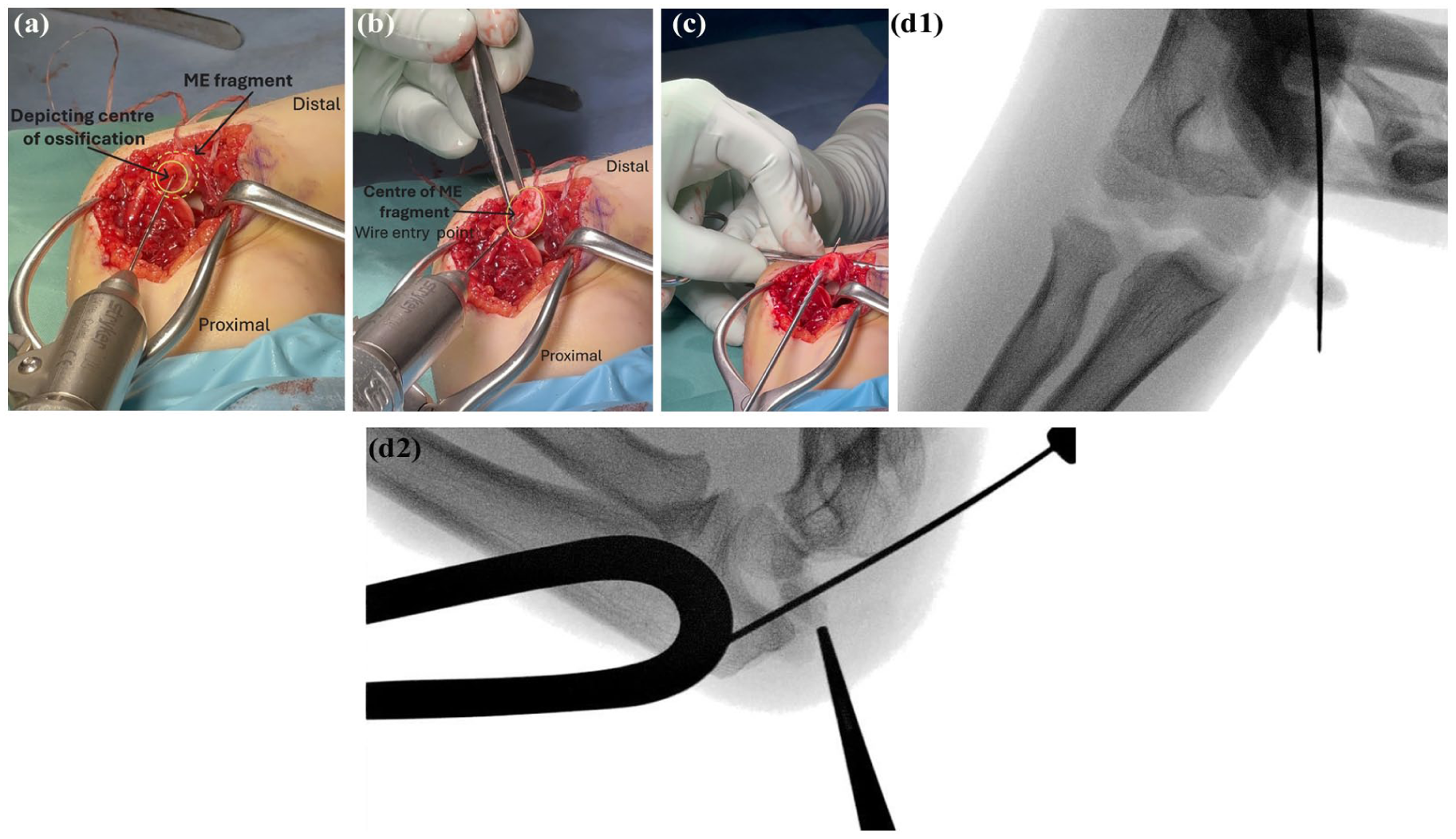
(a) Photo of ME with guidewire placed depicting the centre of the ossification fragment. This is not the entry point for the guidewire in most cases. (b) Photo of the guidewire placed in the centre of the ME fragment being passed in an ‘inside-out’ fashion. (c) Photo of drilling of the ME fragment with pressure placed on the outer aspect of the fragment to prevent fragmentation (d) Image intensifier images with guidewire in centre of ME fragment.
Reduction and screw fixation
Utilizing the traction suture, the ME is reduced, and the wire is placed by hand through both the pre-drilled ME fragment and distal humerus to the far cortex. Length for the screw is measured under image intensifier. A stainless steel, partially threaded cancellous screw with a washer is inserted, ensuring bicortical fixation. Image Intensifier is obtained to confirm far cortex is engaged and the fracture is adequately compressed (photo; Figure 6). It is our preference to use a stainless steel rather than titanium screw due to decreased propensity for screw bending and easier removal.
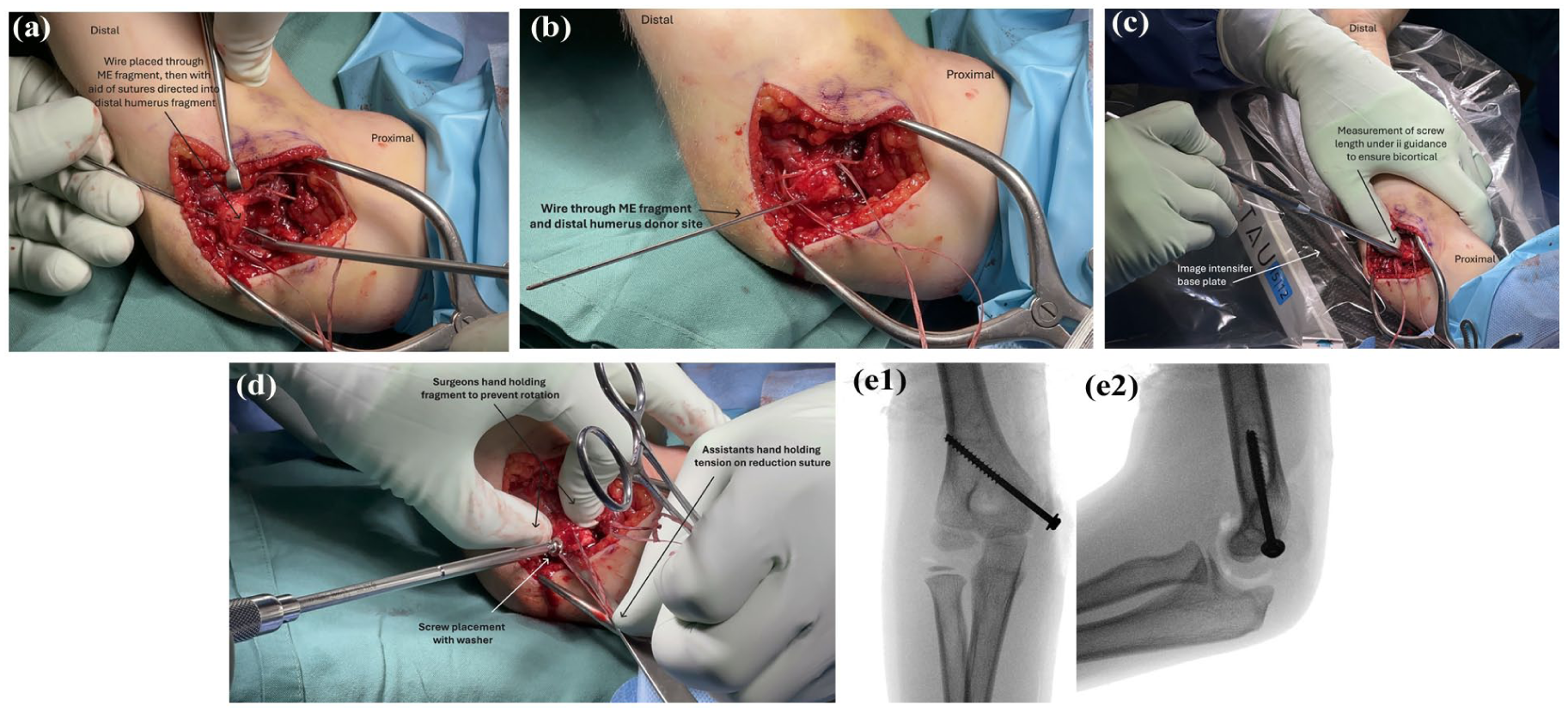
(a) Photo depicting guidewire being placed through ME fragment prior to reduction with aid of sutures. (b) Photo showing wire being docked in the distal humerus donor site tunnel. (c) Photo showing screw length being confirmed under ii guidance to ensure bicortical fixation. (d) Photo showing partially threaded stainless-steel screw with a washer being placed. During this process the surgeon is holding the ME fragment to prevent rotation, whilst the assistant is applying traction through the reduction suture. (e) Image intensifier images showing the final reduction and screw trajectory.
Tension band suture augmentation
Periosteum is elevated on the medial supracondylar ridge up to approximately 1cm above the fracture site. An anterior to posterior bone tunnel is drilled here using a 2 mm drill. The free ends of the traction suture are then passed in a figure-of-8 fashion through this trans-osseous tunnel and tied under maximal tension (Figure 7). This forms a tension-band suture fixation and augments the screw fixation. This dual fixation is particularly important in situation where ME piece is small or noted to be fragmented following drilling or screw placement.
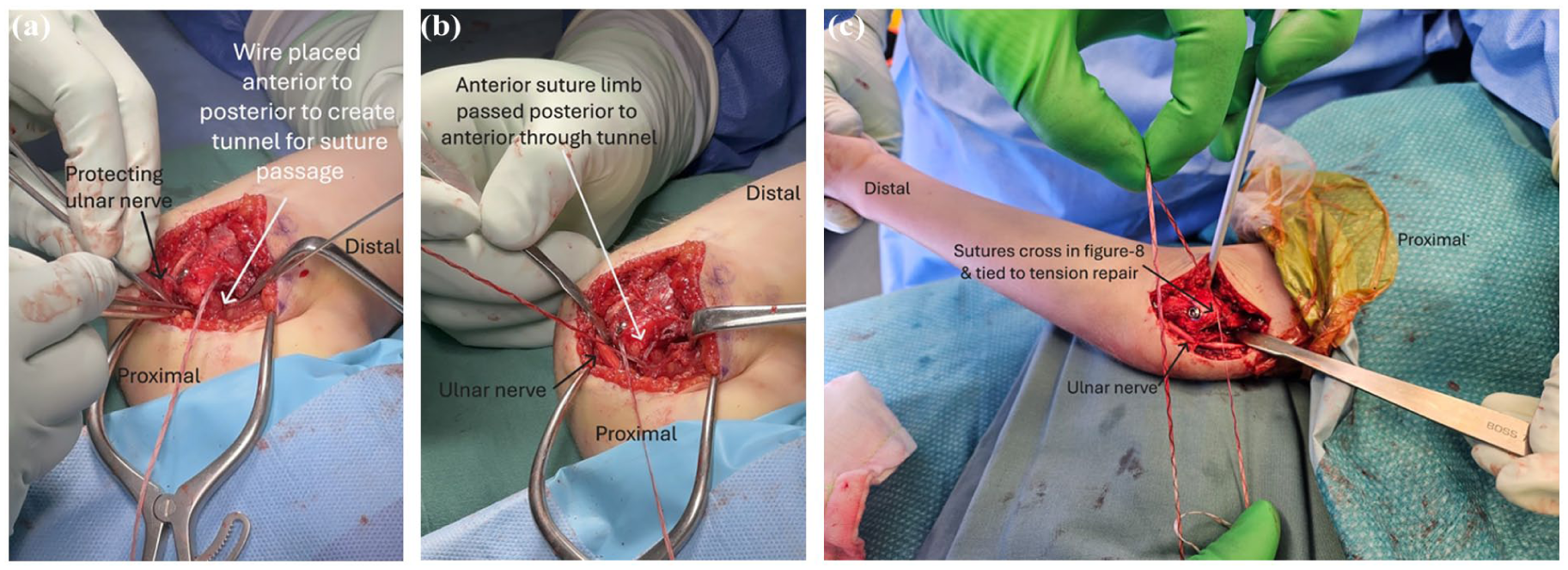
(a) Photo showing trajectory of anterior to posteriorly drilled tunnel to allow passage of tension suture. (b) Photo after anterior limb of suture has been passed posterior to anterior through the drilled tunnel with aid of a suture passer. (c) Photo showing the suture being tensioned and tied in a figure of 8 configuration – yellow line is the transosseous component.
Post-operative care
Post-operatively, the patient is placed in an above-elbow back slab for 10–14 days, then transitioned into a sling allowing full active and passive range of motion out of the sling with a physiotherapist. The sling is discontinued at 4 weeks post-operatively. Resumption of sport is allowed once radiological union is achieved, or when 8 weeks has elapsed since surgery, whichever occurs earlier.
Methods
We performed a retrospective chart review of patients treated with the modified technique. Patients were included if they had at least 6 weeks of follow-up. Notes and radiographs were reviewed for demographic data, injury pattern, associated fractures, time to union, range of motion, complications and reoperation data.
Results in 13 elbows
Between 2022 and 2025, 15 patients were treated with the above surgical technique. Two patients failed to attend follow-up beyond 4 weeks post-operatively and were excluded. The remaining 13 patients (13 elbows) are included for analysis.
The average age at surgery was 12 (range: 6–15). There were 6 boys and 7 girls. Four elbows had ME injury with associated elbow dislocation, and one had an entrapped ME. One elbow had an associated Monteggia fracture/dislocation. The average time from injury to surgery was 5 days (range: 1–13 days). The mean follow-up was 8 months (range: 1.5–17 months). All elbows achieved union, with average time to union 7 weeks (range: 4–13 weeks; Figure 8).
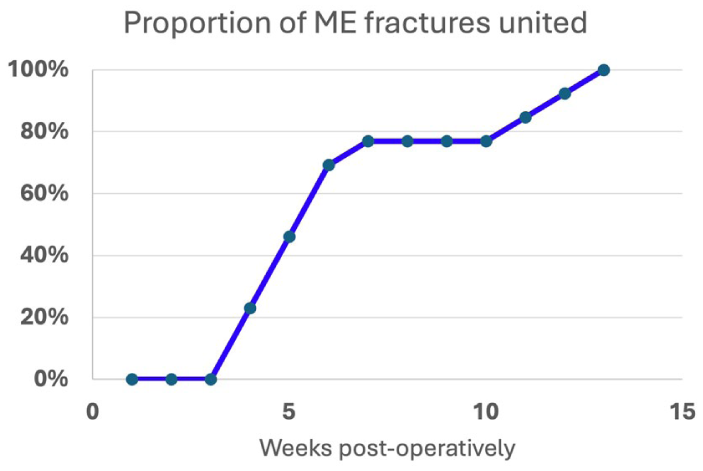
Proportion of medial epicondyle fractures achieving union with the described technique by weeks post-procedure.
No patients reported persistent pain at latest follow-up. All patients obtained a functional range of motion with median flexion 140° (range: 120°–145°) and median extension of 0° extension deficit (range: 10° hyperextension to 10° extension deficit).
Five patients had screw removal during the follow-up period (total 40%). One patient had symptomatic ulnar nerve instability that resolved following screw removal and subcutaneous ulna nerve transposition. No complications of wire breakage, non-union, symptomatic malunion, olecranon fossa perforation, or stiffness requiring contracture release were seen.
Discussion
Biomechanical testing of ME fixation methods in a porcine model identified screw fixation as being stronger and stiffer than alternative divergent K-wire and suture bridge constructs. 7 The mode of failure of screw fixation was fracture fragmentation around the screw head, while the fragment slid off the smooth K-wires and the suture anchors pulled out of the humerus bone model. Nielsen et al. 8 demonstrated similar complications by mode of fixation in their case series. We believe the addition of a tension band construct to screw fixation neutralizes the deforming forces of the CFO, 9 much like in proximal humerus fracture fixation. 10 Additionally, in ME fixation, the fragment is often small and can further become fragmented during drilling and screw placement. Thus, augmentation using a suture-tension band can mitigate the risk of loss of fixation. The security from a secondary fixation method also allows earlier mobilization of the elbow, which commences at the 2-week mark. This may be beneficial in mitigating the risks of post-operative stiffness.
One of the biggest challenges in ME fixation is obtaining and maintaining reduction of the fragment whilst placing the wire centrally in the ME, and through a narrow corridor of bone in the distal humerus. There have been several previous papers describing techniques including milking manoeuvres, 2 using an Esmarch bandage,11,12 joystick of fragment, 2 adjunctive wires or needles,2,11,12 use of reduction clamps and even prone patient positioning.4,11 However, these techniques remain difficult, present positioning challenges for anaesthetists, require experienced assistants, and optimal position of elbow to be effective. Our separate guide-wire insertion and drilling sequence prior to any attempted reduction enables the surgeon to easily achieve optimal position of screw and almost effortless reduction.
Conclusion
We present a technique for ME fracture fixation that improves ease of reduction, increases stability of fixation, allowing earlier range of motion, and may reduce complications. This technique has provided reliable early results in our series of 13 patients.
Supplemental Material
sj-docx-2-cho-10.1177_18632521251400160 – Supplemental material for Modified screw fixation technique for medial epicondyle fractures to reduce complications and improve stability of fixation
Supplemental material, sj-docx-2-cho-10.1177_18632521251400160 for Modified screw fixation technique for medial epicondyle fractures to reduce complications and improve stability of fixation by Charles Haward, Megan Cain and Kemble Wang in Journal of Children's Orthopaedics
Supplemental Material
sj-pdf-1-cho-10.1177_18632521251400160 – Supplemental material for Modified screw fixation technique for medial epicondyle fractures to reduce complications and improve stability of fixation
Supplemental material, sj-pdf-1-cho-10.1177_18632521251400160 for Modified screw fixation technique for medial epicondyle fractures to reduce complications and improve stability of fixation by Charles Haward, Megan Cain and Kemble Wang in Journal of Children's Orthopaedics
Footnotes
Author contributions
CH: Data analysis, Data collection, Data interpretation, Writing. MC: Data analysis, Data collection, Review and editing. KW: Data analysis, Data collection, Review and editing, Technique development.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical statement
This project was conducted in accordance with the Declaration of Helsinki and received ethical approval from the Melbourne Children’s Campus Research Ethics Department (Project Number 4389) on April 06, 2025. This is an IRB-approved retrospective case series; all patient information was de-identified and patient consent was not required. Our institution does not require ethical approval for reporting individual cases or case series.
Data availability
The dataset generated and analyzed for this study are available from the corresponding author on reasonable request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.