
Abstract
Purpose:
Pediatric femoral neck fractures (PFNFs) are rare (≈1% of pediatric fractures), and avascular necrosis (AVN) is a devastating complication without a universally accepted management. High-degree posterior rotational osteotomy (HDPRO) with three-dimensional (3D) navigation is a novel joint-preserving technique with the potential to improve outcomes.
Methods:
A retrospective case series was conducted with three pediatric patients (2 boys, 1 girl; aged 9–15 years at injury) diagnosed with AVN secondary to PFNF. All underwent HDPRO using Stryker OrthoMap 3D navigation to reposition the viable anteromedial femoral head. Preoperative and postoperative outcomes were assessed using radiographic analysis, functional scoring (Japanese Orthopaedic Association Hip-Disease Evaluation Questionnaire (JHEQ)), and sports participation. Follow-up ranged from 24 to 36 months.
Results:
All patients showed pain relief, functional improvement, stable femoral head morphology, and revascularization. JHEQ improved to 79–84 points; hip motion normalized without impingement. All patients returned to sports (track, volleyball, cycling).
Conclusions:
HDPRO with 3D navigation is a promising joint-preserving option for AVN following PFNF. Preliminary results are favorable; however, the small cohort and limited follow-up warrant larger studies.
Significance of study:
To the best of our knowledge, this is the first report demonstrating that navigation-guided HDPRO reliably relocates the viable anteromedial head to the load-bearing zone.
Level of evidence:
Level IV
Keywords
Background
Avascular necrosis (AVN) associated with pediatric femoral neck fractures (PFNFs) is challenging to treat, representing a major, unresolved issue for orthopedic surgeons. Transtrochanteric rotational osteotomy (TRO), developed by Sugioka, has demonstrated favorable outcomes in managing extensive osteonecrosis of the femoral head (ONFH). 1 TRO relies on achieving a healthy area occupancy of ≥40%, as planned preoperatively, which is critical for successful postoperative results. 2 Achieving this requires precise intraoperative reproduction of the planned osteotomy surface and expertise to minimize vascular injury. However, conventional methods often fail to accurately perform osteotomies as planned. 3 These limitations can lead to insufficient healthy area occupancy, postoperative range of motion restrictions, and delayed motor function recovery. Recent advances in computer-assisted surgery (CAS) have addressed these challenges by enabling the precise execution of the preoperative osteotomy plan, resulting in improved postoperative outcomes. 4 High-degree posterior rotational osteotomy (HDPRO), as developed by Atsumi et al., offers an innovative approach to treating AVN. By allowing posterior rotation of over 100°, this technique repositions the viable anteromedial portion of the femoral head into the weight-bearing zone, yielding excellent clinical outcomes.5–8 From a vascular perspective, the anteromedial portion of the femoral head is frequently preserved in cases of AVN following PFNF, making it an optimal target for relocation. Herein, we present three cases of AVN following PFNF treated with HDPRO using a navigation system. Functional recovery and radiographic outcomes were assessed, and all patients successfully returned to sports within 1 year postoperatively. This study emphasizes the potential clinical impact of HDPRO as a joint-preserving technique for AVN.
Material and methods
This study focuses on three patients diagnosed with AVN following PFNF. It is presented as a retrospective case series highlighting the application of HDPRO.
Study design and participants
This is a retrospective case series conducted to evaluate the effectiveness of HDPRO in managing AVN after PFNF. Written informed consent for publication was obtained from all participants and their guardians. The participants included one 9-year-old patient and two 15-year-old patients at the time of injury. Fracture types were classified using the Delbet–Colonna classification, with two cases identified as type II and one as type IV (Table 1).
Patient background.
Surgical approach
All surgeries were performed using the HDPRO technique with the Stryker OrthoMap three-dimensional (3D) navigation system. The surgical concept and the effect of high-degree posterior rotation are illustrated in Figure S1 by comparing the femoral head position before osteotomy and after rotational osteotomy. A detailed, stepwise technical description, including registration, osteotomy execution, and rotational adjustment, has been previously reported. 9 This technique enables precise alignment while minimizing soft tissue damage. Preoperative imaging classified all cases as type C2, stage IIIb according to the Japanese Investigation Committee Classification (JIC) criteria for ONFH.
Imaging and preoperative planning
To ensure accurate visualization of the osteotomy plane and surrounding structures, preoperative computed tomography (CT) scans with 1.25 mm slice thickness were performed; CT data were imported into the Stryker OrthoMap system for surgical simulation. Based on coronal CT images, the proportion of the viable femoral head area within the weight-bearing region was evaluated using Miyanishi’s method. 2
Postoperative evaluation
Radiographic evaluation
Joint space narrowing and leg length discrepancy (LLD) were measured in the standing position at 2 years postoperatively.
Femoral anteversion angle
Changes in femoral anteversion angles pre- and postoperatively were measured using the OrthoMap 3D system to assess surgical alignment.
Functional outcomes
Pain, function, and quality of life were assessed using the Japanese Orthopaedic Association Hip-Disease Evaluation Questionnaire (JHEQ) as a patient-reported outcome measure. 10
Video-based assessment
Motor function approximately 1 year postoperatively was documented in a video.
Results
Case 1
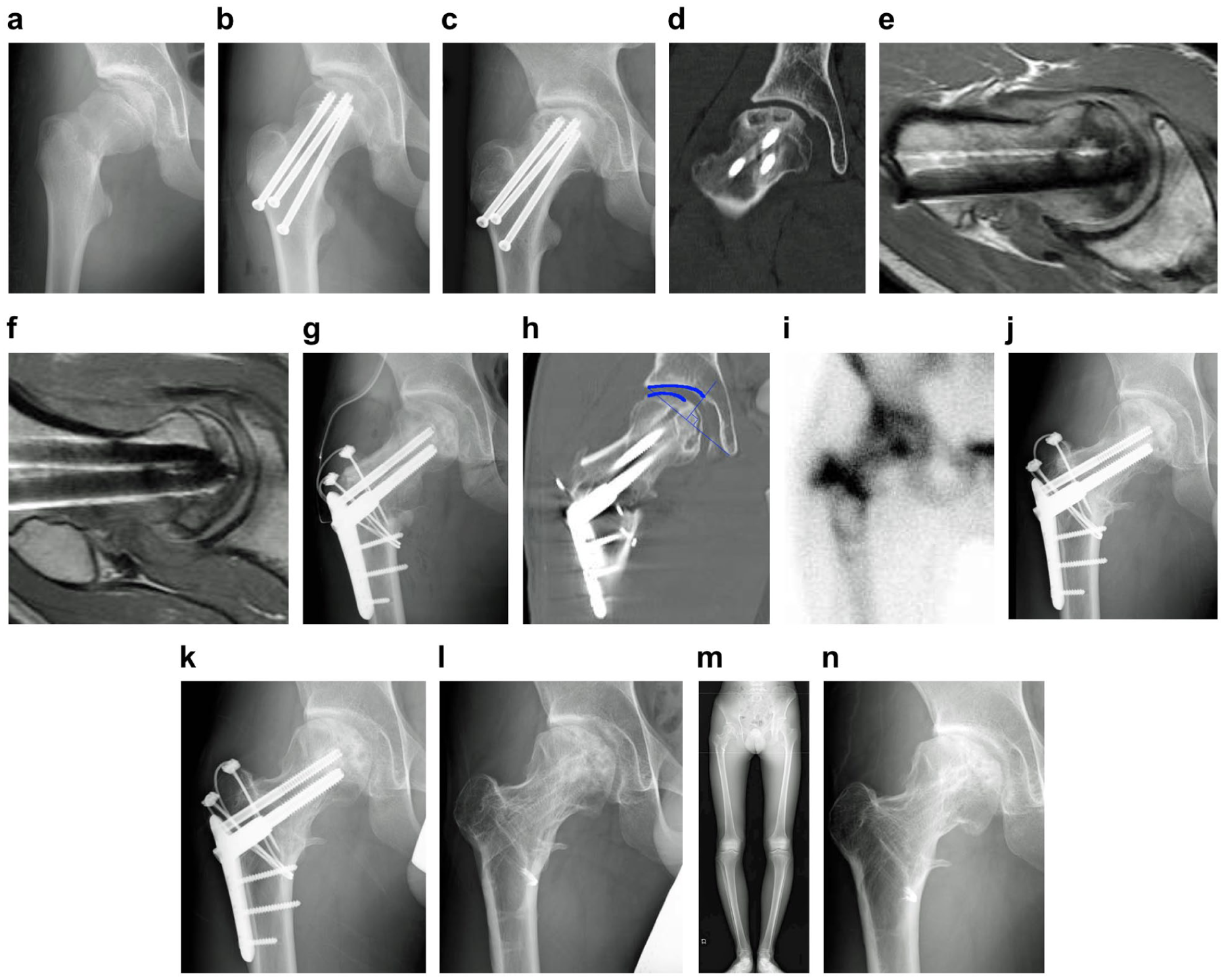
A 9-year-old girl (Delbet II) (Figure 1(a)) underwent urgent closed reduction and internal fixation (CRIF) within 24 h (Figure 1(b)) but developed progressive collapse by 11 months (Figure 1(c)); JIC C2 stage IIIb was confirmed. (Figure 1(d)). Radial MRI 7 showed no viable sector at ~90° (Figure 1(e)), but a clear anteromedial viable sector was visible at 120° (Figure 1(f)). Thus, HDPRO 120° with 10° varus was performed (Figure 1(g)). Operative time was 145 min; blood loss was 300 mL. Healthy area occupancy reached 56% on CT (Figure 1(h)). 5 At 4 weeks, bone scintigraphy showed good uptake (Figure 1(i)). Partial weight-bearing was advanced per protocol; full weight-bearing at 6 months (Figure 1(j)). Running was allowed 9 months after surgery. Union was confirmed by 16 months with hardware removal thereafter (Figure 1(k)). At 1 year and 7 months after surgery, she entered junior high school, joined the track and field team (Figure 1(l)), and enjoys youth (Table 2). At the last observation 3 years after surgery (Figure 1(m)), the range of motion was good, with a perfect JHEQ score of 84 points. The LLD at 2 years after surgery was 9 mm on X-ray (Figure 1(n)); however, there was no perceived LLD (Table 3).
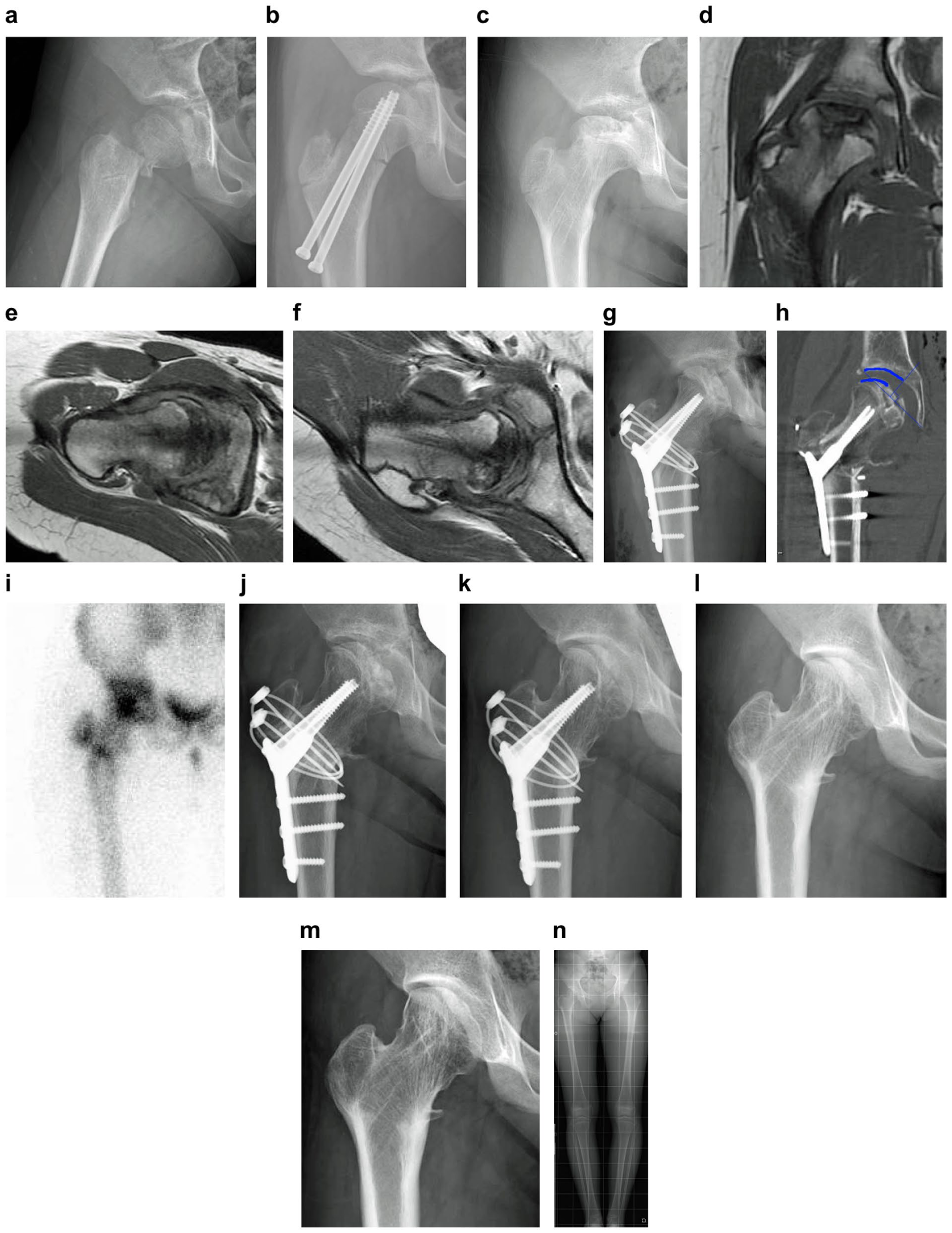
(a) Delbet–Colonna type II fall trauma. (b) Closed reduction and internal fixation. (c) Extensive crushing was observed at the time of initial examination at our hospital. (d) Stage IIIb using the Japanese Investigation Committee Classification on magnetic resonance imaging, equivalent to type C2. (e) Radial magnetic resonance imaging 90° Lauenstein view. No healthy area was observed anteriorly and posteriorly. (f) Radial magnetic resonance imaging 130° Lauenstein view showing a healthy area in front. (g) Immediate postoperative 120 high-degree posterior rotational osteotomy 10° internal rotation. Operation time was 145 min, and blood loss was 300 mL. (h) Healthy area occupancy rate of 56% observed in the center slice of the femoral head on coronal computed tomography according to Miyanishi’s method. (i) 99mTc bone scintigraphy shows accumulation and good blood flow. (j) At 6 months after surgery, bone union at the osteotomy site was observed, and full load-bearing was permitted. (k) At 1 year and 4 months after surgery, bone union was seen, and intraosseous foreign body removal was performed. (l) At 2 years after surgery, the patient is a member of the track and field team and enjoying youth. (m) At 3 years after surgery, at the time of the final observation, spherical reconstruction of the femoral head is observed with no osteoarthritis changes. (n) There is no subjective leg length difference, although there is a 9 mm left–right difference of the whole lower extremity 2 years after surgery.
Postoperative clinical evaluation.
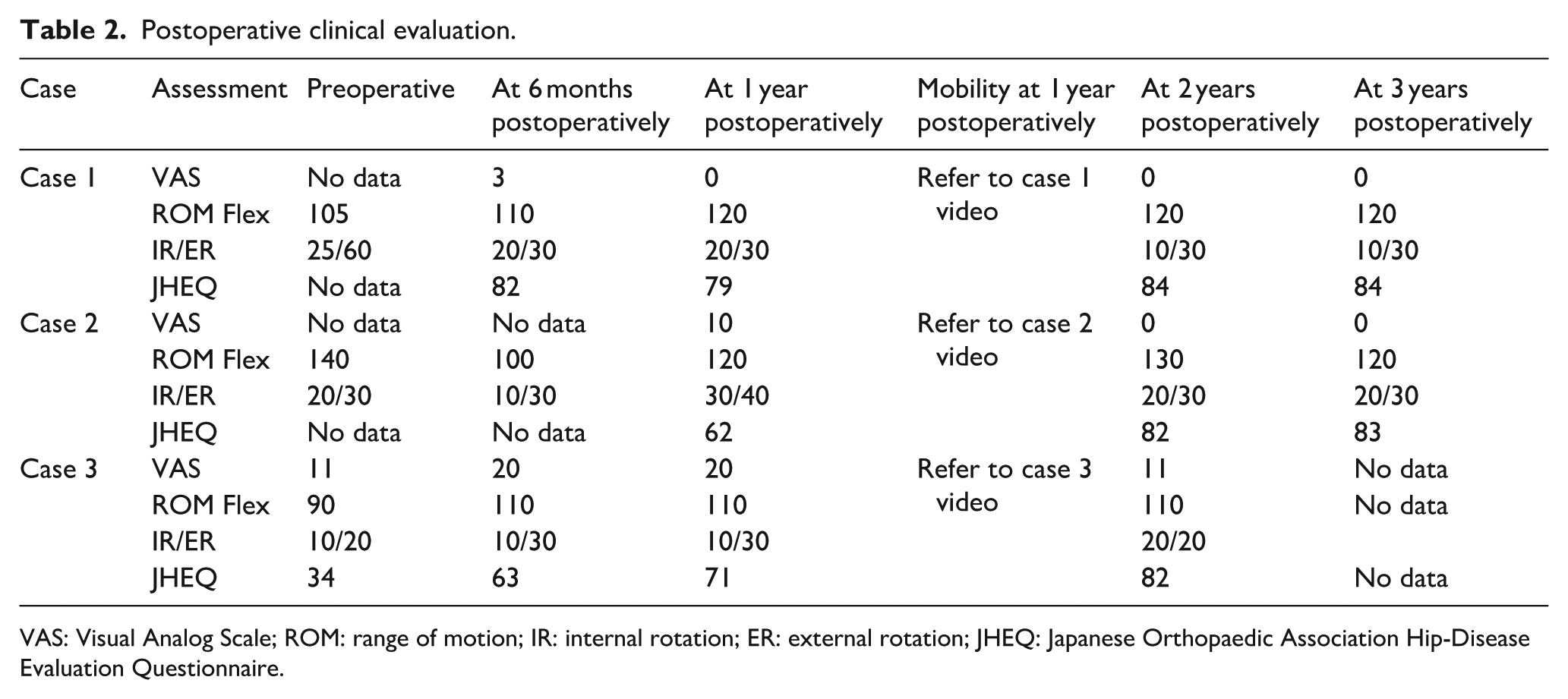
VAS: Visual Analog Scale; ROM: range of motion; IR: internal rotation; ER: external rotation; JHEQ: Japanese Orthopaedic Association Hip-Disease Evaluation Questionnaire.
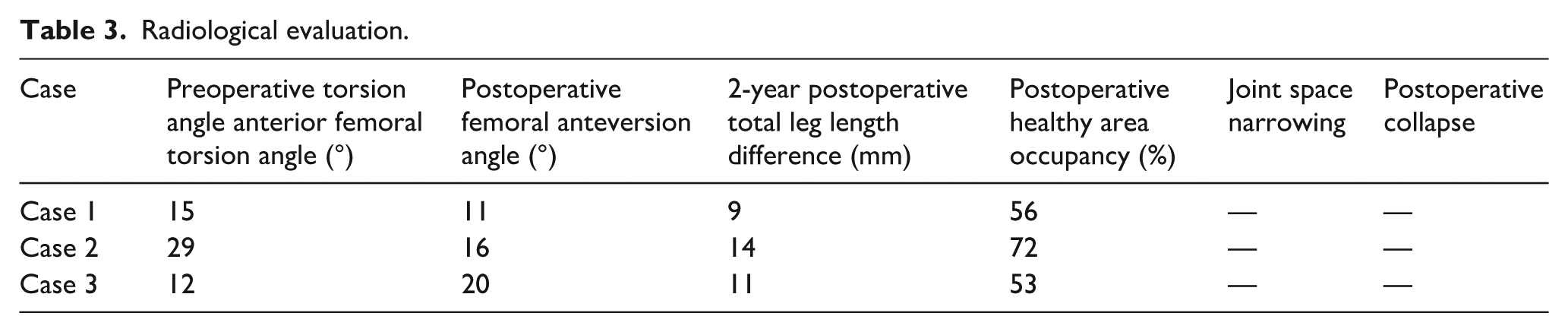
Radiological evaluation.
Case 2
A 15-year-old boy (Delbet II) (Figure 2(a)) treated with CRIF (Figure 2(b)) developed C2 stage IIIb AVN. (Figure 2(c) and (d)). Radial MRI demonstrated no viable sector at ~90° (Figure 2(e)) but a preserved anteromedial sector was visible at 120°–130° (Figure 2(f)); HDPRO 130° with 10° internal rotation was performed. Operative time was 120 min; blood loss was 750 mL (Figure 2(g)). Healthy area occupancy was 72% (Figure 2(h)). Scintigraphy at 1 month showed good uptake (Figure 2(i)). Full loading at 6 months (Figure 2(j)); return to volleyball at 1 year (Figure 2(k)) (Table 2); and hardware removal at 15 months. The patient has been engaged in moderately strenuous physical labor at 2 years after surgery (Figure 2(l)). LLD at 2 years after surgery was 14 mm (Figure 2(m)). No perceived LLD was observed (Table 3). At the last observation, the range of motion was good at 3 years after surgery (Figure 2(n)), with a JHEQ score of 83 points (Table 2).
(a) Delbet–Colonna type II fall injury while riding a bicycle. (b) Closed reduction and internal fixation with 3 × 6.5 mm screws within 24 hours. (c) At 8 months after closed reduction and internal fixation, the patient was referred to our hospital upon noticing crushing. (d) Type C2, stage IIIb, diagnosed at the time of the consultation using the Japanese Investigation Committee Classification. (e) Radial magnetic resonance imaging 90° Lauenstein view. No healthy areas were observed anteriorly and posteriorly. (f) Radial magnetic resonance imaging 130° Lauenstein view. A healthy area was observed anteriorly. (g) 130 high-degree posterior rotational osteotomy 10° internal rotation. Surgery time was 120 min, and blood loss was 750 mL. (h) Healthy area occupancy rate of 72% seen in the center slice of the femoral head on coronal computed tomography according to Miyanishi’s method. (i) 99mTc bone scintigraphy shows accumulation and good blood flow. (j) At 6 months after surgery, full load-bearing was permitted. (k) Permission to return to sports at 1 year after surgery. (l) At 2 years after surgery, the patient is engaged in light physical labor. (m) Leg length discrepancy at 2 years after surgery was 14 mm, but no subjective leg length difference was perceived. (n) Range of motion is good at 3 years after surgery. The Japanese Orthopaedic Association Hip-Disease Evaluation Questionnaire score was high.
Case 3
A 15-year-old boy (Delbet IV) (Figure 3(a) and (b)) who was initially treated conservatively developed painful collapse (C2 stage IIIb) (Figure 3(c) and (d)). Radial MRI showed no viable sector at ~90° (Figure 3(e)) but anteromedial viability at 120°–130° (Figure 3(f)). HDPRO 130° (varus 10°) was performed. Operative time was 89 min; blood loss was 400 mL (Figure 3(g)). Healthy occupancy was 53% (Figure 3(h)); scintigraphy was positive at 1 month (Figure 3(i)). Full loading at 6 months (Figure 3(j)); rapid return to road cycling (Table 2). At 1 year after surgery, he had no pain at all (Figure 3(k)). Hardware removal was performed at 15 months after surgery, and the patient entered a road cycling vocational school at 2 years after surgery (Figure 3(l)). At 2 years after surgery, his JHEQ score was good at 82 points. Two years postoperatively, the radiographic LLD was 11 mm (Figure 3(m)), but there was no perceived LLD (Table 3).
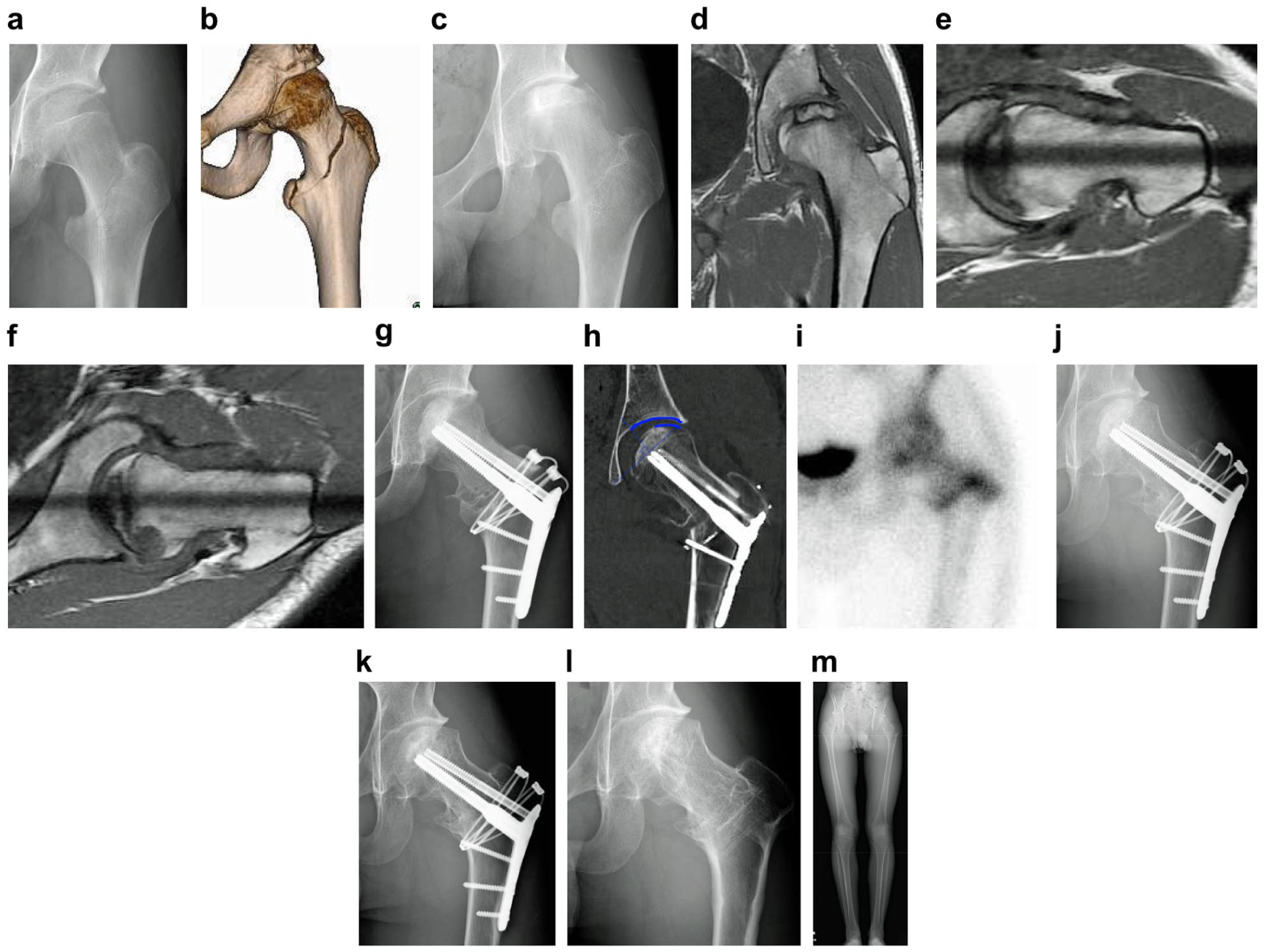
(a) Delbet–Colonna type IV injury sustained in a traffic accident between bicyclists. (b) Three-dimensional computed tomography image at the time of injury. A trochanteric fracture line was observed. (c) Crushing of the femoral head was seen at the time of the initial examination at our hospital. (d) Magnetic resonance imaging revealed type C2, stage IIIb according to the Japanese Investigation Committee Classification. (e) Radial magnetic resonance imaging 90°, Lauenstein view. No healthy areas were seen anteriorly or posteriorly. (f) Radial magnetic resonance imaging 130°, Lauenstein view. A healthy area was seen anteriorly. (g) 130° Posterior rotational osteotomy, Varus 10°. Operation time was 89 min, and blood loss was 400 mL. (h) The healthy area occupancy rate is 53%. (i) 99mTc bone scintigraphy shows accumulation and good blood flow. (j) At 6 months after surgery, full load-bearing was permitted, and the patient returned to road cycling. (k) No pain at 1 year after surgery. (l) At 2 years after surgery, the patient has advanced to the next stage of education and is enjoying road cycling. (m) Leg length difference at 2 years after surgery was 11 mm, but there was no subjective leg length difference.
Discussion
Femoral neck fractures are rare and account for <1% of all pediatric fractures, with many reports indicating complications. 11 Complications include AVN, valgus deformity, pseudarthrosis, and LLD,12–14 with AVN occurring in 25%–45% of patients and having the most detrimental clinical outcomes.11,13 Compared to symptomatic ONFH, AVN after PFNF has a greater extent of necrosis,11,15 and the femoral head may decay more rapidly. Xin et al. 15 conclude that the presence of hip pain symptoms and the degree of JIC classification are two risk factors for collapse progression. AVN prognosis after PFNF was poor, with only 11.6% of the 147 patients (17/147) having a satisfactory final prognosis and 88.4% (130/147) having an unsatisfactory prognosis. 15 Extensive research has been conducted to avoid AVN as much as possible, and risk factors for AVN include Delbet fracture type, 16 waiting time from injury to surgery,14,17 initial dislocation of the fracture,13,18 degree of anatomic repair,13,17 and age,13,16 among others. 16 In all three cases, surgery was performed within 24 hours of the injury, good reduction was achieved, and in the third case, the patient had Delbet IV, which is said to occur in only 5% of cases. We believe that it is crucial to deal with AVN, which occurs after PFNF.
Regarding conservative therapy, Maeda et al. 19 recommended a period of at least 1 year of none-weight Bearing (NWB) to avoid severe depression of the femoral head based on biopsy results for AVN after PFNF. However, in patients with mild dislocation, specimens obtained >1 year after the injury are not fully repaired, and the required duration of NWB is unknown. Although the efficacy of bisphosphonates in the early stages before crushing has been noted,20,21 once crushing has occurred, administration is ineffective. In addition, bone-preserving surgery after crushing causes instability due to deformity of the bone head, which leads to progressive deformity and poor postoperative results in younger patients, even though remodeling is more likely to occur.
Currently, there are case reports of joint-preserving surgery for AVN after PFNF, including core decompression (CD), 22 magnesium (Mg) screw-fixed pedicle iliac bone flap, 23 and valgus osteotomy 12 modified TRO 24 ; however, there is no consensus on surgical treatment. Furthermore, while joint fusion or joint replacement exists as a last resort, they hesitate when considering the long life that will follow. Regarding CD, AVN after PFNF has a large extent of necrosis, 15 and CD alone should be reserved for cases with a large extent of necrosis. 22 It has also been reported that the likelihood of returning to preoperative physical function and running activities with CD alone is as low as 13.7%. 25 Regarding valgus intertrochanteric osteotomy (VITO), it has been found by finite element modeling of the proximal femur that the anterolateral part of the femoral head has the most weight-bearing in the standing position, 26 and theoretically, VITO is not suitable because it externalizes the necrotic area to bear the greatest weight. 12 Although it is effective for pseudoarthrosis, the results of its adaptation to AVN are poor. 12 Total hip arthroplasty (THA) improves hip function, reduces pain, and improves quality of life in all patients. However, THA is generally avoided in teenage patients. Overall, reoperation rates are high, primarily due to aseptic loosening. 27 Although the revision rate tends to decline with the advent of highly cross-linked polyethylene, even the short-term results of 5.2% with an average follow-up of 5.8 years are not comparable to the results for regular osteoarthritis, and the indication for THA should be a cautious last resort. 28
TRO was developed by Sugioka, with good results of ONFH being reported.1,29 As a rule, the rotation was limited to 90°. Atsumi et al.5–7 performed angiography and reported good results with a posterior rotation of more than 100° and less than 150° after PRO by loosening the posterior column artery, which they termed HDPRO. We reported good HDPRO results, especially for patients with ONFH, which occurs for numerous reasons in teenagers with vigorous remodeling. 8 HDPRO is a procedure that moves the healthy anteromedial lower portion of the femoral head to the weight-bearing area. In all three cases of this report, radial MRI images (Figures 1(e), 2(e), and 3(e)), which correspond to the 90° Lauenstein view of the preoperative plan, revealed no healthy areas anteriorly and posteriorly, and the original TRO method was not suitable. MRI for HDPRO (Figures 1(f), 2(f), and 3(f)) with the hip in 120° flexion and 45° abduction showed a healthy area on the anteromedial part of the femoral head. In the three cases presented here, the surgery to move that healthy part to the loading area was performed as preoperatively planned using navigation, and good results were obtained.
After HDPRO, the femoral head is rotated as a whole, including the previously collapsed segment. Therefore, some degree of postoperative morphological incongruity or early osteoarthritic change is considered a realistic consequence of joint-preserving surgery for advanced post-traumatic AVN, especially in older adolescents.
Although increasing varus correction may theoretically improve femoral head coverage, excessive varus inevitably results in increased LLD, which negatively affects gait and patient satisfaction. Thus, in the present series, varus correction was intentionally limited once a postoperative healthy area occupancy of at least 40% was achieved, which is a threshold previously associated with favorable outcomes. This strategy represents a deliberate balance between joint congruity and functional outcome. Thus, mild radiographic asymmetry may be observed, but no progressive collapse, joint space narrowing, or clinical instability was detected during follow-up.
Abbas et al. 24 reported good results in three patients with AVN after PFNF who underwent a modified TRO without transverse dissection to prevent the TRO complication of pseudarthrosis of the greater trochanter. Rotation of 90° or less is possible without a greater trochanterectomy, but backward rotation of 130° is not possible without a greater trochanterectomy.
The arteries feeding the femoral head are the superior retinacular artery (SRA) and inferior retinacular artery (IRA), which are branches of the medial femoral circumflex artery, the artery of ligamentum teres, which branches from the obturator artery, and the anterior retinacular artery (ARA), a branch of the lateral femoral circumflex artery (LFCA). These arteries enter the femoral head and then form the main trunk of the epiphyseal artery and metaphyseal artery, which anastomose with each other to form the epiphyseal artery network. 30 AVN after PFNF occurs due to the insufficient blood supply to the SRA that feeds the weight-bearing area. In the superolateral region of the femoral head, there are fewer secondary anastomoses and arterial arches than in other regions. Therefore, compromised perfusion of the SRA-dominant retinacular system can readily lead to perfusion disturbance. Conversely, the anterior part of the femoral head near the center of the epiphyseal artery network shows more anastomoses, and the ARA and IRA complement each other. 30 Traditionally, the LFCA was thought not to be significantly involved in blood flow to the femoral head; however, recent reports have shown that it does supply blood flow to the anterior neck of the femoral head,31,32 albeit to a limited extent. Dewar et al. 31 reported that the largest contribution (48%) of LFCA to the femoral head is the supply of blood flow to the anterior inferior part of the femoral neck by the ARA. Moreover, even if the ARA is damaged, blood flow is often supplied by the IRA, which has a complementary relationship with the ARA, and blood flow in the lower anterior hip is easily maintained. Lazaro et al. 33 report that the ARA nourishes the femoral head at 74°–116°, while the IRA nourishes the femoral head at 185°–219°, and more importantly, the IRA is located 1.6 mm away from the femoral neck and is less likely to be damaged during fracture.30,33 Thus, the anterior inferior portion of the femoral head is often preserved even in AVN following PFNF, where necrosis is said to be more extensive than in symptomatic ONFH. By rotating this healthy part backward by 130° on the cervical axis, the femoral head anterior to the weight-bearing area forms healthy, viable bone. Therefore, HDPRO is considered the optimal surgical treatment for AVN, which is a devastating complication of PFNF. In all three cases reported here, although achieving a sufficiently healthy range of motion with rotation up to 90° was difficult, the lower anteromedial portion of the femoral head survived, and good results could be obtained by moving the same portion to the weight-bearing area.
In recent years, there have been numerous reports of reduced operative time and less blood loss in THA 34 and pelvic osteotomy 35 using CAS. It has been reported that 3D navigation-assisted pelvic and femoral osteotomies for pediatric developmental dysplasia of the hip shorten the operative time, reduce intraoperative blood loss and X-ray exposure, and demonstrate therapeutic effectiveness. It has also been reported that 3D navigation-assisted hip osteotomy might be clinically superior to conventional osteotomies in terms of postoperative outcomes. 36 The use of the navigation system in this study also allowed us to reproduce the precise osteotomy as planned preoperatively, and the postoperative internal and external rotation was maintained within the normal range of motion, with good enough results to allow the patient to return to sports as soon as possible after surgery (Table 2). Details on HDPRO using navigation are described in another paper. 9
Limitations
This study acknowledges the limitations of a small sample size and retrospective design. To validate the findings, future studies with larger cohorts and prospective data collection are recommended. Currently, it is impossible to trace the central bone fragment where osteotomy was performed, and the angle of rotation and the varus anteversion angle may differ slightly from the preoperative plan. We look forward to further development of the navigation technology.
Long-term follow-up is required to determine whether subtle postoperative morphological incongruity may lead to degenerative osteoarthritis over time, specifically in older adolescents.
Conclusions
This report provides preliminary evidence suggesting the potential effectiveness of HDPRO as a bone-preserving procedure for AVN, which is the poorest prognostic complication after PFNF surgery. This is the first example of the effectiveness of HDPRO surgery with a navigation system in moving the anteromedial portion of the femoral head to the weight-bearing area as preoperatively planned, which is relatively easy to preserve even in AVN after PFNF. The use of navigation has the potential to standardize surgical procedures and significantly improve patient outcomes. Future research should focus on expanding the sample size, conducting prospective controlled studies, and evaluating long-term functional and radiographic outcomes to confirm the effectiveness and safety of this technique.
Supplemental Material
sj-pdf-1-cho-10.1177_18632521261417847 – Supplemental material for 3D-guided high-degree posterior rotational osteotomy for avascular necrosis in pediatric femoral neck fractures: A three-case study
Supplemental material, sj-pdf-1-cho-10.1177_18632521261417847 for 3D-guided high-degree posterior rotational osteotomy for avascular necrosis in pediatric femoral neck fractures: A three-case study by Minoru Watanabe, Satoshi Kagaya, Daichi Kuzushima and Itaru Kachi in Journal of Children's Orthopaedics
Supplemental Material
sj-tif-2-cho-10.1177_18632521261417847 – Supplemental material for 3D-guided high-degree posterior rotational osteotomy for avascular necrosis in pediatric femoral neck fractures: A three-case study
Supplemental material, sj-tif-2-cho-10.1177_18632521261417847 for 3D-guided high-degree posterior rotational osteotomy for avascular necrosis in pediatric femoral neck fractures: A three-case study by Minoru Watanabe, Satoshi Kagaya, Daichi Kuzushima and Itaru Kachi in Journal of Children's Orthopaedics
Footnotes
Author contributions
MW conceived and designed the analysis and wrote the paper. DK was responsible for data collection. SK contributed data and analysis tools. IK performed the analysis. All authors read and approved the final manuscript.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethics approval
This study was conducted in accordance with the ethical principles outlined in the Declaration of Helsinki (2013), developed by the World Medical Association. As this is a case report involving three patients, the Ethics Committee of Showa University determined that an ethical review was not required.
Consent to participate
Written informed consent was obtained from both the patient, who is a minor, and their guardian.
Consent for publication
We confirm that written informed consent for publication has been obtained from all individuals (or their parents/legal guardians in the case of minors) whose data, images, or videos are included in this manuscript.
Data availability statement
The datasets supporting the conclusions of this article are included within the article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.