
Abstract
Background:
Adolescent idiopathic scoliosis (AIS) develops between the ages of 10 and skeletal maturity and can lead to physical, psychosocial, and medical complications if untreated. Posterior spinal fusion (PSF) is the primary surgical intervention when bracing fails. Although sociodemographic factors affect access to care, surgical candidacy, perioperative risk, and recovery, these variables are rarely reported in randomized controlled trials (RCTs), limiting assessment of equity and generalizability in AIS outcomes.
Methods:
Following Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines, PubMed, Embase, and Scopus were searched on 9 April 2024, using “posterior spinal fusion,” “randomized controlled trial,” and “adolescent idiopathic scoliosis.” Inclusion criteria were full-text RCTs on PSF in AIS; exclusions were non-English publications, cadaver studies, and technique articles. Two authors independently screened studies, with disagreements resolved by a third. Extracted variables included demographics and social factors. Analyses used descriptive statistics, chi-squared tests, and Fisher’s exact test (p < 0.05).
Results:
Of 148 studies, 44 met the inclusion criteria. Age (97.7%) and sex (95.5%) were reported more frequently than race (6.8%) or ethnicity (9.1%) (p < 0.001). No studies reported household income, insurance status, housing, employment, or education. Reporting did not differ by journal (Fisher’s exact test, p = 0.999) or publication year (chi-squared test, p = 0.185), although reporting increased slightly after 2017.
Conclusions:
RCTs on PSF for AIS rarely report sociodemographic variables beyond age and sex. This gap limits understanding of whether outcomes are consistent across populations or if disparities exist in treatment response or recovery. Improved sociodemographic reporting is essential for transparency, external validity, and equity in AIS care.
Level of Evidence:
Systematic review of Level II.
Keywords
Introduction
Adolescent idiopathic scoliosis (AIS) is the most common form of scoliosis in adolescents, with an incidence of 0.47%–5.2%, and may require posterior spinal fusion (PSF) for progressive curves exceeding surgical thresholds.1–4 Although PSF is an effective and well-established treatment, access to timely diagnosis, surgical evaluation, and postoperative recovery can be strongly influenced by sociodemographic factors such as race, insurance coverage, and socioeconomic status. 5 These determinants not only shape who receives surgical care but also affect perioperative risks, complication rates, and long-term outcomes. 6 Despite this relevance, sociodemographic characteristics remain inconsistently reported in randomized controlled trials (RCTs), limiting assessment of whether current evidence reflects the populations most affected by AIS.
Disparities in evaluation and perioperative care have been documented across orthopedic subspecialties, including PSF, yet the factors underlying these inequities cannot be adequately assessed when reporting is incomplete.5–9 Sociodemographic variables encompass both demographic characteristics (age, sex, race, ethnicity) and socioeconomic indicators (insurance status, education, income, and housing stability). However, prior work has demonstrated that these variables are frequently underreported in randomized trials across medicine and surgery.10–14 Without their consistent inclusion, it is difficult to determine whether published RCT outcomes are equitable, generalizable, or representative of the broader AIS population.
RCTs are considered the highest level of evidence for evaluating treatment effectiveness; however, when key sociodemographic characteristics are not collected or reported, important effect modifiers may be obscured. Because these variables can influence both access to surgery and postoperative outcomes, underreporting limits the ability to assess confounding, stratify risk, and determine whether findings are externally valid across diverse patient populations. Accordingly, the purpose of this study is to determine the rate of sociodemographic reporting in RCTs investigating PSF for AIS. We hypothesized that these trials would significantly under-report sociodemographic variables.
Methods
Literature review
This study was conducted according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines (Supplemental A). The databases PubMed, Embase, and Scopus were searched for the terms “posterior spinal fusion,” “randomized controlled trial,” and “adolescent idiopathic scoliosis” on 9 April 2024. Inclusion criteria were RCTs investigating PSF in adolescents with idiopathic scoliosis published in English with an accessible full text. Exclusion criteria were studies not published in English, studies that did not have the full-text available, cadaver studies, technique articles, and study designs other than RCTs. Studies were screened for inclusion by two authors. Any disagreement was resolved by a third author.
Data collection
The title, journal, and year of publication for each article were recorded. Demographic variables, such as sex or gender, race, ethnicity, and age, and socioeconomic variables such as insurance status, income/Childhood Opportunity Index (COI), a surrogate for socioeconomic status, housing status, familial work status, and familial level of education were collected. Two authors thoroughly reviewed each manuscript to determine which variables were included in the paper. The information was collected in a binary manner, categorizing whether each variable was present or absent as either “yes” or “no,” respectively. Data are available from the authors upon reasonable request.
Statistical analysis
Data were analyzed using descriptive statistics. Chi-squared tests were used to compare the reporting frequency of sociodemographic variables (e.g., age/sex vs. race/ethnicity) and to evaluate differences across journals. Fisher’s exact test was used for comparisons across time intervals (pre-2017 vs. post-2017), where cell sizes were small. A p-value <0.05 was considered statistically significant.
Results
The initial database search identified 148 studies, of which 64 duplicates were removed. An additional 32 studies were removed after title and abstract screening because they did not meet the inclusion criteria. The full text of the remaining 52 studies was assessed for eligibility. Of the 52 studies, 8 studies were excluded because they did not have a full text. In all, 44 RCTs were selected for inclusion (Figure 1).
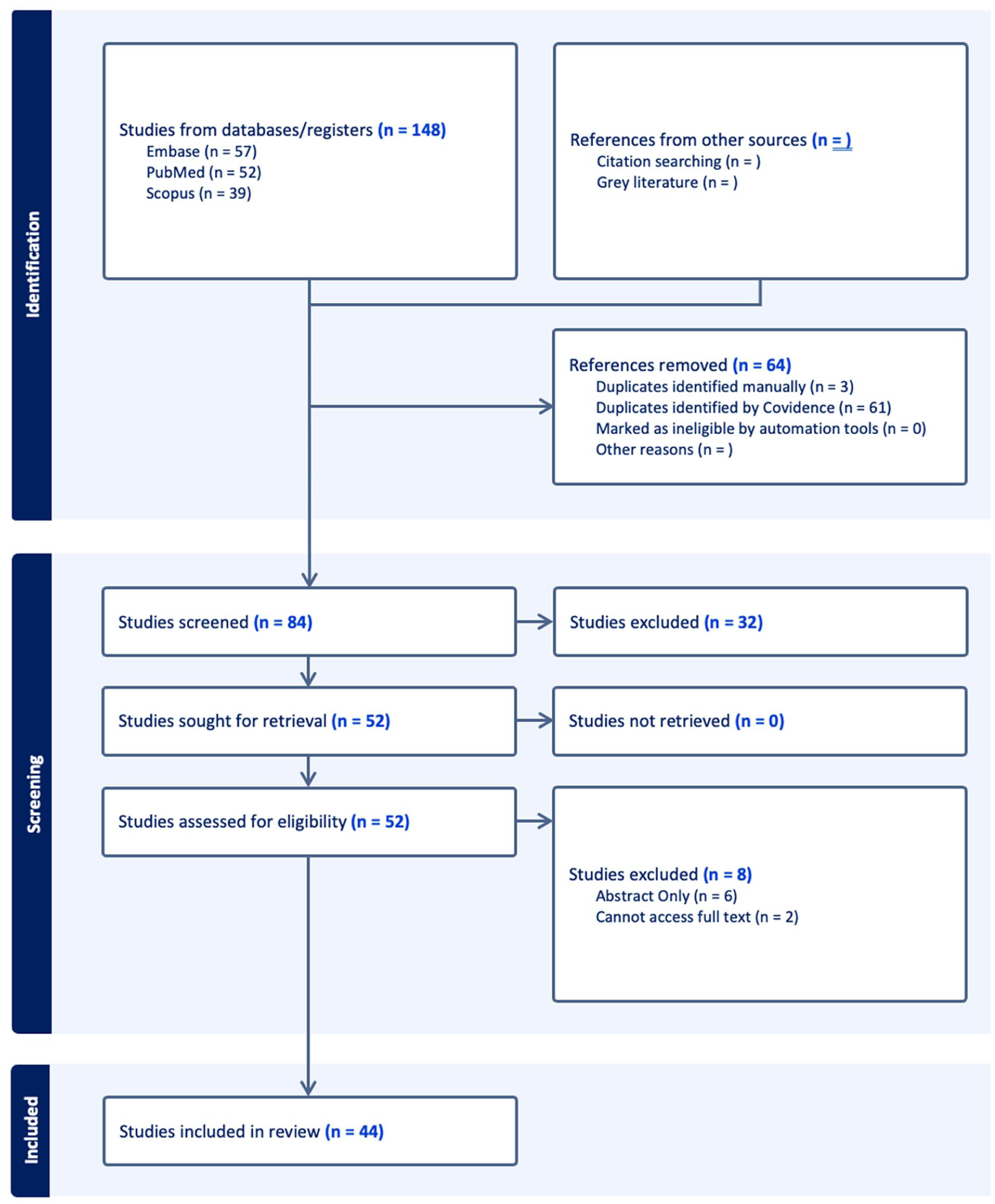
Study selection process following the PRISMA framework.
The included RCTs were published in 19 journals from 1988 to 2024.15–58 The age of study participants was reported in 43 out of the 44 total studies (97.7%). Sex or gender was reported in 42 of 44 (95.5%) studies. With respect to other sociodemographic variable reporting, race was included in 3 of 44 (6.8%) studies, and ethnicity in 4 of 44 (9.1%) studies. However, familial income/COI, familial work status, familial level of education, insurance status, and housing status were not mentioned in any study (0/44, 0.0%; Table 1). Age and sex/gender were reported significantly more frequently than race or ethnicity (p < 0.001).
Variable inclusion in pediatric posterior spinal fusion randomized controlled trials.
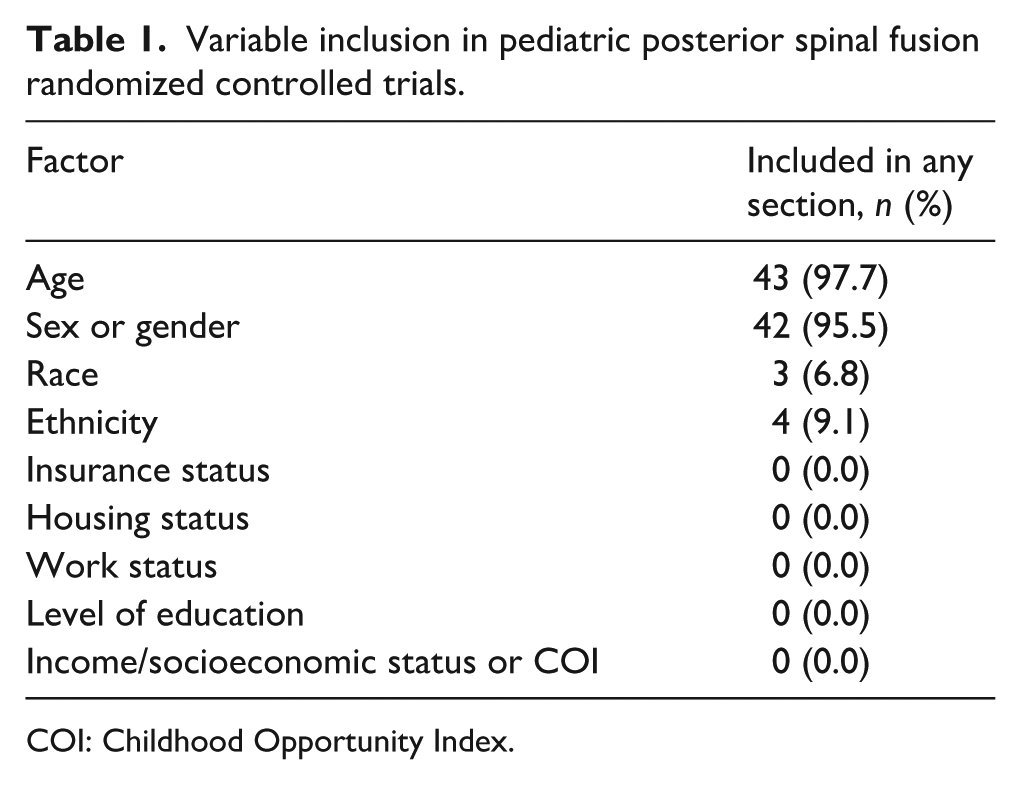
COI: Childhood Opportunity Index.
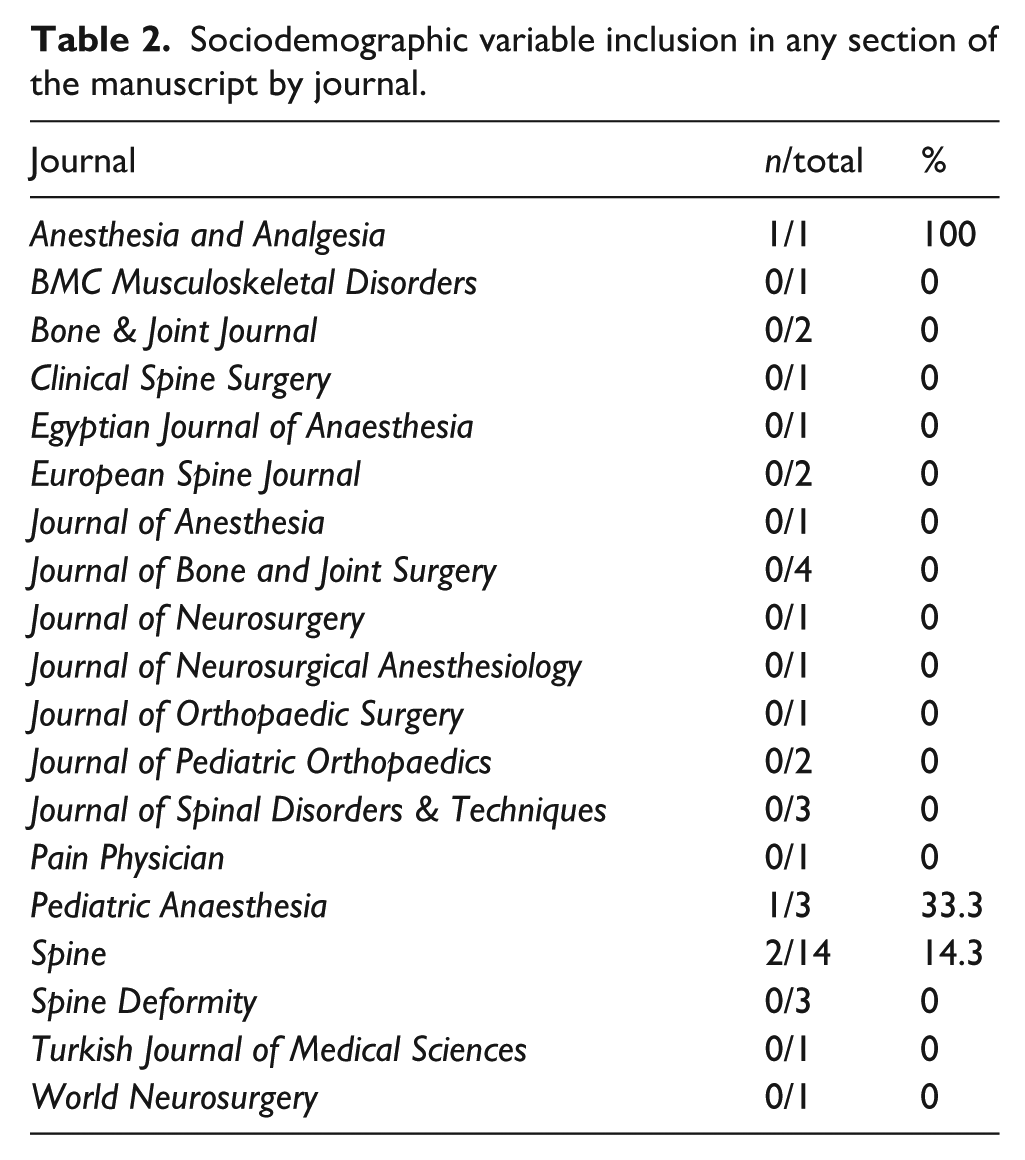
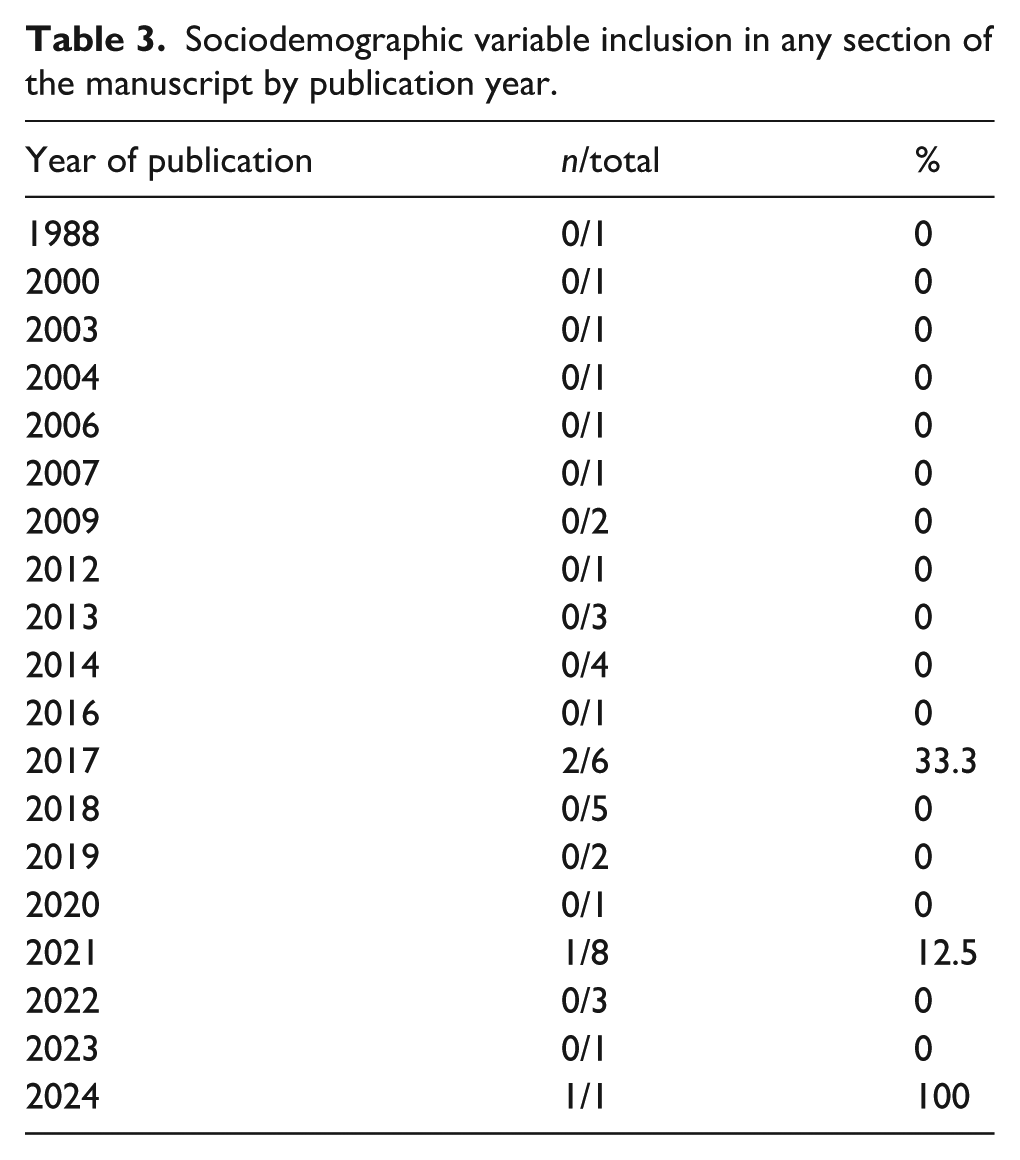
There was no significant difference in reporting of any sociodemographic variables among included journals (p = 0.999) or by year of publication (p = 0.185) (Tables 2 and 3). No studies before 2017 reported any sociodemographic variable (0/17, 0%), whereas multiple studies published since 2017 have done so (4/27, 14.8%).
Sociodemographic variable inclusion in any section of the manuscript by journal.
Sociodemographic variable inclusion in any section of the manuscript by publication year.
Discussion
This review addresses a critical gap in the orthopedic literature: the limited reporting of sociodemographic variables in AIS RCTs, which restricts the ability to evaluate whether surgical outcomes are equitable or generalizable across patient populations. Without these data, key effect modifiers related to access to care, baseline risk, and postoperative recovery cannot be assessed, diminishing both interpretability and external validity. Our findings show that although age and sex were consistently reported, socioeconomic indicators, such as insurance status, income, and education, were almost never included, and race and ethnicity were reported only intermittently in more recent trials. This pattern reflects a persistent disconnect between the known influence of social determinants of health and the variables captured within high-level surgical evidence.
As previously mentioned, age and sex were commonly reported in 97.7% and 95.5% of included studies, respectively, thus reflecting their importance in treating AIS. Many studies have reported higher incidence rates for AIS in females and greater initial curve angles compared to males (18.1° vs. 16.7°). 59 Bondar et al.’s 59 retrospective analysis found the highest AIS incidence among 13-year-old girls (958 per 100,000 per year). Helenius et al. 60 found similar preoperative Cobb angles between males and females (55° vs. 56°) but greater postoperative curve correction in females (p = 0.027). Collis et al. 61 likewise showed sex-based differences in early postoperative recovery, with females reporting higher Visual Analog Scale pain scores (5.0 vs. 3.6, p < 0.0001) and greater opioid use (42.2 mg vs. 31.5 mg, p = 0.01). In both studies, females were also slightly younger at the time of surgery (mean age 15.5–14.2 years vs. 16.2–14.7 years for males).59–61 Because these differences are well recognized, age and sex are already viewed as clinically relevant moderators of surgical outcomes, which explains their near-universal reporting in RCTs. However, the fact that only these two variables are reported, while other potential effect modifiers such as insurance status, socioeconomic environment, and educational background are entirely omitted, illustrates a selective recognition of which patient factors are considered clinically meaningful. This selective reporting is precisely the gap identified in this review: sociodemographic variables beyond age and sex remain overlooked despite having similar potential to influence outcomes.
Race and ethnicity have been documented to play a role in contributing to worse care outcomes in underrepresented populations, but they have been relatively under-reported compared to age and sex in the literature concerning AIS. 62 Among the RCTs included in our review, only three reported race and four reported ethnicity, and none provided stratified outcomes or adjusted analyses, mirroring broader trends in orthopedics where fewer than 6% of RCTs report race and fewer than 2% report ethnicity. 7 Bondar et al. 59 reported that White and African American patients had significantly higher initial curve magnitudes compared to Hispanic patients (p < 0.001 and p < 0.004, respectively) while also demonstrating a lower incidence rate of AIS among African American children. However, they also reported a higher risk of more severe curvature in African American children. Erkkila et al. 63 similarly demonstrated that patients who identified as Black/African American were 2.3 times more likely to present with severe scoliosis than patients who identified as White. Kaushal et al. 64 conducted a retrospective review to identify the differences in blood loss in patients undergoing PSF between African-American and Caucasian patients. Notably, the authors observed lower preoperative hemoglobin levels in African American patients. In a retrospective study, Elsamadicy et al. reported significantly higher levels of blood transfusion among Black patients (25%) compared to patients in the White (16.7%), Hispanic (24.5%), or other cohorts (22.7%), which could be related to the low hemoglobin levels among Black patients as reported by Kaushal et al.64,65 Furthermore, Alomari et al. 66 noted a greater likelihood of preoperative respiratory and cardiac risk factors, along with increased preoperative steroid use, in the Black cohort compared to the White cohort. Of note, it is important to note the impact of race and ethnicity on the financial implications of surgery. Elsamadicy et al. 65 reported the highest cost of admission among their Hispanic patient cohort compared to White, Black, or Other (p < 0.001). These disparities parallel randomized orthopedic evidence demonstrating that sociodemographic variables—including race, income, and education—can exert greater influence on postoperative pain, satisfaction, and functional recovery than surgical or implant-related factors, and subgroup analyses in spine RCTs are often not feasible precisely because these variables are not consistently reported.8,9 These findings support the importance of considering race and ethnicity in assessing preoperative risk factors and improving preoperative care.
Insurance status has been shown to affect treatment access and care pathways for AIS in retrospective cohorts. Thornley et al. 67 reported that publicly insured Black patients were less likely to seek second opinions and receive bracing (p = 0.004 and p < 0.001). Orellana et al. 68 similarly demonstrated a strong association between insurance type, race, and socioeconomic disadvantage, with underrepresented minority patients more frequently holding public insurance and residing in lower COI neighborhoods (46% vs. 13%, p < 0.001). These studies illustrate how socioeconomic factors influence clinical presentation and treatment trajectories in AIS; however, such disparities cannot currently be evaluated within RCTs because insurance status, income, and neighborhood-level proxies like COI are not reported in the randomized literature. This disconnect underscores the central finding of this review: the highest level of evidence in AIS surgery omits key sociodemographic variables that have already been shown in observational studies to affect access and outcomes.
Education status is another important sociodemographic variable that affects patient outcomes. Berg et al. 69 sought to observe the readability of medical resources concerning PSF in treating pediatric scoliosis. They reported a mean reading grade level of 11.6 ± 2.3 for websites containing information regarding PSF, which may affect patients’ understanding of treatment and the quality of care they receive. This idea was backed by a retrospective study by Yang et al., 70 revealing fewer mean days (5.6 vs. 8.9, p < 0.001) and doses of oxycodone (14 vs. 23, p < 0.001) used, along with fewer opioid refills in patients who received preoperative education on prescription and opioid use post-PSF for AIS, compared to those who did not. These findings indicate that educational environment and health literacy can directly influence recovery quality and complication risk, suggesting that education level may act as a clinically relevant effect modifier. However, because no RCTs in this review reported patient or caregiver education level, its impact cannot currently be assessed within the randomized evidence base.
This systematic review has several limitations. First, limiting inclusion to English-language publications may have introduced language-based publication bias; RCTs published in non-English journals may differ in their sociodemographic reporting practices, which could lead to an underestimation of global reporting trends. Moreover, the binary (“yes/no”) coding of sociodemographic reporting does not capture the level of detail or analytic use of these variables. While this study identified the presence of sociodemographic variables in its analysis of RCTs, it did not provide detailed quantitative or qualitative data for each variable, such as the total number of patients, the mean age of patients, and the percentage of each sex among the patients, which could have enriched the study. In addition, while composite socioeconomic scores such as the Concentrated Disadvantage Index and the COI are emerging, it remains unclear which is most useful. Future studies should explore the utility and applicability of these indices to better assess sociodemographic factors and improve the generalizability of findings. Finally, excluding non-English studies may have resulted in underreporting of sociodemographic variables.
Conclusion
RCTs on PSF for AIS rarely report sociodemographic variables beyond age and sex. This omission limits the ability to determine whether outcomes are consistent across patient populations or whether disparities exist in treatment response, perioperative risk, or recovery. Improved sociodemographic reporting is therefore not only a matter of transparency but a prerequisite for assessing external validity and equity in AIS care.
Supplemental Material
sj-docx-2-cho-10.1177_18632521251411158 – Supplemental material for Sociodemographic variables are rarely reported in randomized controlled trials investigating posterior spinal fusion for adolescent idiopathic scoliosis: A systematic review
Supplemental material, sj-docx-2-cho-10.1177_18632521251411158 for Sociodemographic variables are rarely reported in randomized controlled trials investigating posterior spinal fusion for adolescent idiopathic scoliosis: A systematic review by Erin L Brown, Kenneth T Nguyen, Bhavesh R Koppala, Daman P Dhunna, Alexander Kuzma and Nikolas Baksh in Journal of Children's Orthopaedics
Supplemental Material
sj-pdf-1-cho-10.1177_18632521251411158 – Supplemental material for Sociodemographic variables are rarely reported in randomized controlled trials investigating posterior spinal fusion for adolescent idiopathic scoliosis: A systematic review
Supplemental material, sj-pdf-1-cho-10.1177_18632521251411158 for Sociodemographic variables are rarely reported in randomized controlled trials investigating posterior spinal fusion for adolescent idiopathic scoliosis: A systematic review by Erin L Brown, Kenneth T Nguyen, Bhavesh R Koppala, Daman P Dhunna, Alexander Kuzma and Nikolas Baksh in Journal of Children's Orthopaedics
Footnotes
Author contributions
Erin L. Brown: Corresponding author, data analysis, study conception and design, manuscript drafting.
Kenneth T. Nguyen: Data analysis, data extraction, manuscript drafting, literature search.
Bhavesh R. Koppala: Data collection, manuscript revisions, verification of extracted data.
Daman P. Dhunna: Critical review of manuscript, data interpretation, manuscript editing.
Alexander Kuzma: Critical revisions of manuscript for important intellectual content, study supervision.
Nikolas Baksh: Critical revisions of manuscript for important intellectual content, study supervision.
All authors read and approved the final manuscript.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical statement
This study is a systematic review of previously published data and did not involve new human or animal participants. Therefore, institutional review board approval and informed consent were not required.
Data availability statement
This study is a systematic review. All data analyzed in this article are drawn from previously published studies, which are cited in the reference list. No new datasets were generated or analyzed.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.