
Abstract
Purpose:
To identify clinical and radiographic risk factors associated with hip redislocation in children with cerebral palsy (CP) who underwent surgical treatment for hip dislocation.
Methods:
This multicenter retrospective study included children with CP who underwent reconstructive osteotomy for hip dislocation and were followed until triradiate cartilage closure. Demographic, clinical, and radiographic variables were evaluated. Univariate and multivariate logistic regression analyses were performed to identify independent risk factors for redislocation. Additionally, a classification and regression tree (CART) model was developed to stratify redislocation risk.
Results:
Hip redislocation occurred in 25 of 115 hips (21.7%). Redislocation was significantly more frequent in hips treated with femoral osteotomy alone (40%) compared to combined femoral and pelvic osteotomies (16.7%), (p = 0.026). Multivariate analysis identified younger age at surgery (Odds ratio (OR) = 0.981, p = 0.010), higher postoperative Sharp’s angle (OR = 1.082, p = 0.034), and lower postoperative Mose hip ratio (MHR) (OR = 0.007, p = 0.033) as independent predictors of redislocation. Radiographic ratios, including medial joint space to cranial joint space (MJS/CJS) and MJS to maximum capital femoral epiphysis diameter (MJS/MCFED), were also significantly higher in redislocated hips. The CART model classified patients into high- and low-risk groups based on surgical age ≤76 months, postoperative Sharp’s angle ≥48°, and MHR < 0.69.
Conclusions:
Younger surgical age, insufficient correction as indicated by a higher postoperative Sharp angle and lower MHR were independently associated with hip redislocation in CP patients undergoing surgery. MJS/CJS and MJS/MCFED ratios were also associated with redislocation, indicating incomplete reduction.
Significance of study:
This study presents a clinically applicable decision-tree model to predict redislocation risk after CP hip reconstruction using radiographic parameters.
Level of evidence:
Level III, multicenter retrospective study.
Keywords
Introduction
Cerebral palsy (CP) is the most common cause of physical disability in childhood, with a prevalence of approximately 2 per 1000 live births.1,2 Among the various orthopedic manifestations of CP, hip displacement is one of the most clinically significant and commonly observed problems, particularly in nonambulatory children.3,4 Hip displacement can progress gradually and lead to subluxation or dislocation, resulting in pain, impaired sitting, difficulty with perineal hygiene, and reduced quality of life.5,6
The risk of hip displacement in CP is multifactorial and has been linked to the Gross Motor Function Classification System (GMFCS) level, spasticity, muscle imbalance, and growth.3,7,8 While early detection through surveillance and timely surgical intervention have reduced the incidence of dislocation, treatment remains primarily surgical once the hip is dislocated.9,10 Despite surgical treatment, hip redislocation may still occur during growth and skeletal maturation, making hip displacement a persistent challenge in the long-term management of children with CP. However, most previous studies have reported short- to mid-term outcomes or limited follow-up, leaving uncertainty regarding the long-term stability of the hip, particularly through skeletal maturity.11–13
To address this gap, a multicenter study was conducted involving children with CP who underwent surgical treatment with osteotomy for hip displacement and were followed until triradiate cartilage closure. The primary aim was to identify clinical and radiographic risk factors associated with hip redislocation following surgical intervention in this population.
Methods
This multicenter retrospective study was conducted through the national pediatric orthopedic neuromuscular study group, including 15 orthopedic surgeons from 10 specialized centers. The study population consisted of children with CP who underwent reconstructive osteotomy for displacement and were followed until the closure of the triradiate cartilage.
Patients were included if they had a diagnosis of CP with grade IV or V hip displacement according to the Melbourne Cerebral Palsy Hip Classification System14,15 had undergone bony surgery while the triradiate cartilage was open, had follow-up data through triradiate closure, and had available preoperative, early postoperative, and final anteroposterior (AP) pelvic radiographs.14,15
Exclusion criteria included having undergone only soft tissue procedures (e.g. adductor or psoas release), prior bony surgery on the hip, presence of flaccid or hypotonic neurological involvement, or coexisting developmental dysplasia of the hip, particularly in cases where the hip dislocation was identified in the neonatal period or within the first year of life.
For each included patient, demographic and clinical data were collected, including demographics, age at surgery, GMFCS level, and history of previous hip interventions. In cases with pelvic obliquity, the side of the high-riding hip was noted. Surgical details such as the location of osteotomies (isolated femoral varus derotation osteotomy [FO] or combined femoral and pelvic osteotomies [FPO]), the surgical technique used, whether open reduction or additional soft tissue procedures were performed, were recorded.
In all centers, FO was performed with varization typically ranging from 20° to 40°, derotation of 10°–30°, and femoral shortening up to 1.5 cm when necessary to achieve concentric reduction. The type of pelvic osteotomy was selected according to acetabular morphology and surgeon preference, most commonly using Dega-type or Pemberton osteotomies.
If hip redislocation occurred during follow-up, the time of redislocation and any subsequent procedures was documented. Analyses were performed on a per-hip basis. In cases with bilateral reconstructive osteotomies, each hip was evaluated separately.
Radiographic evaluation was performed using standardized AP radiographs. The following measurements were assessed: migration index (MI), pelvic obliquity, Tönnis angle, Sharp’s angle, medial joint space (MJS), cranial joint space (CJS), Mose hip ratio (MHR), and maximum capital femoral epiphysis diameter (MCFED).16–20 Ratios such as MJS/CJS and MJS/MCFED were also calculated, Figure 1. The presence or absence of hip redislocation was determined on the final radiograph obtained after triradiate closure. Hip redislocation was defined as a MI greater than 60% on follow-up radiographs.4,21,22 This threshold was selected as a practical indicator of substantial loss of reduction, representing a stage of severe subluxation before complete dislocation, in line with definitions commonly applied in previous literature, although no uniform consensus currently exists.4,21,22
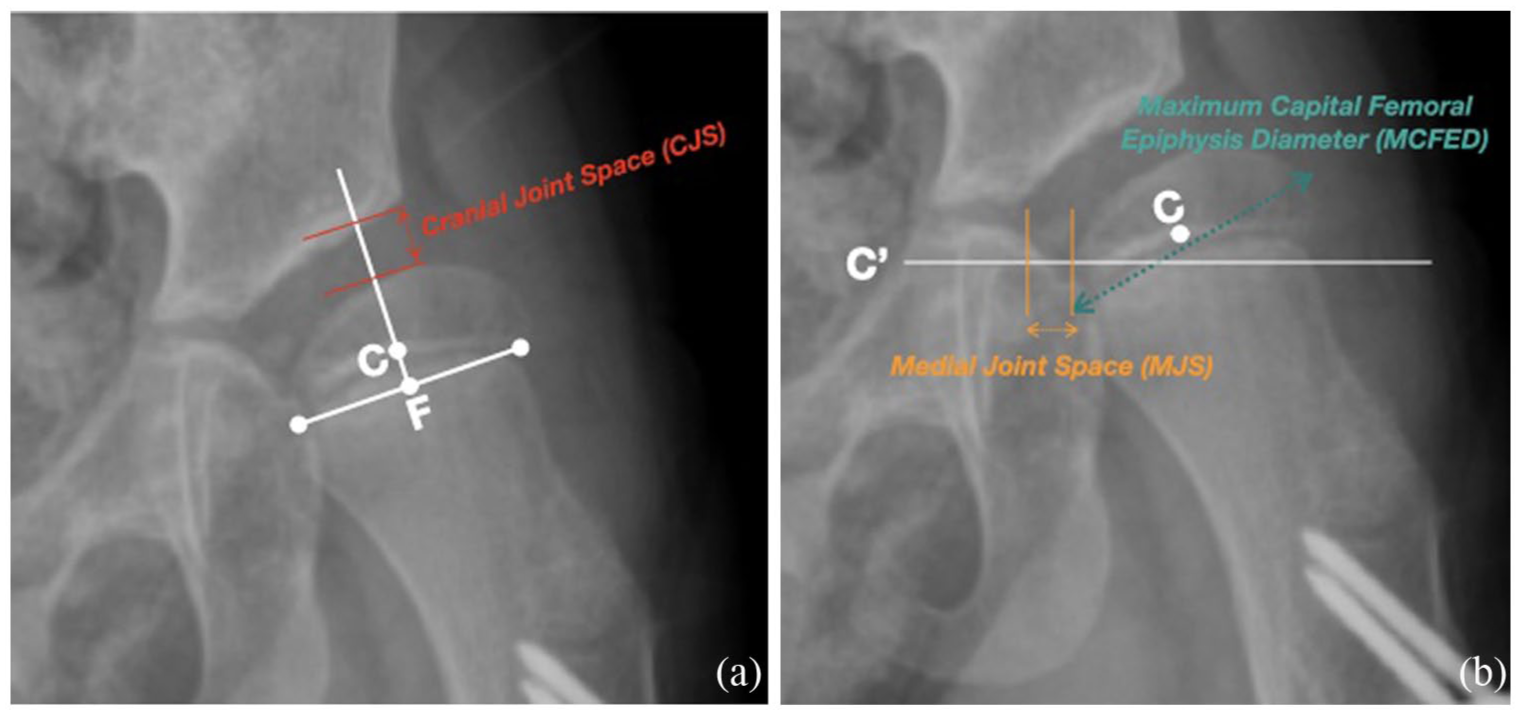
AP pelvis radiographs of the left hip illustrating the radiographic measurements used in the study.
The study protocol was approved by the institutional ethics committee (IRB No: GO 23/393). Data collection and analysis were performed in accordance with the ethical standards of the Declaration of Helsinki.
Statistical analysis
Analyses were performed using the free and open-source software R (version 4.4.1, https://cran.r-project.org), SPSS for Windows Version 23.0 statistical package (Chicago, IL) by an academic biostatistician. Normality of the data was assessed using the Kolmogorov–Smirnov test and Q-Q plot, and variance homogeneity was tested using Levene’s test. Descriptive statistics were presented as mean ± SD, median (25th percentile–75th percentile) and frequencies (percentages) as appropriate. To compare differences between groups, Student’s t-test or Mann–Whitney U test was used for continuous variables, and Pearson chi-squared test, Yates continuity correction chi-square test, or Fisher–Freeman–Halton test used for categorical variables. Cohen’s d effect size for Student’s t test, r = z/
In addition to logistic regression analysis, a classification and regression tree (CART) model was constructed using the “rpart” package in R to visualize and explore the hierarchical structure of the predictors associated with hip dislocation. 23 The decision tree allowed identification of high-risk subgroups based on surgical age, postoperative Sharp’s angle, and postoperative MHR. The decision tree was visualized using the “rpart.plot” package in R. 24 The statistical significance level was accepted as p < 0.05.
Results
A total of 93 children (115 hips) with CP who underwent surgical treatment for hip displacement were analyzed. Of these, 25 hips (21.7%) experienced redislocation, while 90 hips (78.3%) remained stable following surgery and throughout follow-up until triradiate cartilage closure.
Univariate analysis
Patients in the redislocation group were significantly younger at the time of surgery compared to those without redislocation (median 76.0 months vs. 112.5 months; p < 0.001). Redislocation occurred significantly more frequently in hips treated with femoral osteotomy alone (40.0%) compared to those treated with combined FPO (16.7%, p = 0.026), as shown in Table 1, Figure 2.
Univariate analysis of risk factors for hip dislocation.
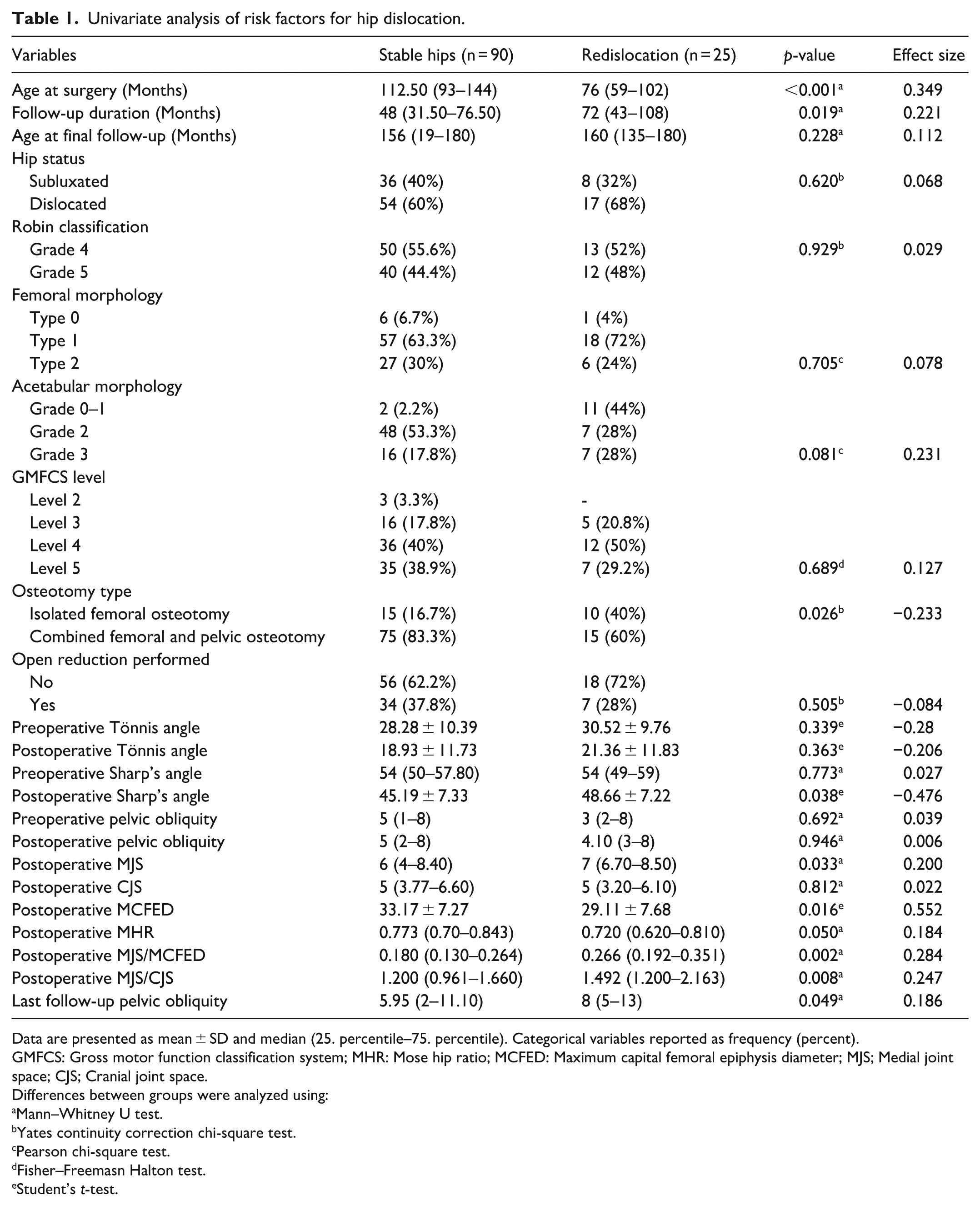
Data are presented as mean ± SD and median (25. percentile–75. percentile). Categorical variables reported as frequency (percent).
GMFCS: Gross motor function classification system; MHR: Mose hip ratio; MCFED: Maximum capital femoral epiphysis diameter; MJS; Medial joint space; CJS; Cranial joint space.
Differences between groups were analyzed using:
Mann–Whitney U test.
Yates continuity correction chi-square test.
Pearson chi-square test.
Fisher–Freemasn Halton test.
Student’s t-test.
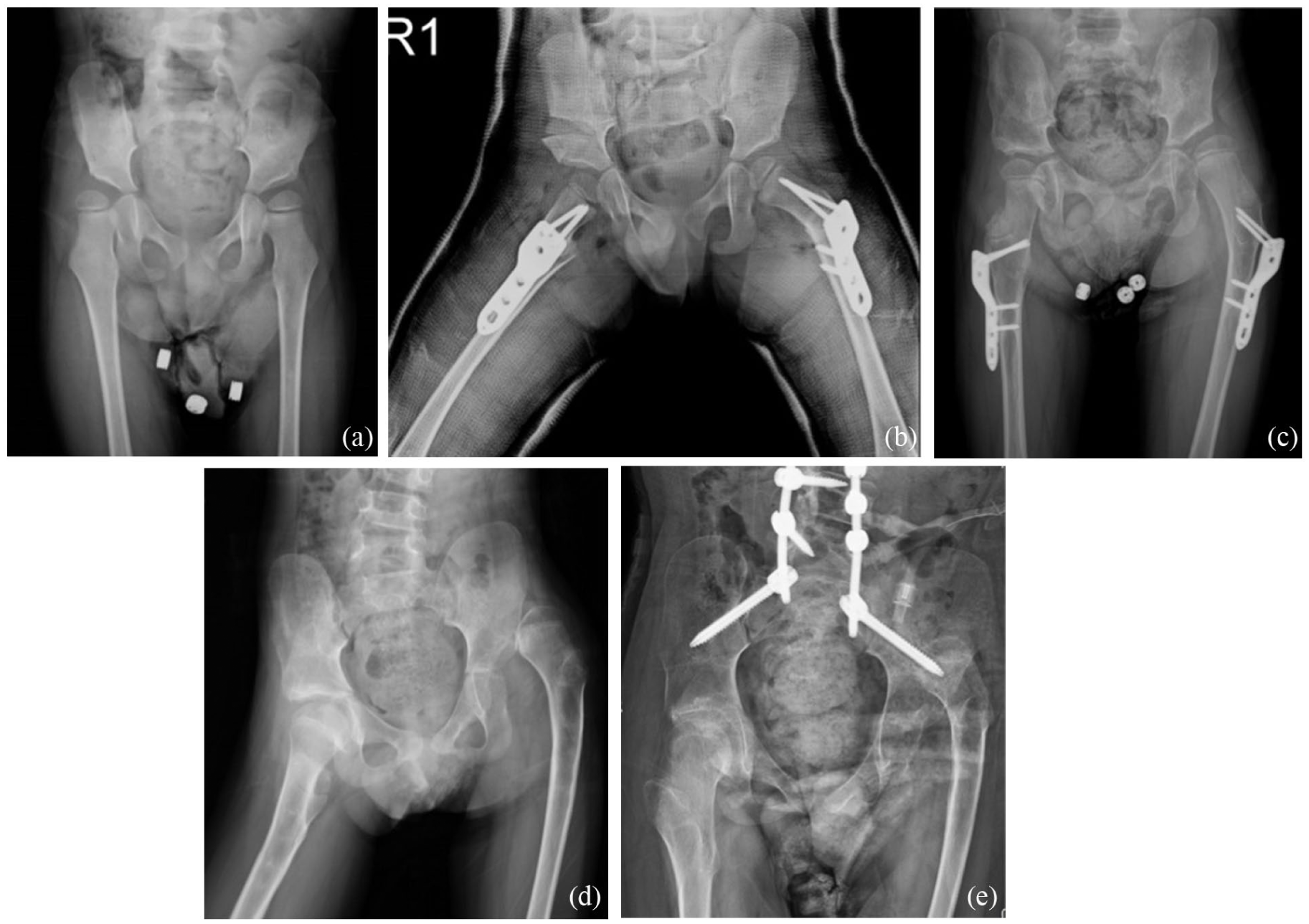
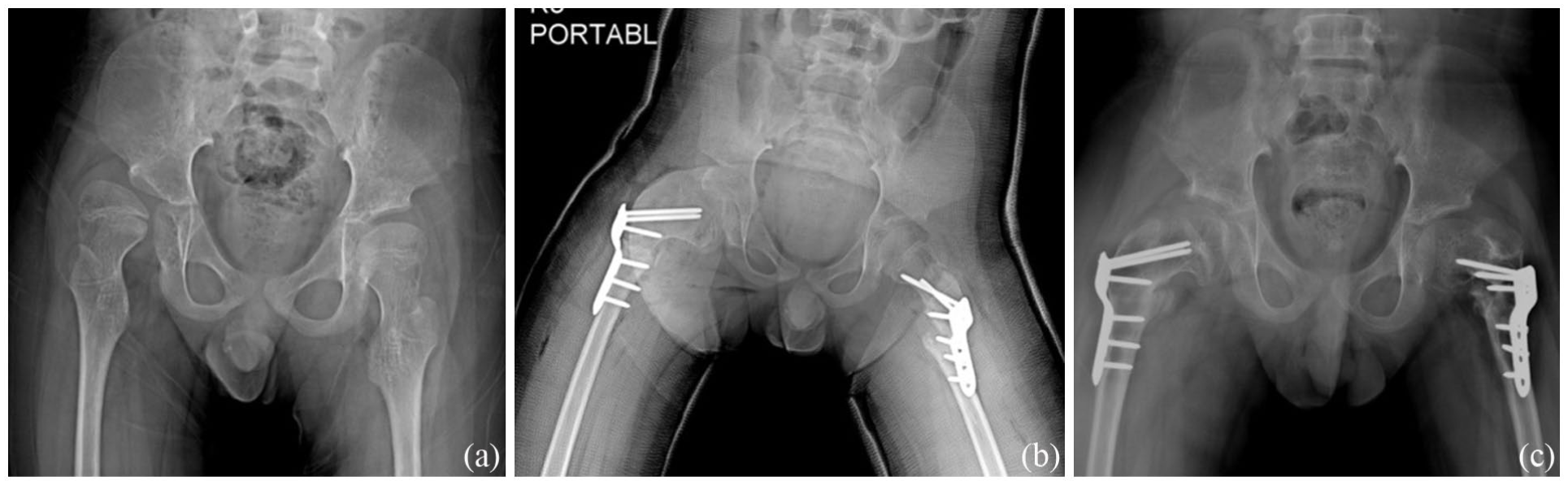
(a) Preoperative radiograph of a 47-month-old male with cerebral palsy (GMFCS level IV). (b) Immediate postoperative radiograph showing right-sided Pemberton osteotomy with femoral VDRO and left-sided femoral VDRO alone. Despite the young age, the left hip was treated with femoral osteotomy alone, with early postoperative MHR of 0.70, Sharp angle of 57° MJS/CJS ratio of 1.787, and MJS/MCFED ratio of 0.293. (c) Three-year follow-up demonstrating redislocation of the left hip. (d) Radiograph at follow-up showing persistent left hip dislocation. (e) Final follow-up at 13.5 years of age showing persistent left hip dislocation.
Radiographic outcomes demonstrated significant differences between groups in the early postoperative period. Hips that later redislocated had a significantly higher postoperative Sharp’s angle (mean 48.7° vs. 45.2°; p = 0.038) and lower postoperative MHR (mean 0.72 vs. 0.77; p = 0.050). Additionally, radiographic ratios reflecting joint congruency were also significantly different. Both the postoperative MJS/CJS (p = 0.011) and the postoperative MJS/MCFED (p = 0.014) were higher in hips that redislocated.
Multivariate logistic regression analysis
Multiple binary logistic regression analysis identified three independent risk factors associated with hip redislocation. These included younger age at surgery (OR = 0.981, 95% CI: 0.967–0.996; p = 0.010), higher postoperative Sharp’s angle (OR = 1.082, 95% CI: 1.006–1.165; p = 0.034), and lower postoperative MHR (OR = 0.007, 95% CI: 0.000–0.681; p = 0.033), as detailed in Table 2.
Binary multiple logistic regression results.
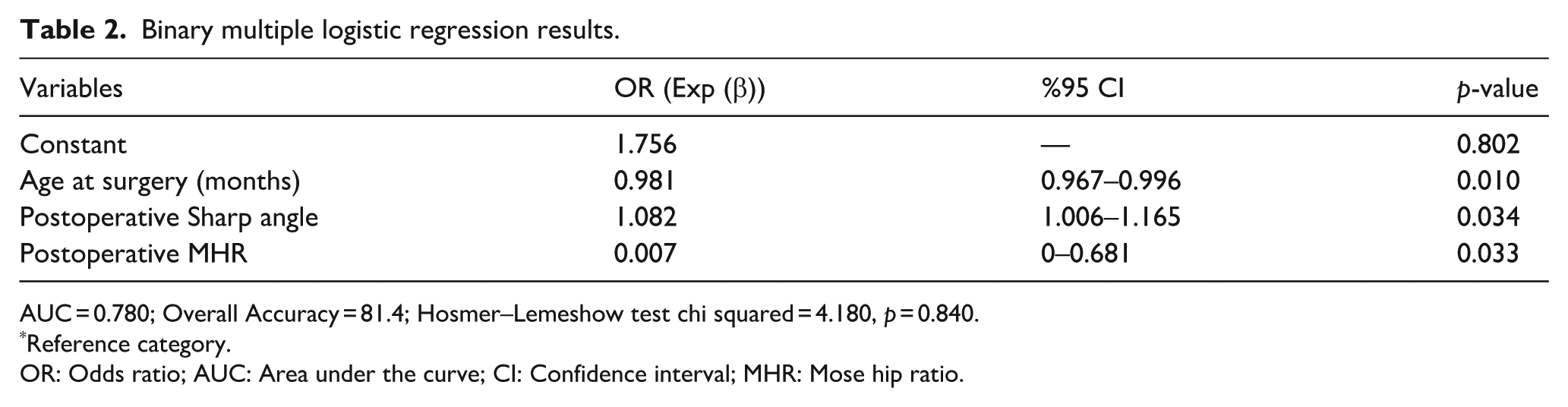
AUC = 0.780; Overall Accuracy = 81.4; Hosmer–Lemeshow test chi squared = 4.180, p = 0.840.
Reference category.
OR: Odds ratio; AUC: Area under the curve; CI: Confidence interval; MHR: Mose hip ratio.
The logistic regression model showed good calibration and discriminatory performance, with an AUC of 0.780, overall accuracy of 81.4%, and a non-significant Hosmer–Lemeshow test result (p = 0.840), suggesting excellent model fit (Figure 3).
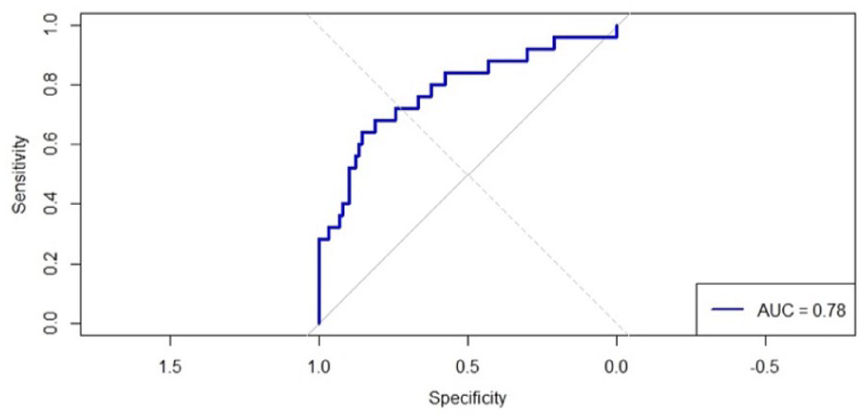
ROC curve illustrating the discriminatory performance of the multivariable logistic regression model for predicting hip dislocation. The model included age at surgery, postoperative Sharp’s angle, and postoperative MHR as independent predictors. The AUC was 0.780, indicating acceptable discriminative ability.
ROC curve analysis
ROC curve analysis for surgical age yielded an optimal cutoff value of 76 months, above which the risk of redislocation significantly decreased. This threshold demonstrated a sensitivity of 64%, specificity of 90%, and an AUC of 0.745, indicating moderate diagnostic performance, Table 3.
ROC analysis results.

CI: Confidence interval, AUC: Area under the curve; ROC: Receiver operating characteristic.
Decision tree model
To further evaluate the interaction between risk factors, a decision tree analysis was performed, Figure 4. The first node split on surgical age, with all patients older than 76 months having a low risk of redislocation. Among patients aged 76 months or younger, those with a postoperative Sharp’s angle ≥48° were at particularly high risk, with an 85% redislocation rate. Within the lower Sharp’s angle subgroup (<48°), postoperative MHR was further discriminative; patients with MHR < 0.69 were classified as redislocated with a 67% probability, whereas those with MHR ≥ 0.69 remained stable in 83% of cases, Table 4, Figure 5.
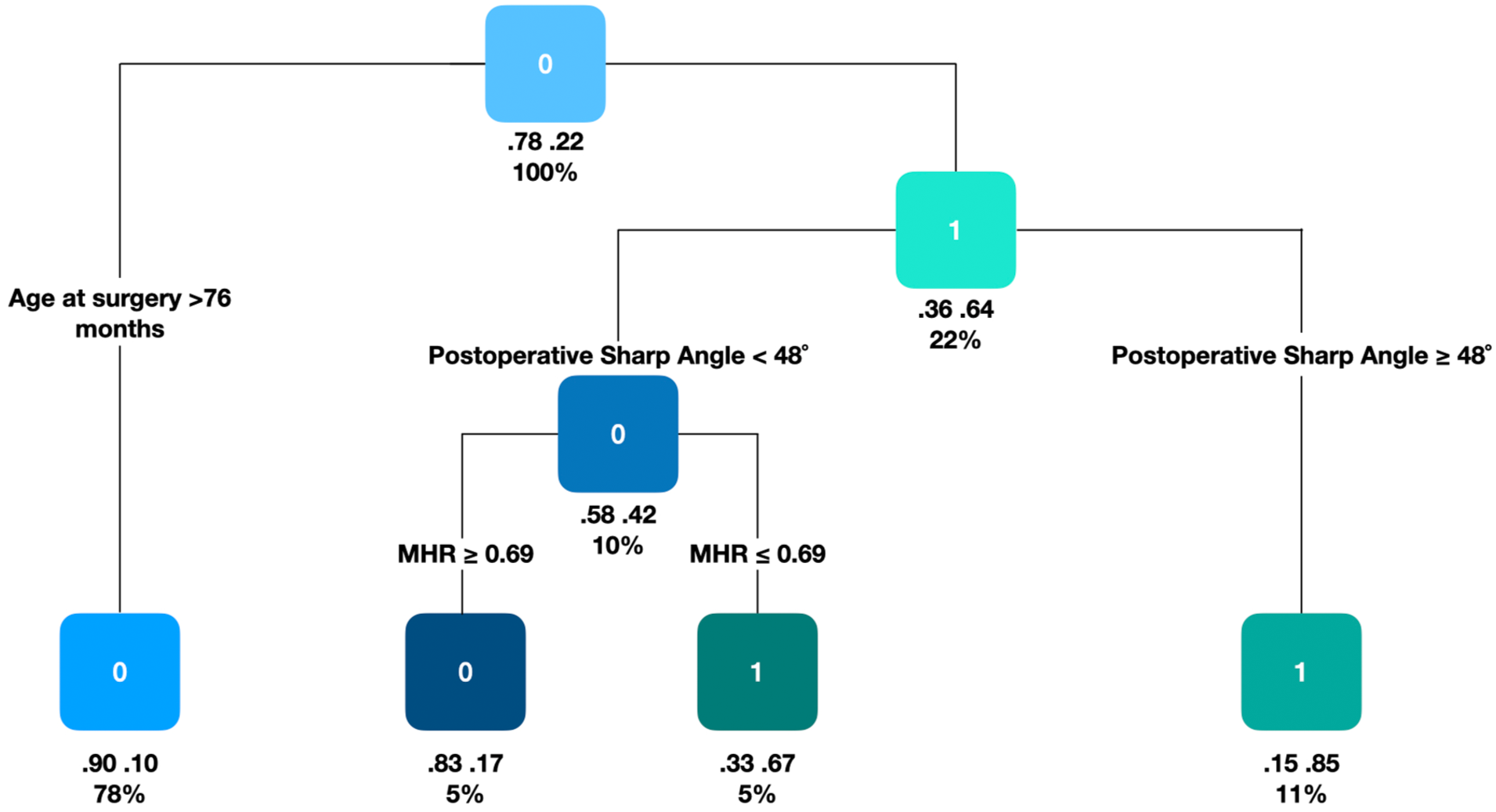
CART model for predicting hip redislocation after reconstructive osteotomy in children with cerebral palsy.
Decision tree-based risk stratification for hip redislocation.
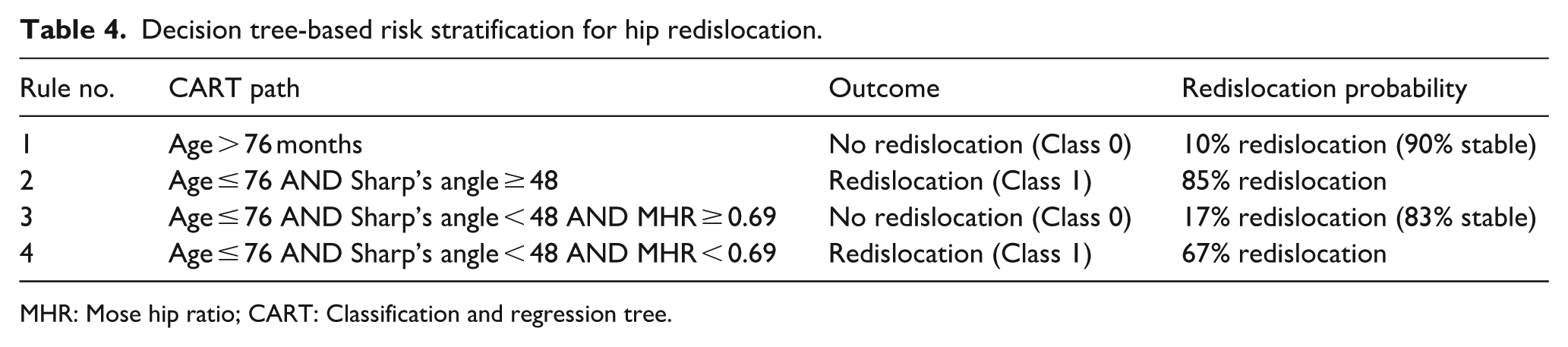
MHR: Mose hip ratio; CART: Classification and regression tree.
(a) Ten-years-old boy with CP, preoperative radiograph showing right-sided hip dislocaiton. (b) Immediate postoperative radiograph demonstrating right-sided Pemberton osteotomy with VDRO and left-sided VDRO. At early postoperative assessment, the right hip demonstrated a MHR of 0.782, Sharp’s angle of 41°, MJS/CJS ratio of 0.988, and MJS/MCFED ratio of 0.128. (c) Final follow-up radiograph at 13 years of age showing maintained hip stability and remodeling.
Discussion
In this multicenter study of children with CP followed to triradiate closure, hip redislocation occurred in 21.7% of surgically treated hips. Younger age at surgery, higher postoperative Sharp’s angle, and lower postoperative MHR were independently associated with redislocation. The decision-tree model allowed identification of high-risk subgroups based on these factors and provided a clinically useful tool for risk stratification and postoperative monitoring.
The elevated risk in younger children may be attributed to ongoing skeletal growth, which can compromise the durability of surgical corrections made at an early stage. In the study by Shore et al., children operated at a younger age had significantly lower 5-year survivorship rates. Specifically, those at GMFCS level V had a 76% success rate, compared to 92% in GMFCS levels I–II, and younger age independently predicted failure with a hazard ratio (HR) of 0.92 per additional year. 11 Delbrück et al. 25 also demonstrated that redislocation was more common in children younger than 8 years, with a pooled redislocation rate of 16.6% in this group versus 7.2% in older children. Their meta-regression further confirmed a statistically significant association between younger age and higher redislocation rates. Together, these findings highlight that the timing of surgery plays a critical role in long-term hip stability and that careful patient selection and extended monitoring are warranted in younger cohorts.11,25 In addition to these factors, it should be noted that children operated at an earlier age often present with a higher preoperative displacement rate, which in turn requires earlier surgery. The higher redislocation rate observed in younger children may therefore reflect more severe preoperative displacement requiring earlier intervention, rather than the effect of age alone. 26
Our study demonstrated a higher rate of redislocation in hips treated with isolated FO compared to those managed with combined FPO, which the reader correctly noted. While this difference reached significance in univariate analysis, it did not remain an independent predictor after multivariate analysis. This finding aligns with several recent studies emphasizing the importance of addressing both femoral and acetabular components in hip reconstruction for children with CP. Kiapekos et al. conducted a prospective 5-year follow-up study involving 163 children and showed that combined FPO was associated with a significantly lower failure rate than isolated FO, despite higher preoperative migration percentages in the FPO group. The HR for failure was 0.32 in favor of FPO, indicating a protective effect against redislocation. 27 Similarly, meta-analysis involving over 6000 hips confirmed that combined procedures achieved superior improvements in key radiological indices compared to FO alone. 28 Additionally, Huh et al. recommended a sequential approach based on intraoperative fluoroscopic and arthrographic assessment. They reported that a substantial proportion of hips with high preoperative MI managed with FO alone developed residual or recurrent subluxation, supporting the need for pelvic osteotomy in selected cases. 29 Together, these findings support our observation that the addition of pelvic osteotomy provides a more comprehensive correction and may be critical to preventing redislocation, particularly in patients with high MI or poor acetabular coverage.
Radiographic parameters, particularly the postoperative Sharp’s angle and MHR were also strongly associated with redislocation risk in our cohort. A higher Sharp’s angle postoperatively likely reflects residual acetabular dysplasia or undercorrection, which may compromise femoral head coverage and increase the chance of recurrence. In a recent meta-analysis, similarly reported that hips with final Sharp’s angles ≥45° had significantly higher redislocation rates, with pooled data showing a 25.2% redislocation rate in this group versus 6.5% for those with better acetabular coverage. 25 Although MHR has been less commonly used in the literature, it provides a reliable surrogate for femoral head sphericity and containment. 18 In our study, a lower postoperative MHR was independently associated with redislocation, suggesting that suboptimal femoral head shape at the time of surgery may predispose to long-term failure.
Our study identified increased postoperative MJS/CJS and MJS/MCFED ratios as significant predictors of hip redislocation, suggesting their potential utility as markers of incomplete femoral head containment and joint incongruity. These derived measurements, indicating nonconcentric reduction and disproportion relative to femoral head size, were notably elevated in hips that dislocated, potentially suggesting loading or early subluxation. Although such ratios are not currently included in standard CP hip surveillance protocols or consensus guidelines, they may offer complementary insight, especially in borderline cases. 30 Although concepts of femoral head containment and remodeling have been discussed in prior work, to our knowledge, this is the first study to demonstrate a significant association between joint space ratios and redislocation risk. 18 These findings may introduce a novel area of radiographic assessment that improve postoperative monitoring and warrant prospective validation in larger cohorts.
The application of a CART decision-tree model in our study allowed us to identify high-risk subgroups for hip redislocation using easily measurable postoperative parameters, offering a clinically interpretable and visually intuitive tool for stratifying patients. While logistic regression has been widely used to identify risk factors in CP hip pathology, few studies have used tree-based models for surgical outcome prediction. Bertoncelli et al., 31 who developed a multicenter logistic regression model (“PredictMed”) to identify risk factors for NM hip dysplasia, achieving 77% accuracy and confirming known predictors such as nonambulatory status and trunk hypotonia. More recent study applied a machine learning-based support vector machine classifier trained on hip surveillance data to categorize hips as normal, at-risk, or dislocated, demonstrating the feasibility of automated classification with high diagnostic accuracy. 32 However, these models primarily focused on surveillance and preoperative risk, rather than predicting postoperative redislocation.31,32 To our knowledge, our study is the first to apply a decision-tree model to stratify redislocation risk after surgical hip reconstruction in children with CP. As multicenter datasets grow, incorporating hybrid models that combine traditional predictors with automated image-based features may further improve prognostic accuracy and guide personalized surgical planning.
This study has several limitations. First, its retrospective design may introduce selection bias and limit the control over surgical decision-making and follow-up protocols across centers. Second, radiographic measurements were based on standardized AP pelvic images, but variability in positioning or image quality may have affected some parameters. Third, while the multicenter nature increases generalizability, it also introduces heterogeneity in surgical techniques, surgeon experience, and postoperative rehabilitation protocols, which were not uniformly controlled. Fourth, the number of redislocation cases was relatively small, potentially limiting the power of subgroup analyses. Additionally, postoperative MI was not analyzed as an independent outcome variable—an acknowledged limitation given its correlation with redislocation risk. This decision was influenced by variable radiograph quality across centers, the known unreliability of manual MI measurements, and uncertainty in identifying the true lateral acetabular margin in Gothic arch deformities. Due to the multicenter design, surgical technique varied by surgeon preference though the choice of osteotomy was not expected to influence outcomes. Lastly, although our decision-tree model provides a clinically intuitive tool for risk stratification, it has not yet been externally validated and should be interpreted as exploratory until confirmed in future prospective studies.
The clinical relevance of these findings may emphasize the importance of timely surgical intervention, particularly in younger patients, before femoral head sphericity is compromised, as preserving head shape is essential for maintaining joint congruency and long-term function. Effective acetabular reconstruction may complement femoral correction to improve containment and stability. Addressing both the femur and acetabulum during reconstruction could be important in reducing the risk of redislocation and optimizing long-term hip stability in children with CP, especially in cases with severe displacement at a younger age. These findings may help guide surgeons in clinical decision-making and surgical planning.
Conclusion
In this multicenter study with follow-up to skeletal maturity, younger surgical age, higher postoperative Sharp’s angle, and lower MHR were identified as independent risk factors for hip redislocation in children CP. The decision-tree model provided a practical tool for risk stratification. These findings demonstrate the importance of adequate radiographic correction and age-appropriate surgical planning to optimize long-term hip stability.
Supplemental Material
sj-pdf-1-cho-10.1177_18632521251411141 – Supplemental material for Risk factors for hip redislocation in surgically treated children with cerebral palsy: A multicenter study with follow-up until skeletal maturity
Supplemental material, sj-pdf-1-cho-10.1177_18632521251411141 for Risk factors for hip redislocation in surgically treated children with cerebral palsy: A multicenter study with follow-up until skeletal maturity by Rafik Ramazanov, Ulaş can Kolaç, Evren Akpinar, Sadettin Ciftci, Guney Yilmaz, Mehmet Salih Soylemez, Murat Celal Sozbilen, Yavuz Saglam, Hakan Senaran, Abdullah Eren, Mehmet Ali Talmac, Ali Seker, Sema Ertan Birsel, Hanife Avci and Muharrem Yazici in Journal of Children's Orthopaedics
Footnotes
Author contributions
All authors contributed to the study conception and design. Surgical treatment of the patients was performed by Rafik Ramazanov, Evren Akpınar, Sadettin Ciftci, Guney Yilmaz, Mehmet Salih Soylemez, Murat Celal Sozbilen, Yavuz Saglam, Hakan Senaran, Abdullah Eren, Mehmet Ali Talmac, Ali Seker, Sema Ertan Birsel Guney Yilmaz and Muharrem Yazici. Data collection and analysis were performed by Rafik Ramazanov and Ulaş Can Kolaç. The first draft of the manuscript was written by Ulaş Can Kolaç and Rafik Ramazanov. Guney Yilmaz and Muharrem Yazici and participated in the reviewing and editing of the manuscript before submission.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethics approval
The study protocol was approved by the institutional ethics committee at Hacettepe University (IRB No: GO 23/393). Data collection and analysis were performed in accordance with the ethical standards of the Declaration of Helsinki.
Consent to participate
Patients gave written informed consent for participation in the study.
Consent for publication
Patients gave written informed consent for the publication of the study.
Data availability
The data that support the findings of this study are available from the corresponding author upon reasonable request.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.