
Abstract
Purpose:
Patients with cerebral palsy commonly exhibit flexed knee gait. Hamstring lengthening is a common intervention, and the popliteal angle test (PAT) is widely used to assess hamstring tightness and guide surgical planning. This systematic review evaluated the role of the popliteal angle test in relation to surgical hamstring lengthening.
Methods:
PubMed, Scopus, Web of Science, Embase, and Cochrane Library were searched from inception to January 29, 2025 for articles involving cerebral palsy, popliteal angle test, and hamstring lengthening.
Results:
Thirty-one articles met the inclusion criteria. Outcomes were reported per patient or per limb, with Gross Motor Function Classification System level specified in 19 studies. Nineteen studies (61.3%) incorporated the popliteal angle test in preoperative assessments, 6 (19.4%) used it as the sole surgical determinant, and 4 (12.9%) applied it intraoperatively to guide additional hamstring lengthening. Twenty-seven studies reported pre- and postoperative popliteal angle test values; among the 21 providing statistical analyses, all showed significant postoperative improvement, although repeat procedures and longer follow-up failed to demonstrate sustained benefit. Kinematic data were reported in 20 studies, but analyses were mostly limited to sagittal knee flexion/extension during stance. Follow-up was reported in 24 studies, but durations rarely exceeded 2 years.
Conclusions:
The popliteal angle test remains widely used in the surgical assessment of flexed knee gait in cerebral palsy, but methodological heterogeneity limits comparability across studies. While postoperative improvements are common, they cannot be reliably correlated with gait outcomes. The main limitation lies in its use as the sole surgical or intraoperative determinant. Standardized protocols, integration with gait analysis, and long-term follow-up are needed to clarify its prognostic value.
Introduction
In cerebral palsy (CP), flexed knee gait is a common pathological gait pattern, with manifestations that vary according to the timing of knee flexion within the gait cycle and the corresponding pelvic and ankle kinematics. 1 Three gait pattern subtypes are commonly described. Jump knee gait is characterized by excessive knee flexion at initial contact and early stance with concomitant ankle equinus, followed by relative knee extension in mid-stance. Apparent equinus gait presents with neutral ankle dorsiflexion and knee flexion producing a toe-walking appearance despite near-normal ankle motion. Flexed knee gait is defined by flexion of the hip, knee, and ankle dorsiflexion, accompanied by reduced plantarflexor–knee extension coupling and diminished ground reaction force support, throughout the stance phase.2,3 Although these gait patterns differ in their kinematic characteristics and underlying mechanisms, clinical evaluation of flexed knee gait has traditionally relied on the popliteal angle test (PAT), an assessment based of the physical examination of knee extension of patients in supine position, as a proxi for hamstrings’ length.4,5
The unilateral PAT is performed with the patient in supine position, the hip flexed to 90° (side being examined), and the contralateral lower limb extended at the examination table. The knee in question is then passively extended until resistance is felt, and the popliteal angle is measured as the angle between the long axes of the tibia and femur. 6 In the bilateral PAT, both hips are flexed to 90° while the examiner passively extends the knee of the tested limb until either the first resistance (R1) or end range (R2), measuring the resulting knee flexion angle with a goniometer. 4 Angles obtained with the bilateral and unilateral methods are not interchangeable; it is essential to documenting both the method used and whether the value represents R1 or R2, as R1 is more strongly associated with knee flexion at initial contact and terminal swing than R2. 6 Furthermore, it is worth mentioning the need to consider the Tardieu scale, which is a useful tool in examining spasticity. Within the Tardieu scale, the first catch felt during a fast passive stretch is recorded as R1, while R2 is the full passive range of motion achieved during a slow stretch. The difference between R2 and R1 (R2–R1) quantifies the dynamic component of spasticity. 7 It is important to notice that the clinical consequences of hamstring contracture differ according to whether the patient is ambulant or non-ambulant. In ambulant patients (GMFCS levels I–III), increased hamstring tone restricts knee extension during stance and initial contact, leading to inefficient gait and increased energy expenditure. 8 In non-ambulant patients (GMFCS levels IV–V), hamstring spasticity and reduced length primarily affect positioning and sitting comfort. 4 Surgical lengthening of the medial and/or lateral hamstring musculature is a widely used treatment in both ambulant and non-ambulant patients,5,9,10 and it may secondarily increase anterior pelvic tilt during gait. 11
One of the key limitations of the PAT as a primary surgical indicator is that it assesses hamstring length in a position that does not replicate the upright posture of gait, where the hips and knees are partially or fully extended during some phases of the gait cycle. 1 Furthermore, a weak correlation between physical examination and three-dimensional motion analysis (3DMA) data has been documented.12–14 For optimal surgical planning in gait disturbances associated with CP, Davids et al. 3 advocate a multimodal assessment approach, and Gage et al. 1 emphasize that surgical indications should derive from the combined interpretation of gait analysis and clinical examination. Nonetheless, the PAT remains far more widely used in clinical practice than more sophisticated tools such as 3DMA, largely due to its simplicity and accessibility. 15 It is of note that previous studies report significant variability in PA measurements across inter-rater, intra-rater, and intersession assessments in children with CP.6,16
Accessibility of the PAT in contrast to less availability of 3DMA may be a factor in the PAT’s continued use. This systematic review examines available evidence for the use of the PAT in relation to surgical hamstring lengthening. Published data on surgical outcomes, kinematic data utilization, and the PAT’s overall utility as a clinical tool for surgical decision-making in patients with CP were investigated.
Materials and methods
Study design
This systematic review was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines to ensure transparency and methodological rigor. The objective was to determine the role of the PAT in the management of flexed knee gait in patients with CP, with particular attention to its use as a surgical indicator, its application in intraoperative decision-making, and its contribution to overall clinical assessment in relation to three-dimensional motion analysis.
Studies were included if they met the following criteria:
Population: Patients diagnosed with CP with lower limb involvement presenting with flexed knee gait.
Assessment method: The study had to include a quantified PAT, reporting at least one of the following: measurement protocol (unilateral or bilateral, hip flexed to 90°, passive knee extension to R1 and/or R2), outcome definition (angle between tibia and femur), or clinical role (surgical indicator, intraoperative tool, or part of overall assessment).
Intervention: When a surgical intervention was evaluated, it was related to distal hamstring lengthening surgeries. Multilevel surgeries were not a criterion for exclusion.
Search strategy
A comprehensive search was performed across five electronic databases: PubMed, Scopus, Cochrane Library, Embase, and Web of Science. The search strategy was based on the following query:
Searches were carried out on November 12, 2024, then re-run on January 29, 2025, to check for any new publications. The search included results from their dates of their inception to execution of search. There were no restrictions on time of publication. Duplicate records were identified and removed before screening. Articles were restricted to full-text articles written in English language.
Study selection
The selection process adhered to the PRISMA framework and involved the following steps:
Identification: All records retrieved from the database search were compiled, and duplicates were removed using Covidence Software.
Screening: Two independent authors conducted a title and abstract screening to assess the relevance of each study. Discrepancies were resolved by discussion between the two authors.
Eligibility: Full-text screening of the remaining studies was performed by one author to confirm inclusion based on predefined eligibility criteria.
Inclusion: Studies meeting all inclusion criteria were included in the final analysis. The PRISMA flow diagram summarizes the number of studies at each stage (Figure 1).
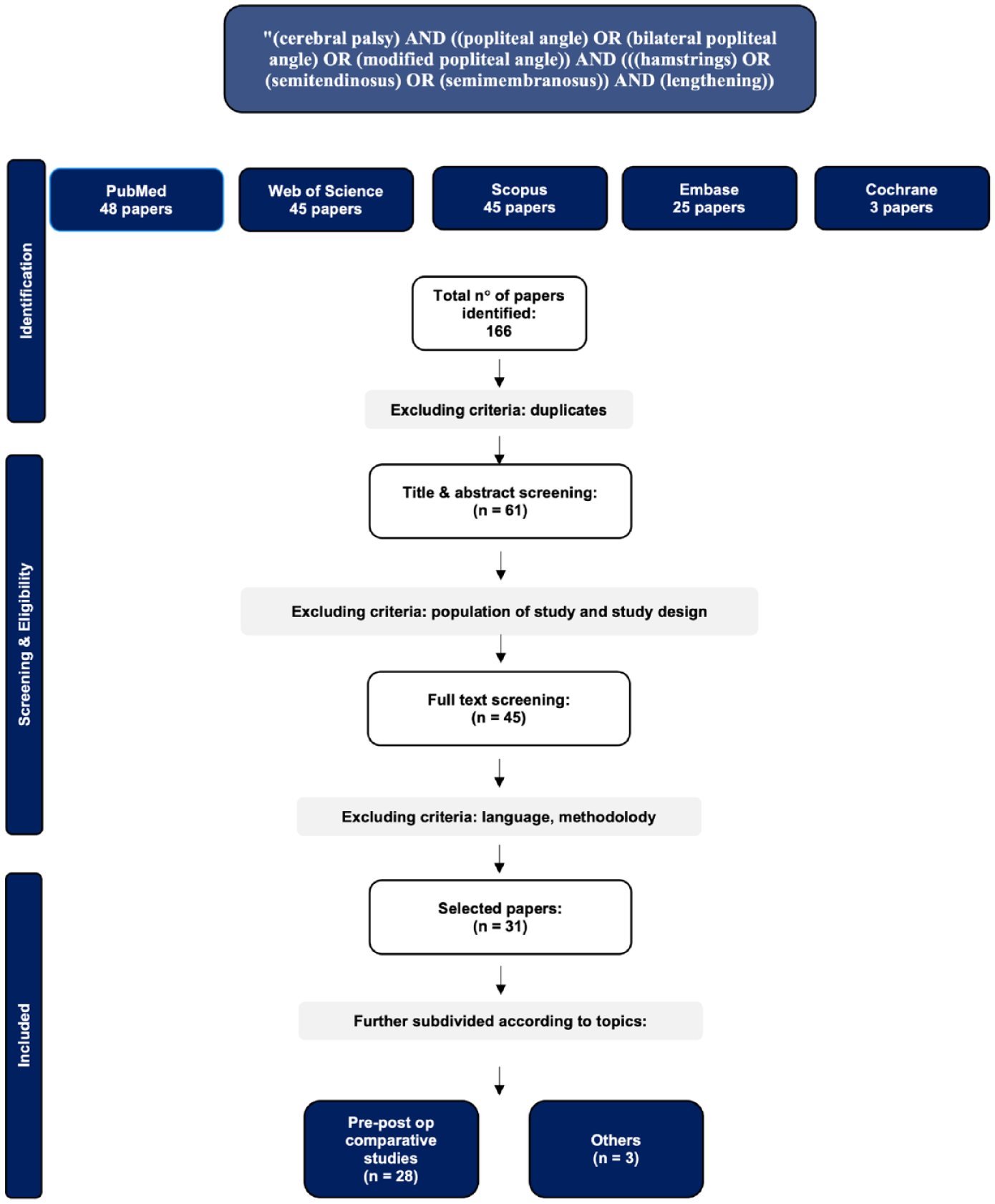
PRISMA flowchart on search strategy for screening and selection process.
Data extraction and management
Data extraction was performed by one author using a predefined template, and the extracted data were independently checked for accuracy by two additional authors.
The following data from each included article was collected:
General study information: Title, authors, journal, and year of publication.
Population characteristics: Sample size, age, Gross Motor Function Classification System (GMFCS) level.
Treatment: Distal hamstring lengthening, when performed.
Pre- and postoperative clinical data: Unilateral popliteal angle, bilateral popliteal angle, flexion deformity/extension deficit.
Pre- and postoperative kinematic data: Knee flexion at initial contact, minimum knee flexion in stance, mean knee flexion in stance, knee flexion at initial swing, and knee flexion at terminal swing, when available.
During data extraction, the included studies were classified into two primary categories: (1) those comparing preoperative and postoperative PAT results, and (2) those evaluating the measurement or clinical application of the PAT without assessing surgical outcomes. The first category was further subdivided according to the role of the PAT in surgical decision-making: (a) sole surgical indicator, (b) intraoperative decision-making tool, and (c) component of an overall clinical assessment.
Results
A total of 62 articles were identified through the literature search, of which 31 studies met the inclusion criteria (Table 1). Twenty-seven studies reported both preoperative and postoperative PAT values. Two studies examined the measurement and clinical application of the PAT without assessing surgical outcomes, while two did not provide complete pre- and postoperative data: one omitted postoperative values, and the other analyzed variation of the PAT under anesthesia.
Summary of data extracted from included studies.
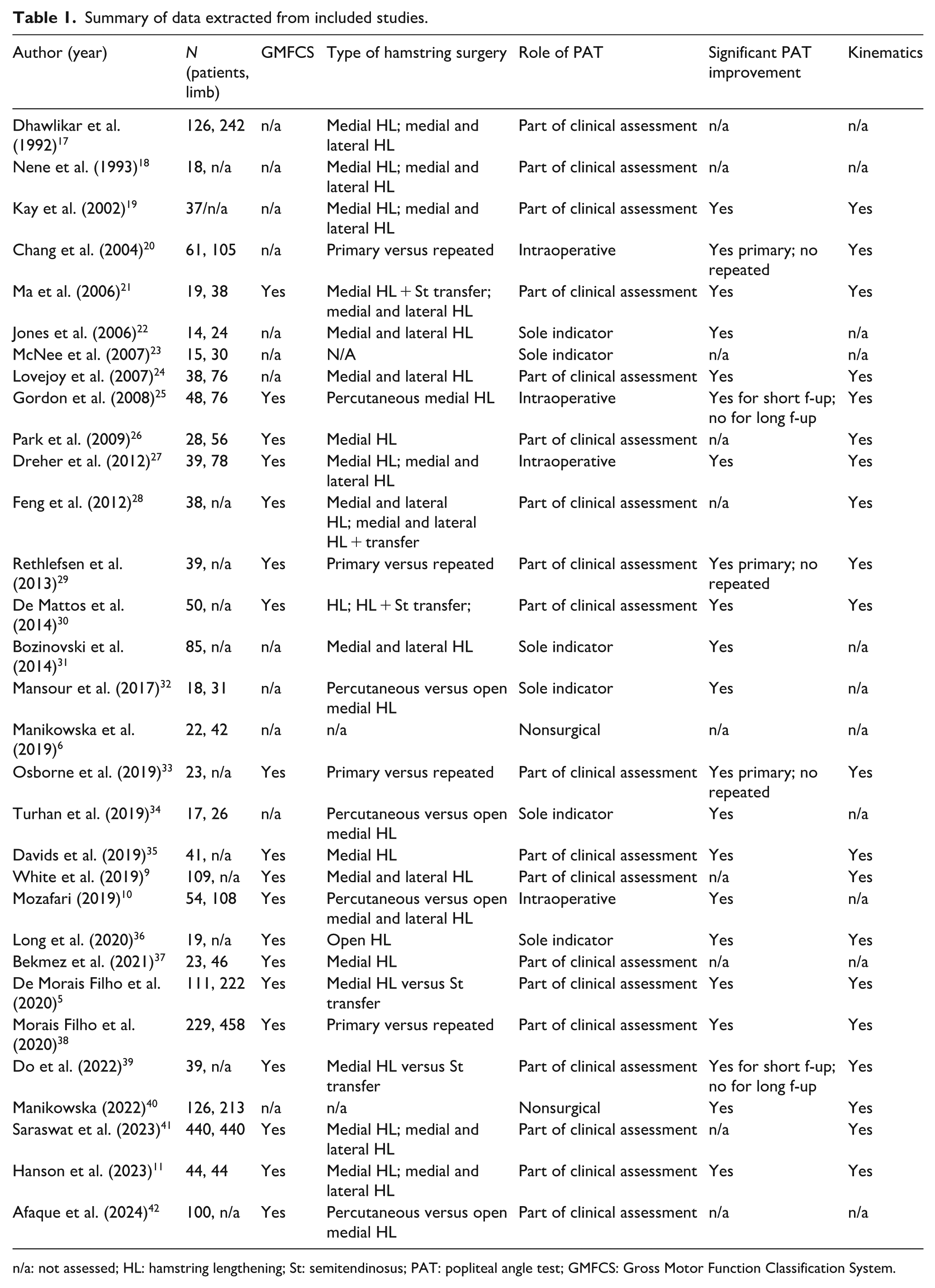
n/a: not assessed; HL: hamstring lengthening; St: semitendinosus; PAT: popliteal angle test; GMFCS: Gross Motor Function Classification System.
Population characteristics
Across the included studies, outcomes were reported either per patient or per limb. The GMFCS level was reported in 19 studies, whereas 12 omitted this information, reflecting variability in the characterization of study populations.
Type of surgeries included
In 21 of the 31 studies, hamstring lengthening was performed in combination with other surgical procedures, most often as part of a multilevel surgical approach. Proximal hamstring lengthening and proximal gastrocnemius lengthening were excluded: the former because it was not the focus of the present review, and the latter because its origin above the knee could act as a confounder in the evaluation of pre- and postoperative PAT values relative to distal hamstring lengthening. Within the context of distal hamstring procedures, the included studies described several technical variations, including medial versus combined medial and lateral hamstring lengthening, primary versus repeat interventions, percutaneous versus open techniques, and comparisons between hamstring lengthening and tendon transfer.
Inclusion of popliteal angle test
Two studies assessed the popliteal angle bilaterally5,6; all others employed a unilateral protocol, with the contralateral hip extended and the tested limb flexed to 90° at the hip. Passive knee extension was then performed, and the angle between femur and tibia measured with a goniometer. One study further examined the effect of hamstring spasticity, reporting mean values at slow and fast velocities with and without hypertonia. 40
Twenty-seven studies reported both pre- and postoperative PAT values. Among the remaining four, one compared PAT under anesthesia and without anesthesia, 23 one omitted postoperative values, 26 and two did not evaluate surgical outcomes.6,40 Of the 27 studies reporting both pre- and postoperative data, 21 provided p values, all of which demonstrated a statistically significant improvement in postoperative PAT values regardless of the surgical technique performed. Among these, three studies that analyzed both primary and repeat procedures found that re-do surgeries did not yield statistically significant changes in PAT values.
Inclusion of kinematics
Twenty of the 31 included studies reported at least one kinematic parameter. Knee flexion/extension was the most consistently evaluated, with particular emphasis on stance phase of gait. Specifically, 11 studies (36.7%) reported values at initial stance and 17 (56.7%) at mid-stance, whereas only 1 (3.3%) addressed terminal stance. Five studies (16.7%) included measurements during the swing phase (Figure 2).
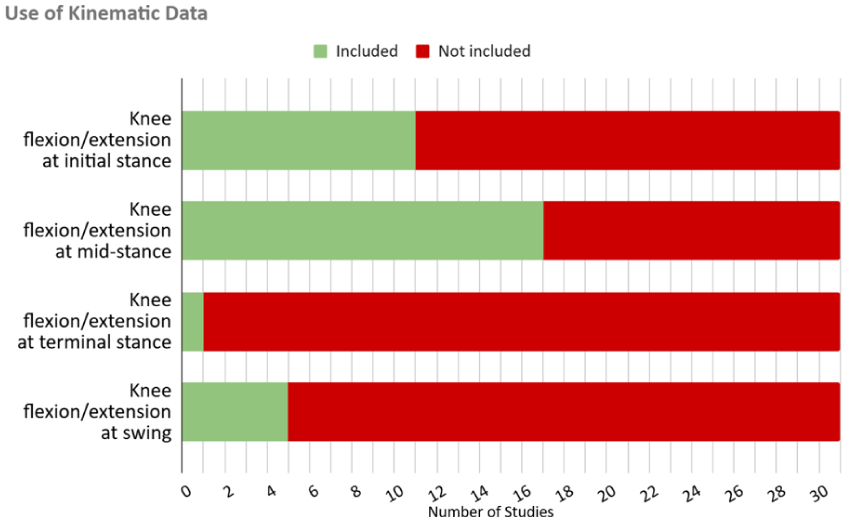
Use of kinematic data across the included studies. Knee flexion/extension was assessed at different phases of the gait cycle, most frequently at initial stance (11 studies) and mid-stance (17 studies), while only 1 study reported terminal stance values and 5 reported swing phase values.
Role of the PAT
Of the 31 included studies, 2 (6.5%) did not address surgical implications but rather investigated the measurement or clinical application of the PAT without assessing surgical outcomes. Nineteen (61.3%) reported the PAT as part of a broader set of clinical and instrumental assessments guiding surgical indication. Six (19.4%) considered the PAT as the sole determinant for surgical indication, and 4 (12.9%) employed it intraoperatively to decide on further hamstring lengthening (Figure 3).
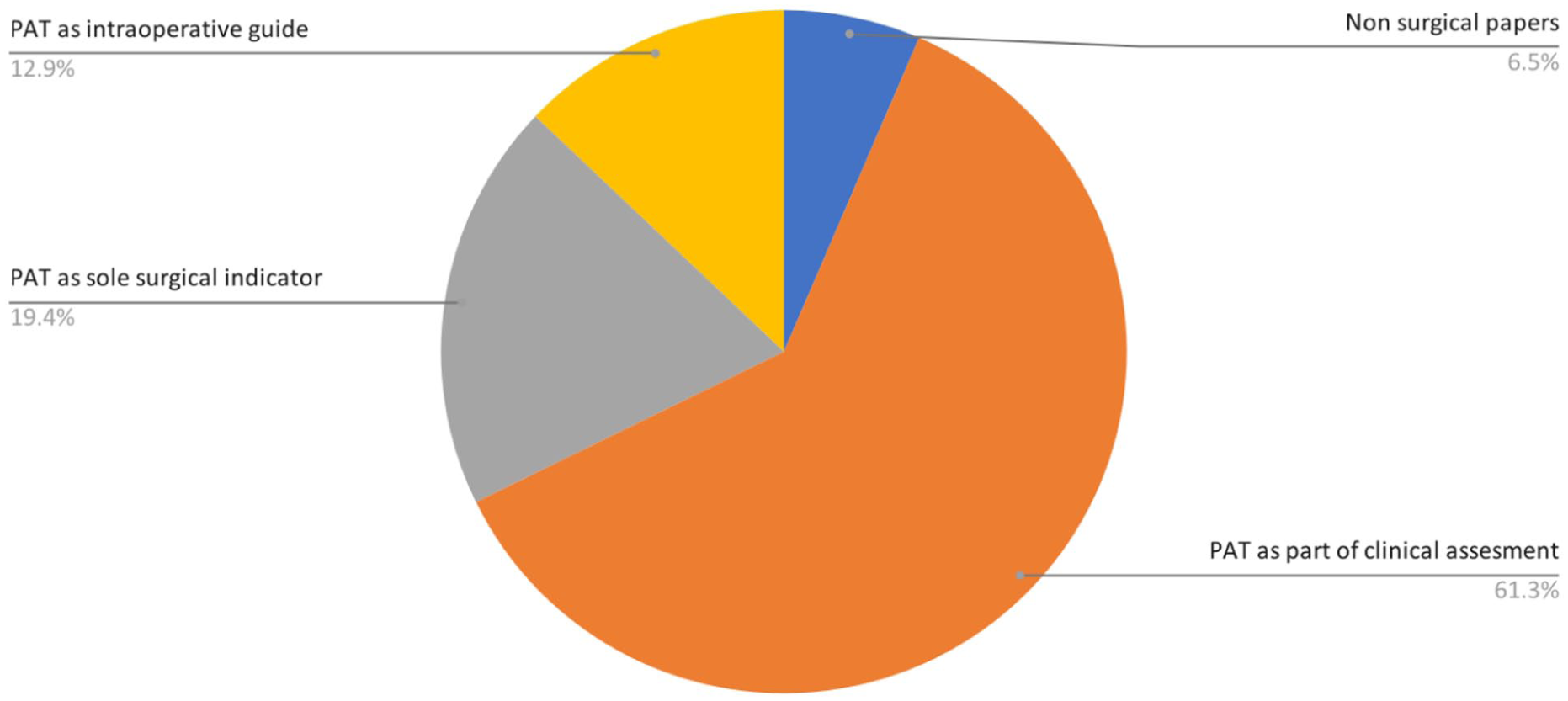
Distribution of the role of the PAT across the 31 included studies. Two studies (6.5%) did not address surgical implications, 19 (61.3%) incorporated the PAT as part of broader clinical assessments, 6 (19.4%) considered it the sole determinant for surgical indication, and 4 (12.9%) used it intraoperatively to guide additional hamstring lengthening.
Follow-up
Follow-up duration was reported in 24 studies, with considerable variability across the literature. Reported intervals ranged from only a few months to more than 12 years. In several studies, both short- and long-term outcomes were provided for the same cohort, while others reported wide ranges without specifying mean or median values. The length of follow-up also differed according to the type of surgical procedure performed, with some reports presenting multiple follow-up points to capture temporal changes. This marked heterogeneity in both duration and reporting precluded a meaningful comparison across studies and limited the possibility of drawing consistent conclusions regarding the stability of postoperative PAT improvement (Figure 4).
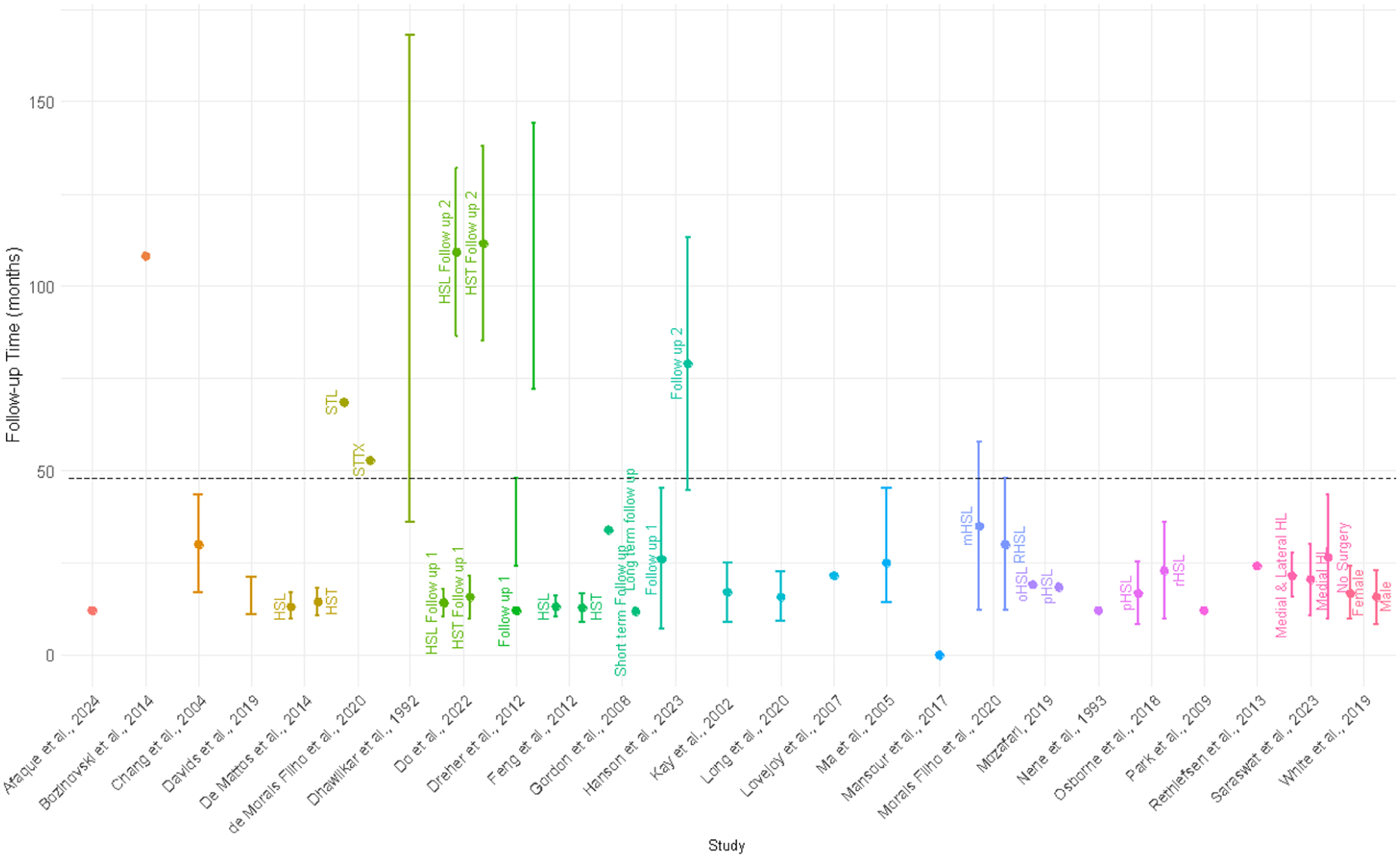
Follow-up times of comparative studies. Three studies were omitted due to no postoperative follow-up period. Means and standard deviations are plotted, or, where applicable, ranges. Horizontal line at 48 months delineates long- and short-term follow-up. Studies are different colors. Treatment groups within studies are labeled.
Discussion
This review included 31 studies evaluating the role of the PAT in the assessment and surgical management of flexed knee gait in individuals with CP. The analysis revealed considerable heterogeneity in study design: sample sizes were often inconsistently reported, either per patient or per limb, and GMFCS levels were frequently missing. In most included studies, hamstring lengthening was performed within a multilevel surgical approach, reflecting current clinical practice. Distal hamstring procedures were variably described, with differences in technique (medial versus medial and lateral, percutaneous versus open, lengthening versus transfer) and patient context (primary versus repeat procedures). Such heterogeneity limits direct comparison of outcomes across studies. Nevertheless, the first consideration that emerges from this review is that the PAT appears to remain widely used in clinical practice, both as part of preoperative assessment and, in selected cases, as a determinant for surgical decision-making.
Of the 31 included studies, 19 (61.3%) incorporated the PAT as part of a broader set of clinical and instrumental assessments guiding surgical indication. Six (19.4%) considered the PAT as the sole determinant for surgery, while 4 (12.9%) reported intraoperative use to guide additional hamstring lengthening with thresholds typically ranging from 20° to 30°.10,20,25,27 Twenty-seven studies reported both pre- and postoperative PAT values, of which 21 included statistical analyses. All demonstrated significant postoperative improvement of the popliteal angle, irrespective of surgical technique. Notably, three of these studies analyzed both primary and repeat procedures, with the latter failing to show significant change.20,29,33 Similarly, two studies reported short-term improvement that was not sustained at longer follow-up, with PAT values returning closed to preoperative levels.25,39 These findings suggest that, although PAT values frequently improve after surgery, the survivalship and correlation with functional outcomes remain uncertain. According to the literature, reliance on PAT across clinical and surgical contexts should warrant careful consideration given ongoing concerns about its validity as a measure of hamstring length in both static assessment and in gait. While increased PAT values are frequently interpreted as indicators of hamstring contracture, over 60% of individuals with flexed knee gait have been shown to present with normal or elongated hamstrings.40,43 Factors such as spasticity, impaired selective motor control, and lever arm dysfunction contribute significantly to flexed knee gait and are not captured by static tests like the PAT.1,40,33 FThe reliability of PAT is further limited by its reported low inter- and intra-rater agreement.15,16 Ten Berge et al. 15 found that all intraclass correlation coefficients were lower in the CP group (n = 15) compared with controls without CP (n = 15), and that intraobserver reliability was reasonable (>0.75) for both groups, but lower in CP patients than controls.
In light of these concerns about the specificity and reliability of the PAT, it is particularly relevant to consider how often, and in what way, studies incorporated three-dimensional motion data. Kinematic were reported in 20 studies, most often restricted to sagittal knee flexion/extension during discrete phases of stance. As emphasized by Gage et al., 1 3DMA provides critical insight into the dynamic components of gait pathology in CP, capturing features that static clinical tests such as the PAT cannot. This review showed fewer than two-thirds of studies included any kinematic assessment, and even when present, analysis was frequently limited to sagittal plane parameters at isolated points in the gait cycle.5,9,11,20,25,26,33,39,40,35–41 Notably, no study systematically analyzed compensatory mechanisms, multilevel joint interactions, or spatiotemporal adaptations throughout the full gait cycle—factors that are highly relevant to the functional expression of flexed knee gait. The correlation between static clinical findings and dynamic gait analysis was weak, 14 and improvements in popliteal angle did not consistently translate to measurable kinematic gains.27,25,39 Although some studies reported parallel improvements in PAT values and gait kinematics,5,19,24,28,30 these findings were not uniform across the literature. Taken together, the evidence suggests that while the PAT may retain clinical utility, the principal limitation lies not in its use per se, but rather in its application as the sole criterion for surgical indication or as an isolated intraoperative determinant.
Beyond questions of validity and correlation with gait function, another major limitation of the available evidence concerns the duration and consistency of follow-up. The limited duration of follow-up in most studies represents a significant limitation in evaluating the long-term impact of interventions guided by the PAT. Only seven studies reported outcomes beyond 2 years. The lack of extended follow-up studies should raise concerns regarding the validity of the present data presenting the PAT as an indicator for surgery and the potential for survivorship bias of the present literature. Although the importance of assessing outcomes at skeletal maturity has been emphasized, 12 most surgical studies included in this review were with pediatric polulations with follow-up less than 2 years.
In this review, the inclusion criteria were restricted to studies that explicitly referenced the PAT, which may have excluded relevant work focusing primarily on kinematic outcomes or other clinical assessments. In addition, variability in outcome measures and inconsistent reporting of participant characteristics—such as functional classification, surgical details, and follow-up protocols—limited the ability to synthesize findings across studies and conduct meta-analysis.
Conclusion
This systematic review suggests that the PAT remains widely used in the evaluation and surgical management of flexed knee gait in children with CP. Although postoperative improvements in PAT values were frequently reported, these outcomes were not reliably compared with results from three-dimensional gait analysis due to marked heterogeneity in study design, reporting methods, and follow-up protocols. Based on this review it appears that the main limitation is not the use of the PAT, but its application as the sole determinant for surgery or as an isolated intraoperative criterion given the paucy of data regarding its validity. Integration of PAT findings with standardized gait analysis should be considered. Future research should prioritize harmonized protocols, consistent reporting of patient characteristics, and long-term follow-up through skeletal maturity to clarify the prognostic value of the PAT within comprehensive surgical decision-making protocols.
Supplemental Material
sj-pdf-1-cho-10.1177_18632521251396657 – Supplemental material for The role of the popliteal angle as an indicator for hamstring lengthening to treat a flexed knee gait in children with cerebral palsy: A systematic review
Supplemental material, sj-pdf-1-cho-10.1177_18632521251396657 for The role of the popliteal angle as an indicator for hamstring lengthening to treat a flexed knee gait in children with cerebral palsy: A systematic review by Giulia Beltrame, Pari Lee Palandjian, Viveka Jain and Paulo Selber in Journal of Children's Orthopaedics
Footnotes
Author contributions
GB led data extraction, performed data analysis, led original drafting of the article, and reviewed and edited the article. PP extracted data, performed data analysis, and reviewed and edited the article. VJ extracted data and reviewed and edited the article. PS conceived review topic, and wrote and edited the article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethics statement
There are no human participants in this article and informed consent is not required.
Data availability statement
The datasets generated and/or analyzed during the current study via data extraction of published articles are available from the corresponding author on reasonable request.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.