
Abstract
Purpose
The distal femoral extension osteotomy (DFEO) is often used in the treatment of crouch gait to help compensate for knee flexion contractures. The effects of DFEO on skeletal and muscle lengths are incompletely understood, but are important to consider in planning concomitant surgeries such as patellar tendon advancement (PTA). Therefore, the purpose of this study was to quantify the changes in femur, quadriceps, and hamstring lengths with DFEO, and to determine the sensitivity to surgical factors such as wedge location and magnitude.
Methods
A musculoskeletal model with six degrees of freedom tibiofemoral and patellofemoral joints was used for analysis. A wedge was removed from the distal femur and the remaining bone segments were plated together to simulate the DFEO. After simulating the knee's post-operative equilibrium, the surgically-induced changes in muscle and bone lengths were analysed.
Results
Relative to the pre-operative state, DFEO stretches the hamstrings while shortening the femur and quadriceps. A more posterior wedge apex location (i.e. creation of a cuneiform wedge) diminished the stretch of the hamstrings, but induced greater shortening of the femur and quadriceps. More proximal wedge locations necessitated greater translation of the distal fragment to maintain the knee joint axis.
Conclusion
Reduced quadriceps length after DFEO shown in this study is consistent with the need for simultaneous PTA. The induced hamstring stretch also may represent a potential mechanism for post-operative nerve palsies. Overall, the numerical results provide a firmer basis for planning the specifics of DFEO such that desired muscle lengths and joint alignment are achieved.
Introduction
Crouch gait is a common gait abnormality in cerebral palsy, and is characterised primarily by excessive knee flexion in stance.1,2 Historically, crouch has been challenging to treat, and recurrence after treatment is common.3,4 The distal femoral extension osteotomy (DFEO) and patellar tendon advancement (PTA) are surgical procedures performed simultaneously in the treatment of crouch gait. 5 The DFEO removes an anterior wedge from the distal femur to compensate for static contracture of the posterior capsule, 5 effectively straightening the lower limb. The PTA moves the patellar tendon insertion distally to take up the slack in the quadriceps induced by the DFEO, and to correct both patella alta and extensor lag, which often co-exist in crouch gait patients. The procedures have been shown to improve gait kinematics, especially at the knee joint,6–9 and maintain them at long-term (8+ years) follow-up. 10 However, despite the benefits, the risk of complications is present and questions regarding the surgical details (magnitude and geometry of correction) persist. 6
By design, DFEO procedures substantially alter the geometry and behaviour of muscles in the lower extremity. Of particular relevance is the effect that the procedure has on muscle lengths, which has implications on the need for concomitant soft-tissue procedures. For example, cuneiform wedges are suggested in the case of larger contractures to shorten the femur and avoid neurovascular compromise in the posterior compartment. 5 Further, a prior study found that DFEO procedures may induce improvements in hamstring operating lengths and speeds in gait, such that concomitant hamstring lengthening is not needed. 11 However, the model used in this study did not consider the effects that surgically induced changes in skeletal geometry have on muscle lengths.
Computational musculoskeletal models can be used to investigate the effects of skeletal deformities and surgical procedures on muscle behaviour. 12 For example, prior studies have investigated the influence of crouch postures and bony deformities on muscle lengths and moment arms.13–18 However, prior models do not include sufficient anatomical complexity and degrees of freedom (dof) at the knee to fully capture the effects of a DFEO. We have recently introduced a novel musculoskeletal model that can be used for surgical simulation. The model includes six dof at the tibiofemoral and patellofemoral joints. 19 This model incorporates the effects of contact and ligamentous constraints, and has been validated against in vivo measures of tibiofemoral and patellofemoral movement during unloaded and loaded activities. 19 It has been used for various applications, including for estimating muscle forces in children with crouch gait and to simulate the PTA procedure. 20
The objective of this study was to use this computational knee model to quantify the effects of a knee flexion contracture and corrective DFEO procedure on femur, quadriceps, and hamstrings lengths. To do this, we first tightened the posterior capsule ligaments to simulate a contracture. Then DFEO was virtually performed, and the post-surgical mechanical behaviour of the knee was determined. A sensitivity study was conducted to assess outcomes with different DFEO wedge locations and magnitudes. We hypothesised that the geometric changes of the DFEO would reduce the lengths of the quadriceps and hamstrings compared with the upright position, but that hamstring length would increase when accounting for an initial knee flexion contracture. The ultimate goal was to help quantify how surgical choices made in DFEO procedures affect the need for and performance of concomitant surgeries that are often used to correct crouch gait.
Materials and methods
The DFEO surgical procedure has been detailed by Novacheck et al. 5 First, an anterior wedge of bone is excised from the distal femur matching the magnitude of the knee flexion contracture (Fig. 1). The distal cut for the wedge is perpendicular to the tibial shaft (which is flexed relative to the femur due to contracture), and the proximal cut is perpendicular to the femoral shaft. The wedge apex location can be varied, such that either a triangular wedge is removed if the apex is at the posterior surface of the femur, or a cuneiform wedge is excised if the apex is more posterior. If an Arbeitsgemeinschaft für Osteosynthesefragen (AO) blade plate (DePuy Synthes, West Chester, Pennsylvania) is to be used for fixation, just prior to creation of the distal cut, the AO chisel (DePuy Synthes, West Chester, Pennsylvania) is placed 5 mm to 10 mm distal and parallel to the intended distal cut plane. This chisel location will later become the location of the fixation plate (blue structure in Fig. 1). A rotation about the wedge apex and a translation along the proximal cut plane are completed such that the fixation plate lines up with the femoral shaft. The goal is to maintain the knee flexion-extension axis, without anterior-posterior translation of the distal fragment. 5
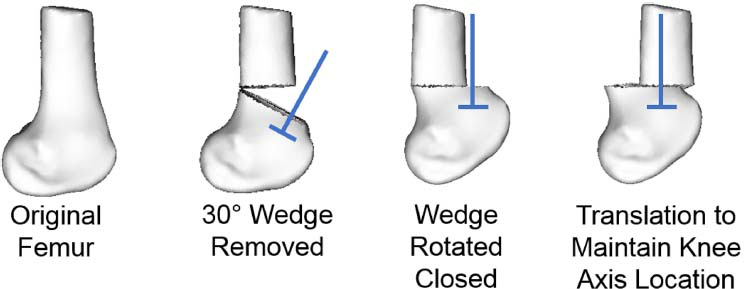
Demonstration of a 30° distal femoral extension osteotomy (DFEO) procedure. A 30° wedge is removed from the femur. Then, based on the placement of the chisel/fixation plate location (represented by the blue structure), the wedge is rotated and translated, such that the knee flexion extension axis remains in the same anterior-posterior location (and the plate aligns with the femoral shaft).
The creation of the lower extremity model with six dof tibiofemoral and patellofemoral joints has been described elsewhere. 19 In brief, we used bone and cartilage geometries and ligament path descriptions from MR images of a healthy adult female (mass 61 kg, height 1.65 m) to create a three body knee model (Fig. 2). Sets of non-linear spring elements 21 forming 14 ligament bundles connected ligament origins and insertions. Cartilage contact pressures were determined by the penetration of the cartilage meshes and an elastic foundation model. 22 The cartilage properties were assumed based on literature values (elastic modulus = 5 MPa,21,23 Poisson's ratio = 0.45,21,23–25 combined cartilage surface thickness = 6 mm (i.e. 3 mm each)). 26 As before, this knee model was then inserted into a lower extremity model from the literature that included 44 musculotendon units acting about the hip, knee and ankle. 27 We should note that this formulation of the model allowed for knee mechanics to evolve naturally, as functions of the muscle, ligament, contact, inertial and external forces. This model has been previously validated against 3D kinematics measured with MRI. 19
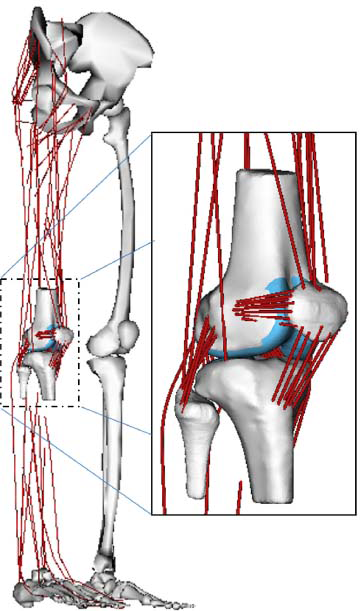
Model of the lower extremity used for simulation.
To better replicate the functional state of a child with crouch gait, the model was altered to include a knee flexion contracture. The reference strains of the posterior capsule bundles were increased such that the knee remained flexed to 30° even when a 5 Nm torque was applied during a passive forward simulation as might be expected in a clinical exam of contracture.
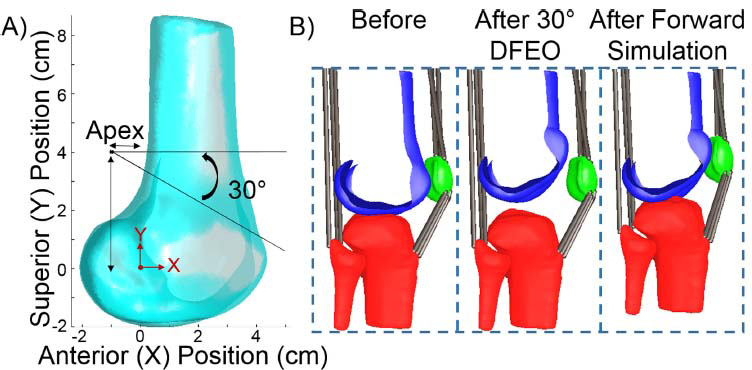
To model the DFEO, we virtually rotated and translated a distal femoral fragment relative to the proximal femur (Fig. 3). To do this, an anterior wedge of bone was removed and the distal fragment was rotated about the wedge apex to close the wedge, and then the distal fragment was translated such that the knee axis remained at the same anterior-posterior location, as described above. The articular cartilage surfaces and ligament origins and insertions were rotated and translated with the distal femur fragment, such that their anatomic locations/insertions were not altered. For each simulated procedure, a passive forward simulation 12 was run in which muscles were assumed to be minimally active (1% activation level). Simulations were continued until both the tibiofemoral and patellofemoral joints settled into new equilibrium configurations. The new lengths of the quadriceps and hamstrings were determined and compared with the lengths of these muscles in the nominal model (i.e. upright) as well as to their length after the simulation of contracture described above. Comparison with the nominal model represents changes in muscle lengths just due to the change in bony geometry, while comparison with the contracted posture takes into account both bony and postural changes at the knee. The semimembranosus was chosen as a representative hamstring muscle and the vastus medialis was chosen as a representative quadriceps muscle. The nominal length of the semimembranosus in this model was 41.09 cm, and the vastus medialis was 18.03 cm.
(
To determine the sensitivity to wedge apex location, the superior and anterior locations of the wedge apex were modified and the simulations re-run. To determine the sensitivity to wedge magnitude, the wedge angle was modified between 10° and 30° in 10° increments.
Results
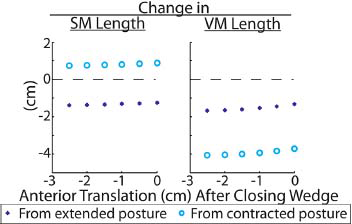
Varying the anterior location of the apex of the DFEO wedge had a larger effect on femur and muscle lengths than varying the superior position (Fig. 4). The osteotomy tended to increase semimembranosus lengths compared with their state in a contracted posture (i.e. from the pre-operative state), though they remained shorter than lengths that would occur in a fully extended intact knee (i.e. when accounting for only bony changes, not postural). Vastus medialis lengths were substantially reduced compared with that seen in both extended and contracted postures pre-surgically.
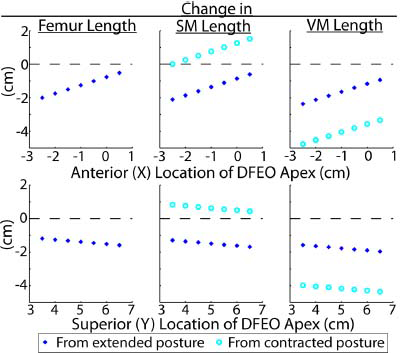
Change in femur, semimembranosus (SM, hamstring), and vastus medialis (VM, quadriceps) lengths between the original model and model with distal femoral extension osteotomy (DFEO) performed. Muscle lengths are referenced to the model both in an extended posture (which quantify muscle length changes due only to alteration in bony anatomy) and to the model with a 30° knee flexion contracture (which quantifies muscle changes due to bony and postural changes). Nominal Y location for the DFEO wedge was 4.0 cm, and X location was -1.0 cm.
Simply closing the wedge by rotating the distal fragment around the cut apex translates the knee axis anteriorly, so posterior translation is needed to maintain the knee axis position. The superior-inferior location of the wedge apex location had a larger effect on the distance needed to translate the distal segment to keep the knee axis at the same anterior-posterior location (Fig. 5). A 1.0 cm change in the superior location of the apex changes the translation distance (or chisel location) by 0.5 cm. In contrast, a 1.0 cm change in the anterior location of the apex needed a 0.1 cm change in translation.
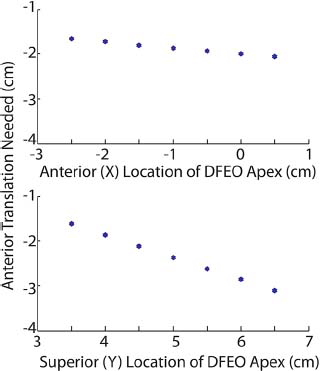
Posterior translation of the distal fragment after rotation for different wedge apex locations. Nominal Y location for the distal femoral extension osteotomy (DFEO) wedge was 4.0 cm, and X location was -1.0 cm as indicated in Figure 3. The magnitude of these changes also represents how far anterior the knee axis would be if the wedge was simply closed with no translation.
For the nominal wedge condition, changing the amount of posterior translation after rotation of the distal fragment around the wedge apex had a small effect on muscle lengths. No translation led to more lengthening of the hamstrings from the contracted position, but less quadriceps shortening. The translation had a larger effect on quadriceps lengths than hamstrings lengths (Fig. 6). A posterior translation of 2.5 cm changed the hamstrings lengths by 0.2 cm compared with no posterior translation, while the quadriceps lengths changed by 0.4 cm from no translation. The effects were non-linear.
Changes in semimembranosus (SM) and vastus medialis (VM) lengths with differences in the posterior translation of the distal fragment. These changes are for a wedge of X = -1.0 cm, Y = 4.0 cm (see Fig. 3), and angle 30°.
Discussion
The aim of this project was to quantify the effect of DFEO wedge location and magnitude on femur and muscle lengths post-operatively. The results show that changing the anterior-posterior location of the wedge apex had a much larger effect on muscle and femur lengths than changing the superior-inferior location. However, changing the super-inferior position had a much larger effect on the knee axis location, with higher positions requiring greater translation of the fragment after rotation to maintain the joint position. These relationships are important for surgeons to understand when completing a DFEO as part of the treatment of crouch gait, and have implications on the need for concomitant soft-tissue surgeries.
The effects of DFEO procedures on hamstring lengths is important to consider given the potential for the hamstrings to induce crouch walking postures. 28 Our study suggests that, compared with the contracted (pre-operative) knee flexion position, the hamstrings tend to undergo stretching when a DFEO procedure is used to straighten the limb. Stretching of the hamstrings is of clinical concern, as this may also introduce tension in the posterior compartment structures. Nerve palsies, presumably from this increased tension, are recognised complications of DFEO.5,6,29 Hamstring stretching can be avoided by removing a cuneiform wedge of bone (posterior wedge apex, Fig. 3). However, a cuneiform wedge increases both femoral shortening and induces additional slack in the quadriceps, which may affect function post-operatively. It is important to recognise that the change in hamstring lengths computed in this study do not necessarily reflect operating/dynamic hamstring lengths, which depend on pelvis, hip and knee postures adopted in walking.30,31 A prior study estimated hamstring lengths from gait kinematics and found that the hamstrings may indeed operate at longer lengths following DFEO. 11 However, this prior study was limited in that it did not account for changes in skeletal geometry induced by DFEO which can affect hamstring lengths and force generation in multiple ways. DFEO can directly alter the moment arms of the muscles about the hip, a cuneiform wedge can directly shorten the path length of the muscle, and translation and/or rotation of the distal segment can alter the shaft relative to the condyles thereby affecting the wrapping length and moment arms about the knee. 11
Quadriceps undergo substantial shortening with DFEO, which can be compensated for by performing a simultaneous PTA. The importance of simultaneous PTA to the clinical outcomes of DFEO procedures has previously been documented. 6 In the generic musculoskeletal model used in this study, we found that ∼ 3 cm distal translation of the patellar insertion is needed after DFEO to re-establish the quadriceps lengths seen in a limb with a 30° knee flexion contracture. This amount is slightly greater than the 2 cm PTA commonly performed, 5 though this discrepancy may in part arise from scaling differences between our adult-size model and children. PTA also acts to correct patella alta, which often coexists in crouch gait patients. However, it is not a given that the quadriceps shortening induced via DFEO would match the PTA needed to correct patella alta. In fact, current surgical guidelines already re-position the patella in an abnormally inferior, or baja, position.5,6 While patella baja does not seem to detrimentally affect knee flexion patterns in walking, it could have implications for joint strengths in flexed postures such as stair climbing and chair rise.6,20 Indeed, a recent study has shown that chair rise is impaired in DFEO with PTA patients. 32 The modelling work in this study provides a stepping stone to planning the specifics of a DFEO such that PTA simultaneously addresses quadriceps shortening, extensor lag, and patella alta.
In the current operative technique, 5 the surgeon aims to keep the flexion-extension axis of the knee in its original anterior-posterior location. This requires translation of the distal fragment, achieved by correct placement of the chisel along the cut plane. A superior location of the osteotomy apex requires a more anterior chisel location (or larger translation of the distal segment), as rotation about this high apex moves the knee axis anterior. If the osteotomy is high enough, the translation is likely not clinically achievable, as it results in severe posterior displacement of the distal segment (Fig. 7). This is important to consider surgically, as high osteotomies will be expected to alter the location of the knee axis. An alteration in this axis likely could have important implications for muscle moment arms and torque generation, and possibly tibiofemoral contact location. These changes will be the subject of future work.
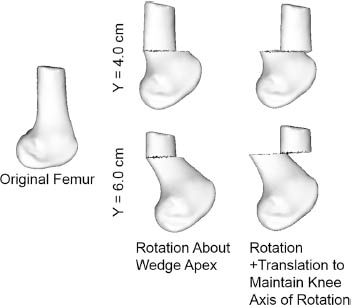
A look at the change in the knee axis locations with two wedge apex locations. All wedges removed are of 30° magnitude. (Top) A wedge location of X = 0.0 cm, Y = 4.0 cm shows only a small anterior translation of the femoral axis (left), which can be corrected with posterior translation (right). (Bottom) A wedge location of X = 0.0 cm, Y = 6.0 cm shows a greater translation of the femoral axis with rotation of the distal segment (left). Translation of the distal fragment to have the knee axis in the original position shows discontinuity between the two segments. This is not clinically feasible, and likely represents a case in which the knee axis will change with surgery.
Musculoskeletal models have previously been used to investigate the effects of crouch gait and treatment on muscle lengths. However, these models have been limited in their ability to make predictions of muscles surrounding the knee joint due to limited degrees of freedom. To overcome this limitation, we used a model with 6 dof tibiofemoral and patellofemoral joints that included ligamentous structures and articular surface geometries. A model of cartilage contact allows us to predict the post-surgical kinematics in an extended posture. In future work, we intend to use the model to simulate knee mechanics during gait, thus allowing further insights into the effects of DFEO on knee function. Of particular interest is the effects of DFEO on cartilage loading patterns, which have been theorised to contribute to changes in tibial slope post-operatively in skeletally immature patients. 33
There are a few limitations to this study. First is our use of an otherwise normal lower extremity model. Many children with crouch receiving this surgery have other bony (e.g. femoral anteversion) or positional (e.g. increased pelvic tilt) abnormalities that may affect our results. A previous study of crouch gait has suggested the effects of anteversion on hamstring lengths may be minimal. 18 Still, in future work, we will determine the sensitivity of our results to these common abnormalities seen in cerebral palsy. Secondly, all of the simulated procedures assumed a cut made perpendicular to the sagittal plane, and did not include any effects of out-of-plane cuts or femoral derotations that are often performed concurrently. Our goal was to examine the effects of extension osteotomy alone, as it is used for the treatment of crouch, though future work will investigate the effects of other surgical alterations of the distal femur. Initial evaluation with our model has that a 30° internal rotation osteotomy shortened the semimembranosus by only 3 mm, and lengthened the vastus medialis by only 2 mm, which agrees well with a prior study supracondylar derotational osteotomies. 34 The muscle length changes that occur with 3D osteotomies is complex, but will be important to understand as modelling work moves towards surgical planning. Thirdly, functional muscle lengths of the biarticular muscles (e.g. rectus femoris, hamstrings) during gait depend on multiple joint angles and often have non-intuitive functions.28,35 Thus, consideration of post-operative gait pattern is important for estimating changes in walking ability after the procedure. Also, this study did not include any representation of spasticity, as it does not play a role in the geometric changes studied here. However, length changes explored here can give some insight into how these muscles may behave dynamically, with stretched hamstring muscles likely exhibiting more passive force and increased spastic response.34,36,37 Overall, the changes associated with postural changes and dynamic function are subject to many more patient-specific factors, which will need further investigation.
In conclusion, the location and magnitude of DFEO can have substantial effects on the muscle and femur lengths seen post-operatively, which we have quantified in this study. These factors should be carefully considered when determining patient-specific DFEO parameters to compensate for knee flexion contractures, and when performing simultaneous procedures such as PTA to treat crouch gait.
Footnotes
This work was supported in part by the Clinical and Translational Science Award Program, through the NIH National Center for Advancing Translation Sciences, grant UL1TR000427. The authors would also like to gratefully acknowledge the support of the NIH (F30AR065838 and R21HD084213) and the UW Medical Sciences Training Program (NIH T32GM008692).
RLL, CRS and DGT have received grants from the NIH to support this work. All other authors declare they have no conflicts of interest.